
Long-Term Use and Application of Systematic Tailored Assessment for Responding to Suicidality (STARS) Protocol Following Original Training

 ,
,  ,
, 

 ,
,  and
and
Abstract
:1. Introduction
1.1. Suicide Risk Assessment Processes—Structured Professional Judgement and Application
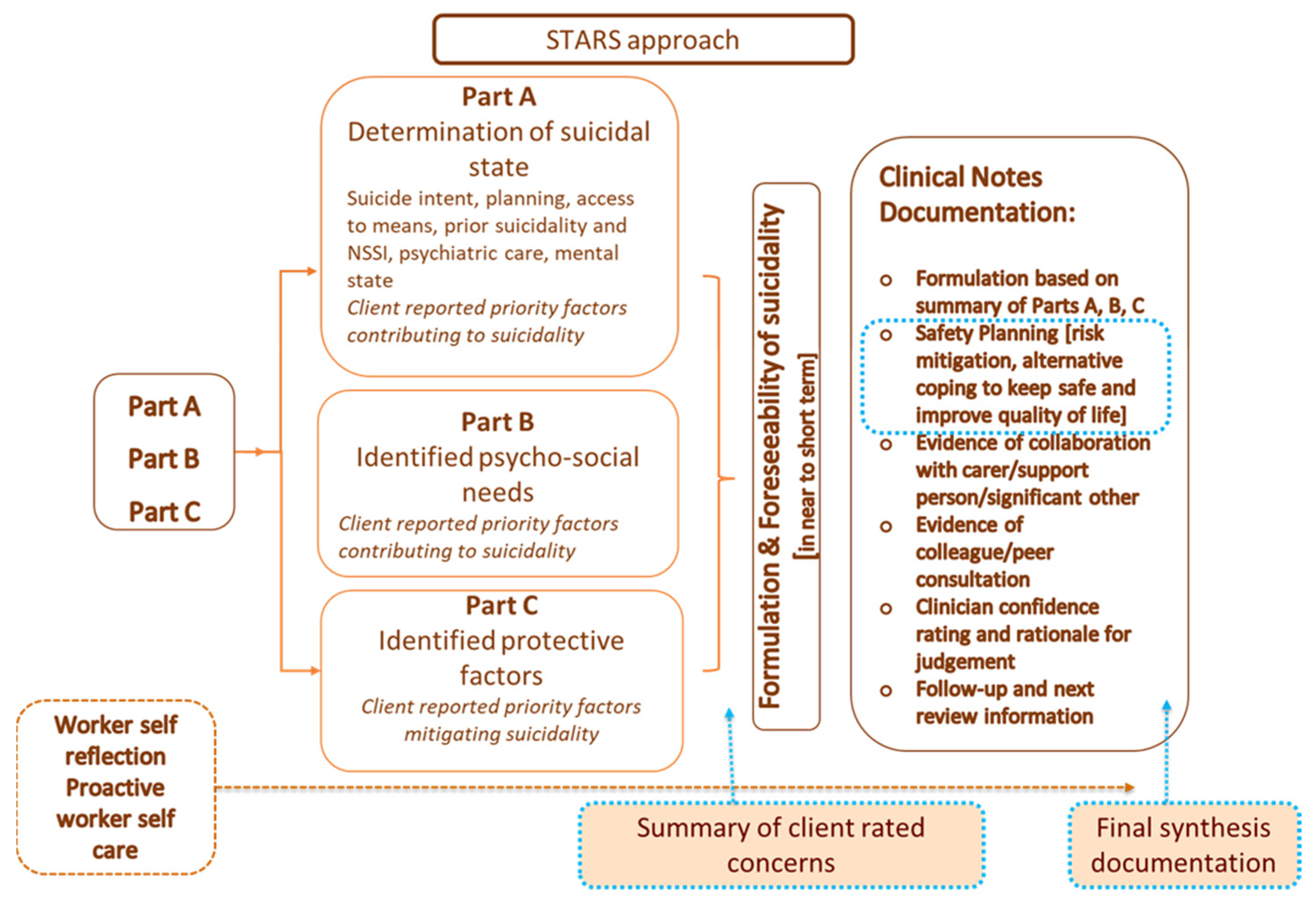
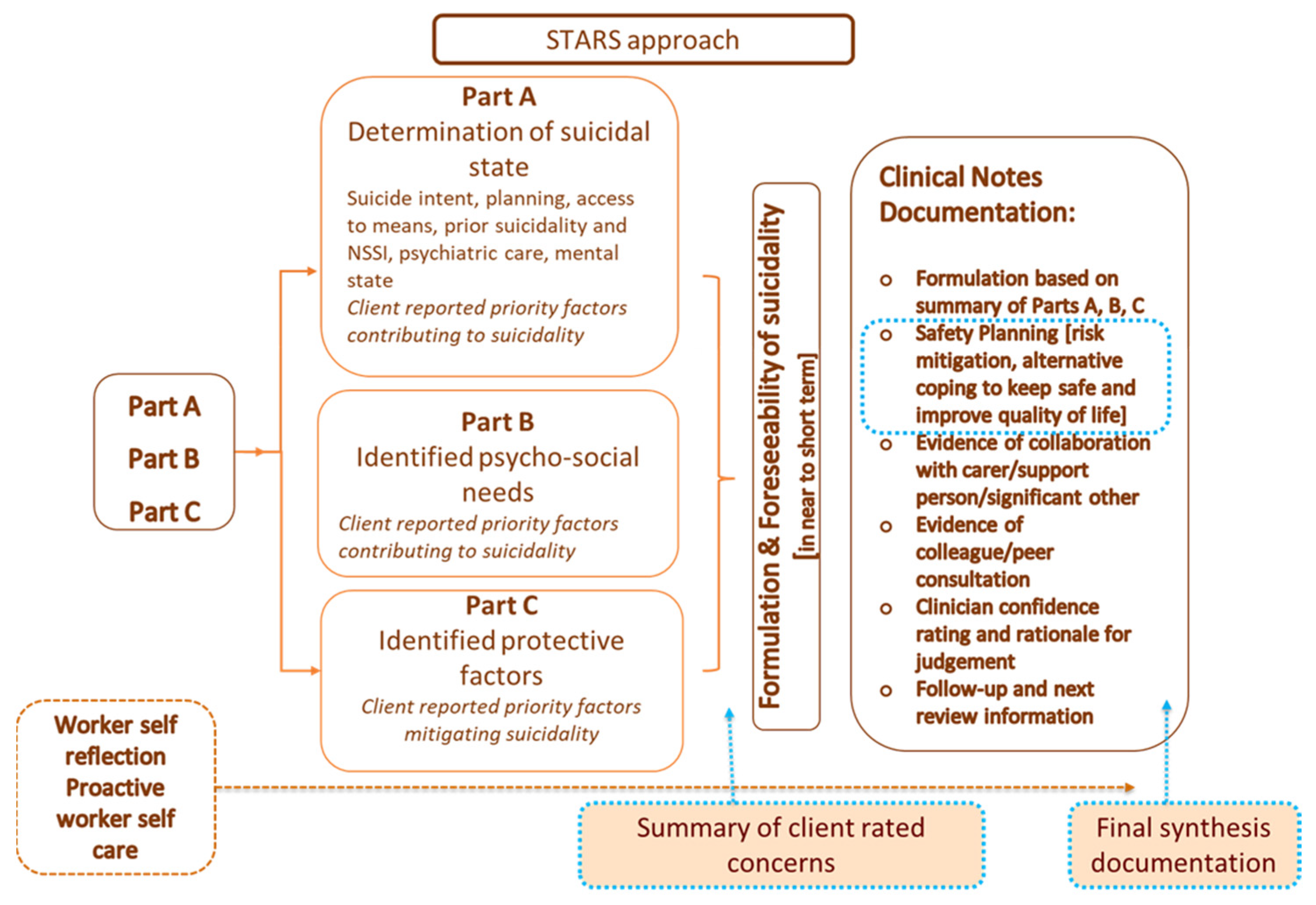
1.2. Systematic Tailored Assessment for Responding to Suicidality
1.3. Mental Health Professionals’ Perceptions of STARS-p and the Need for Training in Its Administration
2. Study Rationale and Aims
- Examine STARS-trained MHPs’ use, perceptions and reasons for use of STARS-p over the 12–24-month period post-training. It was hypothesized that, when using STARS-p, the majority of participants would not use the entire STARS-p with their clients in one administration. Further, it was expected that the main reason for administering STARS-p in practice would be client expressions of suicidality.
- Investigate associations between practitioners’ demographic and clinical characteristics and their use and perceptions of STARS-p in practice over the 12–24-month post-training period. It was hypothesized that greater formal training (workshops) and informal training (supervision) would be associated with more frequent administration of the entire STARS-p. Further, it was hypothesized that practitioners reporting that they typically administered the entire STARS-p would have more positive perceptions of ease of administration, client experience (of being validated), client-centeredness, as well as confidence in the usefulness of data for informing interventions to mitigate suicidality.
3. Materials and Methods
3.1. Participants and Recruitment
3.2. Questionnaire
Use of STARS-Protocol and Clinician Perceptions
3.3. Analyses
4. Results
4.1. Participants
4.2. Use of STARS-p and Reasons for and Perceptions of Use
4.3. Associations between Use of STARS-p, Professional Characteristics, and Perceptions of STARS-p
4.4. STARS-Trained Practitioners’ Perceptions of STARS-p and Improvements for Practice
5. Discussion
5.1. STARS-Trained Practitioners’ Use of STARS-p Sections
5.2. Main Reasons for Using STARS-p in Practice, and Perceptions of STARS-p
5.3. Use of STARS-p and Associations with Professional Characteristics and Perceptions of the STARS-p 12–24 Months after Training
5.4. Perceptions of STARS-p and Improvements for Practice
5.5. Limitations
5.6. Implications
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lewitzka, U.; Sauer, C.; Bauer, M.; Felber, W. Are national suicide prevention programs effective? A comparison of 4 verum and 4 control countries over 30 years. BMC Psychiatry 2019, 19, 158. [Google Scholar] [CrossRef]
- Ahmed, F.; Sifat, R.I. Strategic assessment of mental health and suicide amid COVID-19 pandemic in Bangladesh. Int. J. Health Plan. Manag. 2021, 36, 980–985. [Google Scholar] [CrossRef]
- Gonçalves, M.; André, R.; Sereijo, C.; Andrade, G.; Saraiva, R.; Linhares, L.; Chendo, I.; Abreu, M. Covid 2019 and suicide—A global pandemic: How to prevent? Eur. Psychiatry 2021, 64, S588. [Google Scholar] [CrossRef]
- Moutier, C. Suicide prevention in the COVID-19 Era: Transforming threat into opportunity. JAMA Psychiatry 2021, 78, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Deady, M.; Tan, L.; Kugenthiran, N.; Collins, D.; Christensen, H.; Harvey, S. Unemployment, suicide and COVID-19: Using the evidence to plan for prevention. Med. J. Aust. 2020, 213, 153. [Google Scholar] [CrossRef] [PubMed]
- Davenport, T.A.; Lamonica, H.M.; Rowe, S.; Sturgess, J.; Scott, E.M.; Lee, G.; Cheng, V.W.S.; Hickie, I.B. Innovative preclinic triage system to guide Australians to the right mental health care first time. Aust. Health Rev. 2021, 45, 578–583. [Google Scholar] [CrossRef]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; Pirkis, J.; Appleby, L.; et al. COVID-19 Suicide Prevention Res Co. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. [Google Scholar] [CrossRef]
- Department of Health. The Fifth National Mental Health and Suicide Prevention Plan; National Mental Health Commission: Sydney, NSW, Australia, 2017.
- Department of Health. National Suicide Prevention Adviser Final Advice; Australian Government: Canberra, ACT, Australia, 2020.
- Hawgood, J.; Ownsworth, T.; Kõlves, K.; Spence, S.; Arensman, E.; De Leo, D. Impact of Systematic Tailored Assessment for Responding to Suicidality (STARS) Protocol Training on Mental Health Professionals’ Attitudes, Perceived Capabilities, Knowledge, and Reluctance to Intervene. Front. Psychiatry 2022, 12, 2653. [Google Scholar] [CrossRef]
- Hawgood, J.; Woodward, A.; Quinnett, P.; De Leo, D. Gatekeeper Training and Minimum Standards of Competency. Crisis 2021. [Google Scholar] [CrossRef]
- Cramer, R.; Johnson, S.; McLaughlin, J.; Rausch, E.; Conroy, M. Suicide risk assessment training for psychology doctoral programs: Core competencies and a framework for training. Train. Educ. Prof. Psychol. 2013, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Pisani, A.; Cross, W.; Gould, M. The Assessment and Management of Suicide Risk: State of Workshop Education. Suicide Life-Threat. Behav. 2011, 41, 255–276. [Google Scholar] [CrossRef] [PubMed]
- Carter, G.; Page, A.; Large, M.; Hetrick, S.; Milner, A.; Bendit, N.; Walton, C.; Draper, B.; Hazell, P.; Fortune, S.; et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guideline for the management of deliberate self-harm. Aust. N. Z. J. Psychiatry 2016, 50, 939–1000. [Google Scholar] [CrossRef] [PubMed]
- Carter, G.; Spittal, M. Suicide Risk Assessment. Crisis 2018, 39, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Large, M.; Ryan, C.; Carter, G.; Kapur, N. Can we usefully stratify patients according to suicide risk? BMJ 2017, 359, j4627. [Google Scholar] [CrossRef] [PubMed]
- Pokorny, A. Prediction of Suicide in Psychiatric Patients. Arch. Gen. Psychiatry 1983, 40, 249. [Google Scholar] [CrossRef]
- Quinlivan, L.; Cooper, J.; Meehan, D.; Longson, D.; Potokar, J.; Hulme, T.; Marsden, J.; Brand, F.; Lange, K.; Riseborough, E.; et al. Predictive accuracy of risk scales following self-harm: Multicentre, prospective cohort study. Br. J. Psychiatry 2017, 210, 429–436. [Google Scholar] [CrossRef]
- Chan, M.; Bhatti, H.; Meader, N.; Stockton, S.; Evans, J.; O’Connor, R.; Kapur, N.; Kendall, T. Predicting suicide following self-harm: Systematic review of risk factors and risk scales. Br. J. Psychiatry 2016, 209, 277–283. [Google Scholar] [CrossRef]
- Franklin, J.; Ribeiro, J.; Fox, K.; Bentley, K.; Kleiman, E.; Huang, X.; Musacchio, K.M.; Jaroszewski, A.C.; Chang, B.P.; Nock, M.K. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol. Bull. 2017, 143, 187–232. [Google Scholar] [CrossRef]
- Ribeiro, J.; Franklin, J.; Fox, K.; Bentley, K.; Kleiman, E.; Chang, B.; Nock, M. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: A meta-analysis of longitudinal studies. Psychol. Med. 2015, 46, 225–236. [Google Scholar] [CrossRef]
- Jobes, D.A.; Comtois, K.A.; Gutierrez, P.M.; Brenner, L.A.; Huh, D.; Chalker, S.A.; Ruhe, G.; Kerbrat, A.H.; Atkins, D.C.; Jennings, K.; et al. A randomized controlled trial of the collaborative assessment and management of suicidality versus enhanced care as usual with suicidal soldiers. Psychiatry 2017, 80, 339–356. [Google Scholar] [CrossRef] [Green Version]
- Cramer, R.J.; Kapusta, N.D. A social–ecological framework of theory, assessment, and prevention of suicide. Front. Psychol. 2018, 8, 1756. [Google Scholar] [CrossRef] [PubMed]
- Sequeira, L.; Strudwick, G.; De Luca, V.; Strauss, J.; Wiljer, D. Exploring Uniformity of Clinical Judgment. J. Patient Saf. 2022. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Wittouck, C.; Munck, S.; Portzky, G.; Rijsselberghe, L.; Autreve, S.; Heeringen, K. A Comparative Follow-up Study of Aftercare and Compliance of Suicide Attempters Following Standardized Psychosocial Assessment. Arch. Suicide Res. 2010, 14, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Bergen HHawton KWaters KCooper, J.; Kapur, N. Psychosocial assessment and repetition of self-harm: The significance of single and multiple repeat episode analyses. J. Affect. Disord. 2010, 127, 257–265. [Google Scholar] [CrossRef]
- Kapur, N.; Steeg, S.; Webb, R.; Haigh, M.; Bergen, H.; Hawton, K.; Ness, J.; Waters, K.; Cooper, J. Does clinical management improve outcomes following self-harm? Results from the multicentre study of self-harm in England. PLoS ONE 2013, 8, e70434. [Google Scholar] [CrossRef]
- Gray, N.; John, A.; McKinnon, A.; Raybould, S.; Knowles, J.; Snowden, R. Structured Professional Judgment to Assist the Evaluation and Safety Planning of Suicide Risk: The Risk of Suicide Protocol (RoSP). Front. Psychiatry 2021, 12, 607120. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence: Clinical Guidelines. Self-Harm in Over 8s: Long-Term Management (CG133). 2011. Available online: https://www.nice.org.uk/guidance/cg133 (accessed on 15 September 2020).
- Monahan, M.; Crowley, K.; Arnkoff, D.; Glass, C.; Jobes, D. Understanding Therapists’ Work with Suicidal Patients: An Examination of Qualitative Data. OMEGA J. Death Dying 2020, 81, 330–346. [Google Scholar] [CrossRef]
- Linehan, M.M.; Comtois, K.A.; Ward-Ciesielski, E.F. Assessing and managing risk with suicidal individuals. Cogn. Behav. Pract. 2012, 19, 218–232. [Google Scholar] [CrossRef]
- Hawgood, J.; De Leo, D. STARS Systematic Tailored Assessment for Responding to Suicidality; Griffith University: Brisbane, QLD, Australia, 2018. [Google Scholar]
- Hawgood, J.; De Leo, D. STARS Screening Tool for Assessing Risk of Suicide; Griffith University: Brisbane, QLD, Australia, 2015. [Google Scholar]
- Hawgood, J.; Ownsworth, T.; Mason, H.; Spence, S.; Arensman, E.; De Leo, D. A Pilot Study of Clinicians’ Perceptions of Feasibility, Client-Centeredness, and Usability of the Systematic Tailored Assessment for Responding to Suicidality Protocol. Crisis 2021. [Google Scholar] [CrossRef]
- Jahn, D.; Quinnett, P.; Ries, R. The influence of training and experience on mental health practitioners’ comfort working with suicidal individuals. Prof. Psychol. Res. Pract. 2016, 47, 130–138. [Google Scholar] [CrossRef]
- LoParo, D.; Florez, I.; Valentine, N.; Lamis, D. Associations of Suicide Prevention Trainings with Practices and Confidence among Clinicians at Community Mental Health Centers. Suicide Life-Threat. Behav. 2018, 49, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Roses in the Ocean. Lived Experience of Suicide. 2016. Available online: https://rosesintheocean.com.au/lived-experience-suicide/ (accessed on 2 September 2022).
- Watson, N.; Wooden, M. Identifying factors affecting longitudinal survey response. In Methodology of Longitudinal Surveys; Lynn, P., Ed.; John Wiley & Sons: Hoboken, NJ, USA, 2009; pp. 157–181. [Google Scholar]
- Baker, J.A.; Canvin, K.; Berzins, K. The relationship between workforce characteristics and perception of quality of care in mental health: A qualitative study. Int. J. Nurs. Stud. 2019, 100, 103412. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.; Shannon, S. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Shea, S.C. Suicide assessment: Part 1: Uncovering suicidal intent--a sophisticated art. Psychiatr. Times 2009, 26, 17. [Google Scholar]
- Mirick, R.; McCauley, J.; Bridger, J.; Berkowitz, L. Continuing education on suicide assessment and crisis intervention: What can we learn about the needs of mental health professionals in community practice? Community Ment. Health J. 2015, 52, 501–510. [Google Scholar] [CrossRef]
- Beyond Blue. The Way Back Support Services: Interim Evaluation Short Report. Available online: https://www.beyondblue.org.au/docs/default-source/about-beyond-blue/the-way-back-evaluation-docs/the-way-back-interim-report-short-version.pdf?sfvrsn=9467005e_2 (accessed on 6 June 2022).
- Hill, N.; Halliday, L.; Reavley, N. Guidelines for Integrated Suicide-Related Crisis and Follow-up Care in Emergency Departments and Other Acute Settings. Black Dog Institute. Available online: https://www.blackdoginstitute.org.au/wp-content/uploads/2020/04/delphi-guidelines-clinical-summary_web.pdf (accessed on 6 June 2022).
- Crowley, K. Collaborative Assessment and Management of Suicidality (CAMS): Adherence to a Flexible Clinical Framework. Ph.D. Thesis, The Catholic University of America, Washington, DC, USA, 2015. [Google Scholar]
- Sandford, D.; Kirtley, O.; Thwaites, R.; O’Connor, R. The impact on mental health practitioners of the death of a patient by suicide: A systematic review. Clin. Psychol. Psychother. 2020, 28, 261–294. [Google Scholar] [CrossRef]
- Rothes, I.; Henriques, M.; Leal, J.; Lemos, M. Facing a Patient Who Seeks Help after a Suicide Attempt. Crisis 2014, 35, 110–122. [Google Scholar] [CrossRef]
- Stanley, B.; Brown, G. Safety Planning Intervention: A Brief Intervention to Mitigate Suicide Risk. Cogn. Behav. Pract. 2012, 19, 256–264. [Google Scholar] [CrossRef]
- Gutierrez, P.M.; O’Connor, S.S.; Johnson, L.L.; Dwyer, M.; Mund, N.E.; Jobes, D.A. Training Clinicians to Provide Collaborative Assessment and Management of Suicidality-Group (CAMS-G) for Veterans. Mil. Behav. Health 2020, 8, 21–32. [Google Scholar] [CrossRef]
- Stewart, K.L.; Darling, E.V.; Yen, S.; Stanley, B.; Brown, G.K.; Weinstock, L.M. Dissemination of the safety planning intervention (SPI) to university counseling center clinicians to reduce suicide risk among college students. Arch. Suicide Res. 2020, 24 (Suppl. 1), 75–85. [Google Scholar] [CrossRef]
- Harned, M.S.; Lungu, A.; Wilks, C.R.; Linehan, M.M. Evaluating a multimedia tool for suicide risk assessment and management: The Linehan suicide safety net. J. Clin. Psychol. 2017, 73, 308–318. [Google Scholar] [CrossRef]

{kind=link}
| Gender | N | % |
| Male | 13 | 19.4 |
| Female | 54 | 80.6 |
| Work status | N | % |
| Full time | 45 | 67.2 |
| Part time | 20 | 29.9 |
| Casual | 2 | 3.0 |
| Role | N | % |
| MHP-wQ | 46 | 68.7 |
| * MHP-woQs | 21 | 31.3 |
| Education | N | % |
| High school or TAFE | 5 | 7.5 |
| Undergraduate | 14 | 20.9 |
| Postgraduate | 44 | 65.7 |
| Professional doctorate/PhD degree | 4 | 6.0 |
| Received any FORMAL training in suicide prevention/management SINCE STARS training | N | % |
| No | 43 | 64.2 |
| Yes | 24 | 35.8 |
| Received INFORMAL training | N | % |
| Weekly | 2 | 3.0 |
| Fortnightly | 14 | 20.9 |
| Monthly | 46 | 68.7 |
| Several times per year or less | 5 | 7.5 |
| Contact with suicidal persons | N | % |
| Daily | 5 | 7.5 |
| Several times per week | 10 | 14.9 |
| Weekly | 9 | 13.4 |
| Several times per month | 20 | 29.9 |
| Once per month | 11 | 16.4 |
| Multiple times per year | 12 | 17.9 |
| Loss of client by suicide (missing = 5) | N | % |
| No | 45 | 72.6 |
| Yes | 17 | 27.4 |
| Suicide attempt of client (missing = 1) | N | % |
| No | 11 | 16.7 |
| Yes | 55 | 83.3 |
| Use of STARS-p | 100% of Time | 75% of Time | 50% of Time | 25% of Time | Never | Missing | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | ||
| Administering the entire STARS-p (Parts A, B, C, safety planning and documentation sections) | 9 | 13.4 | 21 | 31.3 | 9 | 13.4 | 15 | 22.4 | 13 | 19.4 | 0 |
| Administering PART A (Suicide Enquiry items) | 44 | 68.8 | 10 | 15.6 | 1 | 1.6 | 4 | 6.3 | 5 | 7.8 | 3 |
| Client rated concerns | 27 | 41.5 | 21 | 32.3 | 3 | 4.6 | 6 | 9.2 | 8 | 12.3 | 2 |
| Therapist rated concerns | 18 | 27.7 | 22 | 33.8 | 9 | 13.8 | 7 | 10.8 | 9 | 13.8 | 2 |
| Administering PART B (Psycho-social risk factors) | 23 | 34.8 | 24 | 36.4 | 9 | 13.6 | 4 | 6.1 | 6 | 9.1 | 1 |
| Client rated concerns | 19 | 28.8 | 27 | 40.9 | 7 | 10.6 | 5 | 7.6 | 8 | 12.1 | 1 |
| Therapist rated concerns | 14 | 21.2 | 27 | 40.9 | 9 | 13.6 | 8 | 12.1 | 8 | 12.1 | 1 |
| Administering PART C (Protective factors) | 37 | 56.1 | 17 | 25.8 | 6 | 9.1 | 1 | 1.5 | 5 | 7.6 | 1 |
| Administering the SAFETY PLANNING section (within the Clinical Notes section) | 33 | 50.0 | 16 | 24.2 | 6 | 9.1 | 4 | 6.1 | 7 | 10.6 | 1 |
| Administering the DOCUMENTATION NOTES section (within the Clinical Notes section) | 19 | 28.8 | 19 | 28.8 | 9 | 13.6 | 6 | 9.1 | 13 | 19.7 | 1 |
| Reason for You to Use the STARS-p with a Client *: | Yes Responses | |
|---|---|---|
| N | % | |
| Direct verbalized suicide ideation | 63 | 94.0 |
| Observed mental illness symptoms/signs (e.g., apathy, withdrawal etc) | 51 | 76.1 |
| Specific mention in the referral | 51 | 76.1 |
| Comments of the person | 51 | 76.1 |
| Circumstances of the person (presenting problem) | 49 | 73.1 |
| Client reported behavioral changes | 48 | 71.6 |
| Emotional/distress observed in voice (e.g., anger, anxiety etc) | 45 | 67.2 |
| Reported life stressors/crises (e.g., financial, custodial, relationship etc) | 44 | 65.7 |
| Observation of the person | 43 | 64.2 |
| Changes in (increase) or habitual drug and alcohol use | 42 | 62.7 |
| Indirect (passive verbalization) ideation | 41 | 61.2 |
| I always conduct a risk assessment—mandatory in my organization | 21 | 31.3 |
| OR | 95% CI | p-Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Full STARS (n = 64) (Nagelkerke R2 = 0.513) | ||||
| Gender (male vs. female) | 17.26 | 2.16 | 138.12 | 0.007 |
| Ease of administration of the STARS-p | 20.43 | 4.11 | 101.51 | <0.001 |
| Part A (n = 61) (Nagelkerke R2 = 0.349) | ||||
| Ease of administration of the STARS-p | 8.94 | 1.76 | 45.40 | 0.008 |
| Suicide attempt of client (yes vs no) | 7.03 | 1.29 | 38.31 | 0.024 |
| Part B (n = 63) (Nagelkerke R2 = 0.203) | ||||
| Confidence in the use of STARS-p | 8.20 | 2.05 | 32.76 | 0.003 |
| Part C (n = 64) (Nagelkerke R2 = 0.301) | ||||
| Confidence in the use of STARS-p | 13.71 | 3.08 | 61.05 | 0.001 |
| Safety planning (n = 64) (Nagelkerke R2 = 0.320) | ||||
| Confidence in the use of STARS-p | 5.09 | 1.15 | 22.46 | 0.032 |
| STARS as a client-centred approach to determination of client’s current suicidality | 6.77 | 1.29 | 35.51 | 0.024 |
| Notes (n = 63) (Nagelkerke R2 = 0.440) | ||||
| Ease of administration of the STARS-p | 4.91 | 1.34 | 17.97 | 0.016 |
| Confidence in the use of STARS-p | 6.39 | 1.02 | 40.00 | 0.048 |
| Gender (male vs. female) | 12.90 | 1.19 | 140.37 | 0.036 |
| Questions (1 and 2 Collapsed) | Facilitators or Advantages to Protocol Use (58 Responses) | Barriers or Factors Discouraging Protocol Use (44 Responses) | Suggestions to Improve Protocol Use (20 Responses) |
|---|---|---|---|
| 1. Perceptions of long-term protocol use (n = 50) 2. Comments & suggestions for protocol & training (n = 36) | Practically helpful for assessment (n = 39) “I really value the program as it enhances and adds value to what I do in assessing clients (thanks)” “STARS is perfect for our complex clients. We are encouraged to do psycho-social needs-based responses, so....” “The protocol is great for my colleagues and I because we get referrals after discharge from hospital and staff at the ED rarely do a psycho-social assessment of needs and rarely ask the client what they think is their most important issue” “Despite hearing others’ refer to the length and intensity of using STARS, I think the tool does reduce clinicians jumping to action and encourages us to really sit with someone experiencing thoughts of suicide to understand their experience and work together on a plan” “STARS training was fabulous” “I found the training was very useful” Flexible for tailoring (n = 7) “I often have the whole session to administer STARS if it is an ‘intake’ session, but if not, I get through Part A and safety planning which is what we were told in the training—plus I would do documentation” “Part B is perfect for just informing the support plan. The documentation section helps with duty of care requirements in our organization” Client-focused in administration (n = 8) “Parts A, B and C and the safety planning section of STARS is really useful and helps to guide the risk assessment in a way that is still client focused” “Very client-centered, have found it very helpful” “Definitely client focused—helps me to confirm my observations and client intent” Comprehensive (n = 2) “I know that the STARS is a comprehensive interview—it takes time, but it is necessary and with COVID we need more reliable data like this” “A mindset” rather than just an assessment (n = 2) “For me it is the approach and mindset rather than the form that is the vital skill” | Time constraints (n = 27) “As a psychologist, usually limited to 50–55-min sessions, it is difficult to complete the whole STARS-p and still provide the client with therapy/treatment and meet the clients’ expectations to sufficiently engage them in therapy (lest they disengage at a point they are suicidal)” “Time constraints in the service make these questions difficult to answer fairly. Is there any way it could be broken down, so it was able to be used more fully in a service with limited client contact time?” Client-related factors (n = 12) “Aboriginal and Torres Strait Islander community prefer to yarn and not use pen and paper” “[However] …Some of my more acute clients would require two sessions to administer the whole protocol, unless I have time for a break and can therefore administer within the one session” “It is sometimes hard to use STARS with all clients. My biggest challenge is using it with people who are completely non-talkative. But when I ask them what they think the factors are they do open up” “I find the need for a risk assessment to be a difficult document as it takes away from me giving the client my whole attention—instead there is a heap of papers between us and it does not feel genuine to me” Cumbersomeness (n = 2) “I find it to be too lengthy”. “I personally find it difficult to use something so structured—something that would really need to be printed and gone through one step at a time”. Organizational (not mandated/required to use) (n = 3) “I do not use the STARS-p; I came to hear about it at the time because I was involved in facilitating a course on suicide prevention at xxx University. We wanted to learn about STARS for this reason, and I was mandated to go and participate in the training” “We are no longer required to use STARS; I use other tools”. “Unfortunately, I did not use it afterwards (after training).” | Changes to STARS-p (sections) (n = 9) “It would be great if the Safety Planning section was expanded with a lot more space. Similarly, this would be helpful in the sections that ask about method, and previous attempts, so there is more space to document the intricacies of what is reported”. “A more time conscious, abbreviated version of the tool would be wonderful given that a 51-min session only enables use of some elements of the protocol, while also conducting the necessary safety planning protocols that my workplace and practice requires” “I think it if had a digital version that succinctly put information together to save time, I would use it more”. “A digital form would be helpful—so that we can update and modify by saving a new copy each new file entry for the same client” Need for ongoing training (n = 6) “I think that people in my service need to get ongoing training in STARS. They have done the first training but then ‘give up’ on using the protocol and simply jot down assessment data in their charts. It is always so busy and staff do not seem to get that if you invest at the beginning, you will be even less likely to stress about needing more time down the track” “We need more refresher training—I did this, and it was excellent” The need to practice using STARS-p (n = 5) “The more I use it the more confident I get knowing I have gathered all the information” “Good instrument—we need to practice/develop better understanding in supervision sessions” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hawgood, J.; Kõlves, K.; Spence, S.H.; Arensman, E.; Krysinska, K.; De Leo, D.; Ownsworth, T. Long-Term Use and Application of Systematic Tailored Assessment for Responding to Suicidality (STARS) Protocol Following Original Training. Int. J. Environ. Res. Public Health 2022, 19, 11324. https://doi.org/10.3390/ijerph191811324
Hawgood J, Kõlves K, Spence SH, Arensman E, Krysinska K, De Leo D, Ownsworth T. Long-Term Use and Application of Systematic Tailored Assessment for Responding to Suicidality (STARS) Protocol Following Original Training. International Journal of Environmental Research and Public Health. 2022; 19(18):11324. https://doi.org/10.3390/ijerph191811324
Chicago/Turabian StyleHawgood, Jacinta, Kairi Kõlves, Susan H. Spence, Ella Arensman, Karolina Krysinska, Diego De Leo, and Tamara Ownsworth. 2022. "Long-Term Use and Application of Systematic Tailored Assessment for Responding to Suicidality (STARS) Protocol Following Original Training" International Journal of Environmental Research and Public Health 19, no. 18: 11324. https://doi.org/10.3390/ijerph191811324
APA StyleHawgood, J., Kõlves, K., Spence, S. H., Arensman, E., Krysinska, K., De Leo, D., & Ownsworth, T. (2022). Long-Term Use and Application of Systematic Tailored Assessment for Responding to Suicidality (STARS) Protocol Following Original Training. International Journal of Environmental Research and Public Health, 19(18), 11324. https://doi.org/10.3390/ijerph191811324