
Social Innovation in Home-Based Eldercare: Strengths and Shortcomings of Integrating Migrant Care Workers into Long-Term Care in Tuscany


Abstract
:1. Introduction
2. Social Innovation in Long-Term Care in Italy and its Regions
2.1. A Systematic Approach to Social Innovation
Social innovation is about new ideas that work to address pressing unmet needs. We simply describe it as innovations that are both social in their ends and in their means. Social innovations are new ideas (products, services, and models) that simultaneously meet social needs (more effectively than alternatives) and create new social relationships or collaborations.(EC, 2010)
what seems to emerge from empirical research is the opportunity to increase the denotative power of the concept of ‘social innovation’ by adopting operational definitions at a lower ladder of abstraction, which, on the one hand, allows the capture of different degrees of innovation and, on the other hand, takes into account the specificities of the policy and the welfare context in which solutions that can be qualified as ‘innovative’ are located.[29] (p. 129)
2.2. Italian Long-Term Care
2.3. Social Innovation in Practice: Regional Social Innovations in Italian Long-Term Care
3. Materials and Methods
3.1. Case Selection
3.2. Data Collection and Analysis
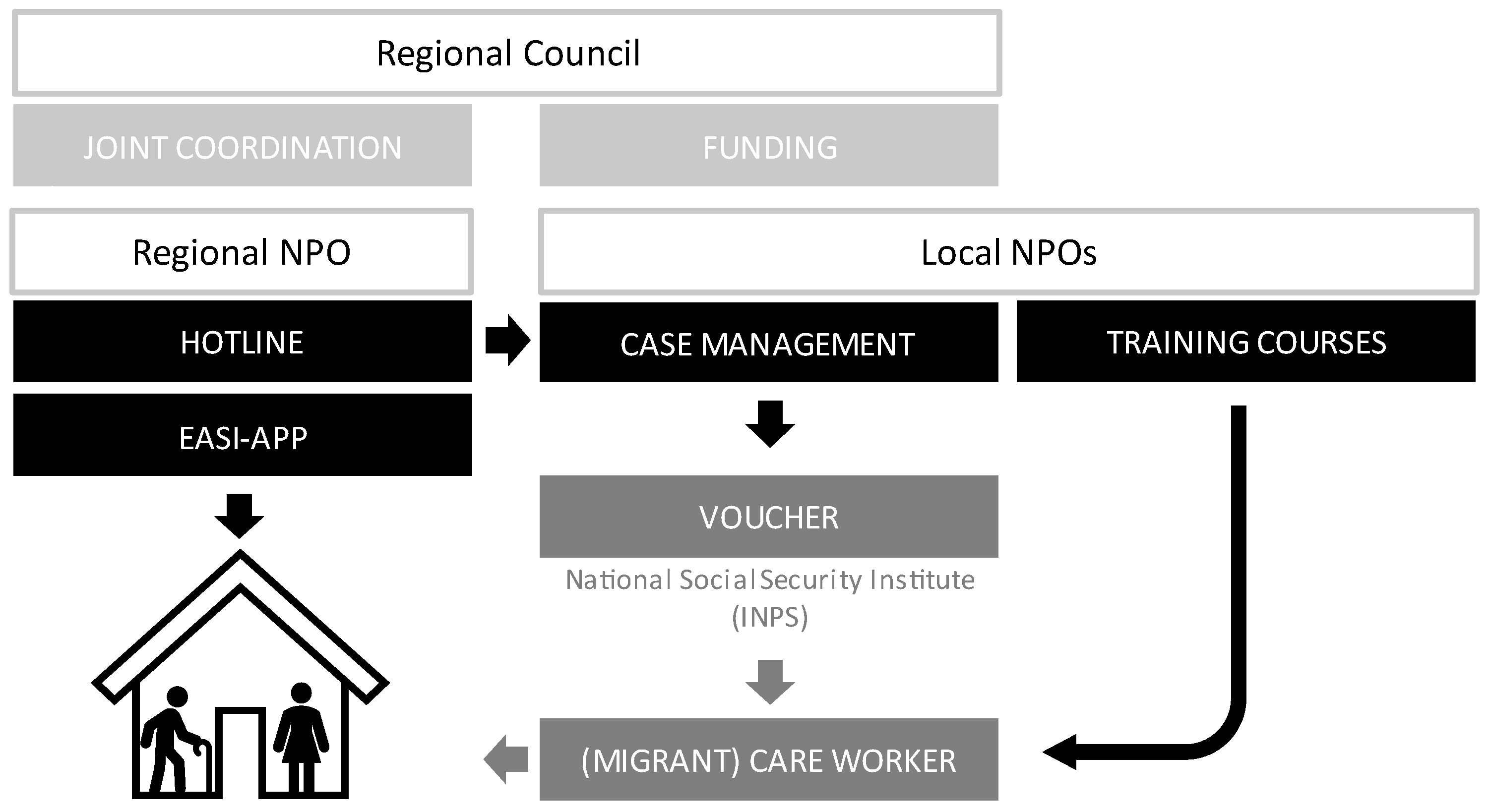
4. Overview of Pronto Badante
[Let’s say] I’m an old man of 80 years, I’m fine, [but then] I fall, I break my femur, I go to the hospital, they take me in, they operate, they do everything they have to do, and then they tell me you can’t stay here because there’s no room for the other [patients]. At that point the family comes into play, but how can the family face this emergency when it has no expertise?(NPO-1)
- More than 81,000 calls to the toll-free hotline;
- Almost 26,000 visits made to elderly persons’ homes;
- More than 18,700 vouchers issued for employed MCWs.
5. Pronto Badante as Social Innovation Good Practice?
6. Strengths
6.1. At-Home Assistance and Integrating Migrant Care Workers
6.2. New Forms of Relations and Collaborations
6.3. Resilience in Pandemic Times through Technology
7. Shortcomings
7.1. Limited Target Audience and Visibility: ‘The World Remains Outside’
7.2. Lacking Pathways to Formalisation and Measures to Cool off the ‘Hot Potato’
8. Conclusions
8.1. Core Findings
8.2. Strengths and Shortcomings
8.3. Limitations of the Study and Future Research
8.4. Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berloto, S.; Notarnicola, E.; Perobelli, E.; Rotolo, A. Report on COVID-19 and Long-Term Care in Italy: Lessons learned from An Absent Crisis Management. Available online: https://ltccovid.org/2020/04/10/report-on-covid-19-and-long-term-care-in-italy-lessons-learned-from-an-absent-crisis-management/ (accessed on 29 April 2022).
- Leitner, S. Varieties of familialism: The caring function of the family in comparative perspective. Eur. Soc. 2003, 5, 353–375. [Google Scholar] [CrossRef]
- Bettio, F.; Plantenga, J. Comparing Care Regimes in Europe. Fem. Econ. 2004, 10, 85–113. [Google Scholar] [CrossRef]
- Saraceno, C.; Keck, W. Can we identify intergenerational policy regimes in Europe? Eur. Soc. 2010, 12, 675–696. [Google Scholar] [CrossRef]
- Le Bihan, B.; Da Roit, B.; Sopadzhiyan, A. The turn to optional familialism through the market: Long-term care, cash-for-care, and caregiving policies in Europe. Soc. Policy Adm. 2019, 53, 579–595. [Google Scholar] [CrossRef]
- Barbabella, F.; Poli, A.; Chiatti, C.; Pelliccia, L.; Pesaresi, F. 2. La Bussola di NNA: Lo Stato dell’Arte basato sui Dati. In L’Assistenza agli Anziani non Autosufficienti in Italia-6° Rapporto-2017/2018-Il Tempo delle Risposte; Network-Non-Autosufficienza, Ed.; Maggioli Editore: Santarcangelo di Romagna, Italy, 2017; pp. 33–54. [Google Scholar]
- INPS. Osservatorio sui Lavoratori Domestici-Statistiche in Breve–Anno 2020; Istituto Nazionale della Previdenza Sociale: Rome, Italy, 2021. [Google Scholar]
- De Luca, M.; Tronchin, C.; Di Pasquale, E. Terzo Rapporto Annuale sul Lavoro Domestico-Analisi, Statistiche, Trend Nazionali e Locali; Osservatorio Nazionale DOMINA Sul Lavoro Domestico: Rome, Italy, 2021. [Google Scholar]
- Andall, J. Gender, Migration and Domestic Service: The Politics of Black Women in Italy; Ashgate: Aldershot, UK, 2000. [Google Scholar]
- Parreñas, R.S. Servants of Globalization: Migration and Domestic Work, 2nd ed.; Stanford University Press: Redwood City, CA, USA, 2015. [Google Scholar]
- Marchetti, S. Black Girls: Migrant Domestic Workers and Colonial Legacies; Brill: Leiden, The Netherlands, 2014. [Google Scholar]
- Ambrosini, M. Irregular but tolerated: Unauthorized immigration, elderly care recipients, and invisible welfare. Migr. Stud. 2015, 3, 199–216. [Google Scholar] [CrossRef]
- Solari, C.D. On the Shoulders of Grandmothers: Gender, Migration, and Post-Soviet Nation-State Building; Routledge: New York, NY, USA, 2017. [Google Scholar]
- van Hooren, F. Varieties of migrant care work: Comparing patterns of migrant labour in social care. J. Eur. Soc. Policy 2012, 22, 133–147. [Google Scholar] [CrossRef]
- Da Roit, B.; Weicht, B. Migrant care work and care, migration and employment regimes: A fuzzy-set analysis. J. Eur. Soc. Policy 2013, 23, 469–486. [Google Scholar] [CrossRef]
- Theobald, H.; Luppi, M. Elderly care in changing societies: Concurrences in divergent care regimes—A comparison of Germany, Sweden and Italy. Curr. Sociol. 2018, 66, 629–642. [Google Scholar] [CrossRef]
- Longo, F.; Notarnicola, E. Home care for the elderly in Sweden, Germany and Italy: A case of multi-level governance strategy-making. Soc. Policy Adm. 2018, 52, 1303–1316. [Google Scholar] [CrossRef]
- Rothgang, H.; Gottschall, K.; Safuta, A.; Noack, K.; Seiffarth, M.; Storath, G.-M. Migrantization of long-term care provision in Europe: A Comparative Analysis of Germany, Italy, Sweden, and Poland; SOCIUM SFB 1342 Working Papers; SOCIUM/SFB: Bremen, Germany, 2021. [Google Scholar]
- Bettio, F.; Simonazzi, A.; Villa, P. Change in care regimes and female migration: The ‘care drain’ in the Mediterranean. J. Eur. Soc. Policy 2006, 16, 271–285. [Google Scholar] [CrossRef] [Green Version]
- Costa, G. Long-Term Care Italian Policies: A Case of Inertial Institutional Change. In Reforms in Long-Term Care Policies in Europe: Investigating Institutional Change and Social Impacts; Ranci, C., Pavolini, E., Eds.; Springer: New York, NY, USA, 2013; pp. 221–241. [Google Scholar]
- ISTAT. Gli Anziani e la Loro Domanda Sociale e Sanitaria Anno 2019; Istituto Nazionale di Statistica: Rome, Italy, 2021. [Google Scholar]
- Schulmann, K.; Reichert, M.; Leichsenring, K. Social Support and Long-Term Care for Older People: The Potential for Social Innovation and Active Ageing. In The Future of Ageing in Europe: Making an Asset of Longevity; Walker, A., Ed.; Springer: Singapore, 2019; pp. 255–286. [Google Scholar]
- Fosti, G.; Notarnicola, E. Il Futuro del Settore LTC Prospettive dai Servizi, dai Gestori e Dalle Policy Regionali; Universitá Bocconi: Milan, Italy, 2019. [Google Scholar]
- Salido, M.F.; Moreno-Castro, C.; Belletti, F.; Yghemonos, S.; Ferrer, J.G.; Casanova, G. Innovating European Long-Term Care Policies through the Socio-Economic Support of Families: A Lesson from Practices. Sustainability 2022, 14, 4097. [Google Scholar] [CrossRef]
- Heinze, R.G.; Naegele, G. Social Innovations in Ageing Societies. In Challenge Social Innovation: Potentials for Business, Social Entrepreneurship, Welfare and Civil Society; Franz, H.-W., Hochgerner, J., Howaldt, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 153–167. [Google Scholar]
- OECD. Health at a Glance 2021; OECD: Paris, France, 2021. [Google Scholar]
- Moulaert, F.; MacCallum, D. Advanced Introduction to Social Innovation; Edward Elgar Publishing: Cheltenham, UK, 2019. [Google Scholar]
- Godin, B. Making sense of innovation: From weapon to instrument to buzzword. Quaderni 2016, 90, 21–40. [Google Scholar] [CrossRef]
- Madama, I.; Maino, F.; Razetti, F. Innovating long-term care policy in Italy from the bottom: Confronting the challenge of inclusive local care environments in Lombardy and Piedmont. Investig. Reg.-J. Reg. Res. 2019, 44, 125–141. [Google Scholar]
- Ranci, C.; Pavolini, E. Restructuring the welfare state: Reforms in long-term care in Western European countries. J. Eur. Soc. Policy 2008, 18, 246–259. [Google Scholar] [CrossRef]
- Da Roit, B.; Moreno-Fuentes, F.J. Cash for care and care employment: (Missing) debates and realities. Soc. Policy Adm. 2019, 53, 1–16. [Google Scholar] [CrossRef]
- Hohnerlein, E.M. Long-Term Care Benefits and Services in Italy. In Long-Term Care in Europe: A Juridical Approach; Becker, U., Reinhard, H.-J., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 229–307. [Google Scholar]
- Pelliccia, L.; Guarna, A.R. Percorsi d’innovazione. In L’assistenza Agli Anziani non Autosufficienti in Italia, 7° Rapporto 2020/2021, Punto di non Ritorno; Autosufficienza, N.N., Ed.; Maggioli Editore: Santarcangelo di Romagna, Italy, 2021; pp. 221–240. [Google Scholar]
- Polverini, F.; Lamura, G. Labour supply in care services: National report on Italy. In Report Written for Newidiem (Wales) on behalf of the European Foundation for the Improvement of Living and Working Conditions; INRCA: Ancona, Italy, 2004. [Google Scholar]
- Arlotti, M.; Parma, A.; Ranci, C. Politiche di LTC e disuguaglianze nel caso italiano: Evidenze empiriche e ipotesi di riforma. Politiche Soc. 2020, 1, 125–148. [Google Scholar] [CrossRef]
- Tediosi, F.; Gabriele, S. The Long Term Care System for the Elderly in Italy; ENEPRI: Brussels, Belgium, 2010. [Google Scholar]
- Arlotti, M.; Aguilar-Hendrickson, M. The vicious layering of multilevel governance in Southern Europe: The case of elderly care in Italy and Spain. Soc. Policy Adm. 2017, 52, 646–661. [Google Scholar] [CrossRef]
- Dorigatti, L.; Mori, A.; Neri, S. Public, private or hybrid? Providing care services under austerity: The case of Italy. Int. J. Sociol. Soc. Policy 2020, 40, 1279–1300. [Google Scholar] [CrossRef]
- Da Roit, B.; Le Bihan, B. Cash for long-term care: Policy debates, visions, and designs on the move. Soc. Policy Adm. 2019, 53, 519–536. [Google Scholar] [CrossRef]
- EC. The 2021 Ageing Report: Economic and Budgetary Projections for the EU Member States (2019–2070); European Commission: Brussels, Belgium, 2021. [Google Scholar]
- Gori, C.; Gubert, E. L’indennità di accompagnamento. In L’assistenza Agli Anziani non Autosufficienti in Italia-Punto di non Ritorno; Autosufficienza, N.N., Ed.; Maggioli Editore: Santarcangelo di Romagna, Italy, 2020; Volume 7, pp. 83–100. [Google Scholar]
- Cinelli, G.; Gugiatti, A.; Meda, F. Struttura, attività e performance del SSN. In OASI Report 2021; OASI, Ed.; Centre for Research on Health and Social Care Management (CERGAS): Milan, Italy, 2021; pp. 37–115. [Google Scholar]
- Moulaert, F.; Mehmood, A. Spaces of social innovation. In Handbook of Local and Regional Development; Routledge: London, UK, 2011; pp. 212–225. [Google Scholar]
- Maino, F.; Razetti, F. Long-Term Care e Innovazione Sociale: Riflessioni e Spunti dall’Unione Europea. Available online: https://www.luoghicura.it/sistema/programmazione-e-governance/2019/07/long-term-care-e-innovazione-sociale-riflessioni-e-spunti-dallunione-europea/ (accessed on 22 August 2022).
- Casanova, G.; Principi, A.; Lamura, G. Social Innovation in Long-Term Care: Lessons from the Italian Case. Int. J. Environ. Res. Public Health 2020, 17, 2367. [Google Scholar] [CrossRef]
- Manfredda, F.; Cibinel, E.; Porzio, G. Indagine Propedeutica allo Sviluppo di un Intervento di Sistema sul Territorio Regionale Nell’ambito Dell’assistenza Familiare; POR Piemonte FSE 2014/2020; Regione Piemonte: Turin, Italy, 2017. [Google Scholar]
- Melchiorre, M.G.; Quattrini, S.; Lamura, G.; Socci, M. Role and Characteristics of Personal Care Assistants of Frail Older People with Functional Limitations Ageing in Place in Italy. Int. J. Environ. Res. Public Health 2022, 19, 3969. [Google Scholar] [CrossRef]
- Pasquinelli, S.; Rusmini, G. Le assistenti familiari e il lavoro privato di cura. In L’assistenza agli Anziani non Autosufficienti in Italia, 7° Rapporto 2020/2021-Punto di non Ritorno; Autosufficienza, N.-N.N., Ed.; Maggioli Editore: Santarcangelo di Romagna, Italy, 2021. [Google Scholar]
- De Luca, M.; Tronchin, C.; Di Pasquale, E. Secondo Rapporto Annuale Sul Lavoro Domestico. Analisi, Statistiche, Trend Nazionali e Locali; Osservatorio Nazionale DOMINA Sul Lavoro Domestico: Rome, Italy, 2020. [Google Scholar]
- Seawright, J.; Gerring, J. Case Selection Techniques in Case Study Research: A Menu of Qualitative and Quantitative Options. Political Res. Q. 2008, 61, 294–308. [Google Scholar] [CrossRef]
- De Vita, L.; Corasaniti, A. Regulating domestic and care work in Italy: Assessing the relative influence of the familistic model today. Crit. Soc. Policy 2021, 42, 531–549. [Google Scholar] [CrossRef]
- Seiffarth, M. Potenziale für „gute Arbeit“ im Privathaushalt? Regulierung und Interessenvertretung migrantischer Pflegekräfte in Italien; WSI-Mitteilungen: Düsseldorf, Germany, 2022. [Google Scholar]
- Osservatorio Sociale Regionale. Di Fronte alla Pandemia: Tutele, Difficoltà, vita Quotidiana delle Persone con Disabilità-Quinto Rapporto Sulle Disabilità in Toscana 2020/2021; Regione Toscana: Florence, Italy, 2020. [Google Scholar]
- Safuta, A.; Noack, K.; Gottschall, K.; Rothgang, H. Migrants to the Rescue? Care Workforce Migrantisation on the Example of Elder Care in Germany. In Causal Mechanisms in the Global Development of Social Policies; Kuhlmann, J., Nullmeier, F., Eds.; Palgrave Macmillan: Cham, Switzerland, 2022. [Google Scholar]
- Széman, Z.; Tróbert, A.M. Social Innovation in the Provision of Services in Long-Term Care. Eur. J. Ment. Health 2017, 12, 204–217. [Google Scholar] [CrossRef]
- Kernisan, L. Promises and Pitfalls: Technology and the Future of Delivering Eldercare. J. Am. Soc. Aging 2016, 40, 92–98. [Google Scholar]
- ILO. Making Decent Work a Reality for Domestic Workers: Progress and Prospects Ten Years after the Adoption of the Domestic Workers Convention, 2011 (No. 189); International Labour Office: Geneva, Switzerland, 2021. [Google Scholar]
- D’Alfonso, A. Italy’s National Recovery and Resilience Plan-Latest State of Play; European Parliamentary Research Service: Brussels, Belgium, 2022. [Google Scholar]

{kind=link}
| Type of Stakeholder Interviewed (Number of Experts) | Interview Reference |
|---|---|
| Policymakers and public administration (5) | PA-1(a,b); PA-2(a,b,c) |
| Non-profit organisation staff (4) | NPO-1; NPO-2; NPO-3; NPO-4 |
| Migrants’ association staff (1) | MA * |
| Employers’ association staff (1) | EA * |
| Trade union staff (1) | TU * |
| Employment agency staff (1) | AG * |
| Total: 13 |
| Condition | How Pronto Badante Meets Conditions | |
|---|---|---|
| 1. | Oriented towards exceptional societal challenges/social issues. | Targets emerging LTC needs not publicly provided and addresses informal labour among family assistants. |
| 2. | Suggests new solutions. | Approaches people in need in their own homes and within a short time of the need being identified. |
| 3. | Creates new configurations of social practices/arrangements. | Makes formal employment of MCWs a condition of receiving the benefit. |
| 4. | Overcomes traditional dichotomisation of technological and social innovations. | Integrates both social (via case manager and voucher) and technological assistance (via app). |
| 5. | Promotes integration and collaboration/partnership of heterogeneous stakeholders that usually do not co-operate. | Brings together stakeholders of the public and third sectors who usually do not co-operate. |
| 6. | Consists of integrated patterns of action. | Has a clear operating procedure. |
| 7. | Includes reflective and interdisciplinary approaches. | Carried out by the project’s scientific committee. |
| 8. | Is oriented towards the key goal of societal usefulness. | Delivers services at no cost to beneficiaries and strengthens NPOs. |
| 9. | Creates sustainable measures. | Fails to fulfil this condition; for example, design and funding do not allow for sustainable change. |
| 10. | Creates new growth potentials in terms of regular employment. | Although benefits are conditional on formal employment of MCWs, the project yields only limited results in terms of growth in formal employment. |
| 11. | Involves end-users as co-producers of services and products. | Partially fulfils condition by testing the project’s app with selected participants. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seiffarth, M.; Aureli, G. Social Innovation in Home-Based Eldercare: Strengths and Shortcomings of Integrating Migrant Care Workers into Long-Term Care in Tuscany. Int. J. Environ. Res. Public Health 2022, 19, 10602. https://doi.org/10.3390/ijerph191710602
Seiffarth M, Aureli G. Social Innovation in Home-Based Eldercare: Strengths and Shortcomings of Integrating Migrant Care Workers into Long-Term Care in Tuscany. International Journal of Environmental Research and Public Health. 2022; 19(17):10602. https://doi.org/10.3390/ijerph191710602
Chicago/Turabian StyleSeiffarth, Marlene, and Giulia Aureli. 2022. "Social Innovation in Home-Based Eldercare: Strengths and Shortcomings of Integrating Migrant Care Workers into Long-Term Care in Tuscany" International Journal of Environmental Research and Public Health 19, no. 17: 10602. https://doi.org/10.3390/ijerph191710602
APA StyleSeiffarth, M., & Aureli, G. (2022). Social Innovation in Home-Based Eldercare: Strengths and Shortcomings of Integrating Migrant Care Workers into Long-Term Care in Tuscany. International Journal of Environmental Research and Public Health, 19(17), 10602. https://doi.org/10.3390/ijerph191710602