2. Materials and Methods
2.1. Design
It was a cross-sectional survey study.
2.2. Study Procedures
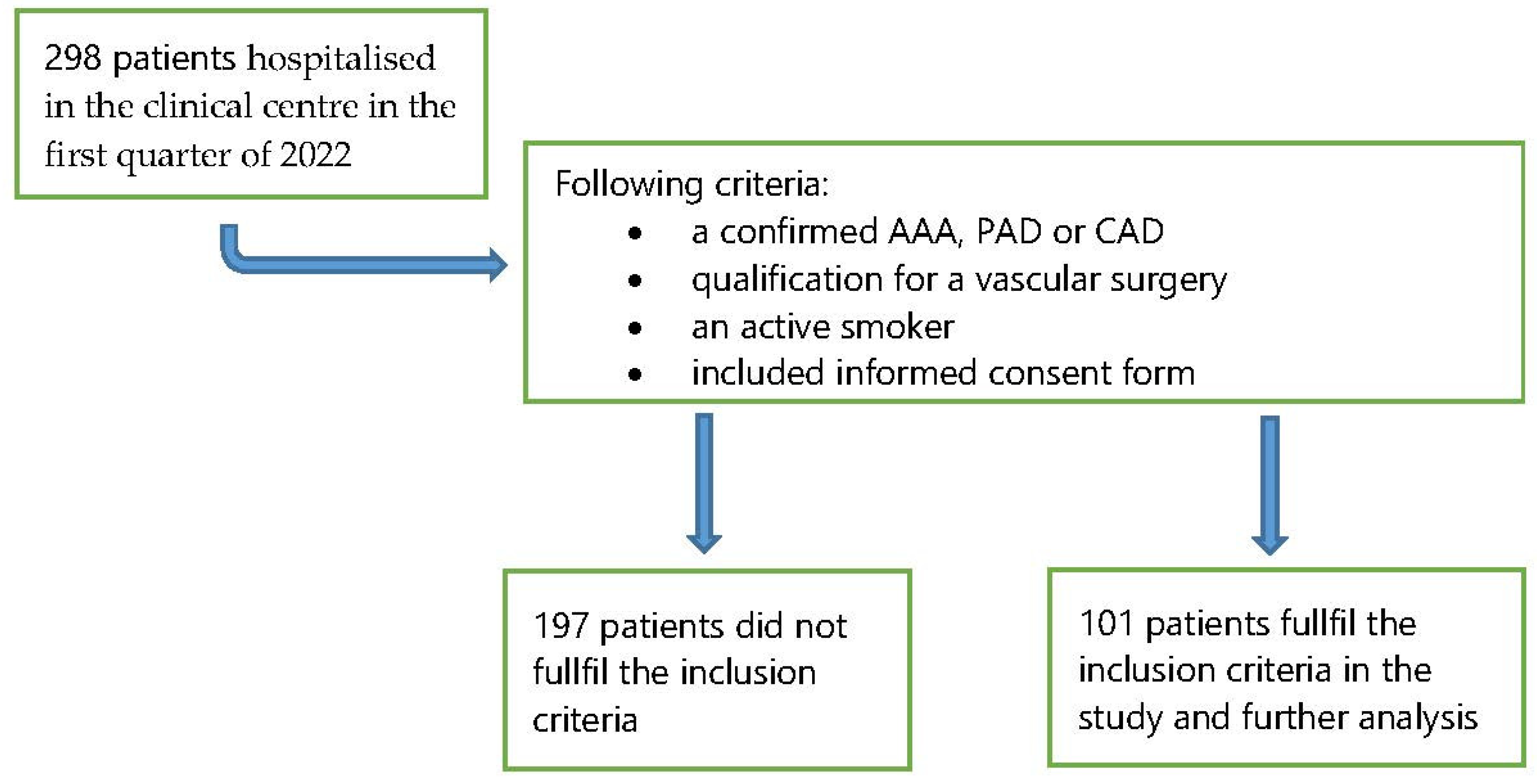
The research was carried out at the Department of Cardiac Surgery and Vascular Surgery of the University Clinical Centre in Gdańsk in 2021. The target group consisted of 101 patients aged 33 to 81 with abdominal aortic aneurysm (AAA), peripheral arterial disease (PAD), carotid artery disease (CAD).
In the prospective research the target group was chosen in accordance with the following criteria:
A confirmed AAA, PAD or CAD;
Qualification for a vascular surgery;
An active smoker;
Included informed consent form.
The data concerning the popularity of smoking were collected in the first quarter of 2022. In that period, there were 298 patients hospitalised in the clinical centre. The analysis included active smokers (
n = 101, 33.9%)—
Figure 1.
All patients received information that in our hospital there is a total ban on smoking, advice encouraging abstinence from smoking, and then patients received nicotine plasters.
2.3. Preparation of the Questionnaire
The diagnostic survey method based on the Fagerström test and Nina Schneider’s test and the original questionnaire were used.
2.3.1. Fagerström Test for Nicotine Dependence (FTND)
A 6-question version of the FTND was applied. The value of score assigned to responses is from 0 to 3 points or from 0 to 1 point. The questions in the test were:
How soon after you wake up do you smoke your first cigarette?
Do you find it difficult to refrain from smoking in places where it is forbidden?
Which cigarette would you hate most to give up?
How many cigarettes per day do you smoke?
Do you smoke more frequently during the first hours after waking than during the rest of the day?
Do you smoke when you are so ill that you are in bed most of the day?
In the Fagerström test, the author assigned the greatest weight to the question concerning the amount of time between waking up in the morning and smoking the first cigarette, as well as the number of cigarettes smoked a day. To assess the degree of addiction, the score of the responses must be summed up. The greater the score in the FTND test, the more intensive nicotine dependence of the patient. Classification of dependence: 0–3 low, 4–6 medium, 7–10 high [
15,
16,
17].
2.3.2. Test of Motivation for Ceasing Smoking by Nina Schneider
The test measuring motivation for ceasing smoking prepared by the University in Los Angeles and used to test the patient’s readiness to cease smoking. The more positive responses, the greatest readiness to cease smoking. In the questionnaire, each response “yes” or “no” is scored individually. “No” means 0 points and “yes” means 1 point. To obtain the result, all scores must be summed up. The maximum possible score is 12. The motivation is considered low if the test result is below 7 points and high if the score equals or is greater than 7 points [
18,
19].
2.3.3. Original Questionnaire
The questionnaire let us collect social and demographic data, such as sex, age, education level, place of residence, marital status, professional activeness. Further questions included the history of smoking: the initiation of nicotine addiction, the time of smoking, the number of cigarettes, attempts of ceasing smoking.
The clinical diagnosis, the type of a planned vascular surgery, and co-existing diseases were defined on the basis of the patient’s medical history.
2.4. Statistical Analysis
All statistical calculations were carried out using the IBM SPSS 23 statistical package and an Excel 2016 spreadsheet. Qualitative variables were presented as numbers and percentages, while quantitative variables were characterized using mean and standard deviation or median, upper and lower quartile. All variables were tested for normal distribution by the Shapiro-Wilk test. The significance of any differences between more than two groups was verified using the Kruskal–Wallis non-parametric significance test and the significance of differences between two groups, by using the Mann–Whitney. Spearman correlation test was used to verify the existence and power of the relationship between the variables. In all calculations, p < 0.05 was assumed as the level of significance.
2.5. Ethical Considerations
While collecting the data, the ethical principles set out in the Helsinki Declaration were taken into account. The research was approved by the Independent Bioethical Committee at the Medical University of Gdańsk, number NKBBN/124/2020.
4. Discussion
In Poland, there are limited data concerning smoking by patients with peripheral arterial disease (PAD), abdominal aortic aneurysms (AAA), and carotid artery disease (CAD), which would involve the level of nicotine dependence and motivation for ceasing smoking. Therefore, the authors designed a pilot survey, which allows for the assessment of that problem. The researchers proved that smoking is strictly correlated with the development of vascular diseases, including peripheral arterial disease (PAD), abdominal aortic aneurysms (AAA), and carotid artery disease (CAD) [
5,
6,
20]. In addition, smoking contributes to the progression of vascular diseases [
19]. Based on the existing guidelines, all patients to undergo vascular surgeries are recommended to cease smoking [
20]. The results of the survey confirm a 40% relative reduction in the risk of all complications if the patient ceases smoking before the surgery [
21].
The analysis of the authors’ survey confirmed that 33.9% of the patients were active smokers before the surgery. Over 70% of them declared that they were willing to cease smoking after the vascular surgery, usually within one week of the end of their hospitalisation. The survey performed by Assadian et al. also confirmed that a significant percentage of patients to undergo vascular surgeries are smokers. In addition, half of them still smoked in the hospital, where smoking is forbidden by law [
22]. The survey performed by Sztuczka et al. indicated that in the group of PAD patients who were originally qualified for the survey, 91.4% of the respondents declared themselves to be addicted smokers. The results of the survey confirmed that the level of motivation for ceasing smoking was not dependent on the clinical progress of the disease. This means that the smokers who were to undergo a bypass surgery, due to the 3rd or 4th degree ischaemia of lower limbs, are less inclined to look for professional help and cease smoking [
18]. The survey conducted in the Canadian centre confirmed that 33.5% of the respondents were smokers during the perioperative period. After the yearly observation of the patients who smoked before the surgery, 41.6% ceased smoking and 58.4% did not do that [
23].
The analysis of the survey hereunder did not confirm the impact of social and demographic factors, such as sex, age, education level, on the level of nicotine dependence and motivation for ceasing smoking. The survey conducted by the Canadian centre confirmed that male patients smoked before the surgery more frequently. The sex was also statistically related with the higher ratios of ceasing smoking among women [
23]. Ponczek et al. confirmed the impact of social and demographic factors on the level of motivation for ceasing smoking. The authors of that survey conclude that the higher education level, the greater readiness to cease smoking. In addition, that survey confirmed that the degree of nicotine dependence among the respondents with vocational education was greater [
24].
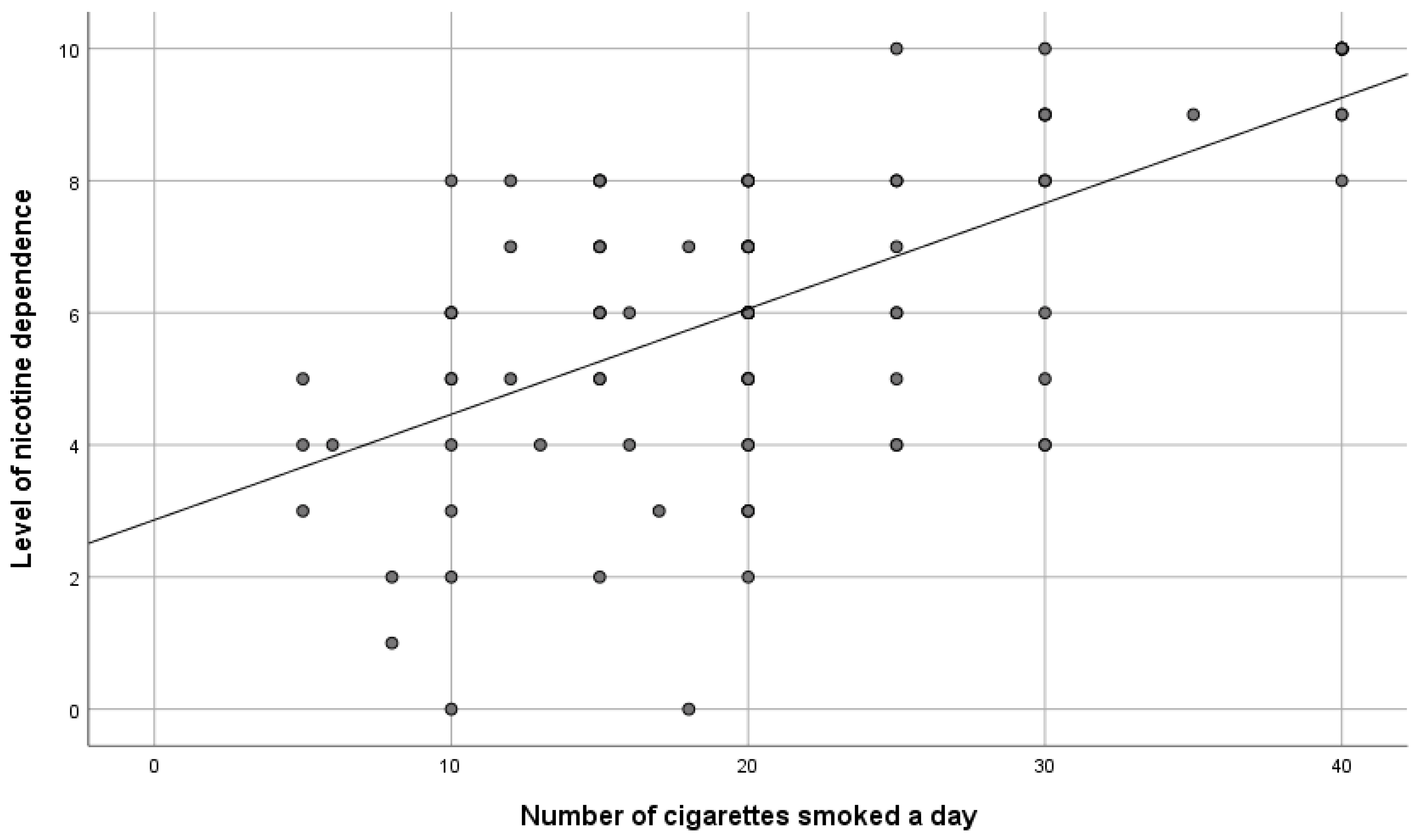
The survey conducted by Smeds et al. indicated that 22% of the patients were active smokers before the vascular surgery. The smokers that smoked less than 10 cigarettes a day were less nicotine dependent (
p = 0.0001) and more inclined to consider ceasing smoking [
25]. The survey hereunder also confirmed that the greater the number of cigarettes smoked a day, the higher the level of nicotine dependence and the lower the motivation for ceasing smoking. In the survey conducted by Walewska et al., it was also confirmed that nicotine dependence increases together with the growth of stress, as a result of which the patient smokes a cigarette and the level of motivation for ceasing smoking decreases [
26].
The surveys prove that nicotine is the major—however, not the only—reason for the development of chronic obstructive pulmonary disease (COPD) [
27,
28,
29,
30] and there seems to be a genetic predisposition, which increases the risk in the case of certain patients [
31]. COPD develops in the case of 10–20% of smokers [
32,
33,
34]. In our surveys, the respondents with a greater number of years of smoking were confirmed to be diagnosed with COPD much more often.
To obtain better results, a special attention should be paid to motivating the patient adequately to attempt to cease smoking and refrain from smoking as long as possible. It must be noted that motivation is a dynamic process and can be strengthened or maintained potentially in the case of each patient [
22,
35]. Our own data indicate that a significant number of patients keep on smoking despite their diagnosis. As ceasing smoking is desirable, all patients should be encouraged to do it [
2,
36].
5. Limitations
Our study has several limitations. The overall sample size was small, so the results of the study cannot be generalized. Additionally, the level of addiction and the motivation to quit smoking may be influenced by other factors that we did not take into account. We believe that the next test should take into account factors, such as financial considerations, free time, stress, and having loved ones who smoke.
In another test, the competence of vascular surgeons and vascular nurses in the area of counseling and smoking cessation treatment should be assessed. This will enable the development of training programs for doctors and nurses in the effective implementation of the diagnostic protocol and the treatment of nicotine addiction.
Despite the limitations, the results of these studies show the magnitude of the problem of nicotine addiction in patients with vascular diseases and can be used to design and implement smoking cessation programs.


 ,
, 


{kind=link}
{kind=link}
{kind=link}