
Disability and Participation in Breast and Cervical Cancer Screening: A Systematic Review and Meta-Analysis

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Defining Disability
2.2. Outcome
2.3. Data Sources and Search Terms
2.4. Inclusion Criteria
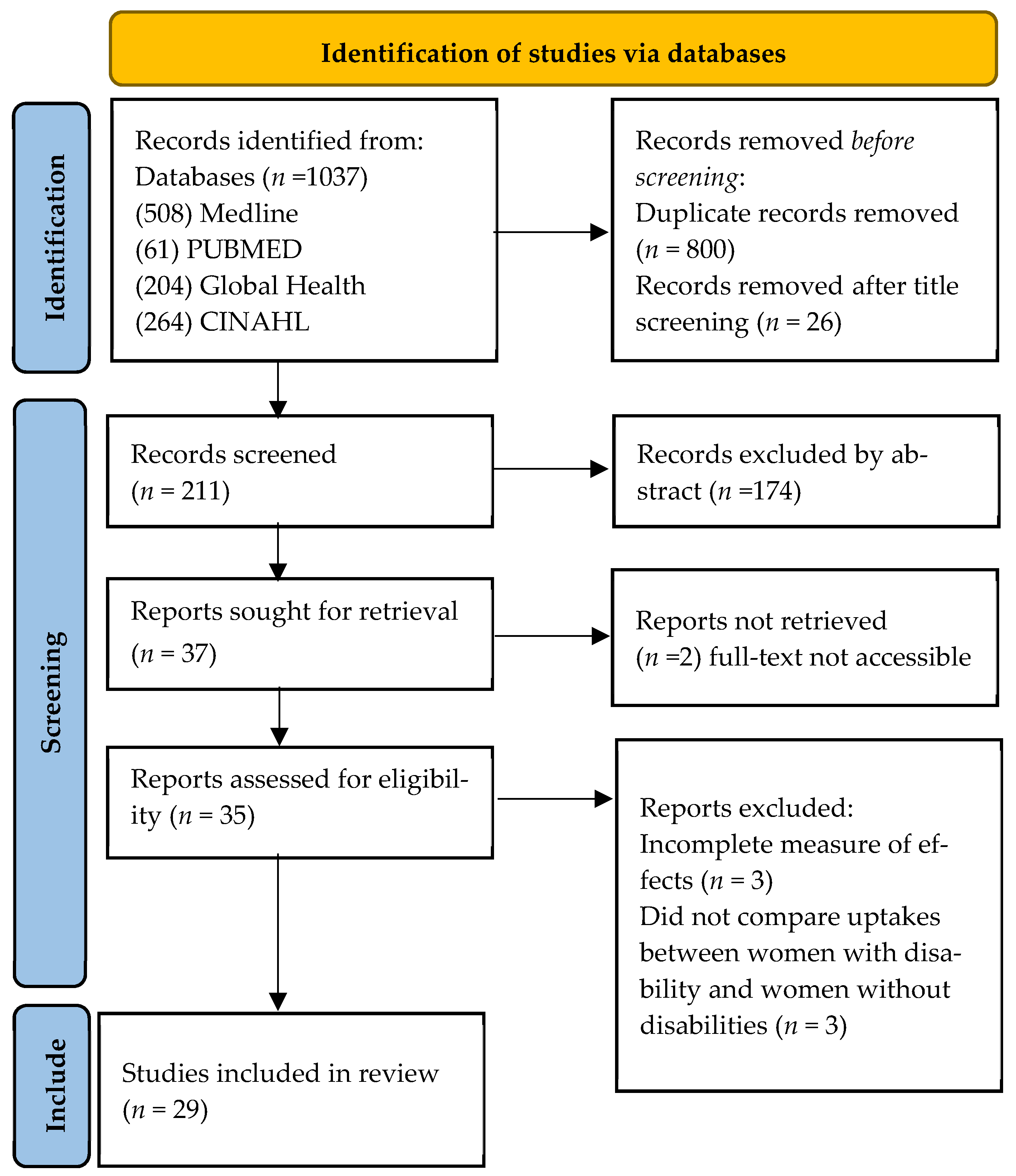
2.5. Study Selection
2.6. Data Extraction
2.7. Risk of Bias Assessment
2.8. Data Synthesis and Meta-Analysis
3. Results
3.1. Study Characteristics
3.1.1. Study Design
3.1.2. Types of Disabilities
3.1.3. Outcome Measurement
3.1.4. Risk of Bias
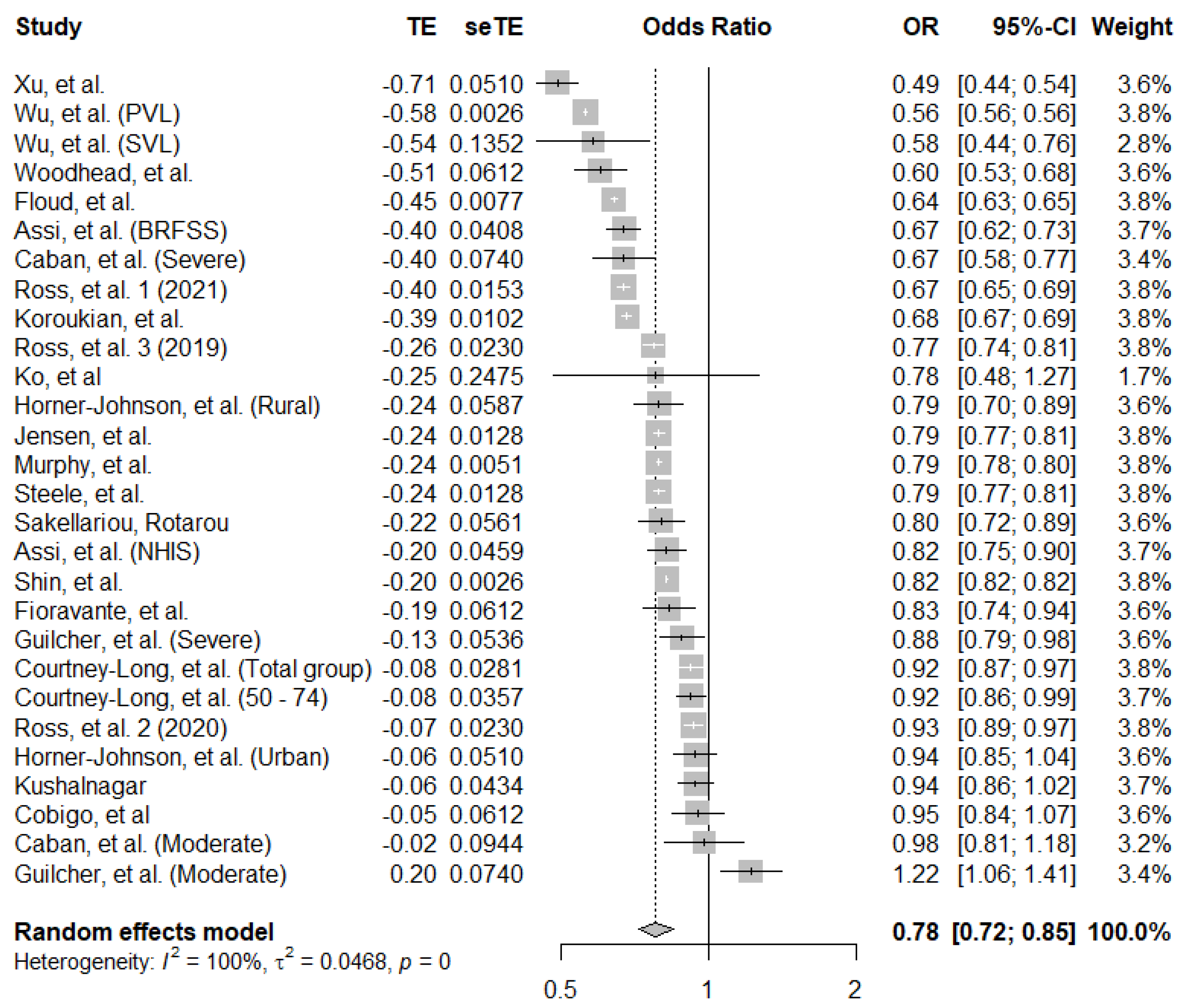
3.1.5. Breast Cancer Screening Uptake in Women with Disability
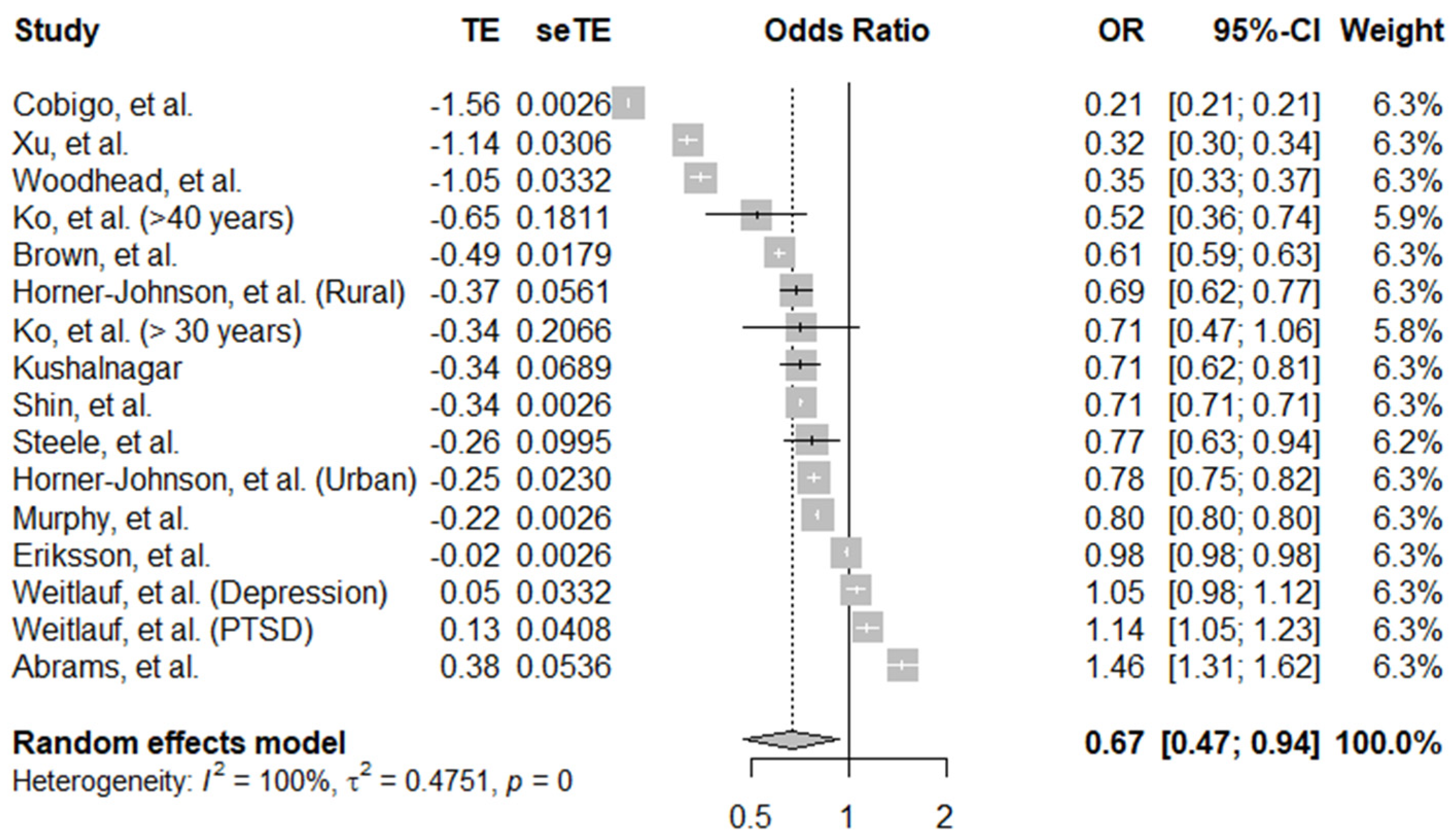
3.1.6. Cervical Cancer Screening
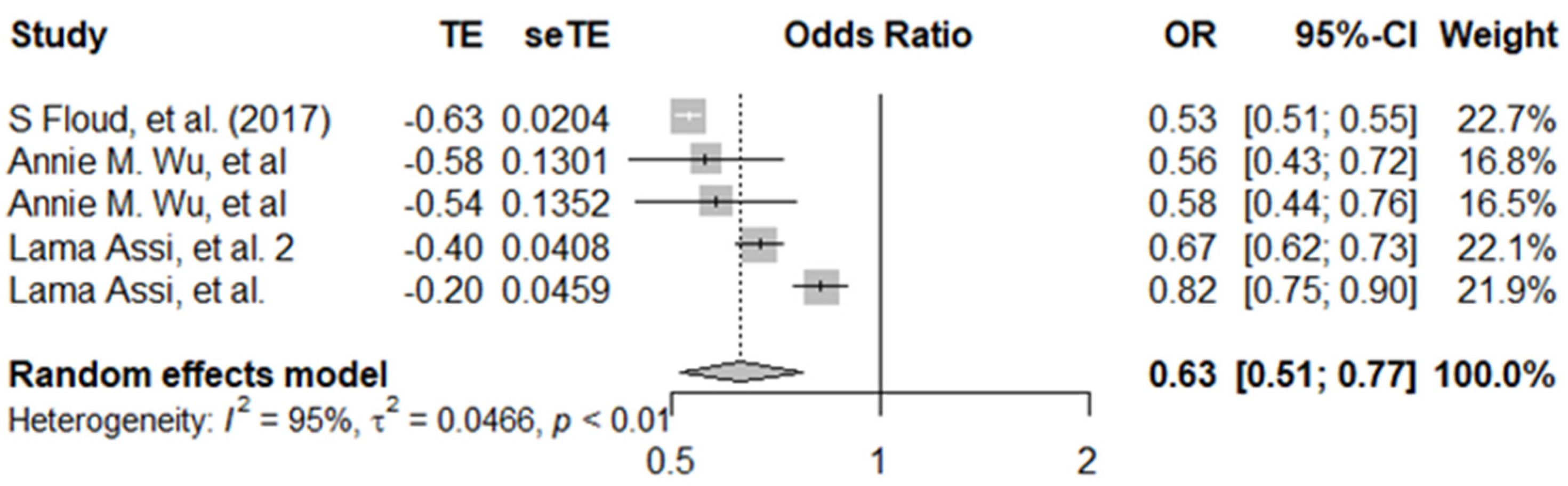
3.2. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Jansen, E.E.L.; Zielonke, N.; Gini, A.; Anttila, A.; Segnan, N.; Vokó, Z.; Ivanuš, U.; McKee, M.; de Koning, H.J.; de Kok, I.M.C.M.; et al. Effect of organised cervical cancer screening on cervical cancer mortality in Europe: A systematic review. Eur. J. Cancer 2020, 127, 207–223. [Google Scholar] [CrossRef]
- Nelson, H.D.; Fu, R.; Cantor, A.; Pappas, M.; Daeges, M.; Humphrey, L. Effectiveness of Breast Cancer Screening: Systematic Review and Meta-analysis to Update the 2009 U.S. Preventive Services Task Force Recommendation. Ann. Intern. Med. 2016, 164, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Damiani, G.; Federico, B.; Basso, D.; Ronconi, A.; Bianchi, C.B.N.A.; Anzellotti, G.M.; Nasi, G.; Sassi, F.; Ricciardi, W. Socioeconomic disparities in the uptake of breast and cervical cancer screening in Italy: A cross sectional study. BMC Public Health 2012, 12, 99. [Google Scholar] [CrossRef] [PubMed]
- Cancer Research UK Cancer Target Missed for 55,000 Patients over 6 Years 2021. Available online: https://news.cancerresearchuk.org/2021/09/22/cancer-target-missed-for-55000-patients-over-six-years/ (accessed on 15 July 2021).
- Ross, E.; Maguire, A.; Donnelly, M.; Mairs, A.; Hall, C.; O’Reilly, D. Disability as a predictor of breast cancer screening uptake: A population-based study of 57,328 women. J. Med. Screen. 2019, 27, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Casebolt, M.T. Barriers to reproductive health services for women with disability in low- and middle-income countries: A review of the literature. Sex. Reprod. Healthc. 2020, 24, 100485. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.N.S.; Law, B.M.H.; Au, D.W.H.; So, W.K.W.; Fan, N. A systematic review of the barriers and facilitators influencing the cancer screening behaviour among people with intellectual disabilities. Cancer Epidemiol. 2022, 76, 102084. [Google Scholar] [CrossRef] [PubMed]
- Floud, S.; Barnes, I.; Verfürden, M.; Kuper, H.; Gathani, T.; Blanks, R.G.; Alison, R.; Patnick, J.; Beral, V.; Green, J.; et al. Disability and participation in breast and bowel cancer screening in England: A large prospective study. Br. J. Cancer 2017, 117, 1711–1714. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.W.; Lee, J.-W.; Jung, J.H.; Han, K.; Kim, S.Y.; Choi, K.S.; Park, J.H.; Park, J.H. Disparities in Cervical Cancer Screening Among Women With Disabilities: A National Database Study in South Korea. J. Clin. Oncol. 2018, 36, 2778–2786. [Google Scholar] [CrossRef]
- Kuper, H.; Heydt, P. The Missing Billion Report. 2019. Available online: https://www.lshtm.ac.uk/media/38726 (accessed on 16 July 2021).
- Office for Disability Issues UK. Disability Facts and Figures. 2021. Available online: https://www.gov.uk/government/statistics/disability-facts-and-figures/disability-facts-and-figures (accessed on 16 July 2021).
- Andresen, E.M.; Peterson-Besse, J.J.; Krahn, G.L.; Walsh, E.S.; Horner-Johnson, W.; Iezzoni, L.I. Pap, Mammography, and Clinical Breast Examination Screening Among Women with Disabilities: A Systematic Review. Women’s Health Issues 2013, 23, e205–e214. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021, 156, 787–788. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001; Available online: https://apps.who.int/iris/handle/10665/42407 (accessed on 26 July 2021).
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Checklist for Cohort Studies. Joanna Briggs Inst. Rev. Man. 2017, 1–7. Available online: https://joannabriggs.org/ebp/critical_appraisal_tools (accessed on 26 July 2021).
- RStuio Team No Title 2020. Available online: http://www.rstudio.com/ (accessed on 30 July 2021).
- Steele, C.B.; Townsend, J.S.; Courtney-Long, E.A.; Young, M. Prevalence of Cancer Screening Among Adults With Disabilities, United States, 2013. Prev. Chronic Dis. 2017, 14, E09. [Google Scholar] [CrossRef]
- Sakellariou, D.; Rotarou, E.S. Utilisation of mammography by women with mobility impairment in the UK: Secondary analysis of cross-sectional data. BMJ Open 2019, 9, e024571. [Google Scholar] [CrossRef]
- Fioravante, N.; Deal, J.A.; Willink, A.; Myers, C.; Assi, L. Preventive Care Utilization among Adults with Hearing Loss in the United States. Semin. Hear. 2021, 42, 37–46. [Google Scholar] [CrossRef]
- Ko, K.D.; Lee, K.Y.; Cho, B.; Park, M.S.; Son, K.Y.; Ha, J.H.; Park, S.M. Disparities in health-risk behaviors, preventive health care utilizations, and chronic health conditions for people with disabilities: The Korean National Health and Nutrition Examination Survey. Arch. Phys. Med. Rehabil. 2011, 92, 1230–1237. [Google Scholar] [CrossRef]
- Assi, L.; Varadaraj, V.; Shakarchi, A.F.; Sheehan, O.C.; Reed, N.S.; Ehrlich, J.R.; Swenor, B.K. Association of Vision Impairment With Preventive Care Use Among Older Adults in the United States. JAMA Ophthalmol. 2020, 138, 1298–1306. [Google Scholar] [CrossRef]
- Abrams, M.T.; Myers, C.S.; Feldman, S.M.; Boddie-Willis, C.; Park, J.; McMahon, R.P.; Kelly, D.L. Cervical cancer screening and acute care visits among Medicaid enrollees with mental and substance use disorders. Psychiatr. Serv. 2012, 63, 815–822. [Google Scholar] [CrossRef]
- Osborn, D.P.J.; Horsfall, L.; Hassiotis, A.; Petersen, I.; Walters, K.; Nazareth, I. Access to Cancer Screening in People with Learning Disabilities in the UK: Cohort Study in the Health Improvement Network, a Primary Care Research Database. PLoS ONE 2012, 7, e43841. [Google Scholar] [CrossRef]
- Woodhead, C.; Cunningham, R.; Ashworth, M.; Barley, E.; Stewart, R.J.; Henderson, M.J. Cervical and breast cancer screening uptake among women with serious mental illness: A data linkage study. BMC Cancer 2016, 16, 819. [Google Scholar] [CrossRef]
- Ross, E.; Maguire, A.; Mairs, A.; Hall, C.; Donnelly, M.J.C.; O’Reilly, D.P.J. Disparities in Breast Cancer Screening Uptake for Women With Mental Illness in the United Kingdom. Am. J. Prev. Med. 2021, 60, e123–e130. [Google Scholar] [CrossRef]
- Emma, R.; Aideen, M.; Michael, D.; Adrian, M.; Clare, H.; Dermot, O. Does poor mental health explain socio-demographic gradients in breast cancer screening uptake? A population-based study. Eur. J. Public Health 2020, 30, 538–543. [Google Scholar] [CrossRef]
- Eriksson, E.M.; Lau, M.; Jonsson, C.; Zhang, C.; Riso Bergerlind, L.-L.; Jonasson, J.M.; Strander, B. Participation in a Swedish cervical cancer screening program among women with psychiatric diagnoses: A population-based cohort study. BMC Public Health 2019, 19, 313. [Google Scholar] [CrossRef]
- Brown, H.K.; Plourde, N.; Ouellette-Kuntz, H.; Vigod, S.; Cobigo, V. Brief report: Cervical cancer screening in women with intellectual and developmental disabilities who have had a pregnancy. J. Intellect. Disabil. Res. 2016, 60, 22–27. [Google Scholar] [CrossRef]
- Weitlauf, J.C.; Jones, S.; Xu, X.; Finney, J.W.; Moos, R.H.; Sawaya, G.F.; Frayne, S.M. Receipt of cervical cancer screening in female veterans: Impact of posttraumatic stress disorder and depression. Womens. Health Issues 2013, 23, e153–e159. [Google Scholar] [CrossRef][Green Version]
- Tuesley, K.M.; Jordan, S.J.; Siskind, D.J.; Kendall, B.J.; Kisely, S. Colorectal, cervical and prostate cancer screening in Australians with severe mental illness: Retrospective nation-wide cohort study. Aust. N. Z. J. Psychiatry 2019, 53, 550–558. [Google Scholar] [CrossRef]
- Jensen, L.F.; Pedersen, A.F.; Bech, B.H.; Andersen, B.; Vedsted, P. Psychiatric morbidity and non-participation in breast cancer screening. Breast 2016, 25, 38–44. [Google Scholar] [CrossRef]
- Murphy, K.A.; Stone, E.M.; Presskreischer, R.; McGinty, E.E.; Daumit, G.L.; Pollack, C.E. Cancer Screening Among Adults With and Without Serious Mental Illness: A Mixed Methods Study. Med. Care 2021, 59, 327–333. [Google Scholar] [CrossRef]
- Koroukian, S.M.; Bakaki, P.M.; Golchin, N.; Tyler, C.; Loue, S. Mental illness and use of screening mammography among Medicaid beneficiaries. Am. J. Prev. Med. 2012, 42, 606–609. [Google Scholar] [CrossRef] [PubMed]
- Cobigo, V.; Ouellette-Kuntz, H.; Balogh, R.; Leung, F.; Lin, E.; Lunsky, Y. Are cervical and breast cancer screening programmes equitable? The case of women with intellectual and developmental disabilities. J. Intellect. Disabil. Res. 2013, 57, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Horner-Johnson, W.; Dobbertin, K.; Iezzoni, L.I. Disparities in receipt of breast and cervical cancer screening for rural women age 18 to 64 with disabilities. Womens Health Issues 2015, 25, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Kushalnagar, P.; Engelman, A.; Simons, A.N. Deaf Women’s Health: Adherence to Breast and Cervical Cancer Screening Recommendations. Am. J. Prev. Med. 2019, 57, 346–354. [Google Scholar] [CrossRef] [PubMed]
- XinLing, X.; McDermott, S.W.; Mann, J.R.; Hardin, J.W.; Deroche, C.B.; Carroll, D.D.; Courtney-Long, E.A. A longitudinal assessment of adherence to breast and cervical cancer screening recommendations among women with and without intellectual disability. Prev. Med. 2017, 100, 167–172. [Google Scholar] [CrossRef]
- Caban, M.; Kuo, Y.F.; Raji, M.; Tan, A.; Freeman, J. Predictors of mammography use in older women with disability: The patients’ perspectives. Med. Oncol. 2011, 28 (Suppl. S1), S8–S14. [Google Scholar] [CrossRef]
- Courtney-Long, E.; Armour, B.; Frammartino, B.; Miller, J. Factors associated with self-reported mammography use for women with and women without a disability. J. Womens Health 2011, 20, 1279–1286. [Google Scholar] [CrossRef]
- Guilcher, S.J.T.; Lofters, A.; Glazier, R.H.; Jaglal, S.B.; Voth, J.; Bayoumi, A.M. Level of disability, multi-morbidity and breast cancer screening: Does severity matter? Prev. Med. 2014, 67, 193–198. [Google Scholar] [CrossRef]
- DongWook, S.; Jonghan, Y.; Juhee, C.; SeKyung, L.; JinHyung, J.; Kyungdo, H.; SoYoung, K.; Yoo, J.E.; KyoungEun, Y.; YeonYong, K.; et al. Breast cancer screening disparities between women with and without disabilities: A national database study in South Korea. Cancer 2020, 126, 1522–1529. [Google Scholar] [CrossRef]
- Wu, A.M.; Morse, A.R.; Seiple, W.H.; Talwar, N.; Hansen, S.O.; Lee, P.P.; Stein, J.D. Reduced Mammography Screening for Breast Cancer among Women with Visual Impairment. Ophthalmology 2021, 128, 317–323. [Google Scholar] [CrossRef]
- XinLing, X.; Mann, J.R.; McDermott, S.W.; Deroche, C.B.; Gustafson, E.; Hardin, J.W. Women with visual impairment and insured by Medicaid or Medicare are less likely to receive recommended screening for breast and cervical cancers. Ophthalmic Epidemiol. 2017, 24, 168–173. [Google Scholar] [CrossRef]
- Ramjan, L.; Cotton, A.; Algoso, M.; Peters, K. Barriers to breast and cervical cancer screening for women with physical disability: A review. Women Health 2016, 56, 141–156. [Google Scholar] [CrossRef]
- Kilic, A.; Tastan, S.; Guvenc, G.; Akyuz, A. Breast and cervical cancer screening for women with physical disabilities: A qualitative study of experiences and barriers...First International Congress of Nursing (Icon-2017), 16–18 March 2017, Grand Park Lara Convention Center, Lara-Antalya, Turkey. J. Adv. Nurs. 2019, 75, 1976–1986. [Google Scholar] [CrossRef]
- Merten, J.W.; Pomeranz, J.L.; King, J.L.; Moorhouse, M.; Wynn, R.D. Barriers to cancer screening for people with disabilities: A literature review. Disabil. Health J. 2015, 8, 9–16. [Google Scholar] [CrossRef]
- Liao, C.-M.; Huang, W.-H.; Kung, P.-T.; Chiu, L.-T.; Tsai, W.-C. Comparison of colorectal cancer screening between people with and without disability: A nationwide matched cohort study. BMC Public Health 2021, 21, 1034. [Google Scholar] [CrossRef]
- Shin, D.W.; Chang, D.; Jung, J.H.; Han, K.; Kim, S.Y.; Choi, K.S.; Lee, W.C.; Park, J.H.; Park, J.H. Disparities in the Participation Rate of Colorectal Cancer Screening by Fecal Occult Blood Test among People with Disabilities: A National Database Study in South Korea. Cancer Res. Treat. 2020, 52, 60–73. [Google Scholar] [CrossRef]
- UN. Realization of the sustainable development goals by, for and with persons with disabilities. Dep. Econ. Soc. Aff. 2018, 390. Available online: https://www.un.org/development/desa/disabilities/wp-content/uploads/sites/15/2018/12/UN-Flagship-Report-Disability.pdf (accessed on 10 July 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study Location | Study Design | Type of Disability | Definition of Disability | Type of Screening | Participants | Age Range (Years) | Follow up Time | |
|---|---|---|---|---|---|---|---|---|---|
| With Disability | Without Disability | ||||||||
| Cobigo et al. (2013) [36] | Canada | Cohort | Learning | Intellectual developmental disabilities based on the ICD-10. | Both | 17,777 | 1,440,962 | 20–69 | Breast: 2 years, Cervix: 3 years |
| Horner-Johnson et al. (2015) [37] | USA | Cohort | Functional | Presence of limitations in basic actions involving physical functions, vision, hearing, or cognition. | Both | 10,985 (urban), 3108 (rural) | 42,834 (urban), 8579 (rural) | Breast: 40–64, Cervix: 18–64 | 6 years |
| Ko et al. (2011) [22] | South Korea | Cross-sectional | Physical and psychosocial. | ICF: Physical, internal organ, and mental. | Both | 23,511 | 11,660 | 42–69 | 2 years |
| Kushalnagar. (2019) [38] | USA | Cross-sectional | Hearing | Functional hearing impairment. | Both | Breast: 324 Cervix: 529 | Breast: 1086 Cervix: 1119 | Breast: 40–74 Cervix: 21–65 | n/a |
| Murphy et al. (2021) [34] | USA | Mixed methods, retrospective for quantitative; and qualitative. | Psychosocial | Serious mental illness (SMI): schizophrenia, bipolar depression, major depression. | Both | Breast 94,921 Cervix 274,643 | Breast: 11,955,674 Cervix: 31,949,537 | 21–64 | 7 years |
| Osborn et al. (2012) [25] | UK | Cohort | Learning | General terms and related terms (e.g., autism, down syndrome, and Fragile X syndrome). | Both | Breast: 2956 Cervix: 6254 | 50,779 | Breast: 50–64 Cervix: 20–65 | 10 years |
| Steele et al. (2017) [19] | USA | Cross-sectional | Physical and functional. | Self-report of disability. | Both | 2580 | 12,499 | 21–75 | n/a |
| Woodhead et al. (2016) [26] | UK | Cross-sectional | Psychosocial | Serious mental illness based on ICD-10 diagnosis. | Both | Breast: 625, Cervix: 1393 | Breast: 25,385, Cervix: 106,554 | Breast: 50–70, Cervix: 25–64 | n/a |
| Xu et al. (2017) [39] | USA | Cohort | Visual | Clinical diagnosis of visual impairment. | Both | Breast: 1308, Cervix: 1247 | Breast: 2635, Cervix: 2483 | Breast: 40–74, Cervix: 20–74 | 11 years |
| Assi et al. (2020) [23] | USA | Cross-sectional | Visual | Self-reported visual impairments. | Breast | 1915 | 10,205 | 50–74 | n/a |
| Caban et al. (2011) [40] | USA | Cohort | Functional and psychosocial. | Reported functional limitations of activity of daily living (ADL) and instrumental activities of daily living (IADL). | Breast | 2281 | 2329 | >65 | 2 years |
| Courtney-Long et al. (2011) [41] | USA | Cross-sectional | Physical and functional. | Self-report of disability. | Breast | 64,905 | 130,394 | 40–74 | 2 years |
| Fioravante et al. (2021) [21] | USA | Cross-sectional | Hearing | Functional hearing loss. | Breast | 2123 | 10,067 | 50–74 | n/a |
| Floud et al. (2017) [9] | UK | Cohort | Functional (including psychological) and physical. | Self-report of disability. | Breast | 109,869 | 363,316 | 50–70 | 5 years |
| Guilcher et al. (2014) [42] | Canada | Cohort | Physical and functional. | Morbidity: presence of limiting disease, e.g., arthritis, hypertension. | Breast | 4660 | 5703 | 50–69 | 2 years |
| Jensen et al. (2016) [33] | Denmark | Cohort | Psychosocial | Schizophrenia, affective disorders, eating disorder. | Breast | 47,648 | 96,616 | 50–69 | Up to 10 years |
| Ross et al. (2020) [6] | Northern Ireland | Cohort | Physical and psychosocial. | Self-report of disability. | Breast | 20,541 | 36,787 | 48–70 | 1 year |
| Ross et al. (2020) [28] | Northern Ireland | Cohort | Psychosocial | Chronic poor mental health. | Breast | 6162 | 51,166 | 50–70 | 4 years |
| Ross et al. (2021) [27] | Northern Ireland | Cohort | Psychosocial | Record of psychotropic prescription. | Breast | 17,521 | 39,807 | 50–70 | 3 years |
| Sakellariou and Rotarou. (2019) [20] | UK | Cross-sectional | Physical | Lower limb impairment. | Breast | 2697 | 6794 | 20–70+ | n/a |
| Shin et al. (2020) [43] | South Korea | Cohort | Physical and psychosocial. | Diagnosis of disability by healthcare professional. | Breast | 419,376 | 5,864,247 | >40 | 10 years |
| Koroukian et al. (2012) [35] | USA | Cohort | Psychosocial | Morbidity: presence of limiting disease, e.g., arthritis, hypertension. | Breast | 61,661 | 68,427 | 50–64 | n/a |
| Wu et al. (2021) [44] | USA | Cohort | Visual | Partial vision loss (PVL) and severe vision loss (SVL). | Breast | PVL: 348, SVL: 348 | 348 | 65–72 | 5 years |
| Abrams et al. (2012) [24] | USA | Cohort | Psychosocial | Psychosis (schizophrenia), substance use disorder, bipolar disorder, or mania. | Cervical | 20,306 | 85,375 | 19–64 | 1 year |
| Brown et al. (2016) [30] | Canada | Cohort | Intellectual and developmental. | Clinical diagnosis of intellectual and developmental disabilities. | Cervical | 5033 | 527,437 | 20–64 | n/a |
| Eriksson et al. (2019) [29] | Sweden | Cohort | Psychosocial | Psychiatric diagnosis. | Cervical | 65,292 | 341,171 | 23–60 | 5 years |
| Shin et al. (2018) [10] | South Korea | Cohort | Physical and functional. | Diagnosis of disability by healthcare professional. | Cervical | 426,189 | 7,376,529 | >50 | 10 years |
| Tuesley et al. (2019) [32] | Australia | Cohort | Psychosocial | Classified as serious mental illnesses, based on prescriptions in the last 12 months. | Cervical | 18,363 | 899,777 | 18–69 | 10 years |
| Weitlauf et al. (2013) [31] | USA | Cohort | Psychosocial | PTSD and depression based on clinical diagnosis ICD 9. | Cervical | 17,295 | 16,828 | 18–65 | 1 year |
| Author | Outcome Definition | Assessment Method | Uptake (%) | Unadjusted OR | aOR (95% CI) | Risk of Bias Rating | |
|---|---|---|---|---|---|---|---|
| Women with Disabilities | Women without Disabilities | ||||||
| Assi et al. [23] | Receipt of mammography in the past 2 years. | Self-report | (−5.02%) difference in proportions | BRFSS: 0.63 (0.56–0.70) | 0.67 (0.59–0.75) | High | |
| NHIS: 0.78 (0.68–0.89) | 0.82 (0.71–0.89) | ||||||
| Caban et al. [40] | Receipt of mammography in the past 1 year of the study period. | Self-report | n/a | n/a | Moderate disability: 0.76 (0.64–0.91) | 0.98 (0.81–1.18) | Low |
| Severe disability: 0.46 (0.40–0.54) | 0.67 (0.54–0.83) | ||||||
| Cobigo et al. [36] | Receipt of mammography in the past 2 years. | Clinical record (Insurance code) | 42% | 60% | 0.47 (0.45–0.50) | 0.95 (0.84–1.08) | Low |
| Courtney-Long et al. [41] | Receipt of mammogram within the past 2 years. | Self-report | Total group: 72% | 78% | n/a | 0.92 (0.87–0.98) | High |
| Aged 50–74: 78% | 83% | n/a | 0.92 (0.85–0.99) | ||||
| Fioravante et al. [21] | Receipt of mammogram within past two years. | Self-report | n/a | n/a | 0.84 (0.73–0.96) | 0.83 (0.72–0.96) | High |
| Floud et al. [9] | Clinical registration of breast cancer screening in the past 3 years. | Clinical record | 83% | 89% | n/a | 0.64 (0.62–0.65) | Low |
| Guilcher, et al. [42] | Receipt of mammography within two years. | Clinical record | Moderate disability: 67% | 68% | n/a | 1.22 (1.09–1.38) | Low |
| Severe disability: 67% | 68% | n/a | 0.88 (0.78–0.99) | ||||
| Horner-Johnson et al. [37] | Receipt of mammography within two years. | Clinical record | Rural: 67% | 70% | 0.63 (0.56–0.72) | 0.79 (0.68–0.91) | Low |
| Urban: 73% | 76% | 0.85 (0.77–0.93) | 0.94 (0.84–1.04) | ||||
| Jensen et al. [33] | Rates of participation in the first 18 months of the screening round. | Clinical record | 74.5% | 81% | 0.65 (0.63–0.68) | 0.79 (0.77–0.82) | Low |
| Ko et al. [22] | Utilisation of breast cancer screening services during the study period. | Self-report | 26% | 32% | n/a | 0.78 (0.43–1.4) | |
| Koroukian et al. [35] | Receipt of screening mammography in the study period and adherence to national guideline. | Clinical record | 38% | 32% | n/a | 0.68 (0.66–0.7) | Low |
| Kushalnagar [38] | Adherence to mammography guidelines. | Self-report | 76% | 82% | n/a | 0.94 (0.77–0.94) | Low |
| Murphy et al. [34] | Receipt of breast cancer screening, during the 6 year study period. | Clinical record | 51% | 62% | 0.88 (0.87–0.89) | 0.79 (0.78–0.8) | Low |
| Osborn et al. [25] | Clinical record of attending for mammography or mammography results during the study period. | Clinical record | 44% | 52% | IRR = 0.78 (0.74–0.83) * | IRR = 0.76 (0.72–0.81) * | Low |
| Ross et al. (2021) [27] | Records of women attending the screening programme from 1 April 2011 to 31 March 2014. | Clinical record | 74% | 81% | 0.71 (0.68–0.74) | 0.67 (0.64–0.7) | Low |
| Ross et al. (2020) [28] | Clinical attendance of screening invitation. | Clinical record | 75% | 81% | 0.53 (0.50–0.57) | 0.93 (0.89–0.98) | Low |
| Ross et al. (2019) [6] | Breast cancer screening attendance. | Self-report | 68% | 80% | 0.67 (0.64–0.70) | 0.77 (0.73–0.82) | Low |
| Sakellariou, Rotarou [20] | Receipt of mammogram within the past three years. | Secondary data analysis | 48% | 46% | n/a | 0.80 (0.70–0.92) | |
| Shin et al. [43] | Clinical attendance or use of mammography for breast cancer screening during 2014–2015. | Clinical record | 41% | 54% | n/a | 0.82 (0.82–0.83) | Low |
| Steele et al. [19] | Receipt of mammogram within the past 2 years. | Self-report | 67% | 73% | n/a | 0.79 (0.77–0.82) | High |
| Woodhead et al. [26] | Receipt of mammography in the past three years, and for aged 50–64 in five years. | Clinical record | 58% | 66% | 0.72 (0.61–0.86) | 0.60 (0.49–0.73) | Low |
| Wu et al. [44] | Receipt of mammogram within past two years. | Insurance record | PVL: 77% | 81% | n/a | 0.56 (0.36–0.87) | Low |
| SVL: 72% | 81% | n/a | 0.58 (0.37–0.9) | ||||
| Xu et al. [39] | Full adherence or partial adherence to screening guidelines, during the study period. | Insurance record | 65% | 75% | n/a | 0.49 (0.40–0.6) | Low |
| Author | Outcome Definition | Assessment Methods | Uptake (%) | Risk of Bias Rating | |||
|---|---|---|---|---|---|---|---|
| Women with Disabilities | Women without Disabilities | Unadjusted OR (95% CI) | aOR (95%CI) | ||||
| Abrams et al. [24] | Clinical attendance to cervical screening over the study period (July 2004–June 2004). | Clinical record | 25% | 18% | n/a | 1.46 (1.36–1.57) | Low |
| Brown et al. [30] | Clinical attendance to cervical screening between 1 April 2007 and 31 March 2010. | Clinical Record (Insurance code) | 68% | 77% | n/a | 0.61 (0.58–0.65) | Low |
| Cobigo et al. [36] | Receipt of at least one Pap test over a 3 year period. | Clinical record | 34% | 67% | 0.26 (0.25–0.27) | 0.21 (0.2–0.21) | Low |
| Eriksson et al. [29] | Clinical participation in cervical cancer screening over the 5 year study cohort period. | Clinical record | 86% | 89% | n/a | 0.98 (0.97–0.98) | Low |
| Horner-Johnson et al. [37] | Receipt of Pap smear with three years. | Clinical record | Rural: 77% | 84% | 0.50 (0.44–0.58) | 0.69 (0.59–0.81) | Low |
| Urban: 82% | 87% | 0.67 (0.62–0.72) | 0.78 (0.87–0.96) | ||||
| Ko et al. [22] | Utilisation of cervical cancer screening services during the study period. | Self-report | >30 years: 29% | 45% | n/a | 0.71 (0.41–1.22) | High |
| >40 years: 23% | 43% | n/a | 0.52 (0.27–0.98) | ||||
| Kushalnagar [38] | Adherence to pap smear guidelines. | Self-report | 78% | 85% | n/a | 0.71 (0.59–0.86) | High |
| Murphy et al. [34] | Receipt of pap smear during the 6 year study period. | Clinical record | 52% | 61% | 0.92 (0.92–0.93) | 0.80 (0.80–0.81) | Low |
| Osborn et al. [25] | Clinical record of attending for Pap smear during the study period. | Clinical record | 68% | 85% | IRR = 0.55 (0.53–0.57) * | IRR = 0.54 (0.52–0.56) * | Low |
| Shin et al. [43] | Use of the cervical cancer screening programme in the past ten years (2006–2015). | Administrative data (clinical record) | 54% | 60% | n/a | 0.71 (0.71–0.72) | Low |
| Steele et al. [19] | Receipt of a Pap smear within the past 2 years. | Self-report | 72% | 82% | n/a | 0.77 (0.60–0.99) | High |
| Weitlauf et al. [31] | Use of Pap smear test in outpatient setting during the study period. | Insurance record | n/a | Depression: 1.04 (0.98–1.09) | 1.05 (0.99–1.12) | Low | |
| PTSD: 1.17 (1.09–1.26) | 1.14 (1.06–1.22) | ||||||
| Woodhead et al. [26] | Receipt of cervical cancer screening any time in the last three years for those aged up to 49 years, or any time in the last five years for those aged 50–64. | Clinical record | 80% | 78% | 1.16 (0.99–1.35) | 0.35 (0.29–0.42) | Low |
| Xu et al. [39] | Full adherence or partial adherence to screening guidelines during the study period. | Insurance record | 64% | 81% | n/a | 0.32 (0.27–0.39) | Low |
| Screening Type | Sub-Group | Studies Included (References) | Pooled Estimate (95% CI) | Heterogeneity (I2) |
|---|---|---|---|---|
| Breast cancer | Visual impairment | N = 3 studies [5,20,33] | 0.63 (0.51–0.77) | 95% |
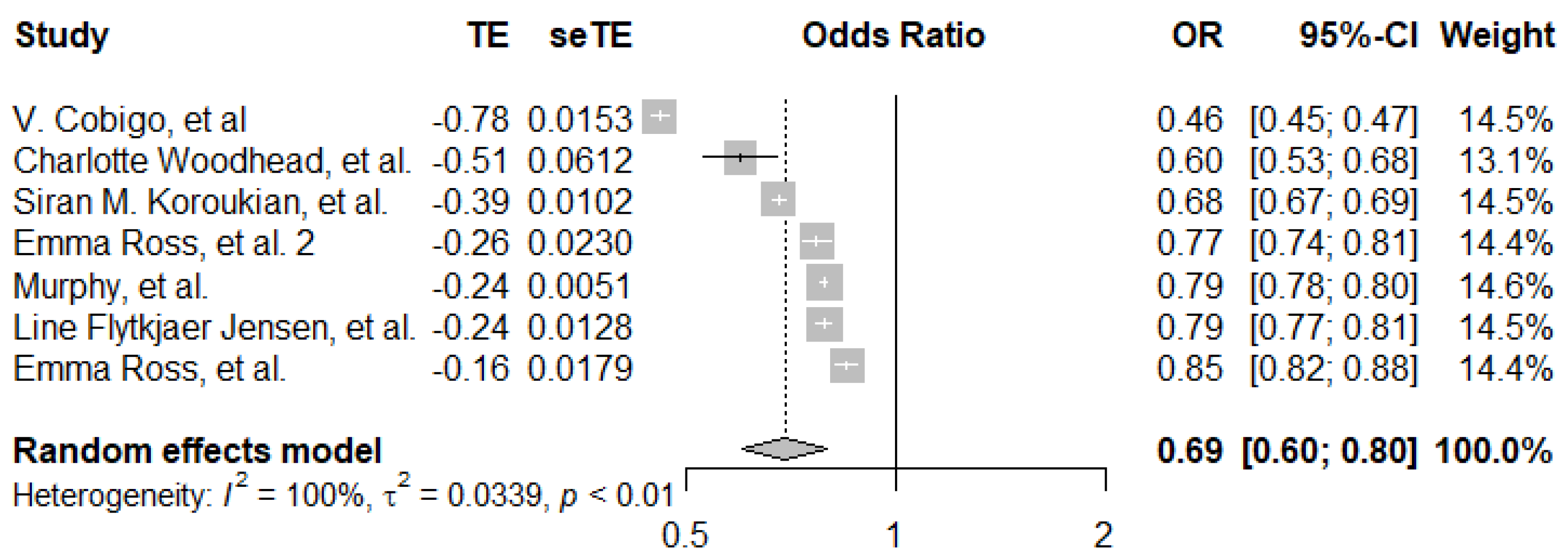
| Breast cancer | Psychosocial | N = 7 studies [22,23,24,25,26,31,32] | 0.69 (0.60–0.80) | 100% |
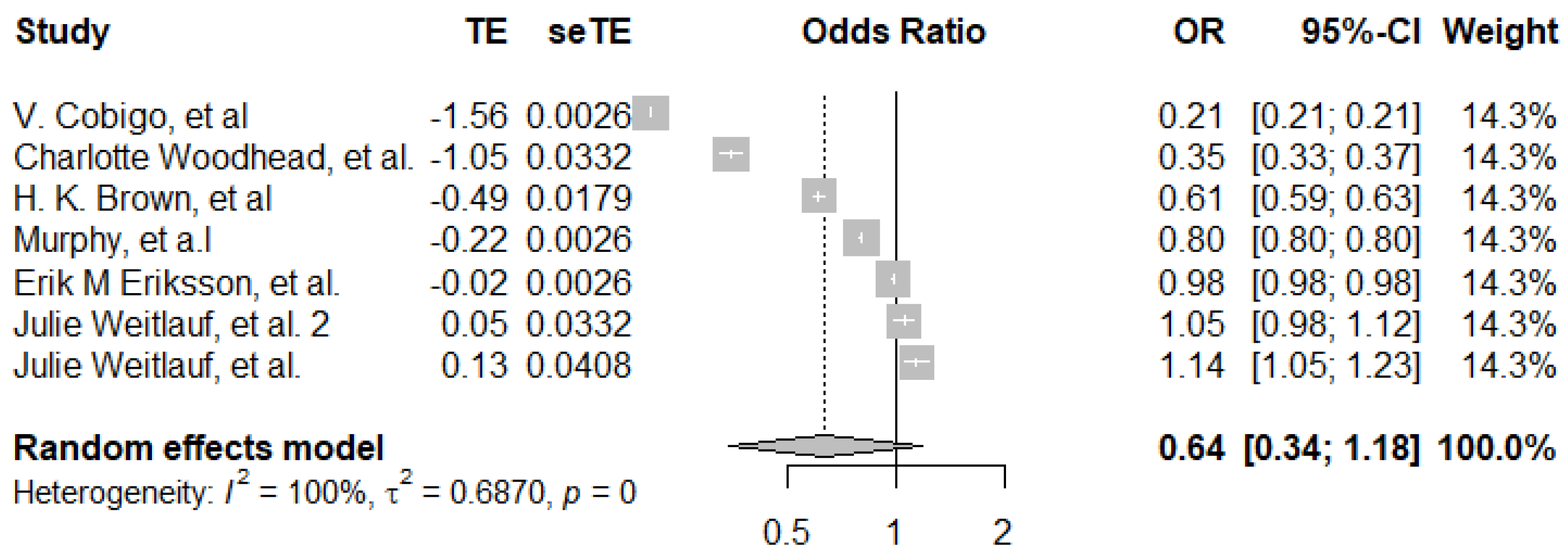
| Cervical cancer | Psychosocial | N = 6 studies [22,24,27,28,29,32] | 0.64 (0.34–1.18) | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andiwijaya, F.R.; Davey, C.; Bessame, K.; Ndong, A.; Kuper, H. Disability and Participation in Breast and Cervical Cancer Screening: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 9465. https://doi.org/10.3390/ijerph19159465
Andiwijaya FR, Davey C, Bessame K, Ndong A, Kuper H. Disability and Participation in Breast and Cervical Cancer Screening: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(15):9465. https://doi.org/10.3390/ijerph19159465
Chicago/Turabian StyleAndiwijaya, Fahrin Ramadan, Calum Davey, Khaoula Bessame, Abdourahmane Ndong, and Hannah Kuper. 2022. "Disability and Participation in Breast and Cervical Cancer Screening: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 15: 9465. https://doi.org/10.3390/ijerph19159465
APA StyleAndiwijaya, F. R., Davey, C., Bessame, K., Ndong, A., & Kuper, H. (2022). Disability and Participation in Breast and Cervical Cancer Screening: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(15), 9465. https://doi.org/10.3390/ijerph19159465