Abstract
Social-norms approaches are increasingly included in behavior-change programming. Recent reviews categorize a large number of norms-shifting programs but do not synthesize evidence about effectiveness. To inform the design of social and behavior-change programs in low- and middle-income countries in response to time-sensitive demands, this rapid systematic review examines the evidence for the effectiveness of interventions that use norms-based approaches to change behavior. Nine indexes and eight websites were electronically searched for both systematic reviews and primary studies. Abstracts and full texts were screened to include: documents published in 2010 and later; documents evaluating the effectiveness of programs that include norms-based approaches; documents measuring behavioral outcomes; and documents employing quantitative analysis of concurrent treatment and comparison groups. Data collected include participant age cohort, program name and duration, scope of norms, intervention activities, category of behavioral outcome, and statement of findings for the main behavioral outcome(s). Primary studies were appraised based on identification strategy. Search and screening yielded 7 systematic reviews and 29 primary studies covering 28 programs. Across the primary studies, the programs are highly heterogeneous, and the findings are mixed, with some strong positive effects and many marginal or null effects on behavior change. Taken together, the evidence shows that meta-norms-based approaches can be part of effective programs but do not assure that programs will change behaviors. Program designers can draw some general conclusions from this review but can also use it to locate specific studies relevant to their evidence needs.
1. Introduction
Social-norms approaches are increasingly included in behavior-change programming [1]. The definition of social norms, simply, is what other people do, believe, and approve of. Behavior-change interventions based on the theory of social norms, ascribed to Perkins and Berkowitz (1986) [2], seek to influence behaviors by providing feedback about existing social norms to change individuals’ perceptions of social norms [2]. The original example in health is binge-drinking behavior in colleges, where showing students that binge drinking is actually less prevalent than they perceived led to decreased binge drinking [2]. Dempsey, et al. (2018) review the evidence for the social norms theory approach for health attitudes and behavior change [3]. Social norms theory is also used to design programs in sectors other than health; a well-known example is social norms information about energy usage reported in letters to households that led to changes in energy conservation [4].
Social-norms approaches also include norms-shifting interventions. These interventions seek to do more than simply provide feedback about current norms. They seek to change norms, particularly norms in the sense of what other people approve of. For example, the prevailing norm may be that the perpetration of intimate partner violence (IPV) is socially accepted. A norms-shifting intervention attempts to change that norm so that individuals increasingly perceive that others do not approve of that behavior. A number of recent articles and reports usefully review theories, define concepts, and describe approaches for social norms interventions to change behavior [5,6,7]. Labels differ across articles, with some authors using norms-shifting or norms-changing to mean all interventions with a norms approach. Heise and Manji (2016) [1] define meta-norms as norms that influence multiple behaviors. They give the example of the norm that violence is not an appropriate form of punishment. Shifting toward that norm may reduce corporal punishment in schools and abuse within households. The Social Norms Lexicon similarly defines meta-norms as foundational norms that serve to create and maintain social norms and, as such, may be harder to shift [8].
A few recent reviews catalog and categorize a large number of norms-shifting programs [9,10,11] but do not report, assess, or synthesize evidence for the effectiveness of these programs, especially not evidence from rigorous evaluations. Thus, it is difficult for decision makers to access effectiveness evidence for program design.
This present review was conducted to meet the needs of my own organization, at which program designers need to respond to opportunities with fixed deadlines. Often, practitioners rely on limited or weak evidence when writing proposals—evidence from best practices based on past programming, one or a handful of academic articles, non-rigorous program evaluations, and even anecdotes. This review is the second pilot review in an initiative to select and refine rapid-review methodologies to provide higher-quality evidence for time-sensitive design work and to share that evidence publicly [12,13,14]. Originally planned for six weeks, the review ultimately took ten weeks from protocol registration to draft manuscript, chiefly due to staffing challenges, but I was able to share initial findings with colleagues as I was conducting the review.
1.1. Rapid Systematic Reviews
Although there is general agreement that rapid-review methodologies produce less reliable findings than full systematic reviews, there is growing demand by decision makers for timely evidence reviews [15,16]. One systematic review of rapid-review studies and their methods finds heterogeneity across methods and ambiguous definitions and standards, including a range of timelines from 1 to 12 months [16]. Another systematic review of rapid reviews finds 82 reviews that use a variety of streamlined methods [17]. An experiment comparing three full systematic reviews to three rapid reviews each for the same questions concludes that rapid reviews “may be feasible for focused clinical questions” (p. 9) but is more skeptical about the sensitivity of a rapid review to a systematic review in the case of complex programs [15]. Nevertheless, rapid reviews can serve the needs of decision makers [18], and to help meet those needs, the World Health Organization has published a guide for rapid reviews in public health [19].
Some rapid systematic reviews limit their searches to existing systematic reviews, some to primary studies, and some include both. The full rapid review conducted here includes both systematic reviews and primary studies as eligible studies. If there are relevant systematic reviews, they may provide program-ready findings about what works, so it is important to seek them out. The systematic reviews found for this review do not provide such findings. In the interest of space, I briefly summarize the findings from the reviews in this article and present the methods, tables, and summaries in the Supplementary Materials.
1.2. Objectives
To inform the design of social and behavior-change programs in low- and middle-income countries in response to time-sensitive opportunities, this rapid systematic review addresses the research question stated in the pre-registered protocol, “What is the recent evidence about the effectiveness of behavior-change interventions that incorporate social-norms approaches in improving behavioral outcomes in support of improving lives in low- and middle-income countries?” Specifically, this manuscript covers studies of interventions that address meta-norms, which are norms intended to influence multiple behaviors. The review reports the scope of the evidence base and provides information about studies to allow program designers to find evidence relevant to their needs. It also explores whether there are consistent features across effective programs.
2. Materials and Methods
The protocol for this review was registered on Open Science Framework on 30 October 2020 (osf.io/3fpnq) in a document modeled on the PROSPERO template [20]. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses [21]) statement checklist is Figure S1 in the Supplementary Materials. The following features of the review design were selected to enable the systematic review to be rapid. The range of eligible publication dates was limited to 2010 to present. This range allowed the review to capture the most recent primary studies and incorporate earlier research through systematic reviews. The electronic search strategies required that the word “norms” appear in the title, abstract, or keywords, and other terms in the string were tested and selected to generate a number of hits that was reasonably large while still feasible to screen within the timeline. The search process did not include a manual search of reference lists or expert consultation. A single reviewer conducted all screening and coding.
To avoid duplication, I conducted a quick search during protocol development for published systematic reviews matching the review objectives and found none. Systematic review protocols were not searched, as there was no guarantee that these reviews would be completed during the required timeline.
Additional details regarding materials and methods are presented in Appendix A.
2.1. Eligibility Criteria
The inclusion criteria for primary studies, listed roughly in order of ease of exclusion, were: (1) published in 2010 or later; (2) published in English; (3) journal article, published institutional report, published institutional working paper, or publicly posted pre-print; (4) reports findings for at least one endline; (5) evaluates an intervention implemented in a low- or middle-income country; (6) evaluates an intervention implemented in the field (i.e., excludes laboratory experiments and lab-in-the-field games); (7) measures a behavioral outcome; (8) uses quantitative study design with data from concurrent intervention and comparison groups using random assignment, natural experiment, fixed effects, or multivariate analysis identification strategies; (9) evaluates an intervention designed or intended to change behavior and includes a norms-based approach; (10) full text is available through our library without excessive cost.
The restriction to English-language publications facilitated the rapid review and accommodated the skills of the reviewers; however, it also ensures that the included studies are accessible to our colleagues using the evidence. This restriction also limits the review as discussion under limitations. All documents passing title and abstract screening were available in full text and screened, so the availability restriction did not bind. For inclusion, behavioral outcomes could be self-reported but needed to measure the actual behavior of the respondent. This definition rules out measures of behavioral intent and measures of the experience from others’ behavior. This latter clarification affected the inclusion of intimate partner and gender-based violence studies, as some of these studies measure whether the respondent experienced violence but do not measure the respondent’s behavior.
The most subjective of the inclusion criteria was the determination that there was a norms-based approach for behavior change. Although the term “norms” was used in the search strings, not all of the studies described the evaluated interventions as norms-based or social norms programs. I applied the eligibility criterion by examining the programs’ activities and the stated objectives of those activities. I looked for the use of actual norms, which are the attitudes held and behaviors exhibited by other people within a social group, or subjective norms, which are one’s perceptions of what most other people within a social group believe and do. I considered norms-based approaches for behavior change to include: activities to change the attitudes of a social group with the intention that the changed attitudes constitute new norms that influence individuals’ behavior; activities to change the behaviors of a social group with the intention that the changed group behavior establishes new norms that influence individuals’ behavior; and activities to inform or change one’s perception of what a social group believes or does with the intention of influencing that person’s behavior.
Note that activities to change group, or community, behavior without the stated intention to shift norms were not counted as norms-based approaches here. For example, a community sanitation program that seeks to increase sanitation behaviors across the community is not a norms-based intervention simply because it is community-based. However, such a program that includes activities to make improved behavior visible with the intent to influence others—for example, participants receive public acknowledgement for installing a toilet—does count as having a norms-based approach.
The word “norms” is sometimes also used to mean methods or processes. For example, Blattman, Hartman and Blair (2014) [22] study an intervention to train communities in the “practices and norms” of alternative dispute resolution. Here, “norms” means how people generally do something rather than what a social group believes or does. “Norms-teaching” interventions, which can be thought of as how-to rather than how-should interventions, were not included in this review.
2.2. Search Strategy
To better capture a wide variety of programs with norms-based approaches, the search strategy used a simple set of thematic terms—focusing on norms and behavior change—instead of attempting to name all the possible intervention types. The strategies also included a set of terms for interventions and a set of terms for evaluation. Figure 1 shows the search strategy for EBSCO minus the separate country terms for all low- and middle-income countries.
Figure 1.
Search strategy for EBSCO platform.
To reduce publication bias and to reduce “publication lag” bias (caused by the longer lag between endline data collection and journal publication for social science impact evaluations than for health impact evaluations [23]), we conducted a website search of eight websites that provide databases of systematic reviews and of impact evaluations for low- and middle-income countries. The librarian conducted the electronic searches on 2 November 2020, and the second reviewer conducted the website searches between 2 and 6 November 2020. Table S1 in the Supplementary Materials catalogues the complete search strings and the number of hits for the index and website searches.
2.3. Selection
After screening, to focus this first manuscript from the review on the types of programs most relevant to my organization’s current design needs, I coded the included studies for whether the evaluated norms-based approach employs direct norms or meta-norms [1]. An example of a direct norm is the prevalence of condom use in a peer group, which is used to influence condom-use behavior. Examples of meta-norms are gender rights and HIV risk prevention (Although HIV risk prevention is specific to one disease, programs promote this norm in order to influence multiple behaviors, such as condom use, testing, and partner concurrency). Most authors do not make the distinction between direct norm and meta-norm when describing their programs, so I made the judgment based on the descriptions, not on labels used in the studies. This manuscript reviews the evidence for the studies of programs employing meta-norms.
2.4. Data Collection
For the primary studies, I coded a primary sector for each study and a second sector for those that spanned more than one. I coded the participants by predominant cohort—children (roughly 0–12), adolescents (roughly 13–18), youth (roughly 16–24), and adults. I also coded whether the primary behavioral outcome(s) was measured for males and females together, both males and females separately, only females, or only males. I extracted the program name and the duration of the intervention in months, defined by when program activities began and ended. An intervention of any duration less than one month was coded as one. In the overview table, I briefly describe the types of norms addressed by each program. The key findings tables include brief descriptions of the activities included in the interventions.
To categorize the behavioral outcomes, I generalized the six domains laid out by Shelton [24] for health systems. The six categories for the review are personal, help seeking, continuation, provider (or employee), pro-social (or anti-social), and decision making. As Shelton explains, there is overlap between some of these categories, so the coding involved some judgment calls. I coded outcomes related to the perpetration of IPV as continuation behaviors, as IPV happens as a repeated cycle of violence in intimate partner relationships. I coded other gender-based violence outcomes as personal. For findings, I extracted the document’s statement of the effect on the main behavioral outcome(s) after confirming these statements against the estimates and statistics provided in the tables. In some studies, the behavioral outcomes are reported as secondary outcomes.
Studies were coded as including cost-effectiveness analysis, including some cost information, or not including any cost information. The extracted sample size is for the sample used to estimate the behavioral effect.
2.5. Appraisal
For the primary studies, given the need for rapid appraisal and to enable the participation of a junior reviewer on the team, as originally planned, the appraisal methodology was largely tied to the identification strategy. The first step in appraisal was to determine the identification strategy for the effect estimation for the primary behavioral outcome. I used the hierarchy from Waddington, et al.’s recommendation for risk-of-bias assessment, which has four levels: randomized controlled trial, natural experiment (i.e., as-if random assignment), double difference (or fixed effects), and single difference (or multivariate regression) [25]. I added to this a fifth level, between the first and second, for cluster randomized controlled trial. I calculated a simple score by assigning points 1 through 5 for identification strategy level and then adding a point each for concerns assessed, as described in Appendix A.1.4. Based on the clustering of the scores, I grouped the studies into strong, good, and weak confidence in the findings as discussed further in Section 3.
2.6. Analysis
For the primary studies, I report study characteristics and confidence-in-findings assessments for all 29 studies. To address risk of bias in the synthesis, I present and discuss the key findings separately according to the three categories of confidence in findings. To examine patterns in the findings for the strong- and good-confidence studies, I identify the level of the intervention as individual, community, or both.
The purpose of the rapid evidence review is to provide useful information to my colleagues and other practitioners for immediate program design decisions, not to prove or disprove the effectiveness of an approach. Thus, I did not conduct meta-analysis. The heterogeneity of interventions and outcomes also precludes meaningful quantitative synthesis.
2.7. Inclusion of Systematic Reviews
The methods and results for the search and screening for systematic reviews is reported in Appendix B. As explained further below, none of the reviews provide synthesized evidence specific to meta-norms interventions’ effects on behavior change.
2.8. Departures from the Protocol
The primary departure from the registered protocol [20] is that the bulk of the review was conducted by a single reviewer instead of the two reviewers named in the protocol. The second reviewer, an intern, left the project earlier than expected. This unexpected change in staffing partly explains the delay in the completion of the review, which was shared with colleagues ten weeks after the protocol was registered instead of six. However, the reliance on a single reviewer also ensured consistency in screening, appraisal, and data extraction. Other departures from the protocol are reported in Appendix A.1.5.
3. Results
3.1. Literature Search
Figure 2 presents the PRISMA flow diagram for this review. After de-duplication, 1307 title and abstract records were screened, resulting in 216 records passing to full-text screening. A total of 89 full texts met the inclusion criteria. Coding for the scope of norms intervention—direct or meta—produced a set of 7 included systematic reviews and 29 included primary studies. The final set of 28 primary studies includes 1 substitution article [26], which reports the primary trial results related to an included study [27] that only reports secondary data analysis. The secondary analysis explains that there was a norms aspect to the intervention but does not include the primary findings from the evaluation.
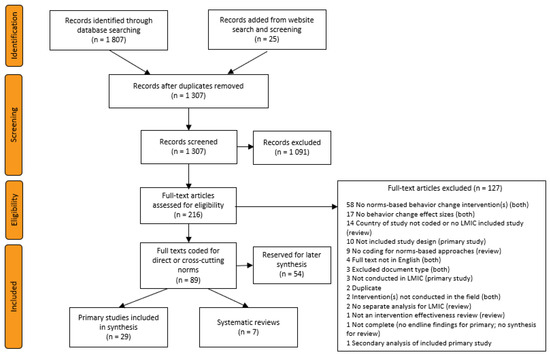
Figure 2.
PRISMA flow diagram of search and screening results.
3.2. Characteristics of Included Primary Studies
Figure 3 displays the heat map of the study locations by country. The majority of the studies come from Africa (21 out of 29), and there is roughly equal distribution (10, 9, and 10) of studies across low-income, lower-middle-income, and upper-middle-income countries.
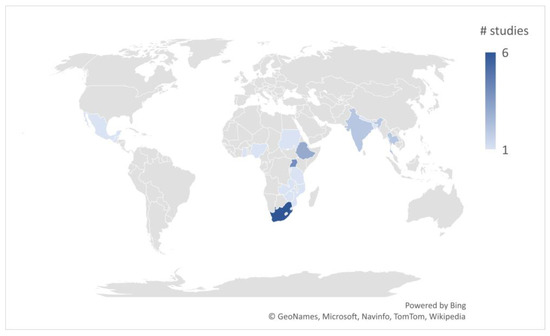
Figure 3.
Heat map of primary studies.
Table 1 presents the main features of each of the primary studies. All the documents report studies of distinct programs, except for two that evaluate that SASA! program [28,29]. The two documents for the SASA! evaluation, a journal article and an evaluation report, focus on different sets of outcomes. All but 2 of the 29 studies fall within the health or DRG sectors as the primary sector (not in table). Of the two exceptions, one tests a social marketing project to alter sustainable consumption behavior [30] (coded as environment and climate change), and the other studies an economic empowerment program to change education and employment behavior [31] (coded as economic growth). The majority of the studies concern HIV prevention [26,32,33,34,35,36,37], gender-based or intimate partner violence [38,39,40,41], or a combination of the two [28,29,42,43,44,45].
The DRG studies that are not about interpersonal violence include studies of: a community-based skills development program to delay child marriage [46]; a community development fund to increase pro-social behavior [47]; a school-based gender attitudes curriculum to improve boys’ behavior [48]; and a community-based program to encourage advocacy of gender equality [49]. The health studies that are not about HIV or interpersonal violence include: a community-based program to improve maternal health seeking [50]; a couples intervention to improve maternal health seeking and other behaviors [51]; a school-based program to reduce bullying [52]; a school-based sex education program to encourage safe sex behavior [53]; and community workshops to promote increased use of modern contraception [54]. The duration of interventions ranges from 1 month or less to 50 months. Half the interventions were shorter than 1 year; a third lasted between 18 months and 3 years; and the rest lasted 4 or more years.

Table 1.
Features of included primary studies.
Table 1.
Features of included primary studies.
| Study ID | Title | Country | Program | Norms | Duration Months | Participant Age/Sex | Behavioral Outcome |
|---|---|---|---|---|---|---|---|
| Amin 2018 [46] | Skills-building programs to reduce child marriage in Bangladesh: A randomized controlled trial | Bangladesh | Bangladeshi Association for Life Skills, Income, and Knowledge for Adolescents (BALIKA) | Gender rights | 18 | Adolescents/Female | Personal |
| Avdeenko 2014 [47] | International interventions to build social capital: Evidence from a field experiment in Sudan | Sudan | Community Development Fund | Community pro-sociality | 50 | Adults/Together | Pro-social |
| Banerjee 2019 [32] | The entertaining way to behavioral change: Fighting HIV with MTV | Nigeria | MTV Shuga | Sexual health and HIV prevention | 1 | Youth/Together | Personal |
| Christofides 2020 [38] | Effectiveness of a multi-level intervention to reduce men’s perpetration of intimate partner violence: A cluster randomised controlled trial | South Africa | Sonke Community Health Action for Norms and Gender Equality (CHANGE) | Gender power, gender-based violence, sexuality | 18 | Adults/Male | Continuation |
| Cowan 2010 [33] | The Regai Szive Shiri project: Results of a ramonized trial of an HIV prevention intervention for youth | Zimbabwe | Regai Dzive Shiri | Sexual and reproductive health | 48 | Youth/Both | Personal |
| Dhar 2018 [48] | Reshaping adolescents’ gender attitudes: evidence from a school-based experiment in India | India | Breakthrough classes | Gender equality | 30 | Adolescents/Together | Continuation |
| Dougherty 2018 [50] | A mixed-methods evaluation of a community-based behavior-change program to improve maternal health outcomes in the upper west region of Ghana | Ghana | Community Benefits Health | Maternal health and breastfeeding | 24 | Adults/Female | Help seeking |
| Doyle 2018 [51] | Gender-transformative Bandebereho couples’ intervention to promote male engagement in reproductive and maternal health and violence prevention in Rwanda: Findings from a randomized controlled trial | Rwanda | Bandebereho | Gender equality, fatherhood, maternal health, intimate partner violence | 5 | Adults/Both | Help seeking |
| Figueroa 2016 [34] | Effectiveness of community dialogue in changing gender and sexual norms for HIV prevention: Evaluation of the Tchova Tchova program in Mozambique | Mozambique | Tchova Tchova | Gender equality, sexuality, HIV prevention | 18 | Adults/Together | Personal |
| Gottert 2020 [55] | Gaining traction: Promising shifts in gender norms and intimate partner violence in the context of a community-based HIV prevention trial in South Africa | South Africa | Tsima | Gender equality, relationship violence, sexual health | 36 | Adults/Male | Continuation |
| Kalichman 2013 [35] | Randomized community-level HIV prevention intervention trial for men who drink in South African alcohol-serving venues | South Africa | Alcohol–HIV risk reduction workshops | Safe sex, interpersonal communication | 3 | Adults/Male | Personal |
| Kraft 2012 [36] | Effects of the Gama Cuulu radio serial drama on HIV-related behavior change in Zambia | Zambia | Gama Cuulu Radio Serial Drama | Sexual health, sexual cleansing, child sexual abuse, HIV prevention | 24 | Adults/Together | Personal |
| Kyegombe 2014 [28] | The impact of SASA!, a community mobilization intervention, on reported HIV-related risk behaviours and relationship dynamics in Kampala, Uganda | Uganda | SASA! | Gender equality and power, gender-based violence | 48 | Adults/Both | Personal |
| Lundgren 2018 [49] | Does it take a village? Fostering gender equity among early adolescents in Nepal | Nepal | Choices, Voices, and Promises | Gender equity | 3 | Adolescents/Together | Personal |
| Maman 2020 [42] | Results from a cluster-randomized trial to evaluate a microfinance and peer health leadership intervention to prevent HIV and intimate partner violence among social networks of Tanzanian Men | Tanzania | Microfinance and peer health program for social networks of men | Gender-based violence and power, safe sex | 30 | Adults/Male | Continuation |
| Miller 2014 [39] | Evaluation of a gender-based violence prevention program for student athletes in Mumbai, India | India | Parivartan (Coaching Boys Into Men) | Gender equity, gender-based violence, abuse | 4 | Adolescents/Male | Personal |
| Naidoo 2016 [52] | Verbal bullying changes among students following an educational intervention using the integrated model for behavior change | South Africa | School-based education program | Gender-based violence, bullying | 5 | Adolescents/Together | Pro-social |
| Pettifor 2018 [43] | Community mobilization to modify harmful gender norms and reduce HIV risk: results from a community cluster randomized trial in South Africa | South Africa | Sonke One Man Can community mobilization | Sexual health, gender equality and power, gender-based violence, social cohesion | 24 | Youth/Together | Personal |
| Pulerwitz 2015 [40] | Changing gender norms and reducing intimate partner violence: Results from a quasi-experimental intervention study with young men in Ethiopia | Ethiopia | Male Norms Initiative | Gender equality, sexual health, intimate partner violence | 1 | Youth/Male | Continuation |
| Rijsdijk 2011 [53] | The world starts with me: A multilevel evaluation of a comprehensive sex education programme targeting adolescents in Uganda | Uganda | World Starts With Me | Sexual and reproductive health and rights | 6 | Adolescents/Together | Personal |
| Schuler 2015 [54] | Interactive workshops to promote gender equity and family planning in rural communities of Guatemala: Results of a community randomized study | Guatemala | C-Change couples workshops | Gender equality, sexual and reproductive health | 1 | Adults/Together | Continuation |
| Sharma 2020 [44] | Effectiveness of a culturally appropriate intervention to prevent intimate partner violence and HIV transmission among men, women and couples in rural Ethiopia: Findings from a cluster-randomized controlled trial | Ethiopia | Unite for a Better Life | Gender equality and power, sexuality, violence | 2 | Adults/Both | Continuation |
| Sosa-Rubi 2017 [41] | True Love: Effectiveness of a school-based program to reduce dating violence among adolescents in Mexico City | Mexico | True Love | Gender equality, dating violence, sexual rights | 4 | Adolescents/Both | Personal |
| Stark 2018 [31] | Effects of a social empowerment intervention on economic vulnerability for adolescent refugee girls in Ethiopia | Ethiopia | Creating Opportunities through Mentoring, Parental Involvement and Safe Spaces (COMPASS) | Gender power, reproductive health | 10 | Adolescents/Female | Personal |
| Thato 2013 [37] | A brief, peer-led HIV prevention program for college students in Bangkok, Thailand | Thailand | Brief, Peer-Led HIV Prevention Program | Sexual health, HIV prevention | 1 | Youth/Together | Personal |
| Vantamay 2019 [30] | “3S Project”: A community-based social marketing campaign for promoting sustainable consumption behavior among youth | Thailand | 3S Project | Sustainable consumption | 3 | Youth/Together | Continuation |
| Wagman 2015 [45] | Effectiveness of an integrated intimate partner violence and HIV prevention intervention in Rakai, Uganda: Analysis of an intervention in an existing cluster randomised cohort | Uganda | Safe Homes and Respect for Everyone Project (SHARE) | Gender rights, intimate partner violence | 4 | Adults/Both | Continuation |
| Watts 2015 [29] | The SASA! study: A cluster randomised triral to assess the impact of a violence and HIV prevention programme in Kampala, Uganda | Uganda | SASA! | Gender equality and power, gender-based violence | 32 | Adults/Together | Continuation |
| Wechsberg 2016 [26] | The male factor: Outcomes from a cluster randomized field experiment with a couples-based HIV prevention intervention in a South African township | South Africa | Couples Health Coop, Women’s/Men’s Health Coop | Gender equality, sexuality, intimate partner violence, communication | 1 | Adults/Both | Personal |
Of the eight studies conducted outside of Africa, four come from South Asia [39,46,48,49], two from Thailand [30,37], and one each from Guatemala [54] and Mexico [41]. The programs in South Asia and Latin America are all gender equality and gender-based violence programs. From Thailand, one study evaluates an HIV prevention program and the other a sustainable consumption project.
Half of the studies measure outcomes for adults, six for youth, eight for adolescents, and none for children. Twelve studies measure outcomes for males and females combined, eight for males separately and females separately, three for only females, and six for only males. Although there were six possible coding categories for behavioral outcomes, almost all of the studies measure personal (freestanding) behaviors or behavioral continuation, with some fuzziness between these two categories, as discussed above. Two studies measure help seeking [50,51], and two studies characterize the behavioral outcomes as pro-social [47,52]. None of the studies measure service provider or policy- and decision-making behavioral outcomes.
Data coded but not reported in the table show that only one study presents a cost-effectiveness analysis [29], and two others present limited cost information [33,36]. A recent report may assist future evaluators to provide costing information [56].
3.3. Confidence in Findings
Table 2 displays the results of the confidence-in-findings assessment according to the three groupings: strong confidence, good confidence, and weak confidence. Only one study is a randomized controlled trial (RCT); however, several are cluster randomized controlled trials (CRCT). It is not surprising to see the prevalence of cluster assignment when the interventions are targeting meta-norms, which often involve community-level activities. The 15 studies assessed as having strong confidence in the findings use random assignment and have one or fewer concerns. There are no studies that use as-if random assignment, so the step down to good confidence in the findings indicates random assignment studies with at least two concerns or studies that use double difference (DD) as the identification strategy and have no concerns. There are seven studies in this category. The seven studies assessed as having weak confidence in the findings all use single-difference (SD) comparisons for identification, that is, they do not control for any selection on unobservable variables, except for one DD study that also has one concern. Table 2 also lists the sample size used to estimate the primary behavioral outcome effect, but sample size was not a factor in the appraisal.
Table 2.
Confidence-in-findings appraisal and sample size for behavioral outcome of primary studies.
3.4. Estimated Effects on Behavior Change
Table 3, Table 4 and Table 5 present the main findings for the behavioral outcomes of the studies with strong, good, and weak confidence in the findings, respectively. The findings are mixed. Looking first at those appraised as strong and good (i.e., those with a design that controls for at least some unobservable characteristics), many programs did not demonstrate an effect on behavioral outcomes; for example, the Sonke CHANGE program in South Africa [38] and the related Tsima intervention implemented by Sonke [55] showed no effect on men’s perpetration of IPV, and the Regai Dzive Shiri program in Zimbabwe showed no effect on sexual or pregnancy prevention behavior [33]. Some programs demonstrated moderate or suggestive effects; for example, contraceptive use improved but not statistically significantly as an outcome of the C-Change couples’ workshops in Guatemala [54], and COMPASS in Ethiopia produced moderate improvements in schooling and transactional sex [31]. A few demonstrated large and statistically significant effects, such as the Bandebereho program in Rwanda, which produced substantial improvements in outcomes, including women’s attendance and men’s accompaniment at ante-natal clinics [51], and the alcohol–HIV risk reduction workshops in South Africa that caused men to increase condom use and engage in more conversations about HIV/AIDS [35].
Table 3.
Main findings for behavioral outcomes from primary studies assessed as having strong confidence in the findings.
Table 4.
Main findings on behavioral outcomes for primary studies assessed as having good confidence in the findings.
Table 5.
Main findings on behavioral outcomes for primary studies assessed as having weak confidence in the findings.
While the presence of so many studies without positive findings may be an encouraging sign that there is no publication bias, many of the studies that did not detect changes in behavior did detect positive changes in other outcomes, such as attitudes and perceived social norms. Therefore, there may be additional evaluations that did not detect behavior changes or other changes that have not been published.
Findings are similarly mixed for the studies with weak confidence in the findings, shown in Table 5. The SHARE program in Uganda demonstrated detectable behavior changes in the disclosure of HIV status but did not demonstrate an effect on male-reported IPV perpetration [45]. The Parivartan program in India measured reduced bullying behaviors but only marginally statistically significantly [39]. The Tchova Tchova program in Mozambique increased the likelihood that respondents talked with their partners about HIV [34].
3.5. Analysis of Program Design
There is great heterogeneity in the activities included in the different programs, with most programs incorporating a mix of activities. Looking at the various sets of activities, though, we can see that some programs operate primarily at the community level, some at the individual level, and some at both. An example of a community-level program is the Community Development Fund in Sudan, which included community construction projects, social mobilizers, and community scorecards among other activities [47]. An example of an individual-level program is the use of Breakthrough classes in schools in India, which covered a curriculum of topics with students over time [48]. An example that combines the two levels is the True Love program in Mexico, which combined classroom-based workshops with community engagement activities [41]. I categorized the programs evaluated by the included studies in this review into the three groups—community, individual, or both—based on the descriptions of the activities in the studies.
There is very limited evidence of positive behavioral outcomes from community-level programs from the studies with strong confidence in the findings. Avdeenko and Gilligan (2015) explain that, while the respondents in the community development fund communities in Sudan self-reported greater civic participation behavior than those in the control communities, when the authors examined participants’ behavior using a game, there were no differences [47]. The only community-level program among the good-confidence studies is the SASA! program in Uganda, which did produce positive outcomes for HIV prevention but did not measure direct behavioral outcomes for IPV [28,29]. The two studies of community-level programs among those with weak confidence did measure positive changes, one on maternal health behaviors [50] and the other on HIV communication behaviors [34]. These programs implemented different sets of activities, but perhaps of note, they had longer durations—18 to 48 months.
The most convincing positive findings among the strong and good evaluations of programs with activities at both the community level and individual level are from the alcohol–HIV risk reduction workshops in South Africa [35]. The men who participated in these workshops and community activities reported improvements in some, but not all, HIV risk reduction behaviors compared to the control. The True Love evaluation compares a combined community and individual intervention to only a community intervention and finds that the combined intervention reduces the perpetration of psychological violence relative to the community intervention alone [41]. Among the weak evaluations, the studies of programs implemented at both the community and individual level found limited positive outcomes.
There are two multi-arm studies that compare combined interventions to single interventions—one compares to community only and the other to individual only. The Pulerwitz, et al. (2015) [40] study, appraised as having good confidence in the findings, tests two variants against a control, one with community engagement activities only and one with community engagement and interactive group education for men. In this case, both elements are supposed to be norms-shifting, but the study offers a comparison of only working at the community level vs. working at both the community and the individual level. Both arms produced reductions in the perpetration of violence toward partners, although the community-engagement-alone arm has better statistical support. However, the combined intervention showed better results for other (non-behavioral) outcomes. The authors do not draw any conclusions about whether the combined activities are better than the community engagement intervention on its own.
The Lundgren, et al. (2018) [49] study, appraised to have weak confidence in the findings, compares an individual-level intervention (Choices) with that intervention combined with a family-level intervention (Voices) and a community-level intervention (Promises). All three are intended to change norms, so like the Pulerwitz, et al. study, it does not compare a “with norms approach” to a “without norms approach” but rather, individual-level approach to combined community, family, and individual. The study does suggest that the combined intervention had a greater effect on one of the measured behaviors.
Among the individual-level programs, which account for the plurality of programs among the three appraisal categories, the findings are also mixed, with some programs demonstrating positive behavioral outcomes, for example, the classroom curriculum implemented by Breakthrough in India [48], and others not, for example, the microfinance and peer health leadership intervention in Tanzania [42]. No patterns emerge when looking at the features of the programs, including participants, duration, norms, and interventions.
3.6. Systematic Reviews
As reported in Figure 2, the search, screening, and coding for meta-norms approaches identified seven systematic reviews. One explanation for the small number of systematic reviews screened is that the selection criteria (see Supplementary Materials) required that the review report the country for each included study, include studies from LMICs, and present the findings to allow for separate synthesis of evidence for LMICs. An abbreviated ROBIS [57] risk-of-bias assessment categorized no reviews as having a low risk of bias; three as having an unclear risk of bias; and the other four as having a high risk of bias. Appendix B includes summaries of the three reviews with an unclear risk of bias, but while all three reviews included one or more study of interventions that had meta-norms-based approaches and include one or more study that estimated effects on measured behavior changes, the syntheses do not isolate the evidence for meta-norms-based approaches on behavior-change outcomes.
4. Discussion
Taken together, the studies included in this review reveal a growing evidence base for programs using social-norms approaches targeting meta-norms in low- and middle-income countries. No two interventions are the same, however, and the findings across studies are mixed with some strong positive effects and many marginal or null effects. From the evidence in this review, it is clear that meta-norms approaches can be effective to change behavior, but they are not always so. Put differently, incorporating meta-norms into programs is not sufficient to change behavior, as evidenced by the prevalence of studies in this review that show no effects on behavior.
For program design, it is also important to know whether norms shifting is necessary to produce behavior changes. There are many behavior theories applied to programming that do not involve norms. A primary example is Bandura’s social cognitive theory [58], which focuses on how people learn behaviors by observing others. On the other hand, prevailing social norms are considered key factors for some behaviors, for example, IPV, suggesting that these behaviors cannot be changed without shifting social norms. One way to explore this question is with multi-arm studies that compare with norms to without norms. This review only identified one such study.
The Amin, et al. (2018) [46] study is appraised as having a strong confidence in the findings. They implemented a four-arm CRCT in Bangladesh, where one arm was an educational support intervention, one was a gender rights awareness intervention, one was livelihoods training, and the fourth was the control. These were all community-based interventions, in the sense that the capacity development was delivered through community centers, but these were not community engagement interventions. The activities were delivered directly to the participating girls. Gender rights awareness is the most clearly a norms-shifting approach of the three. The primary outcome was child marriage. The finding is that all three interventions reduced child marriage without much measurable difference between them. Therefore, in this case, building girls’ skills in any of these three ways made a difference, and the gender rights awareness approach was not necessary.
Even if a norms approach is not necessary for a program to produce detectable changes in behaviors over a fixed period of time, it is likely still true that shifting social norms is necessary to produce sustainable, community-wide changes in behaviors such as IPV perpetration, for which social norms play a big role. The studies in this review are program evaluations, so what they show is which programs were able to achieve detectable changes in respondents’ behaviors over the evaluation period, which can inform the design of future programs that need to demonstrate the same.
The key findings reported in Table 3, Table 4 and Table 5 point to the studies for which positive behavioral outcomes can be detected. The heterogeneity in interventions, norms, and outcomes makes it impossible to draw conclusions about what works that can be applied across contexts. Program designers can use the evidence in this review by selecting the studies most relevant to the context, norms, participants, and outcomes they seek to address.
As reported in Table 1, the programs reviewed here targeted a variety of norms. The evaluations do not use a standardized framework for labeling the norms and provide limited information about the specific norms messages delivered. The information reported in Table 1 is thus descriptive without intending to establish categories across studies. Just as meta-norms influence multiple behaviors, there are behaviors that may be influenced by multiple norms. For example, IPV perpetration may be influenced by norms around violence and criminality and also by norms around family responsibility. Similarly, HIV risk reduction may be influenced by norms around personal responsibility and self-care and also by norms around responsibility to others. In such cases, for program design, we want to know if one norm is more effective than another at changing behavior. Unfortunately, the studies in this review do not allow us to answer these questions. There are no multi-arm studies implementing the same activities but with different norms messages. In addition, there is not enough information about norms messages or consistency in approaches across studies that we can attribute the success of one program compared to another as explained by the specific norms targeted.
In spite of the growing evidence base, there are challenges for implementers and program designers to incorporate the latest learning on social norms. One challenge is simply getting the concepts and terminology straight. First, we can think of two kinds of norms approaches. The original social norms theory for behavior change is not about changing norms but about changing individuals’ knowledge or perceptions of what the existing social norms are in order to change their behavior, for example, the college drinking and utility bills experiments. These interventions often use direct norms, that is, the norm directly associated with the behavior.
In designing and implementing programs for development funders, we are more often tasked with changing, or shifting, norms in order to change behavior. The programs that address meta-norms, reviewed here, are generally of the latter type—trying to change norms. The interventions that use norms are generally quite different than the interventions that change norms, so evidence from one type should not be used to design the other.
Second, within the numerous interventions that seek to change norms, there is a fuzzy line between actually addressing social norms (what others do and believe) and simply addressing attitudes (what each individual thinks), which eventually changes norms through aggregation. This fuzziness is one reason that measuring changes in norms is complicated—people may misperceive or misattribute their own attitude change to a change in social norms. Cislaghi and Shakya (2018) argue that “the norms as attitudes school is not helpful for practitioners dealing with pluralistic ignorance…” [5] (p. 40). Many of the studies excluded from the review measure norms as an outcome even though the interventions addressed only knowledge and attitudes.
Limitations
The limitations to this review mostly arise from the rapid-review design decisions. The review is biased toward more recent studies, although the systematic reviews include numerous studies published before 2010. The narrowed search strings mean that some eligible studies were certainly missed. The public health rapid reviews reported in Affengruber, et al. (2020) [15] included fewer than half the included studies in the reference review. Those rapid reviews relied on an electronic search of a single index and reference list checking, and the missed studies were all non-indexed studies. The methodology used here improves on that by electronically searching multiple indexes to yield a much larger number of abstracts to screen and by searching websites to find grey and non-indexed studies.
The English-only restriction is a notable limitation, especially when reviewing studies conducted in low- and middle-income countries. The review is missing, for example, research conducted in Francophone Africa and published in French. We balanced this limitation against the demand to conduct a rapid review using available resources.
One reviewer for all screening and coding improves the consistency relative to a rapid-review design where multiple reviewers screen separate studies. However, bias and mistakes in screening and coding are more likely when there is only one reviewer per record instead of screening and coding in duplicate [15]. The review question covers research published in both health and social science outlets. Based on my experience with this and an earlier review [59], I suspect that the search missed more eligible social science articles than health articles. One indication is that the number of hits from EconLit was relatively low (55 hits). One explanation for this bias is that social science abstracts do not follow a consistent template and often leave out key details, and some social science journals do not use abstracts at all. The definition of what is a norms-based approach is unavoidably imprecise, meaning some of the screening decisions required more of a judgment call than others.
5. Conclusions
In the last decade, dozens of behavior-change interventions using norms-based approaches have been rigorously evaluated. The majority of these address a direct norm tied to a specific behavior; however, 29 studies evaluate behavior-change outcomes for 28 different programs that address meta-norms, such as gender rights, reproductive health, sexuality, and IPV. In addition, seven systematic reviews published since 2010 examine behavioral outcomes from a wide variety of interventions, some of which include meta-norms-based approaches. Taken together, the evidence shows there are some effective programs that include norms-based approaches, but addressing meta-norms does not guarantee that a program will produce individual behavior changes.
The scope of interventions eligible for this review was broad, allowing for all sectors, themes, and activities and allowing for any kind of meta-norm. As such, the included programs are highly heterogeneous. While this complicates evidence synthesis, it should reflect that the programs are being designed with each context and relevant social norms in view.
This review finds that the evidence base for behavior-change interventions using meta-norms-based approaches primarily covers HIV prevention, gender-based or intimate partner violence, or a combination of the two. Program designers in those fields will find the most relevant evidence here, especially for countries in Africa. Program designers for meta-norms approaches in other fields can also use this review to look for studies relevant to their evidence needs. All the studies from South Asia and Latin American evaluate programs addressing gender equality and gender-based violence.
I recommend that program designers seeking to shift meta-norms consider including community-level activities in their programs, and that programs implemented only at the community level be implemented over a longer period of time before expecting to detect behavior changes. Because the effectiveness of meta-norms approaches varies by context and program, program designers should conduct both formative research to inform their program design and formative evaluation to test for feasibility and acceptability of the proposed intervention prior to starting a full implementation. Some studies reviewed here, for example, Gottert, et al. (2020) [55], find positive outcomes for both the program and comparison groups, so new programs should also be subject to impact evaluation (i.e., evaluation against the counterfactual) before going to scale to ensure that positive outcomes can be attributed to the program.
In terms of future research, this review reminds us that it is necessary to measure behavioral outcomes when evaluating programs intended to change behavior. Many studies were excluded because they did not actually measure behavioral outcomes, and in the included studies, we see that positive outcomes for knowledge, attitudes, perceptions, and intent do not always translate into behavior change. Researchers should also pay more attention to how they are analyzing and interpreting findings when they measure a large number of outcomes. The multiple comparisons concerns caused a handful of the included studies to be downgraded during critical appraisal. It is difficult for program designers to use evidence to predict the effects of their planned program when there are only a few positive findings among a large number of measured outcomes. Finally, future research will also be more useful to decision makers and accessible for review if evaluators more carefully document the norms targeted and which activities are designed specifically to shift norms, especially when evaluating complex programs.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph19127312/s1, Figure S1: PRISMA 2009 Checklist; Table S1: Index searches; Table S2: Website searches. Reference [21] is cited in the Supplementary Materials.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. This study received a non-human-subjects research determination from the FHI 360 Official of International Research Ethics on December 10, 2020. (Project #: 1695760-1).
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are openly available in Open Science Framework at osf.io/qmg3k.
Acknowledgments
I thank Alison Burns for her excellent contributions as the search librarian for this review and her colleague in the FHI 360 Library, Tamara Fasnacht, for article retrieval. I acknowledge the contributions of Isaiah Braxton, who provided research assistance at the beginning of the review. I thank Kara Tureski for her engaging discussions and valuable feedback in the development of the protocol, throughout the review process, and on the draft manuscript.
Conflicts of Interest
The author declares no conflict of interest.
Appendix A
Appendix A.1. Additional Methods and Materials Details
Appendix A.1.1. Search Strategy
Together with a search librarian, we developed separate primary study and systematic review search strategies for Academic Search Premier, EconLit, Education Full Text (H.W. Wilson), Environment Complete, ERIC, and Global Health APA PsycInfo indexes (using the EBSCO platform) and Scopus. We developed a combined search strategy for PubMed.
When the screening was complete, I searched for journal articles associated with each of the included institutional reports and working papers and replaced two such documents with corresponding journal articles. In both cases, the documents were found in website searches, but the title, abstracts, and keywords for the journal article versions did not include the terms used in the electronic searches, which explains why the electronic searches did not uncover them.
Appendix A.1.2. Selection
The librarian exported the search results from the index searches into Endnote, and the reviewers imported them into Covidence for de-duplication and screening. Both reviewers screened the same 100 title and abstract records in Covidence and compared and discussed the results to serve as a training exercise for the second reviewer. The second reviewer conducted the website searches. Because not all websites allow search hits to be exported in a file, the reviewer screened titles and abstracts in the websites and imported the results of the website search and title/abstract screening into Covidence. I then screened all titles and abstracts and all full texts in Covidence.
Appendix A.1.3. Data Collection
The nine sector categories (education; health; democracy, rights, and governance; agriculture and food security; crisis and conflict; economic growth, finance, and trade; environment and climate change; water and sanitation; and energy) correspond roughly to the sectors used by the United States Agency for International Development (USAID), which are similar to those used by other program funders. Studies that focus on IPV and on other violent behavior (for example, bullying) are categorized under the health or democracy, human rights, and governance (DRG) sectors, not under crisis and conflict, because these studies focus on interpersonal behavior, not on political conflict. All data were extracted into Microsoft Excel.
Appendix A.1.4. Appraisal
After determining the identification strategy, the reviewer marked whether the study is reported in a working paper or institutional report as opposed to a peer-reviewed journal. These studies receive one “concern point” as they have likely not undergone the same degree of quality review as the journal articles, and the published results may change between the working paper and final publication in a journal. The reviewer then assessed three aspects of the study for possible concern: the fidelity of the intervention implementation; the fidelity of the research implementation; and the quality of measurement and analysis. The first two of these are typically reported in the study; examples include program implementation challenges for the first and participant attrition for the second. The third required more judgment on the part of the reviewer. The majority of the studies for which I marked a concern on measurement and analysis are cases in which the study reports findings for a large number of outcomes without any correction or discussion of multiple comparisons.
Appendix A.1.5. Departures from the Protocol
Another departure from the protocol is that I did not code the norms as being descriptive or injunctive. For the interventions targeting meta-norms, this distinction was not clear or meaningful, as the activities delivered a variety of messages, which likely included both descriptive and injunctive norms. The appraisal methodology was a bit more detailed than what the protocol described. It assessed five domains instead of three. Based on the clustering of the scores, I reported only three categories of confidence in findings instead of the four listed in the protocol. As explained above, in this manuscript, I present the findings from a subset of the studies for the larger review as laid out in the protocol.
Appendix B
Appendix B.1. Systematic Reviews
Appendix B.1.1. Materials and Methods
The inclusion criteria for systematic reviews, listed roughly in order of ease of exclusion, were: (1) published in 2010 or later; (2) published in English; (3) journal article, published institutional report, published institutional working paper, or publicly posted pre-print; (4) reports findings from synthesis; (5) review question includes effectiveness of interventions; (6) includes quantitative studies that use the study designs for included primary studies; (7) reports country of study for each included study and includes at least one study of an intervention implemented in an LMIC; (8) analyzes some or all findings separately for LMICs and high-income countries; (9) includes studies of behavior-change interventions that include a norms-based approach; (10) allows identification of included studies that have a norms-based approach; (11) reports findings for behavioral outcomes; (12) full text is available through our library without excessive cost.
For the systematic reviews, I collected descriptive information and extracted the number of included documents and programs.
To assess the risk of bias for the included systematic reviews, I applied the ROBIS tool [57] in an abbreviated manner to accommodate the timeline of the rapid review. I documented a low, unclear, or high level of concern for each of the four ROBIS domains using the criteria within each domain but without documenting answers to each of the sub-questions. Following the tool’s Phase 3 instructions, I combined those assessments with the three overall criteria for judging the risk of bias to arrive at the overall level of concern.
The relevant findings from the systematic reviews without a high risk of bias are summarized narratively.
Appendix B.1.2. Characteristics of Included Systematic Reviews
Table A1 summarizes the features of the systematic reviews. None of the reviews overlap closely with the present review. While the interventions covered in the reviews are broader in the sense that they are not limited to norms-based approaches, they are narrower in that they are focused on specific themes or outcomes. Most of the reviews are limited to adolescent or youth participants. While they all report at least one type of behavioral outcome, they report a large number of other outcomes as well. Because of the selection criteria that a review must report the country for each study, include studies from LMICs, and allow for separate synthesis for LMICs, the reviews are mostly limited to LMICs or even smaller geographies. None of the studies include meta-analysis, which is typically explained as due to the heterogeneity of interventions, contexts, and outcomes.
Table A1.
Features of included systematic reviews.
Table A1.
Features of included systematic reviews.
| Study ID | Title | Geography | Interventions | Participants | Behavioral Outcomes |
|---|---|---|---|---|---|
| Bourey 2015 [60] | Systematic review of structural interventions for intimate partner violence in low- and middle-income countries: organizing evidence for prevention | LMIC | Structural interventions to prevent male-perpetrated IPV including economic, social, and combined economic and social interventions | Adults | IPV incidence (or prevalence) |
| Harrison 2010 [61] | HIV prevention for South African youth: Which interventions work? A systematic review of current evidence | South Africa | In-school and out-of-school, curriculum-based HIV prevention programs for youth | Youth | Sexual and HIV risk |
| Levy 2020 [62] | Characteristics of successful programmes targeting gender inequality and restrictive gender norms for the health and wellbeing of children, adolescents, and young adults: a systematic review | Global | Community engagement and social support, economic stability, education and awareness building, physical environment | Youth | Various |
| Nikolova 2018 [63] | Review of the evidence of gender-focused interventions including men to reduce HIV risk and violence against women in sub-Saharan Africa | Sub-Saharan Africa | HIV and HIV risk programs including or focused on men that also address violence against women | Adults | HIV risk |
| Sunguya 2016 [64] | Ability of HIV advocacy to modify behavioral norms and treatment impact: A systematic review | Global | HIV advocacy interventions, e.g., media, print materials, youth outreach, social marketing | Youth and Adults | HIV risk, HIV testing |
| Temin 2020 [65] | Close to home: Evidence on the impact of community-based girl groups | LMIC | Community-based girl group programs, also known as safe spaces | Adolescents | Various |
| Wamoyi 2014 [66] | A review of interventions addressing structural drivers of adolescents’ sexual and reproductive health vulnerability in sub-Saharan Africa: implications for sexual health programming | Sub-Saharan Africa | Economic empowerment, economic empowerment plus school attendance, safe spaces, behavior-change communication | Adolescents | Various |
Table A2 reports the risk-of-bias assessment and the number of included studies. Three reviews have an unclear risk of bias, and the rest have a high risk of bias. Concerns about bias are often that the review does not include a risk-of-bias assessment or that the authors do not address the risk of bias in their synthesis. There are also concerns for several reviews that the authors extract and then count or otherwise synthesize a large number of outcomes from each study without addressing possible multiple comparisons problems. The number of included studies in these reviews ranges from 13 to 61.
Table A2.
Risk-of-bias assessment and number of included studies for systematic reviews.
Table A2.
Risk-of-bias assessment and number of included studies for systematic reviews.
| Study ID | Eligibility Criteria | Identification and Selection | Data Collection and Appraisal | Synthesis and Findings | Overall Risk of Bias | Notes | Number of Included Studies |
|---|---|---|---|---|---|---|---|
| Bourey 2015 [60] | Low | Unclear | Unclear | Unclear | Unclear | Only two indexes searched and no web search; extracted same outcomes from multiple articles of same study; risk of bias not addressed in results synthesis; emphasis of results based on statistical significance | 20 articles covering 16 programs |
| Harrison 2010 [61] | Unclear | Unclear | Unclear | High | High | Some of the exclusion criteria seem arbitrarily applied; no details about screening process; no risk-of-bias assessment | 13 articles covering 8 programs |
| Levy 2020 [62] | Low | Unclear | Unclear | High | High | Limited information on search terms and selection procedures; no risk-of-bias assessment other than methods parameters; synthesis methods not clear but emphasis on statistical significance | 61 documents covering 59 programs |
| Nikolova 2018 [63] | Low | Low | Unclear | Unclear | Unclear | Extracted same outcomes from multiple articles of same study; quality-rating methodology not clear; rating addressed in results synthesis; vote counting | 17 articles covering 13 programs |
| Sunguya 2016 [64] | Low | Low | Low | Unclear | Unclear | No summary measure risk of bias, risk of bias not addressed in results synthesis | 25 |
| Temin 2020 [65] | Low | High | High | High | High | Limited search terms produced very few initial hits; no risk-of-bias assessment; extracted large number of outcomes from each study; vote counting | 30 programs |
| Wamoyi 2014 [66] | Low | High | High | Unclear | High | Almost all screening at title level; no study design criteria; extracted large number of outcomes for each program; no risk-of-bias assessment | 21 documents covering 15 programs |
Appendix B.1.3. Systematic Review Findings
I summarize here the three systematic reviews assessed as having an unclear risk of bias.
The review by Bourey, et al. [60] looks at the evidence for structural interventions to address intimate partner violence in LMICs. The review includes 20 articles covering 16 studies. Four of the included articles are also included as primary studies in the present review [28,39,40,45]. The Bourey, et al. review design overlaps with the present review in that it includes, but is not exclusive to, norms-based interventions, and it includes, but is not exclusive to, behavior-change outcomes. It is more limited in theme and sector. It includes a broader set of study designs, including evaluations with pre-post design.
Bourey, et al.’s review question is, what is the evidence for the impact of structural interventions to prevent IPV perpetrated by men against women. The authors define four categories of structural interventions but only find studies for two of the categories—economic and social—as well as studies of programs that combine those two. The authors do not define social interventions as norms-based interventions per se, but the potential social interventions listed in their Table 1 include norms-based approaches, for example, “educational entertainment media” and “transformation of gender norms among men” (p. 3).
Bourey, et al. discuss both IPV outcomes and secondary outcomes as reported in the included studies. Not all of the IPV outcomes are behavior-change outcomes. They conclude that the reviewed studies “suggest the potential for structural interventions to reduce or prevent IPV” (p. 14). They list types of activities from studies that reported positive outcomes, but they do not extend their analysis to recommend any specific activities or interventions. They do not incorporate their risk-of-bias assessments into their synthesis of study results, but they do caution that there is a varied risk of bias among the included studies. Bourey, et al. highlight three interventions that combine economic and social components and demonstrate positive IPV outcomes. For two of the three, the social component is a participatory learning program [67,68,69,70] and for the third, gender dialogue groups for couples [71]. Several of the included studies report positive results for secondary outcomes, including changes in social norms. The review authors’ recommendations focus on the need for more rigorous evaluation and better measurement of structural interventions for IPV.
Nikolova and Small [63] review gender-focused interventions that address both HIV risk and violence against women. The review includes 17 articles covering 13 studies. Three of the included articles are included as primary studies in the present review [35,40,45]. The Nikolova and Small review design overlaps with the present review in that the interventions include, but are not exclusive to, norms-based approaches, and it includes, but is not limited to, behavioral outcomes. The sectors and themes are more limited. It includes a broader set of study designs.
Nikolova and Small’s review explores the range of interventions that combine violence against women with HIV risk, the methodological rigor of the evidence, and the effectiveness of interventions. To be included, the interventions must include men. The authors identify only one of the interventions as using social norm theory, but several others fit within the definition of norms-based approaches used in the present review as indicated by peer, community leader, and community engagement elements. The authors do not synthesize the results based on any intervention categories. Overall, they conclude that “most interventions showed positive effects” p. 87, but due to the heterogeneity in interventions and in the outcomes measured, they do not draw conclusions about which interventions are more effective. Based on the findings for non-behavioral outcomes, they cite the SASA! intervention as an example for their inference that “violence is a cultural issue that must be approached on a community (meso) level” (p. 109). The also infer that “interventions addressing sexual risk behaviors have the potential impact couple relationships and gender norms” (p. 111).
Sunguya, et al. [64] review HIV advocacy interventions globally. The review includes 25 articles covering 25 studies, one of which is included in the present review [36]. The review design overlaps with the present review in that the interventions include, but are not exclusive to, norms-based approaches, and it includes, but is not limited to, behavioral outcomes. The sector and theme are more limited. It includes a broader set of countries and a broader set of study designs.
Sunguya, et al. examine the effectiveness of HIV advocacy interventions with the objective of drawing lessons for advocacy programs to address non-communicable diseases. The interventions include a variety of activities, such as mass communication, educational materials, celebrities, and counseling. The authors categorize the studies in terms of outcomes, which they group into shifts in social norms and changes in impact. Their social norms outcomes include behavior-change outcomes, including sexual risk behaviors and health seeking, which means they are measuring descriptive social norms (i.e., what other people do) in addition to injunctive social norms. They find that HIV advocacy programs have reduced risky sexual behavior and increased health seeking, and they also find effects on self-efficacy, attitudes, and stigma. Some of the lessons that the authors draw for non-communicable disease advocacy interventions touch on norms-based approaches. They recommend enlisting at-risk people to help deliver the advocacy, because they can serve as role models. They also recommend using peer advocates and celebrities.
References
- Heise, L.; Manji, K. Social norms. In GSDRC Professional Development Reading Pack; Department for International Development: London, UK, 2016. [Google Scholar]
- Perkins, H.W.; Berkowitz, A.D. Perceiving the Community Norms of Alcohol Use among Students: Some Research Implications for Campus Alcohol Education Programming. Int. J. Addict. 1986, 21, 961–976. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, R.C.; McAlaney, J.; Bewick, B.M. A Critical Appraisal of the Social Norms Approach as an Interventional Strategy for Health-Related Behavior and Attitude Change. Front. Psychol. 2018, 9, 2180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allcott, H. Social norms and energy conservation. J. Public Econ. 2011, 95, 1082–1095. [Google Scholar] [CrossRef] [Green Version]
- Cislaghi, B.; Shakya, H. Social Norms and Adolescents’ Sexual Health: An Introduction for Practitioners Working in Low and Mid-income African countries. Afr. J. Reprod. Health 2018, 22, 38–46. [Google Scholar] [CrossRef]
- Ashburn, K.; Costenbader, B.; Igras, S.; Pirzadeh, M.; Homan, R. Social Norms Background Reader; Institute for Reproductive Health, Georgetown University: Washington, DC, USA, 2016; Available online: https://www.alignplatform.org/resources/social-norms-background-reader-0 (accessed on 11 March 2021).
- Tankard, M.E.; Paluck, E.L. Norm perception as a vehicle for social change. Soc. Issues Policy Rev. 2016, 10, 181–211. [Google Scholar] [CrossRef]
- Lundgren, R.; Uysal, J.; Barker, K.; McLarnon-Silk, C.; Shaw, B.; Greenberg, J.; Kohli, A. Social Norms Lexicon; Institute for Reproductive Health, Georgetown University for the U.S. Agency for International Development; Institute for Reproductive Health, Georgetown University: Washington, DC, USA, 2021. [Google Scholar]
- Nguyen, G.; Costenbader, E.; Plourde, K.F.; Kerner, B.; Igras, S. Scaling-up Normative Change Interventions for Adolescent and Youth Reproductive Health: An Examination of the Evidence. J. Adolesc. Health 2019, 64, S16–S30. [Google Scholar] [CrossRef] [Green Version]
- Learning Collaborative to Advance Normative Change. Identifying and Describing Approaches and Attributes of Norms-Shifting Interventions; Institute for Reproductive Health, Georgetown University: Washington, DC, USA, 2017. [Google Scholar]
- Yamin, P.; Fei, M.; Lahlou, S.; Levy, S. Using Social Norms to Change Behavior and Increase Sustainability in the Real World: A Systematic Review of the Literature. Sustainability 2019, 11, 5847. [Google Scholar] [CrossRef] [Green Version]
- Brown, A.N. An approach to rapid evidence review and what we learned when we piloted it. R&E Search for Evidence, 30 September 2020. [Google Scholar]
- Brown, A.N.; Shieh, J. What evidence in there for interventions to address the dual burden of malnutrition? A rapid review. R&E Search for Evidence, 13 October 2020. [Google Scholar]
- Brown, A.N.; Shieh, J. School-based physical activity and diet interventions can be effective for addressing obesity in children in LMICs: Evidence from systematic reviews. R&E Search for Evidence, 13 November 2020. [Google Scholar]
- Affengruber, L.; Wagner, G.; Waffenschmidt, S.; Lhachimi, S.K.; Nussbaumer-Streit, B.; Thaler, K.; Griebler, U.; Klerings, I.; Gartlehner, G. Combining abbreviated literature searches with single-reviewer screening: Three case studies of rapid reviews. Syst. Rev. 2020, 9, 162. [Google Scholar] [CrossRef]
- Featherstone, R.M.; Dryden, D.M.; Foisy, M.; Guise, J.-M.; Mitchell, M.D.; Paynter, R.A.; Robinson, K.A.; Umscheid, C.A.; Hartling, L. Advancing knowledge of rapid reviews: An analysis of results, conclusions and recommendations from published review articles examining rapid reviews. Syst. Rev. 2015, 4, 50. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Antony, J.; Zarin, W.; Strifler, L.; Ghassemi, M.; Ivory, J.; Perrier, L.; Hutton, B.; Moher, D.; Straus, S.E. A scoping review of rapid review methods. BMC Med. 2015, 13, 224. [Google Scholar] [CrossRef] [Green Version]
- Khangura, S.; Konnyu, K.; Cushman, R.; Grimshaw, J.; Moher, D. Evidence summaries: The evolution of a rapid review approach. Syst. Rev. 2012, 1, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Langlois, E.V.; Straus, S.E. (Eds.) Rapid Reviews to Strengthen Health Policy and Systems: A Practical Guide; World Health Organization: Geneva, Switzerland, 2017; p. 119.
- Brown, A.N. Rapid Evidence Review of The Effectiveness of Behavior Change Interventions That Incorporate Social Norms Approaches in Low- And Middle-Income Countries. 2020. Available online: https://osf.io/3fpnq (accessed on 28 April 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blattman, C.; Hartman, A.C.; Blair, R.A. How to promote order and property rights under weak rule of Law? An experiment in changing dispute resolution behavior through Community Education. Am. Political Sci. Rev. 2014, 108, 100–120. [Google Scholar] [CrossRef]
- Brown, A.N. Public health vs. social science: Do publication lags matter? R&E Search for Evidence, 18 December 2019. [Google Scholar]
- Shelton, J.D. The 6 domains of behavior change: The missing health system building block. Glob. Health Sci. Pract. 2013, 1, 137–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waddington, H.; Aloe, A.M.; Becker, B.J.; Djimeu, E.W.; Hombrados, J.G.; Tugwell, P.; Wells, G.; Reeves, B. Quasi-experimental study designs series-paper 6: Risk of bias assessment. J. Clin. Epidemiol. 2017, 89, 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wechsberg, W.M.; Zule, W.A.; El-Bassel, N.; Doherty, I.A.; Minnis, A.M.; Novak, S.D.; Myers, B.; Carney, T. The male factor: Outcomes from a cluster randomized field experiment with a couples-based HIV prevention intervention in a South African township. Drug Alcohol Depend. 2016, 161, 307–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speizer, I.S.; Zule, W.A.; Carney, T.; Browne, F.A.; Ndirangu, J.; Wechsberg, W.M. Changing sex risk behaviors, gender norms, and relationship dynamics among couples in Cape Town, South Africa: Efficacy of an intervention on the dyad. Soc. Sci. Med. 2018, 209, 95–103. [Google Scholar] [CrossRef]
- Kyegombe, N.; Abramsky, T.; Devries, K.M.; Starmann, E.; Michau, L.; Nakuti, J.; Musuya, T.; Heise, L.; Watts, C. The impact of SASA!, a community mobilization intervention, on reported HIV-related risk behaviours and relationship dynamics in Kampala, Uganda. J. Int. AIDS Soc. 2014, 17, 19232. [Google Scholar] [CrossRef]
- Watts, C.; Devries, K.; Kiss, L.; Abramsky, T.; Kyegombe, N.; Michau, L. The SASA! Study: A Cluster Randomised Trial to Assess the Impact of a Violence and HIV Prevention Programme in Kampala, Uganda; International Initiative for Impact Evaluation: New Delhi, India, 2015; pp. 1–34. [Google Scholar]
- Vantamay, N. “3S project”: A community-based social marketing campaign for promoting sustainable consumption behavior among youth. J. Komun. Malays. J. Commun. 2019, 35, 32–49. [Google Scholar] [CrossRef]
- Stark, L.; Seff, I.; Assezenew, A.; Eoomkham, J.; Falb, K.; Ssewamala, F.M. Effects of a Social Empowerment Intervention on Economic Vulnerability for Adolescent Refugee Girls in Ethiopia. J. Adolesc. Health 2018, 62, S15–S20. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, A.; Ferrara, E.L.; Orozco-Olvera, V.H. The Entertaining Way to Behavioral Change: Fighting HIV with MTV. 2019. Available online: http://www.nber.org/papers/w26096.pdf (accessed on 13 November 2020).
- Cowan, F.M.; Pascoe, S.J.; Langhaug, L.F.; Mavhu, W.; Chidiya, S.; Jaffar, S.; Mbizvo, M.T.; Stephenson, J.M.; Johnson, A.M.; Power, R.M.; et al. The Regai Dzive Shiri project: Results of a randomized trial of an HIV prevention intervention for youth. Aids 2010, 24, 2541–2552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueroa, M.E.; Poppe, P.; Carrasco, M.; Pinho, M.D.; Massingue, F.; Tanque, M.; Kwizera, A. Effectiveness of Community Dialogue in Changing Gender and Sexual Norms for HIV Prevention: Evaluation of the Tchova Tchova Program in Mozambique. J. Health Commun. 2016, 21, 554–563. [Google Scholar] [CrossRef] [Green Version]
- Kalichman, S.C.; Simbayi, L.C.; Cain, D.; Carey, K.B.; Carey, M.P.; Eaton, L.; Harel, O.; Mehlomakhulu, V.; Mwaba, K. Randomized community-level HIV prevention intervention trial for men who drink in South African alcohol-serving venues. Eur. J. Public Health 2013, 24, 833–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraft, J.; Hill, Z.; Membe, I.; Zhang, Y.; Meassick, E.; Monsour, M.; Maumbi, M.; Ndubani, P.; Manengu, J.; Mwinga, A. Effects of the Gama Cuulu Radio Serial Drama on HIV-Related Behavior Change in Zambia. J. Health Commun. 2012, 17, 929–945. [Google Scholar] [CrossRef] [PubMed]
- Thato, R.; Penrose, J. A Brief, Peer-Led HIV Prevention Program for College Students in Bangkok, Thailand. J. Pediatr. Adolesc. Gynecol. 2013, 26, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Christofides, N.J.; Hatcher, A.M.; Rebombo, D.; McBride, R.S.; Munshi, S.; Pino, A.; Abdelatif, N.; Peacock, D.; Levin, J.; Jewkes, R.K. Effectiveness of a multi-level intervention to reduce men’s perpetration of intimate partner violence: A cluster randomised controlled trial. Trials 2020, 21, 359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, E.; Das, M.; Tancredi, D.J.; McCauley, H.L.; Virata, M.C.; Nettiksimmons, J.; O’Connor, B.; Ghosh, S.; Verma, R. Evaluation of a gender-based violence prevention program for student athletes in Mumbai, India. J. Interpers Violence 2014, 29, 758–778. [Google Scholar] [CrossRef]
- Pulerwitz, J.; Hughes, L.; Mehta, M.; Kidanu, A.; Verani, F.; Tewolde, S. Changing Gender Norms and Reducing Intimate Partner Violence: Results from a Quasi-Experimental Intervention Study with Young Men in Ethiopia. Am. J. Public Health 2015, 105, 132–137. [Google Scholar] [CrossRef]
- Sosa-Rubi, S.; Saavedra-Avendano, B.; Piras, C.; Van Buren, S.; Bautista-Arredondo, S.; Sosa-Rubi, S.G.; Van Buren, S.J. True Love: Effectiveness of a School-Based Program to Reduce Dating Violence among Adolescents in Mexico City. Prev. Sci. 2017, 18, 804–817. [Google Scholar] [CrossRef]
- Maman, S.; Mulawa, M.I.; Balvanz, P.; Luz McNaughton Reyes, H.; Kilonzo, M.N.; Yamanis, T.J.; Singh, B.; Kajula, L.J. Results from a cluster-randomized trial to evaluate a microfinance and peer health leadership intervention to prevent HIV and intimate partner violence among social networks of Tanzanian men. PLoS ONE 2020, 15, e0230371. [Google Scholar] [CrossRef] [Green Version]
- Pettifor, A.; Lippman, S.A.; Gottert, A.; Suchindran, C.M.; Selin, A.; Peacock, D.; Maman, S.; Rebombo, D.; Twine, R.; Gómez-Olivé, F.X.; et al. Community mobilization to modify harmful gender norms and reduce HIV risk: Results from a community cluster randomized trial in South Africa. J. Int. AIDS Soc. 2018, 21, e25134. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Leight, J.; Verani, F.; Tewolde, S.; Deyessa, N. Effectiveness of a culturally appropriate intervention to prevent intimate partner violence and HIV transmission among men, women, and couples in rural Ethiopia: Findings from a cluster-randomized controlled trial. PLoS Med. 2020, 17, e1003274. [Google Scholar] [CrossRef] [PubMed]
- Wagman, J.A.; Gray, R.H.; Campbell, J.C.; Thoma, M.; Ndyanabo, A.; Ssekasanvu, J.; Nalugoda, F.; Kagaayi, J.; Nakigozi, G.; Serwadda, D.; et al. Effectiveness of an integrated intimate partner violence and HIV prevention intervention in Rakai, Uganda: Analysis of an intervention in an existing cluster randomised cohort. Lancet Glob. Health 2015, 3, e23–e33. [Google Scholar] [CrossRef] [Green Version]
- Amin, S.; Saha, J.S.; Ahmed, J.A. Skills-Building Programs to Reduce Child Marriage in Bangladesh: A Randomized Controlled Trial. J. Adolesc. Health 2018, 63, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Avdeenko, A.; Gilligan, M.J. International Interventions to Build Social Capital: Evidence from a Field Experiment in Sudan. Am. Political Sci. Rev. 2015, 109, 427–449. [Google Scholar] [CrossRef] [Green Version]
- Dhar, D.; Jain, T.; Jayachandran, S. Reshaping Adolescents’ Gender Attitudes: Evidence from a School-Based Experiment in India. 2018. Available online: http://www.nber.org/papers/w25331.pdf (accessed on 13 November 2020).
- Lundgren, R.; Gibbs, S.; Kerner, B. Does it take a village? Fostering gender equity among early adolescents in Nepal. Int. J. Adolesc. Med. Health 2018, 32, 20170164. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, L.; Stammer, E.; Derbile, E.; Dery, M.; Yahaya, W.; Gle, D.B.; Otieno, J.; Fotso, J.C. A Mixed-Methods Evaluation of a Community-Based Behavior Change Program to Improve Maternal Health Outcomes in the Upper West Region of Ghana. J. Health Commun. 2018, 23, 80–90. [Google Scholar] [CrossRef]
- Doyle, K.; Levtov, R.G.; Barker, G.; Bastian, G.G.; Bingenheimer, J.B.; Kazimbaya, S.; Nzabonimpa, A.; Pulerwitz, J.; Sayinzoga, F.; Sharma, V.; et al. Gender-transformative bandebereho couples’ intervention to promote male engagement in reproductive and maternal health and violence prevention in Rwanda: Findings from a randomized controlled trial. PLoS ONE 2018, 13, e0192756. [Google Scholar] [CrossRef] [Green Version]
- Naidoo, S.; Satorius, B.K.; de Vries, H.; Taylor, M. Verbal Bullying Changes Among Students Following an Educational Intervention Using the Integrated Model for Behavior Change. J. Sch. Health 2016, 86, 813–822. [Google Scholar] [CrossRef]
- Rijsdijk, L.E.; Bos, A.E.; Ruiter, R.A.; Leerlooijer, J.N.; De Haas, B. The World Starts with Me: A multilevel evaluation of a comprehensive sex education programme targeting adolescents in Uganda. BMC Public Health 2011, 11, 334. [Google Scholar] [CrossRef]
- Schuler, S.R.; Nanda, G.; Ramírez, L.F.; Chen, M. Interactive workshops to promote gender equity and family planning in rural communities of Guatemala: Results of a community randomized study. J. Biosoc. Sci. 2015, 47, 667–686. [Google Scholar] [CrossRef] [PubMed]
- Gottert, A.; Pulerwitz, J.; Haberland, N.; Mathebula, R.; Rebombo, D.; Spielman, K.; West, R.; Julien, A.; Twine, R.; Peacock, D.; et al. Gaining traction: Promising shifts in gender norms and intimate partner violence in the context of a community-based HIV prevention trial in South Africa. PLoS ONE 2020, 15, e0237084. [Google Scholar] [CrossRef] [PubMed]
- Homan, R. Costing of Norms-Shifting Interventions: A Primer from the Passages Project; Institute for Reproductive Health, Georgetown University for the U.S. Agency for International Development; Institute for Reproductive Health, Georgetown University: Washington, DC, USA, 2020. [Google Scholar]
- Whiting, P.; Savović, J.; Higgins, J.P.T.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R.; ROBIS Group. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Brown, A.N.; Skelly, H.J. How much evidence is there really? Mapping the evidence base for ICTD interventions. Inf. Technol. Int. Dev. 2019, 15, 16–33. [Google Scholar]
- Bourey, C.; Williams, W.; Bernstein, E.E.; Stephenson, R. Systematic review of structural interventions for intimate partner violence in low- and middle-income countries: Organizing evidence for prevention. BMC Public Health 2015, 15, 1165. [Google Scholar] [CrossRef] [Green Version]
- Harrison, A.; Newell, M.L.; Imrie, J.; Hoddinott, G. HIV prevention for South African youth: Which interventions work? A systematic review of current evidence. BMC Public Health 2010, 10, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, J.K.; Darmstadt, G.L.; Ashby, C.; Quandt, M.; Halsey, E.; Nagar, A.; Greene, M.E. Characteristics of successful programmes targeting gender inequality and restrictive gender norms for the health and wellbeing of children, adolescents, and young adults: A systematic review. Lancet Glob. Health 2020, 8, e225–e236. [Google Scholar] [CrossRef] [Green Version]
- Nikolova, S.P.; Small, E. Review of the evidence of gender-focused interventions including men to reduce HIV risk and violence against women in sub-Saharan Africa. J. HIV/AIDS Soc. Serv. 2018, 17, 87–117. [Google Scholar] [CrossRef]
- Sunguya, B.F.; Munisamy, M.; Pongpanich, S.; Junko, Y.; Jimba, M. Ability of HIV Advocacy to Modify Behavioral Norms and Treatment Impact: A Systematic Review. Am. J. Public Health 2016, 106, e1–e8. [Google Scholar] [CrossRef]
- Temin, M.; Heck, C.J. Close to home: Evidence on the impact of community-based girl groups. Glob. Health Sci. Pract. 2020, 8, 300–324. [Google Scholar] [CrossRef]
- Wamoyi, J.; Mshana, G.; Mongi, A.; Neke, N.; Kapiga, S.; Changalucha, J. A review of interventions addressing structural drivers of adolescents’ sexual and reproductive health vulnerability in sub-Saharan Africa: Implications for sexual health programming. Reprod. Health 2014, 11, 131–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jewkes, R.; Gibbs, A.; Jama-Shai, N.; Willan, S.; Misselhorn, A.; Mushinga, M.; Washington, L.; Mbatha, N.; Skiweyiya, Y. Stepping Stones and Creating Futures intervention: Shortened interrupted time series evaluation of a behavioural and structural health promotion and violence prevention intervention for young people in informal settlements in Durban, South Africa. BMC Public Health 2014, 14, 1325. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.C.; Watts, C.H.; Hargreaves, J.R.; Ndhlovu, L.X.; Phetla, G.; Morison, L.A.; Busza, J.; Porter, J.D.H.; Pronyk, P. Understanding the impact of a microfinance-based intervention on women’s empowerment and the reduction of intimate partner violence in South Africa. Am. J. Public Health 2007, 97, 1794–1802. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Ferrari, G.; Abramsky, T.; Watts, C.; Hargreaves, J.; Morison, L.; Phetla, G.; Porter, J.; Pronyk, P. Assessing the incremental effects of combining economic and health interventions: The IMAGE study in South Africa. Bull World Health Organ 2009, 87, 824–832. [Google Scholar] [CrossRef]
- Pronyk, P.M.; Hargreaves, J.R.; Kim, J.C.; Morison, L.A.; Phetla, G.; Watts, C.; Busza, J.; Porter, J.D. Effect of a structural intervention for the prevention of intimate-partner violence and HIV in rural South Africa: A cluster randomised trial. Lancet 2006, 368, 1973–1983. [Google Scholar] [CrossRef]
- Gupta, J.; Falb, K.L.; Lehmann, H.; Kpebo, D.; Xuan, Z.; Hossain, M.; Zimmerman, C.; Watts, C.; Annan, J. Gender norms and economic empowerment intervention to reduce intimate partner violence against women in rural Côte d’Ivoire: A randomized controlled pilot study. BMC Int. Health Hum. Rights 2013, 13, 46. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).