
Factors Associated with School Sports Injury among Elementary and Middle School Students in Shanghai, China

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Procedure
2.4. Statistics
3. Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Emery, C.; Tyreman, H. Sport participation, sport injury, risk factors and sport safety practices in Calgary and area junior high schools. Pediatr. Child Health 2009, 14, 439–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molcho, M.; Harel, Y.; Pickett, W.; Scheidt, P.C.; Mazur, J.; Overpeck, M.D.; Hbsc Violence and Injury Writing Group. The epidemiology of non-fatal injuries among 11-, 13- and 15-year old youth in 11 countries: Findings from the 1998 WHO-HBSC cross national survey. Int. J. Inj. Control Saf. Promot. 2006, 13, 205–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gore, G.C.; Magdalinos, H.; Pless, I.B. School Injuries and Preventive Policies and Programs. Can. J. Public Health 2004, 95, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Samuel, B.; Sheps, G.D.E. Epidemiology of school injuries: A 2-year experience in a municipal health department. Pediatrics 1987, 79, 69–75. [Google Scholar]
- Emery, C.A.; Roy, T.O.; Whittaker, J.L.; Nettel-Aguirre, A.; van Mechelen, W. Neuromuscular training injury prevention strategies in youth sport: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 865–870. [Google Scholar] [CrossRef] [Green Version]
- Vriend, I.; Gouttebarge, V.; Finch, C.F.; van Mechelen, W.; Verhagen, E.A.L.M. Intervention Strategies Used in Sport Injury Prevention Studies: A Systematic Review Identifying Studies Applying the Haddon Matrix. Sports Med. 2017, 47, 2027–2043. [Google Scholar] [CrossRef] [Green Version]
- MacKay, M.; Scanlan, A.; Olsen, L.; Reid, D.; Clark, M.; McKim, K.; Raina, P. Looking for the evidence: A systematic review of prevention strategies addressing sport and recreational injury among children and youth. J. Sci. Med. Sport 2004, 7, 58–73. [Google Scholar] [CrossRef]
- Josse, J.M.; MacKay, M.; Osmond, M.H.; MacPherson, A.K. School injury among Ottawa-Area Children: A population-based study. J. Sch. Health 2009, 79, 45–50. [Google Scholar] [CrossRef]
- MacKay, M. Playground injuries. Inj. Prev. 2003, 9, 194–196. [Google Scholar]
- Rosen, B.N.; Peterson, L. Gender differences in children’s outdoor play injuries: A review and an integration. Clin. Psychol. Rev. 1990, 10, 187–205. [Google Scholar]
- Emery, C.A. Risk factors for injury in child and adolescent sport: A systematic review of the literature. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2003, 13, 256–268. [Google Scholar] [CrossRef] [PubMed]
- Lysens, R.; Steverlynck, A.; van den Auweele, Y.; Lefevre, J.; Renson, L.; Claessens, A.; Ostyn, M. The predictability of sports injuries. Sports Med. 1984, 1, 6–10. [Google Scholar] [CrossRef]
- Bahr, R.; Holme, I. Risk factors for sports injuries—A methodological approach. Br. J. Sports Med. 2003, 37, 384–392. [Google Scholar] [CrossRef]
- Bahr, R.; Krosshaug, T. Understanding injury mechanisms: A key component of preventing injuries in sport. Br. J. Sports Med. 2005, 39, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.C.; Gao, Y.; Yang, W.D.; Cheng, F.Y.; Tang, D.C.; Li, L.P. Physical activity-related injury and its associated factors among iddle school students in Southern China. Int. J. Environ. Res. Public Health 2018, 15, 1244. [Google Scholar] [CrossRef] [Green Version]
- Tang, D.; Cai, W.; Yang, W.; Gao, Y.; Li, L. Gender-specific risk factors of physical activity-related injuries among middle school students in Southern China. Int. J. Environ. Res. Public Health 2019, 16, 2359. [Google Scholar] [CrossRef] [Green Version]
- Bronikowska, M.; Krzysztoszek, J.; Lopatka, M.; Ludwixzak, M.; Pluta, B. Comparison of physical activity levels in youths before and during a pandemic lockdown. Int. J. Environ. Res. Public Health 2021, 18, 5139. [Google Scholar] [CrossRef]
- Richmond, S.A.; Kang, J.; Doyle-Baker, P.K.; Nettel-Aguirre, A.; Emery, C.A. A School-Based Injury Prevention Program to Reduce Sport Injury Risk and Improve Healthy Outcomes in Youth: A Pilot Cluster-Randomized Controlled Trial. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2016, 26, 291–298. [Google Scholar] [CrossRef]
- Emery, C.A.; Cassidy, J.D.; Klassen, T.P.; Rosychuk, R.J.; Rowe, B.H. Effectiveness of a home-based balance-training program in reducing sports-related injuries among healthy adolescents: A cluster randomized controlled trial. CMAJ Can. Med. Assoc. J. 2005, 172, 749–754. [Google Scholar] [CrossRef] [Green Version]
- Nauta, J.; Knol, D.L.; Adriaensens, L.; Klein Wolt, K.; van Mechelen, W.; Verhagen, E.A. Prevention of fall-related injuries in 7-year-old to 12-year-old children: A cluster randomised controlled trial. Br. J. Sports Med. 2013, 47, 909–913. [Google Scholar] [CrossRef]
- Joseph, F.; Hair, J.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 8th ed.; Cengage Learning EMEA: Andover, UK, 2019. [Google Scholar]
- Deits, J.; Yard, E.E.; Collins, C.L.; Fields, S.K.; Comstock, R.D. Patients with ice hockey injuries presenting to US emergency departments, 1990–2006. J. Athl. Train. 2010, 45, 467–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilchrist, J.; Haileyesus, T.; Murphy, M.W.; Yard, E.E. Nonfatal sports and recreation heat illness treated in hospital emergency departments—United States, 2001–2009. MMWR Morb. Mortal. Wkly. Rep. 2011, 60, 977–980. [Google Scholar]
- Theisen, D.; Malisoux, L.; Seil, R.; Urhausen, A. Injuries in Youth Sports: Epidemiology, Risk Factors and Prevention. /Verletzungen im Jugendsport: Epidemiologie, Risikofaktoren und Prävention. Ger. J. Sports Med./Dtsch. Z. Sportmed. 2014, 65, 248–252. [Google Scholar]


{kind=link}
| Items | Domain | Factors | Direction |
|---|---|---|---|
| 1. I will perform physical activities on slippery ground. | External | Facility | Positive |
| 2. I will perform physical activities on uneven ground. | External | Facility | Positive |
| 3. I will perform physical activities in places with poor light. | External | Facility | Positive |
| 4. I will perform physical activities in small venues. | External | Facility | Positive |
| 5. I will perform physical activities in crowded venues. | External | Facility | Positive |
| 6. I will do outdoor physical activities during hot weather. | External | Playing Time | Positive |
| 7. I will do outdoor physical activities when the weather is very cold. | External | Playing Time | Positive |
| 8. I will be physically active when I am sick. | External | Playing Time | Positive |
| 9. I will run and chase on campus. | Internal | Safety Awareness | Positive |
| 10. I will wear necklaces and other accessories during sports activities. | Internal | Safety Awareness | Positive |
| 11. I will wear glasses during sports activities. | Internal | Safety Awareness | Positive |
| 12. When participating in physical activities, I will pay attention to my pulse or heartbeat and other physical conditions. | Internal | Safety Awareness | Negative |
| 13. I will abide by the rules and pay attention to the safety of others when performing physical activities or competitions. | Internal | Safety Awareness | Negative |
| 14. During exercise, if I feel dizzy, I will stop exercising immediately. | Internal | Safety Knowledge | Negative |
| 15. Before exercise or competitions, I will pay attention to maintaining a good sleep to conserve energy. | Internal | Safety Knowledge | Negative |
| 16. Right after the 800-meter race and other strenuous exercises, I will sit down and rest immediately. | Internal | Safety Knowledge | Positive |
| 17. When an ankle is sprained, I will take quick measures, such as applying an ice pack to the wound. | Internal | Safety Knowledge | Negative |
| 18. I will play sports on facilities or equipment with potential safety hazards. | Internal | Safety Awareness | Positive |
| 19. During the exercise, I will drink water regularly. | Internal | Safety Knowledge | Negative |
| Characteristics 1 | All (N =1303) n (%) | Non-SSI (N = 918) n (%) | SSI (N = 385) n (%) | χ2/t * | p-Value 3 |
|---|---|---|---|---|---|
| Gender | 8.949 | 0.003 ** | |||
| Boy | 685 (52.6) | 458 (66.9) | 227 (33.1) | ||
| Girl | 618 (47.4) | 460 (74.4) | 158 (25.6) | ||
| Study Year | 74.993 | 0.000 *** | |||
| Elementary school | 676 (51.9) | 405 (59.9) | 271 (40.1) | ||
| Middle school | 627 (48.1) | 513 (81.8) | 114 (18.2) | ||
| Parental marital status | 3.383 | 0.184 | |||
| Married | 1172 (89.9) | 831 (70.9) | 341 (29.1) | ||
| Divorced/Separated | 122 (9.4) | 83 (68.0) | 39 (32.0) | ||
| Others | 9 (0.7) | 4 (44.4) | 5 (55.6) | ||
| Sports team member | 13.086 | 0.000 *** | |||
| No | 1078 (82.7) | 782 (72.5) | 296 (27.5) | ||
| Yes | 225 (17.3) | 136 (60.4) | 89 (39.6) | ||
| Sleep duration | 28.644 | 0.000 *** | |||
| <7 h/d | 130 (10.0) | 101 (77.7) | 29 (22.3) | ||
| 7–<8 h/d | 273 (21.0) | 221 (81.0) | 52 (19.0) | ||
| 8–<9 h/d | 406 (31.2) | 281 (69.2) | 125 (30.8) | ||
| ≥9.00 h/d | 494 (37.8) | 315 (63.8) | 179 (36.2) | ||
| Chronic disease/symptom | 3.349 | 0.067 | |||
| No | 1282 (98.4) | 907 (70.7) | 375 (29.3) | ||
| Yes | 21 (1.6) | 11 (52.4) | 10 (47.6) | ||
| Living in a school dormitory | 1.349 | 0.246 | |||
| No | 1292 (99.2) | 912 (70.6) | 380 (29.4) | ||
| Yes | 11 (0.8) | 6 (54.5) | 5 (45.5) | ||
| Nearsightedness | 10.758 | 0.001 ** | |||
| No | 606 (46.5) | 400 (66.0) | 206 (34.0) | ||
| Yes | 697 (53.5) | 518 (74.3) | 179 (25.7) | ||
| Only child family | 7.639 | 0.006 ** | |||
| No | 760 (58.3) | 513 (67.5) | 247 (32.5) | ||
| Yes | 543 (41.7) | 405 (74.6) | 138 (25.4) | ||
| Age (x ± s, years) | 12.10 ± 1.85 | 12.38 ± 1.86 | 11.43 ± 1.65 | 8.717 | 0.000 *** |
| BMI 2 (x ± s, kg/m2) | 19.56 ± 4.50 | 19.67 ± 4.46 | 19.34 ± 4.93 | 1.202 | 0.230 |
| Internal risk factors | 2.02 ± 0.85 | 1.99 ± 0.85 | 2.11 ± 0.87 | −2.400 | 0.017 * |
| External risk factors | 1.90 ± 1.10 | 1.84 ± 1.04 | 2.05 ± 1.20 | −3.126 | 0.002 ** |
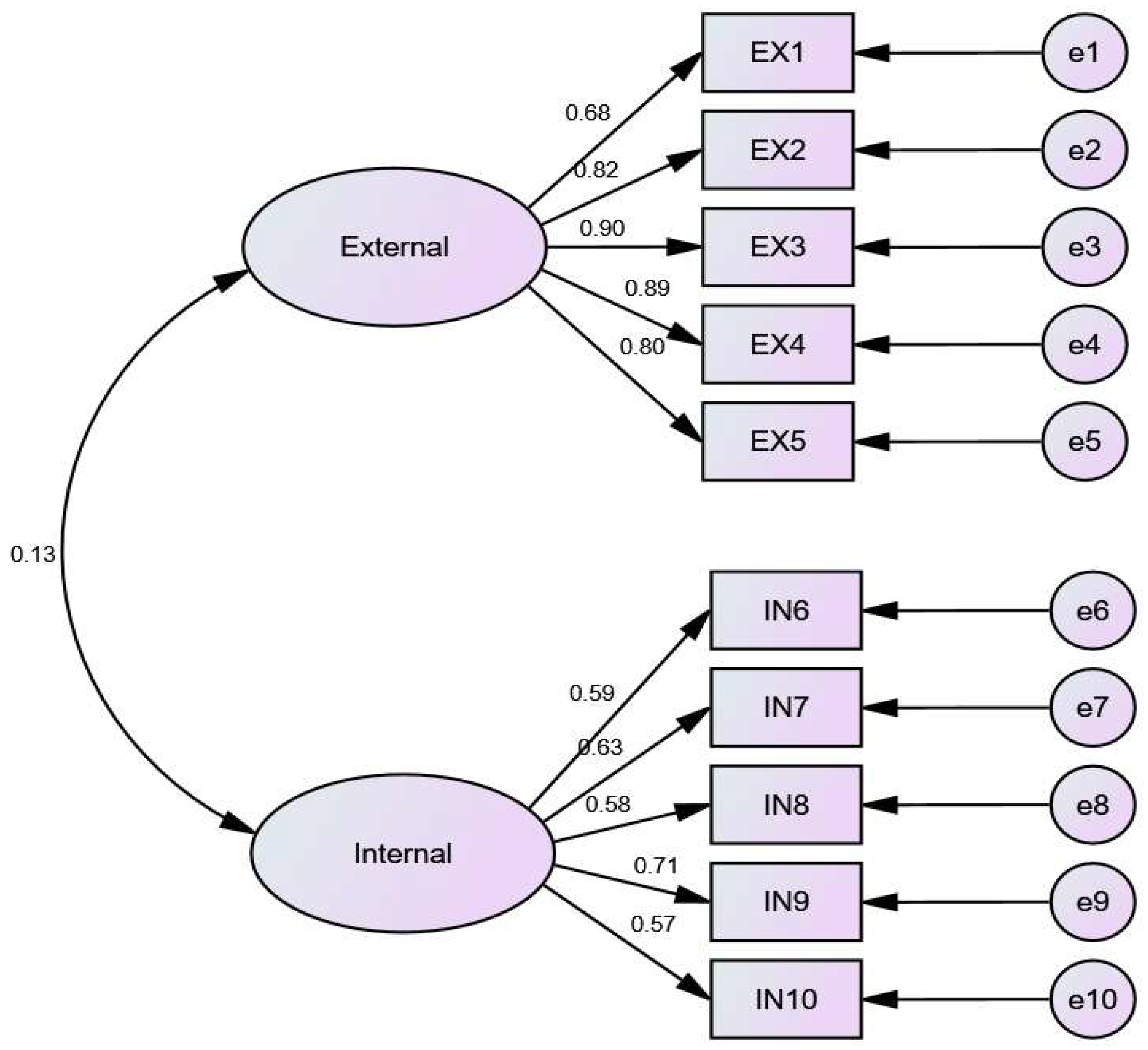
| Items | Mean | SD | FL |
|---|---|---|---|
| EX1. I will perform physical activities on slippery ground. | 3.94 | 1.416 | 0.797 |
| EX2. I will perform physical activities on uneven ground. | 4.09 | 1.316 | 0.858 |
| EX3. I will perform physical activities in places with poor light. | 4.09 | 1.241 | 0.871 |
| EX4. I will perform physical activities in small venues. | 4.16 | 1.260 | 0.856 |
| EX5. I will perform physical activities in crowded venues. | 4.20 | 1.199 | 0.836 |
| IN6. When participating in physical activities, I will pay attention to my pulse or heartbeat and other physical conditions. | 3.38 | 1.332 | 0.627 |
| IN7. I will abide by the rules and pay attention to the safety of others when performing physical activities or competitions. | 4.27 | 1.058 | 0.662 |
| IN8. During exercise, if I feel dizzy, I will stop exercising immediately. | 3.83 | 1.291 | 0.625 |
| IN9. Before exercise or competitions, I will pay attention to maintaining a good sleep to conserve energy. | 4.12 | 1.101 | 0.792 |
| IN10. When an ankle is sprained, I will take quick measures, such as applying an ice pack to the wound. | 3.77 | 1.326 | 0.640 |
| Model Fit Index | Value Considered Good Fit | Model Fit Value | Indication of Fit |
|---|---|---|---|
| χ2/df | Value lower than 3 | 6.155 | Acceptable |
| RMSEA | 0.03–0.08 | 0.073 | Reasonable |
| CFI | Value > 0.9 | 0.960 | Perfect |
| AGFI | Value > 0.9 | 0.930 | Good |
| GFI | Value > 0.9 | 0.956 | Perfect |
| NFI | Value > 0.9 | 0.953 | Perfect |
| RMR | Value < 0.05 | 0.057 | Acceptable |
| IFI | Value > 0.9 | 0.960 | Perfect |
| Characteristics | β | Wald | p-Value | Adjusted OR | 95% CI |
|---|---|---|---|---|---|
| Gender | |||||
| Girl | 1 | ||||
| Boy | 0.312 | 5.530 | 0.019 * | 1.367 | 1.053–1.773 |
| Study year | |||||
| Elementary | 1 | ||||
| Middle | −0.670 | 5.455 | 0.020 * | 0.512 | 0.292–0.898 |
| Parental marital status | |||||
| Married | 1 | ||||
| Divorced/Separated | 0.366 | 2.703 | 0.100 | 1.443 | 0.932–2.233 |
| Others | 1.356 | 3.663 | 0.056 | 3.882 | 0.968–15.568 |
| Sport team | |||||
| No | 1 | ||||
| Yes | 0.524 | 10.569 | 0.001 ** | 1.689 | 1.231–2.317 |
| Sleep Duration | |||||
| <7 h/d | 1 | ||||
| 7–<8 h/d | −0.227 | 0.688 | 0.407 | 0.797 | 0.466–1.363 |
| 8–<9 h/d | 0.122 | 0.226 | 0.634 | 1.130 | 0.683–1.870 |
| ≥9.00 h/d | 0.100 | 0.143 | 0.705 | 1.105 | 0.658–1.855 |
| Chronic disease/symptom | |||||
| No | 1 | ||||
| Yes | 0.716 | 2.393 | 0.122 | 2.047 | 0.826–5.073 |
| School dormitory residence | |||||
| No | 1 | ||||
| Yes | 0.243 | 0.146 | 0.703 | 1.275 | 0.366–4.438 |
| Nearsightedness | |||||
| No | 1 | ||||
| Yes | −0.037 | 0.074 | 0.785 | 0.964 | 0.740–1.255 |
| Only child | |||||
| No | |||||
| Yes | −0.047 | 0.114 | 0.736 | 0.954 | 0.727–1.252 |
| Age (years) | −0.120 | 2.337 | 0.126 | 0.887 | 0.760–1.034 |
| BMI 1 (kg/m2) | 0.004 | 0.095 | 0.758 | 1.004 | 0.977–1.032 |
| External Factors | 0.133 | 5.419 | 0.020 * | 1.142 | 1.021–1.277 |
| Internal Factors | 0.227 | 9.187 | 0.002 ** | 1.255 | 1.084–1.454 |
| Characteristics | All (N = 385) N(%) | Gender | χ2 | p-Value | |
|---|---|---|---|---|---|
| Boys (N = 223) n (%) | Girls (N = 156) n (%) | ||||
| Number of SSI | 0.114 | 0.945 | |||
| 1 | 250 (64.9) | 146 (64.3) | 104 (65.8) | ||
| 2 | 86 (22.3) | 52 (22.9) | 34 (21.5) | ||
| ≥3 | 49 (12.7) | 29 (12.8) | 20 (12.7) | ||
| Consequences of SSI | |||||
| Immediately stop the SSA | 2.626 | 0.105 | |||
| No | 170 (44.2) | 108 (47.6) | 62 (39.2) | ||
| Yes | 215 (55.8) | 119 (52.4) | 96 (60.8) | ||
| Absent from the next SSA | 0.453 | 0.501 | |||
| No | 299 (77.7) | 179 (78.9) | 120 (75.9) | ||
| Yes | 86 (22.3) | 48 (21.1) | 38 (24.1) | ||
| Class absence next day | 1.982 | 0.159 | |||
| No | 343 (89.1) | 198 (87.2) | 145 (91.8) | ||
| Yes | 42 (10.9) | 29 (12.8) | 13 (8.2) | ||
| See a doctor or hospitalization | 4.296 | 0.038 * | |||
| No | 343 (89.1) | 193 (86.3) | 147 (93.0) | ||
| Yes | 42 (10.9) | 31 (13.7) | 11 (7.0) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, L.; Brewer, B.W.; Mackey, M.; Cai, H.; Zhang, J.; Song, Y.; Cai, Q. Factors Associated with School Sports Injury among Elementary and Middle School Students in Shanghai, China. Int. J. Environ. Res. Public Health 2022, 19, 6406. https://doi.org/10.3390/ijerph19116406
Ding L, Brewer BW, Mackey M, Cai H, Zhang J, Song Y, Cai Q. Factors Associated with School Sports Injury among Elementary and Middle School Students in Shanghai, China. International Journal of Environmental Research and Public Health. 2022; 19(11):6406. https://doi.org/10.3390/ijerph19116406
Chicago/Turabian StyleDing, Liyi, Britton W. Brewer, Marcia Mackey, Hao Cai, Jianqiang Zhang, Yudong Song, and Qunhui Cai. 2022. "Factors Associated with School Sports Injury among Elementary and Middle School Students in Shanghai, China" International Journal of Environmental Research and Public Health 19, no. 11: 6406. https://doi.org/10.3390/ijerph19116406
APA StyleDing, L., Brewer, B. W., Mackey, M., Cai, H., Zhang, J., Song, Y., & Cai, Q. (2022). Factors Associated with School Sports Injury among Elementary and Middle School Students in Shanghai, China. International Journal of Environmental Research and Public Health, 19(11), 6406. https://doi.org/10.3390/ijerph19116406