
Exercise Capacity and Cardiorespiratory Fitness in Children with Congenital Heart Diseases: A Proposal for an Adapted NYHA Classification

 , , , ,
, , , ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Functional Classification
- Do you feel you are limited during physical activities or exercise compared to your peers?
- Would an external viewer notice some differences in your performance compared to your peers or teammates?
- Does it happen that you feel any kind of functional limitation during vigorous physical activities or exercise (i.e., physical activities or exercise where the intensity is such that it is impossible to speak—RPE 18/20 on Borg scale)?
2.2. Cardiopulmonary Exercise Testing
2.3. Statistical Analyses
3. Results
4. Discussion
4.1. Limitations
4.2. Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moons, P.; Bovijn, L.; Budts, W.; Belmans, A.; Gewillig, M. Temporal Trends in Survival to Adulthood among Patients Born with Congenital Heart Disease from 1970 to 1992 in Belgium. Circulation 2010, 122, 2264–2272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wren, C.; O’sullivan, J.J. Survival with Congenital Heart Disease and Need for Follow up in Adult Life. Heart 2001, 85, 438–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buys, R.; Cornelissen, V.; van de Bruaene, A.; Stevens, A.; Coeckelberghs, E.; Onkelinx, S.; Thomaes, T.; Delecluse, C.; Budts, W.; Vanhees, L. Measures of Exercise Capacity in Adults with Congenital Heart Disease. Int. J. Cardiol. 2011, 153, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Bredy, C.; Ministeri, M.; Kempny, A.; Alonso-Gonzalez, R.; Swan, L.; Uebing, A.; Diller, G.P.; Gatzoulis, M.A.; Dimopoulos, K. New York Heart Association (NYHA) Classification in Adults with Congenital Heart Disease: Relation to Objective Measures of Exercise and Outcome. Eur. Heart J. Qual. Care Clin. Outcomes 2018, 4, 51–58. [Google Scholar] [CrossRef]
- Baumgartner, H.; de Backer, J.; Babu-Narayan, S.V.; Budts, W.; Chessa, M.; Diller, G.P.; Iung, B.; Kluin, J.; Lang, I.M.; Meijboom, F.; et al. 2020 ESC Guidelines for the Management of Adult Congenital Heart Disease. Eur. Heart J. 2021, 42, 563–645. [Google Scholar] [CrossRef]
- Schwerzmann, M.; Goossens, E.; Gallego, P.; Kovacs, A.H.; Moons, P.; Swan, L.; Tobler, D.; de Stoutz, N.; Gabriel, H.; Greutmann, M.; et al. Recommendations for Advance Care Planning in Adults with Congenital Heart Disease: A Position Paper from the ESC Working Group of Adult Congenital Heart Disease, the Association of Cardiovascular Nursing and Allied Professions (ACNAP), the European Association for Palliative Care (EAPC), and the International Society for Adult Congenital Heart Disease (ISACHD). Eur. Heart J. 2020, 41, 4200–4210. [Google Scholar]
- Fredriksen, M.; Veldtman, G.; Hechter, S.; Therrien, J.; Chen, A.; Warsi, M.A.; Freeman, M.; Liu, P.; Siu, S.; Thaulow, E.; et al. Aerobic Capacity in Adults with Various Congenital Heart Diseases. Am. J. Cardiol. 2001, 87, 310–314. [Google Scholar] [CrossRef]
- Budts, W.; Pieles, G.E.; Roos-Hesselink, J.W.; de La Garza, M.S.; D’Ascenzi, F.; Giannakoulas, G.; Müller, J.; Oberhoffer, R.; Ehringer-Schetitska, D.; Herceg-Cavrak, V.; et al. Recommendations for Participation in Competitive Sport in Adolescent and Adult Athletes with Congenital Heart Disease (CHD): Position Statement of the Sports Cardiology Exercise Section of the European Association of Preventive Cardiology (EAPC), the European Society of Cardiology (ESC) Working Group on Adult Congenital Heart Disease and the Sports Cardiology, Physical Activity and Prevention Working Group of the Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 2020, 41, 4191–4199. [Google Scholar]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2016, 74, 1037–1147. [Google Scholar]
- Mosterd, A.; Hoes, A.W. Clinical Epidemiology of Heart Failure. Heart 2007, 93, 1137–1146. [Google Scholar] [CrossRef] [Green Version]
- Thibodeau, J.T.; Mishkin, J.D.; Patel, P.C.; Mammen, P.P.A.; Markham, D.W.; Drazner, M.H. IIIB or Not IIIB: A Previously Unanswered Question. J. Card. Fail. 2012, 18, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Longmuir, P.E.; Brothers, J.A.; de Ferranti, S.D.; Hayman, L.L.; van Hare, G.F.; Matherne, G.P.; Davis, C.K.; Joy, E.A.; McCrindle, B.W. Promotion of Physical Activity for Children and Adults with Congenital Heart Disease: A Scientific Statement from the American Heart Association. Circulation 2013, 127, 2147–2159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, D.A.; Liu, P.; Walters, J.E.; Goodman, J.M.; Siu, S.C.; Webb, G.D.; Williams, W.G.; McLaughlin, P.R.; Toronto, F. Cardiopulmonary function in adult patients late after Fontan repair. J. Am. Coll. Cardiol. 1995, 26, 1016–1021. [Google Scholar] [CrossRef] [Green Version]
- Diller, G.P.; Dimopoulos, K.; Okonko, D.; Li, W.; Babu-Narayan, S.V.; Broberg, C.S.; Johansson, B.; Bouzas, B.; Mullen, M.J.; Poole-Wilson, P.A.; et al. Exercise Intolerance in Adult Congenital Heart Disease: Comparative Severity, Correlates, and Prognostic Implication. Circulation 2005, 112, 828–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vecchiato, M.; Neunhaeuserer, D.; Quinto, G.; Bettini, S.; Gasperetti, A.; Battista, F.; Vianello, A.; Vettor, R.; Busetto, L.; Ermolao, A. Cardiopulmonary exercise testing in patients with moderate-severe obesity: A clinical evaluation tool for OSA? Sleep Breath. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Baba, R.; Nagashima, M.; Goto, M.; Nagano, Y.; Yokota, M.; Tauchi, N.; Nishibata, K. Oxygen Uptake Efficiency Slope: A New Index of Cardiorespiratory Functional Reserve Derived from the Relation between Oxygen Uptake and Minute Ventilation during Incremental Exercise. J. Am. Coll. Cardiol. 1996, 28, 1567–1572. [Google Scholar] [CrossRef]
- Paolillo, S.; Agostoni, P. Prognostic Role of Cardiopulmonary Exercise Testing in Clinical Practice. In Proceedings of the Annals of the American Thoracic Society. Am. Thorac. Soc. 2017, 14, S53–S58. [Google Scholar] [CrossRef]
- Holland, R.; Rechel, B.; Stepien, K.; Harvey, I.; Brooksby, I. Patients’ Self-Assessed Functional Status in Heart Failure by New York Heart Association Class: A Prognostic Predictor of Hospitalizations, Quality of Life and Death. J. Card. Fail. 2010, 16, 150–156. [Google Scholar] [CrossRef]
- Fredriksen, M.; Therrien, J.; Veldtman, G.; Warsi, M.A.; Liu, P.; Thaulow, E.; Webb, G. Aerobic Capacity in Adults with Tetralogy of Fallot. Cardiol. Young 2002, 12, 554–559. [Google Scholar] [CrossRef]
- Gläser, S.; Opitz, C.F.; Bauer, U.; Wensel, R.; Ewert, R.; Lange, P.E.; Kleber, F.X. Assessment of Symptoms and Exercise Capacity in Cyanotic Patients with Congenital Heart Disease. Chest 2004, 125, 368–376. [Google Scholar] [CrossRef] [Green Version]
- Trojnarska, O.; Gwizdala, A.; Lanocha, M.; Katarzynska, A.; Katarzynski, S.; Oko-Sarnowska, Z.; Szyszka, A.; Chmara, E. Exercise Testing in Adults after Repair of Aortic Coarctation Evaluation of Cardiopulmonary Exercise Capacity and B-Type Natriuretic Protein Levels. Clin. Investig. 2007, 34, 412. [Google Scholar]
- Trojnarska, O.; Gwizdała, A.; Katarzyński, S.; Katarzyńska, A.; Oko-Sarnowska, Z.; Brȩborowicz, P.; Grajek, S. Evaluation of Exercise Capacity with Cardiopulmonary Exercise Testing and BNP Levels in Adult Patients with Single or Systemic Right Ventricles. Arch. Med. Sci. 2010, 6, 192–197. [Google Scholar] [CrossRef]
- Giardini, A.; Khambadkone, S.; Rizzo, N.; Riley, G.; Napoleone, C.P.; Muthialu, N.; Picchio, F.M.; Derrick, G. Determinants of Exercise Capacity After Arterial Switch Operation for Transposition of the Great Arteries. Am. J. Cardiol. 2009, 104, 1007–1012. [Google Scholar] [CrossRef]
- Gavotto, A.; Abassi, H.; Rola, M.; Serrand, C.; Picot, M.C.; Iriart, X.; Thambo, J.B.; Iserin, L.; Ladouceur, M.; Bredy, C.; et al. Factors Associated with Exercise Capacity in Patients with a Systemic Right Ventricle. Int. J. Cardiol. 2019, 292, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.D.; Saval, M.A.; Robbins, J.L.; Ellestad, M.H.; Gottlieb, S.S.; Handberg, E.M.; Zhou, Y.; Chandler, B. New York Heart Association Functional Class Predicts Exercise Parameters in the Current Era. Am. Heart J. 2009, 158, S24–S30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, B.B.; Young, M.L.; Niu, J.; Mendoza, L.E.; Chan, K.C.; Roth, T. Relation Between New York Heart Association Functional Class and Objective Measures of Cardiopulmonary Exercise in Adults with Congenital Heart Disease. Am. J. Cardiol. 2019, 123, 1868–1873. [Google Scholar] [CrossRef] [PubMed]
- Spoladore, R.; Fragasso, G.; Montanaro, C.; D’Amato, R.; Palloshi, A.; Salerno, A.; Arioli, F.; Margonato, A. NYHA Class II subgrouping: Correlation with left ventricular dysfunction questionnaire (LVD-36) and ejection fraction. Minerva Cardioangiol. 2010, 58, 441–448. [Google Scholar] [CrossRef]
- Handler, S.S.; Hallis, B.J.; Tillman, K.A.; Krolikowski, M.; Kuhn, E.M.; Kirkpatrick, E.C.; Brosig, C.L. Assessment of quality of life in pediatric patients with pulmonary hypertension. Pulm. Circ. 2019, 9, 2045894018822985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guimarães, G.V.; d’Avila, V.M.; Camargo, P.R.; Moreira, L.F.; Lanz, J.R.; Bocchi, E.A. Prognostic value of cardiopulmonary exercise testing in children with heart failure secondary to idiopathic dilated cardiomyopathy in a non-beta-blocker therapy setting. Eur. J. Heart Fail. 2008, 10, 560–565. [Google Scholar] [CrossRef]
- Guazzi, M.; Adams, V.; Conraads, V.; Halle, M.; Mezzani, A.; Vanhees, L.; Arena, R.; Fletcher, G.F.; Forman, D.E.; Kitzman, D.W.; et al. Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations. Circulation 2012, 126, 2261–2274. [Google Scholar] [CrossRef]
- Ermolao, A.; Gasperetti, A.; Rigon, A.; Patti, A.; Battista, F.; Frigo, A.C.; Duregon, F.; Zaccaria, M.; Bergamin, M.; Neunhaeuserer, D. Comparison of Cardiovascular Screening Guidelines for Middle-Aged/Older Adults. Scand. J. Med. Sci. Sports 2019, 29, 1375–1382. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| NYHA I (n = 235) | NYHA IIA (n = 66) | NYHA IIB (n = 31) | I vs. IIA | I vs. IIB | IIA vs. IIB | |
|---|---|---|---|---|---|---|
| Age (years) | 13 (11.0–15.0) | 14 (11.8–15.0) | 13 (11.0–15.0) | 0.290 | ||
| Gender (male %) | 163 (70) | 38 (57.6) | 19 (61.3) | 0.060 | 0.327 | 0.729 |
| BMI (kg/m2) | 19.3 ± 3.4 | 19.7 ± 2.3 | 18.4 ± 3.7 | 1.000 | 0.521 | 0.258 |
| BMI (percentiles) | 47.7 ± 29.7 | 49.3 ± 32.9 | 46.1 ± 32.2 | 0.933 | 0.955 | 0.881 |
| Resting HR (bpm) | 67 (60–75) | 70 (63–81) | 74 (67–82) | 0.042 | 0.001 | 0.127 |
| HR max (bpm) | 190 (181–196) | 176 (159–187) | 162 (139–181) | <0.001 | < 0.001 | 0.083 |
| HR max (% of predicted) | 91 (87–94) | 86 (77–90) | 79 (67–87) | <0.001 | <0.001 | 0.054 |
| HR Reserve (bpm) | 120 (111–130) | 105 (95–116) | 88 (67–99) | <0.001 | <0.001 | 0.023 |
| Exercise time (min:sec) | 11:54 ± 1:46 | 10:25 ± 1:56 | 8:34 ± 2:14 | <0.001 | <0.001 | <0.001 |
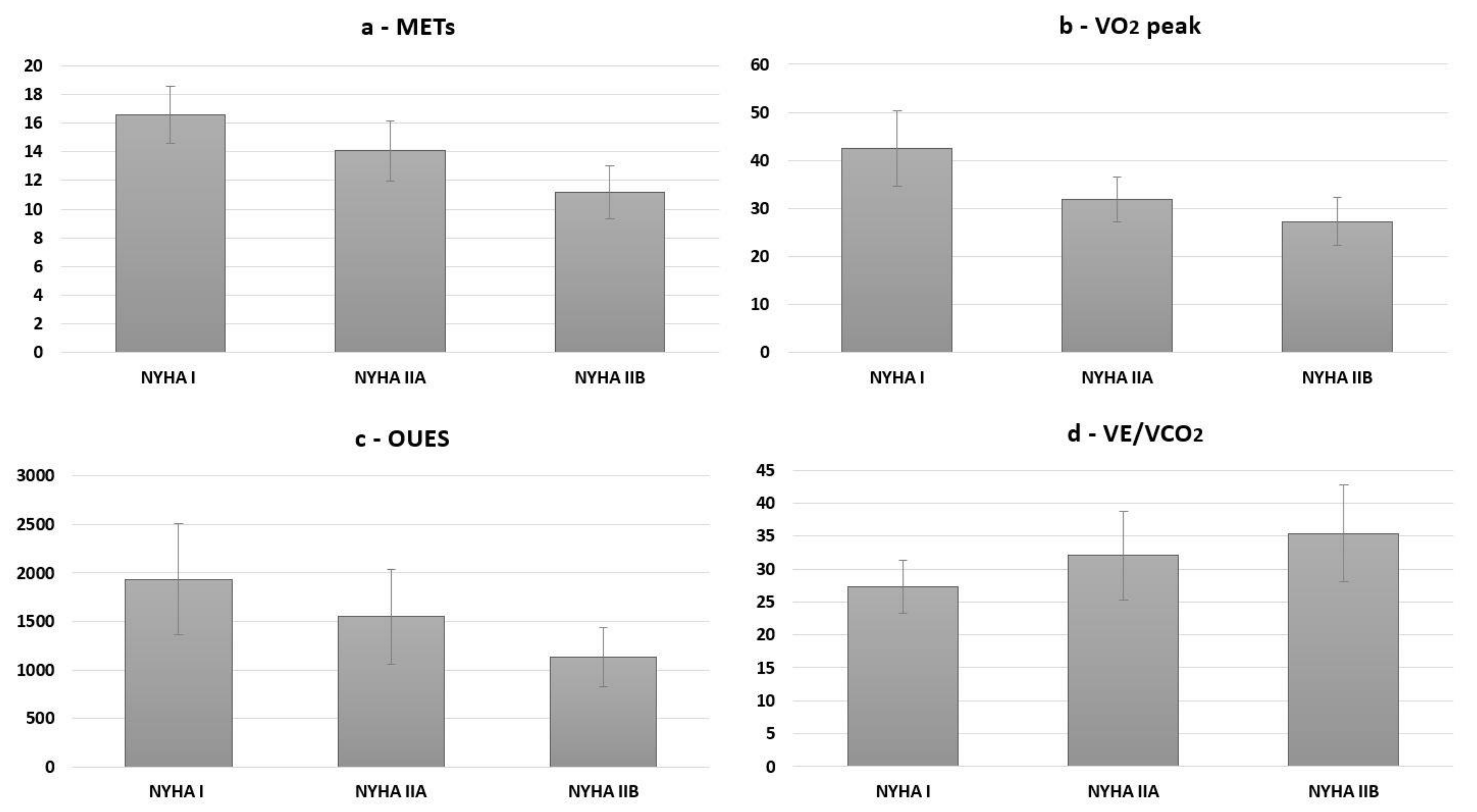
| METs max | 16.8 (15.3–17.8) | 13.9 (13.1–15.5) | 11.0 (10.0–12.7) | <0.001 | <0.001 | <0.001 |
| VO2 peak (l/min) | 1.93 (1.55–2.46) | 1.58 (1.23–1.85) | 1.18 (0.91–1.44) | <0.001 | <0.001 | 0.001 |
| VO2 peak (ml/kg/min) | 42.4 ± 7.8 | 31.9 ± 4.7 | 27.3 ± 5.0 | <0.001 | <0.001 | 0.010 |
| OUES (n = 319) | 1848 (1554–2290) | 1479 (1276–1826) | 1057 (867–1399) | <0.001 | <0.001 | 0.001 |
| PETCO2 at anaerobic threshold (mmHg) (n = 321) | 37.8 (35.4–39.9) | 33.5 (29.7–36.7) | 28.7 (26.3–34.7) | <0.001 | <0.001 | 0.079 |
| VE/VCO2 at anaerobic threshold (n = 321) | 26.8 (24.7–29.2) | 31.0 (27.7–34.8) | 34.8 (28.0–40.5) | <0.001 | <0.001 | 0.129 |
| VE/VCO2 at peak exercise (n = 321) | 31.4 (28–33.5) | 35.6 (28.9–42.1) | 37.3 (31.4 – 45.1) | <0.001 | <0.001 | 0.178 |
| SpO2 at rest (%) (n = 329) | 100 (99–100) | 98 (96–100) | 98 (94–100) | <0.001 | <0.001 | 0.104 |
| Peak SpO2 (%) (n = 322) | 98 (97–99) | 95 (91–98) | 93 (87–98) | <0.001 | <0.001 | 0.531 |
| SYMPTOMS | ||
|---|---|---|
| NYHA I | Always asymptomatic. Physical activity and exercise do not cause fatigue, palpitations and dyspnea, even when performed at strenuous intensity or compared to their peers. | |
| NYHA II | IIA | Asymptomatic for every-day life activities but show a slight limitation to competitive physical exercise among peers during leisure time activities and sports as well as at high intensity efforts. |
| IIB | Slight limitation during physical activity. No symptoms at rest. Ordinary activities cause fatigue, palpitations or dyspnea. | |
| NYHA III | Marked limitation in physical activity due to symptoms, even during less-than-ordinary activity. Comfortable only at rest. | |
| NYHA IV | Severe limitations. Experiences symptoms even while at rest. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neunhaeuserer, D.; Battista, F.; Mazzucato, B.; Vecchiato, M.; Meneguzzo, G.; Quinto, G.; Niebauer, J.; Gasperetti, A.; Vida, V.; Di Salvo, G.; et al. Exercise Capacity and Cardiorespiratory Fitness in Children with Congenital Heart Diseases: A Proposal for an Adapted NYHA Classification. Int. J. Environ. Res. Public Health 2022, 19, 5907. https://doi.org/10.3390/ijerph19105907
Neunhaeuserer D, Battista F, Mazzucato B, Vecchiato M, Meneguzzo G, Quinto G, Niebauer J, Gasperetti A, Vida V, Di Salvo G, et al. Exercise Capacity and Cardiorespiratory Fitness in Children with Congenital Heart Diseases: A Proposal for an Adapted NYHA Classification. International Journal of Environmental Research and Public Health. 2022; 19(10):5907. https://doi.org/10.3390/ijerph19105907
Chicago/Turabian StyleNeunhaeuserer, Daniel, Francesca Battista, Barbara Mazzucato, Marco Vecchiato, Giulia Meneguzzo, Giulia Quinto, Josef Niebauer, Andrea Gasperetti, Vladimiro Vida, Giovanni Di Salvo, and et al. 2022. "Exercise Capacity and Cardiorespiratory Fitness in Children with Congenital Heart Diseases: A Proposal for an Adapted NYHA Classification" International Journal of Environmental Research and Public Health 19, no. 10: 5907. https://doi.org/10.3390/ijerph19105907
APA StyleNeunhaeuserer, D., Battista, F., Mazzucato, B., Vecchiato, M., Meneguzzo, G., Quinto, G., Niebauer, J., Gasperetti, A., Vida, V., Di Salvo, G., Varnier, M., & Ermolao, A. (2022). Exercise Capacity and Cardiorespiratory Fitness in Children with Congenital Heart Diseases: A Proposal for an Adapted NYHA Classification. International Journal of Environmental Research and Public Health, 19(10), 5907. https://doi.org/10.3390/ijerph19105907