
The Gaps in Health-Adjusted Life Years (HALE) by Income and Region in Korea: A National Representative Bigdata Analysis

 , , ,
, , ,
Abstract
1. Background
2. Materials and Methods
2.1. Data and Units of Analysis
2.2. Statistical Analysis
3. Results
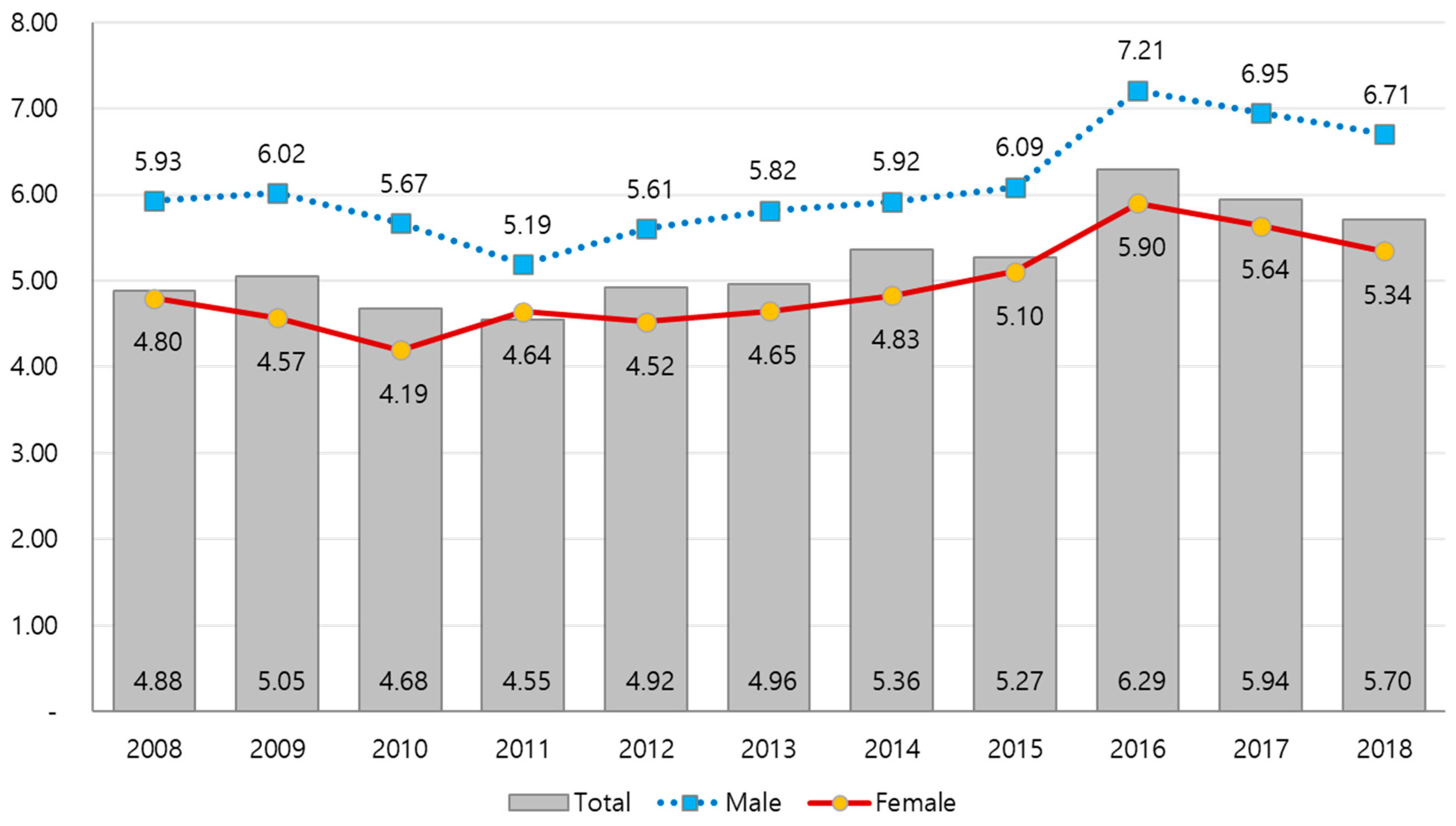
3.1. HALE in Korea, by Gender, Income Level, and Year
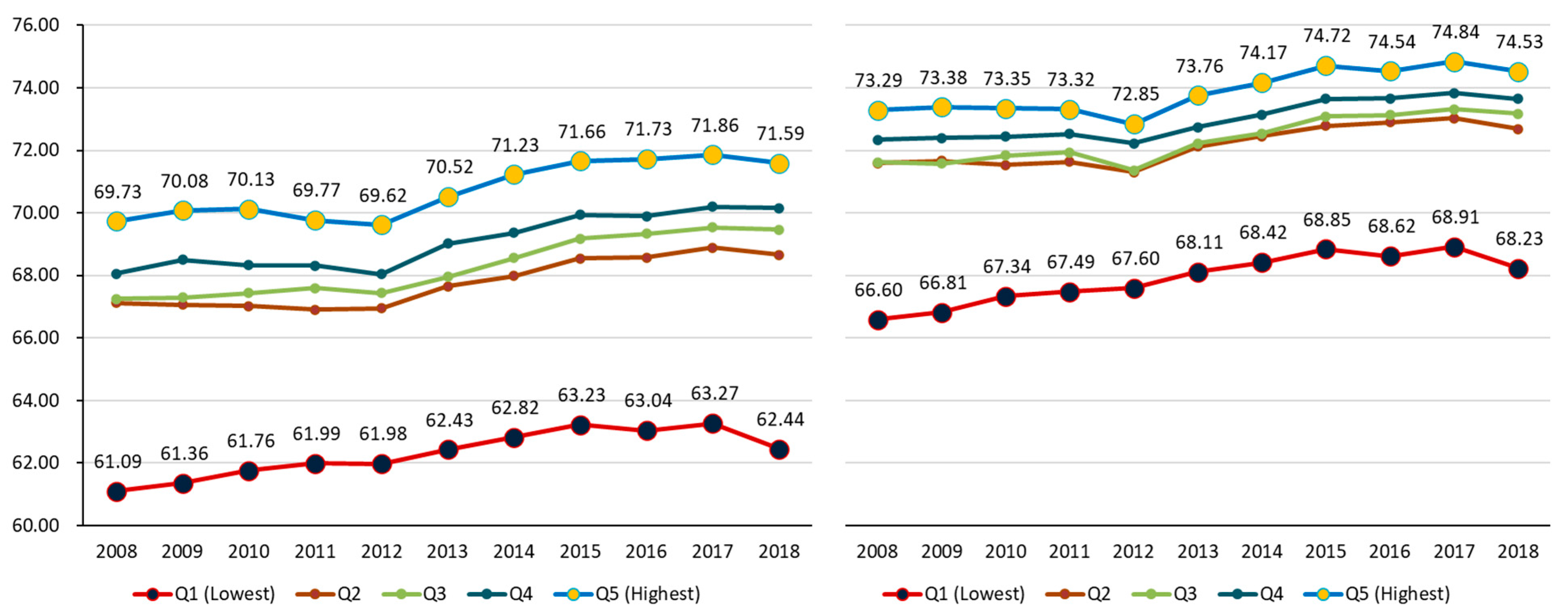
3.2. HALE by Income Level for Males and Females in Korea
3.3. Distribution of the HALE by Region
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| (DFLE) | Disability-free life expectancy |
| (GBD) | Global Burden of Disease |
| (HALE) | Health-adjusted life years/expectancy |
| (HLE) | Healthy life expectancy |
| (IHME) | Institute for Health Metrics and Evaluation |
| (KCDC)(NHIS) | Korea Centers for Disease Control and Prevention National Health Insurance Service |
| (PAF) | Population attributable fractions |
| (WHO) | World Health Organization |
| (YLD) | Years lived with disability |
References
- Crimmins, E.M. Lifespan and Healthspan: Past, Present, and Promise. Gerontology 2015, 55, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Hyder, A.A.; Puvanachandra, P.; Morrow, R.H. Measuring the health of populations: Explaining composite indicators. J. Public Health Res. 2012, 1, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Mathers, C.D.; Vos, T.; Lopez, A.D. National Burden of Disease Studies: A Practical Guide, 2nd ed.; Global Program on Evidence for Health Policy; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. WHO Methods for Life Expectancy and Healthy Life Expectancy. In Global Health Estimates Technical Paper WHO/HIS/HSI/GHE; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Vos, T.; Flaxman, A.D.; Naghavi, M. Years lived with disability (YLD) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Lee, J.Y.; Ock, M.; Kim, S.H.; Go, D.-S.; Kim, H.J.; Jo, M.-W. Health-Adjusted Life Expectancy (HALE) in Korea: 2005–2011. J. Korean Med. Sci. 2016, 31, S139. [Google Scholar] [CrossRef] [PubMed]
- Lim, D.; Bahk, J.; Ock, M. Income-related inequality in quality-adjusted life expectancy in Korea at the national and district levels. Health Qual. Life Out. 2020, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance System. Available online: https://www.nhis.or.kr/static/html/wbd/g/a/wbdga0302.html (accessed on 2 August 2020).
- Statistics Korea. Available online: http://kostat.go.kr/portal/eng/index.action (accessed on 2 July 2020).
- National Health Insurance System. Available online: https://www.nhis.or.kr/menu/retriveMenuSet.xx?menuId=B2220 (accessed on 2 July 2020).
- Korea Centers for Disease Control and Prevention. Injury Surveillance. Available online: http://www.cdc.go.kr/contents.es?mid=a20303010501 (accessed on 2 July 2020).
- Statistics in Korea. Available online: http://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B42 (accessed on 2 July 2020).
- World Health Organization. Available online: https://www.who.int/healthinfo/global_burden_disease/tools_software/en/ (accessed on 2 August 2020).
- Kim, Y.E.; Jo, M.W.; Park, H. Updating disability weights for measurement of healthy life expectancy and disability-adjusted life year in Korea. J. Korean Med. Sci. 2020, 35, e219. [Google Scholar]
- Kim, Y.-E.; Park, H.; Jo, M.-W.; Oh, I.-H.; Go, D.-S.; Jung, J.; Yoon, S.-J. Trends and Patterns of Burden of Disease and Injuries in Korea Using Disability-Adjusted Life Years. J. Korean Med. Sci. 2019, 34, e75. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- Sullivan, D.F. A Single Index of Mortality and Morbidity. HSMHA Health Rep. 1971, 86, 347. [Google Scholar] [CrossRef] [PubMed]
- GBD DALYs Hale Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef]
- Khang, Y.H. Developing Indicators for Evaluating and Monitoring the Health Plan 2020 Using the National Health Information Database of the National Health Insurance Service in Korea; Seoul National University R&DB Foundation: Seoul, Korea, 2016. [Google Scholar]
- Khang, Y.-H.; Bahk, J.; Lim, D.; Kang, H.-Y.; Lim, H.-K.; Kim, Y.-Y.; Park, J.H. Trends in inequality in life expectancy at birth between 2004 and 2017 and projections for 2030 in Korea: Multiyear cross-sectional differences by income from national health insurance data. BMJ Open 2019, 9, e030683. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.; Bahk, J.; Yoon, T.-H.; Yun, S.-C.; Khang, Y.H. Income Differences in Smoking Prevalences in 245 Districts of South Korea: Patterns by Area Deprivation and Urbanity, 2008–2014. J. Prev. Med. Public Health 2017, 50, 100–126. [Google Scholar] [CrossRef]
- Kwak, C.W.; Han, K.-T.; Nam, C.M.; Moon, K.T.; Yoon, H.-S.; Park, E.-C. Income disparity and mortality among patients with alcohol use disorder in South Korea. Psychiatry Res. 2017, 258, 358–364. [Google Scholar] [CrossRef]
- Kim, I.-G.; So, W.-Y. The Relationship between Household Income and Physical Activity in Korea. J. Phys. Ther. Sci. 2014, 26, 1887–1889. [Google Scholar] [CrossRef]
- GBD Compare. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 2 July 2020).
- WHO Global Health Observatory Data Repository. Available online: http://apps.who.int/gho/data/view.main.HALEXv?lang=en (accessed on 31 January 2021).
- World Health Organization. World Health Statistics 2016: Monitoring Health for the SDGs Sustainable Development Goals; WHO: Geneva, Switzerland, 2016. [Google Scholar]



{kind=link}
{kind=link}
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall population | 68.89 | 69.05 | 69.16 | 69.20 | 68.97 | 69.69 | 70.10 | 70.59 | 70.56 | 70.78 | 70.43 |
| Gender | |||||||||||
| Male | 66.47 | 66.69 | 66.78 | 66.77 | 66.66 | 67.36 | 67.82 | 68.35 | 68.33 | 68.58 | 68.25 |
| Female | 71.00 | 71.09 | 71.24 | 71.32 | 71.00 | 71.72 | 72.08 | 72.54 | 72.49 | 72.72 | 72.37 |
| Difference (Female-Male) | 4.53 | 4.40 | 4.46 | 4.54 | 4.34 | 4.36 | 4.26 | 4.20 | 4.16 | 4.14 | 4.12 |
| Income level | |||||||||||
| Q1 (Lowest) | 63.82 | 64.06 | 64.53 | 64.72 | 64.76 | 65.25 | 65.58 | 66.00 | 65.78 | 66.03 | 65.24 |
| Q2 | 69.52 | 69.53 | 69.43 | 69.42 | 69.25 | 70.03 | 70.37 | 70.80 | 70.89 | 71.10 | 70.81 |
| Q3 | 69.61 | 69.61 | 69.81 | 69.94 | 69.56 | 70.25 | 70.73 | 71.30 | 71.40 | 71.59 | 71.48 |
| Q4 | 70.39 | 70.66 | 70.59 | 70.63 | 70.33 | 71.08 | 71.47 | 72.00 | 71.98 | 72.21 | 72.10 |
| Q5 (Highest) | 71.76 | 72.01 | 72.00 | 71.80 | 71.48 | 72.39 | 72.93 | 73.44 | 73.37 | 73.58 | 73.28 |
| Difference (Q5-Q1) | 7.94 | 7.95 | 7.47 | 7.08 | 6.72 | 7.14 | 7.35 | 7.44 | 7.58 | 7.55 | 8.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-E.; Jung, Y.-S.; Ock, M.; Park, H.; Kim, K.-B.; Go, D.-S.; Yoon, S.-J. The Gaps in Health-Adjusted Life Years (HALE) by Income and Region in Korea: A National Representative Bigdata Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3473. https://doi.org/10.3390/ijerph18073473
Kim Y-E, Jung Y-S, Ock M, Park H, Kim K-B, Go D-S, Yoon S-J. The Gaps in Health-Adjusted Life Years (HALE) by Income and Region in Korea: A National Representative Bigdata Analysis. International Journal of Environmental Research and Public Health. 2021; 18(7):3473. https://doi.org/10.3390/ijerph18073473
Chicago/Turabian StyleKim, Young-Eun, Yoon-Sun Jung, Minsu Ock, Hyesook Park, Ki-Beom Kim, Dun-Sol Go, and Seok-Jun Yoon. 2021. "The Gaps in Health-Adjusted Life Years (HALE) by Income and Region in Korea: A National Representative Bigdata Analysis" International Journal of Environmental Research and Public Health 18, no. 7: 3473. https://doi.org/10.3390/ijerph18073473
APA StyleKim, Y.-E., Jung, Y.-S., Ock, M., Park, H., Kim, K.-B., Go, D.-S., & Yoon, S.-J. (2021). The Gaps in Health-Adjusted Life Years (HALE) by Income and Region in Korea: A National Representative Bigdata Analysis. International Journal of Environmental Research and Public Health, 18(7), 3473. https://doi.org/10.3390/ijerph18073473