
Linking Health Literacy to Self-Care in Hypertensive Patients with Physical Disabilities: A Path Analysis Using a Multi-Mediation Model


Abstract
1. Introduction
2. Materials and Methods
2.1. Sampling and Data Collection
2.2. Measurement
2.2.1. Health Literacy
2.2.2. Access to Healthcare
2.2.3. Provider–Patient Interactions
2.2.4. Hypertension Knowledge
2.2.5. Hypertension Control Self-Efficacy
2.2.6. Hypertension Self-Care
2.2.7. Demographic and Health-Related Characteristics
2.3. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Multi-Collinearity among Research Variables
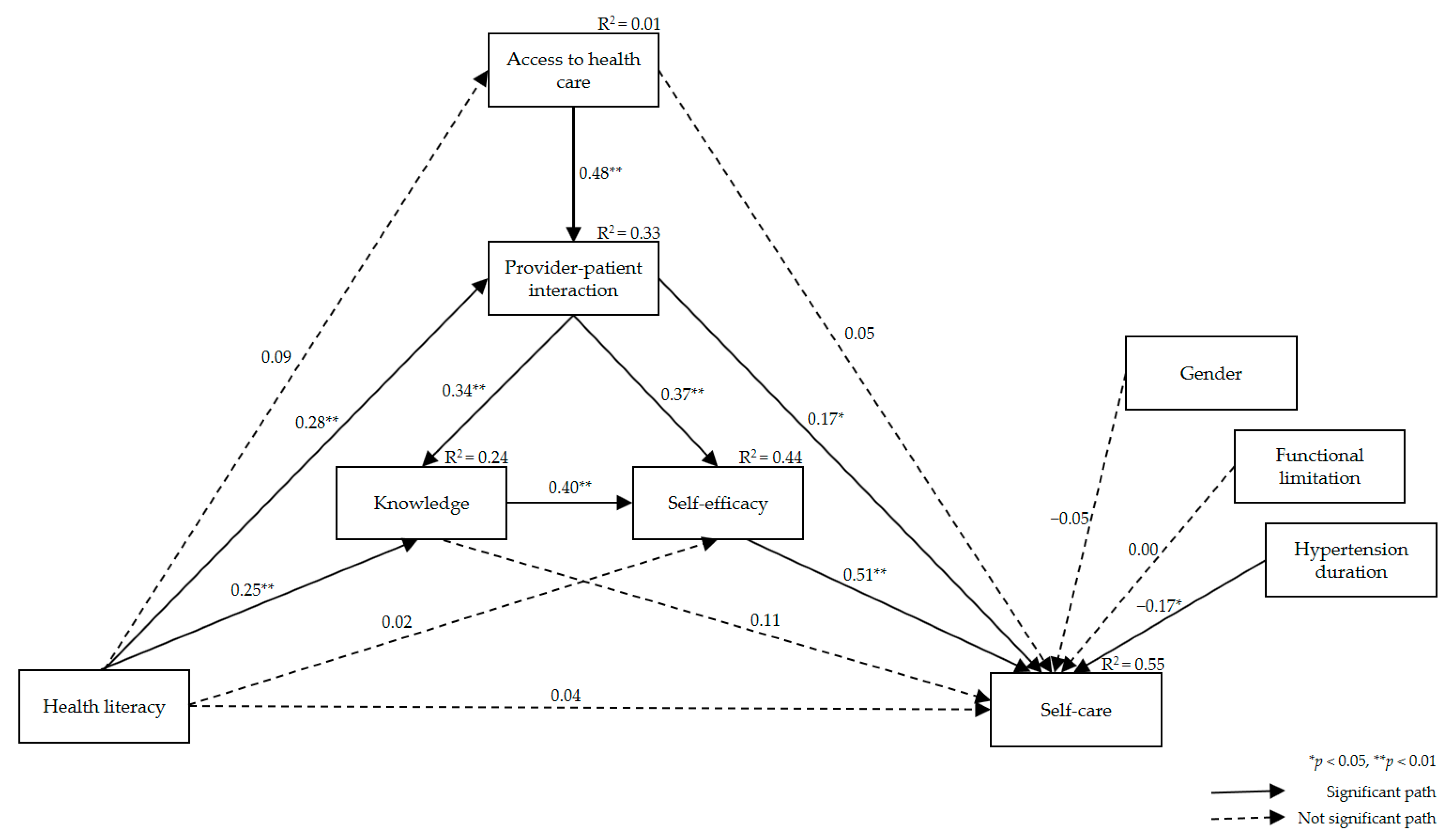
3.3. Fitness of the Hypothetical Path Model
3.4. Effect Analysis of the Multi-Mediation Model
3.5. Indirect Effect Analysis Using Phantom Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Disability and Health; WHO Press: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/fact-sheets/detail/disability-and-health (accessed on 10 January 2021).
- Krahn, G.L.; Walker, D.K.; Correa-De-Araujo, R. Person with disabilities as an unrecognized health disparity population. Am. J. Public Health 2015, 105, S198–S206. [Google Scholar] [CrossRef]
- Havercamp, S.M.; Scandlin, D.; Roth, M. Health disparities among adults with developmental disabilities, adults with other disabilities, and adults not reporting disability in North Carolina. Public Health Rep. 2004, 119, 418–426. [Google Scholar] [CrossRef]
- Kim, S.; Lee, Y.; Oh, W.; Hwang, J.; Oh, M.; Lee, M.; Lee, N.; Oh, D.; Kang, D.; Kwon, S.; et al. 2017 National Survey of the Disabled Persons; Ministry of Health and Welfare, Korea Institute for Health and Social Affairs: Sejong, Korea, 2017. [Google Scholar]
- Ministry of Health and Welfare. 2020 Statistics of People with Disabilities Lives; Ministry of Health and Welfare: Sejong, Korea, 2020.
- Motlagh, S.F.Z.; Chaman, R.; Sadeghi, E.; Eslami, A.A. Self-care behaviors and related factors in hypertensive patients. Iran. Red. Crescent. Med. J. 2016, 18, e35805. [Google Scholar] [CrossRef]
- Son, Y.; Song, E.K. Impact of health literacy on disease-related knowledge and adherence to self-care in patients with hypertension. J. Korean. Acad. Fundam. Nurs. 2012, 19, 6–15. [Google Scholar] [CrossRef]
- Omisakin, F.D.; Ncama, B.P. Self, self-care and self-management concepts: Implications for self-management education. Edu. Res. 2011, 2, 1733–1737. [Google Scholar]
- Gazmararian, J.A.; Williams, M.V.; Peel, J.; Baker, D.W. Health literacy and knowledge of chronic disease. Patient Educ. Couns. 2003, 51, 267–275. [Google Scholar] [CrossRef]
- Poureslami, I.; Nimmon, L.; Rootman, I.; Fizgerald, M.J. Priorities for action: Recommendations from an international roundtable on health literacy and chronic disease management. Health Promot. Int. 2017, 32, 743–754. [Google Scholar] [CrossRef]
- World Health Organization. Track 2: Health Literacy and Health Behavior. In Proceedings of the 7th Global Conference on Health Promotion, Nairobi, Kenya, 26–30 October 2009; WHO Press: Geneva, Switzerland. Available online: https://www.who.int/healthpromotion/conferences/7gchp/track2/en/ (accessed on 15 January 2021).
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Yehle, K.S.; Albert, N.M.; Ferraro, K.F.; Mason, H.L.; Murawski, M.M.; Plake, K.S. Relationships between health literacy and heart failure knowledge, self-efficacy, and self-care adherence. Res. Soc. Adm. Pharm. 2014, 10, 378–386. [Google Scholar] [CrossRef]
- Osborn, C.Y.; Paasche-Orlow, M.K.; Bailey, S.C.; Wolf, M.S. The mechanisms linking health literacy to behavior and health status. Am. J. Health Behav. 2011, 35, 118–128. [Google Scholar] [CrossRef]
- Aboumatar, H.J.; Carson, K.A.; Beach, M.C.; Roter, D.L.; Copper, L.A. The impact of health literacy on desire for participation in healthcare, medical visit communication, and patient reported outcomes among patients with hypertension. J. Gen. Intern. Med. 2013, 28, 1469–1476. [Google Scholar] [CrossRef]
- Hall, E.; Lee, S.; Clark, P.C.; Perilla, J. Social ecology of adherence to hypertension treatment in Latino migrant and seasonal farmworkers. J. Transcult. Nurs. 2014, 27, 33–41. [Google Scholar] [CrossRef]
- Shi, D.; Li, J.; Wang, Y.; Wang, S.; Liu, K.; Shi, R.; Zhang, Q.; Chen, X. Association between health literacy and hypertension management in a Chinese community: A retrospective cohort study. Intern. Emerg. Med. 2017, 12, 765–776. [Google Scholar] [CrossRef]
- Nguyen, J.; Gilbert, L. Health literacy among individuals with disabilities: A health information national trends survey analysis. Perm. J. 2019, 23, 19.034. [Google Scholar] [CrossRef]
- Johnston, M.V.; Diab, M.; Kim, S.S.; Kirshblum, S. Health literacy, morbidity, and quality of life among individuals with spinal cord injury. J. Spinal. Cord. Med. 2005, 28, 230–240. [Google Scholar] [CrossRef]
- Paasche-Orlow, M.K.; Wolf, M.S. The causal pathways linking health literacy to health outcomes. Am. J. Health Behav. 2007, 31, S19–S26. [Google Scholar] [CrossRef] [PubMed]
- Dennison, C.R.; McEntee, M.L.; Samuel, L.; Johnson, B.J.; Rotman, S.; Kielty, A.; Russell, S.D. Adequate health literacy is associated with higher heart failure knowledge and self care confidence in hospitalized patients. J. Cardiovasc. Nurs. 2011, 26, 359–367. [Google Scholar] [CrossRef]
- Macabasco-O’Connell, A.; DeWalt, D.A.; Broucksou, K.A.; Hawk, V.; Baker, D.W.; Schillinger, D.; Ruo, B.; Bibbins-Domingo, K.; Holmes, G.M.; Erman, B.; et al. Relationship between literacy, knowledge, self-care behaviors, and heart failure-related quality of life among patients with heart failure. J. Gen. Intern. Med. 2011, 26, 979–986. [Google Scholar] [CrossRef] [PubMed]
- McCleary-Jones, V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011, 22, 25–32. [Google Scholar] [PubMed]
- Ministry of Health and Welfare. Policy for People with Disabilities; Ministry of Health and Welfare: Sejong, Korea, 2013. Available online: https://www.mohw.go.kr/react/policy/policy_bd_vw.jsp (accessed on 10 January 2021).
- Hoe, S.L. Issues and procedures in adopting structural equation modelling technique. J. Quant. Methods 2008, 3, 76–83. [Google Scholar]
- Lee, T.W.; Kang, S.J. Development of the short form of the Korean health literacy scale for the elderly. Res. Nurs. Health 2013, 36, 524–534. [Google Scholar] [CrossRef]
- Penchansky, R.; Thomas, J.W. The Concept of Access. Med. Care 1981, 19, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Gil, E.; Oh, H. Testing a middle-range theory of self-care of chronic illness: A validation for Korean adult patients with severe hypertension. J. Korean Acad. Nurs. 2018, 48, 521–533. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S. Impact of Shared Decision Making on Patient’s Satisfaction in Rheumatic Disease. Master’s Thesis, Hanyang University, Seoul, Korea, 2011. [Google Scholar]
- Lim, J.; Ko, G.P.; Han, E.; Jung, W.; Park, M.J.; Han, J.O. The Effects Assessment of Chronic Care Management Based on Primary Clinics for Hypertension, Diabetes Patients; Korea Health Promotion Institute: Seoul, Korea, 2012. [Google Scholar]
- Viera, A.J.; Cohen, L.W.; Mitchell, C.M.; Sloane, P.D. High blood pressure knowledge among primary care patients with known hypertension: A North Carolina Family Medicine Research Network (NC-FM-RN) study. J. Am. Board. Fam. Med. 2008, 21, 300–308. [Google Scholar] [CrossRef]
- Park, Y. An Effect of the Self-Regulation, Program for Hypertensives, Synthesis & Testing of Orem and Bandura’s Theory. Ph.D. Thesis, Seoul National University, Seoul, Korea, 1994. [Google Scholar]
- Lee, Y.H. A study of the effect of an efficacy expectation promoting program on self-efficacy and self-care. J. Korean Acad. Nurs. 1995, 7, 212–227. [Google Scholar]
- Washington Group on Disability Statistics. The Washington Group on Disability Short Set of Disability Questions; The U.S. National Center for Health Statistics: Hyattsville, MD, USA, 2020.
- Kim, H.Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef]
- Nevitt, J.; Hancock, G.R. Performance of bootstrapping approaches to model test statistics and parameter standard error estimation in structural equation modeling. Structural Equ. Model. 2001, 8, 353–377. [Google Scholar] [CrossRef]
- Bollen, K.A.; Stine, R.A. Bootstrapping goodness-of-fit measures in structural equation models. Sociol. Methods Res. 1992, 21, 205–229. [Google Scholar] [CrossRef]
- Kim, G.S. AMOS Structural Equation Model Analysis; Hannarae: Seoul, Korea, 2013; pp. 120–132. [Google Scholar]
- Macho, S.; Ledermann, T. Estimating, testing, and comparing specific effects in structural equation models: The phantom model approach. Psychol. Methods 2011, 16, 34–43. [Google Scholar] [CrossRef]
- Kim, M.; Song, M. Effects of self-management program applying Dongsasub training on self-efficacy, self-esteem, self-management behavior and blood pressure in older adults with hypertension. J. Korean Acad. Nurs. 2015, 45, 576–586. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Disability and Primary Health: A Review of the Literacy; Te Pou o Te Whakaaro Nui: Wellington, New Zealand, 2013. Available online: https://www.donaldbeasley.org.nz/assets/publications/health/primary-health-and-disability-a-review-of-the-literature.pdf (accessed on 8 February 2021).
- Fisher, W.A.; Fisher, J.D.; Harman, J. The information-motivation-behavioral skills model: A general social psychological approach to understanding and promoting health behavior. Soc. Psychol. Found. Health Illn. 2003, 22, 82–106. [Google Scholar] [CrossRef]
- Schoenthaler, A.; Chaplin, W.F.; Allegrante, J.P.; Fernandez, S.; Diaz-Gloster, M.; Tobin, J.N.; Ogedegbe, G. Provider communication effects medication adherence in hypertensive African Americans. Patient. Educ. Couns. 2009, 75, 185–191. [Google Scholar] [CrossRef]
- Wallace, A. Low health literacy: Overview, assessment, and steps toward providing high-quality diabetes care. Diabetes Spectr. 2010, 23, 220–227. [Google Scholar] [CrossRef][Green Version]
- Lee, Y.Y.; Lin, J.L. The effects of trust in physician on self-efficacy, adherence and diabetes outcomes. Soc. Sci. Med. 2009, 68, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- McColl, M.A.; Forster, D.; Shortt, S.E.; Hunter, D.; Dorland, J.; Godwin, M.; Rosser, W. Physician experiences providing primary care to people with disabilities. Health Policy 2008, 4, e129. [Google Scholar] [CrossRef]
- Levy, H.; Janke, A. Health literacy and access to care. J. Health Commun. 2016, 21, 43–50. [Google Scholar] [CrossRef]
- Harrington, A.L.; Hirsch, M.A.; Hammond, F.M.; Norton, H.J.; Bockenek, W.L. Assessment of primary care services and perceived barriers to care in persons with disabilities. Am. J. Phys. Med. Rehabil. 2009, 88, 852–863. [Google Scholar] [CrossRef]
- Jeon, B.; Kwon, S.; Kim, H. Health care utilization by people with disabilities: A longitudinal analysis of the Korea Welfare Panel Study (KoWePS). Disabil. Health J. 2015, 8, 353–362. [Google Scholar] [CrossRef]
- Shin, H.I. Strategic Research for Improving the Disabled People’s Health; Ministry of Health and Welfare: Sejong, Korea, 2015.
- Ahn, Y.H.; Ham, O.K. Factors associated with medication adherence among Medical-aid beneficiaries with hypertension. West. J. Nurs. Res. 2016, 38, 1298–1312. [Google Scholar] [CrossRef] [PubMed]
- Rios, D.; Magasi, S.; Novak, C.; Harniss, M. Conducting accessible research: Including people with disabilities in public health, epidemiological, and outcomes studies. Am. J. Public Health 2016, 106, 2137–2144. [Google Scholar] [CrossRef]
- Taber, K.S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Categories | n (%) or Mean ± SD |
|---|---|---|
| Gender | Male | 70 (33.2) |
| Female | 141 (66.8) | |
| Age (year) | 42.09 ± 8.98 | |
| 20~29 | 11 (5.2) | |
| 30~39 | 79 (37.4) | |
| 40~49 | 95 (45.0) | |
| 50~59 | 14 (6.6) | |
| ≥60 | 12 (5.7) | |
| Marital status | With spouse | 123 (58.3) |
| No spouse | 88 (41.7) | |
| Level of education | ≤Middle school | 12 (5.7) |
| High school | 108 (51.2) | |
| ≥College | 91 (43.1) | |
| Monthly household income (KRW 1000) | <100 | 39 (18.5) |
| 100~199 | 62 (29.4) | |
| 200~299 | 70 (33.2) | |
| 300~399 | 32 (15.2) | |
| ≥400 | 8 (3.7) | |
| Disability severity 1 | Mild | 135 (64.0) |
| Severe | 76 (36.0) | |
| Functional limitation | No | 108 (51.2) |
| Yes 2 | 103 (48.8) | |
| Duration of hypertension (month) | 47.03 ± 55.01 | |
| Health literacy | 11.45 ± 0.79 (range 6–12) | |
| Hypertension self-care | 57.23 ± 7.91 (range 33–74) | |
| Access to healthcare | 16.23 ± 2.87 (range 5–25) | |
| Provider–patient interaction | 24.94 ± 4.82 (range 9–35) | |
| Hypertension knowledge | 3.93 ± 1.77 (range 0–7) | |
| Hypertension control self-efficacy | 66.67 ± 14.42 (range 19–100) | |
| Variables | X1 | X2 | X3 | X4 | X5 | X6 | X7 | X8 | X9 |
|---|---|---|---|---|---|---|---|---|---|
| Pearson’s Correlation Coefficient | |||||||||
| Health literacy | 1 | ||||||||
| Access to healthcare | 0.09 | 1 | |||||||
| Provider–patient interaction | 0.32 *** | 0.50 *** | 1 | ||||||
| Knowledge | 0.36 *** | 0.20 ** | 0.43 *** | 1 | |||||
| Self-efficacy | 0.28 *** | 0.33 *** | 0.55 *** | 0.57 *** | 1 | ||||
| Self-care | 0.28 *** | 0.48 *** | 0.33 *** | 0.53 *** | 0.68 *** | 1 | |||
| Gender | −0.14 * | 0.10 | 0.01 | 0.08 | 0.16 * | 0.04 | 1 | ||
| Functional limitation | −0.05 | −0.05 | −0.02 | −0.06 | −0.05 | −0.05 | −0.02 | 1 | |
| Duration of hypertension | 0.06 | −0.02 | 0.09 | 0.13 | 0.10 | −0.09 | 0.01 | 0.01 | 1 |
| Pathways | Estimate | SE | 95% CI 1 | p | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Health literacy → Access to healthcare → Self-care | 0.05 | 0.10 | −0.07 | 0.36 | 0.394 | |
| Health literacy → Access to healthcare → Provider–patient interaction | → Self-care | 0.07 | 0.08 | −0.04 | 0.30 | 0.206 |
| → Knowledge → Self-care | 0.02 | 0.02 | −0.01 | 0.09 | 0.169 | |
| → Knowledge → Self-efficacy → Self-care | 0.03 | 0.03 | −0.02 | 0.10 | 0.229 | |
| → Self-efficacy → Self-care | 0.08 | 0.09 | −0.06 | 0.29 | 0.284 | |
| Health literacy → Provider–patient interaction | → Self-care | 0.48 | 0.24 | 0.09 | 1.07 | 0.018 |
| → Knowledge → Self-efficacy → Self-care | 0.20 | 0.07 | 0.11 | 0.39 | <0.001 | |
| → Knowledge → Self-care | 0.11 | 0.07 | 0.00 | 0.27 | 0.059 | |
| → Self-efficacy → Self-care | 0.54 | 0.25 | 0.21 | 1.11 | 0.001 | |
| Health literacy → Knowledge | → Self-efficacy → Self-care | 0.53 | 0.29 | 0.16 | 1.24 | 0.001 |
| → Self-care | 0.28 | 0.21 | −0.01 | 0.85 | 0.059 | |
| Health literacy → Self-efficacy → Self-care | 0.09 | 0.40 | −0.80 | 0.76 | 0.818 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, H.J.; Yoon, J.Y. Linking Health Literacy to Self-Care in Hypertensive Patients with Physical Disabilities: A Path Analysis Using a Multi-Mediation Model. Int. J. Environ. Res. Public Health 2021, 18, 3363. https://doi.org/10.3390/ijerph18073363
Nam HJ, Yoon JY. Linking Health Literacy to Self-Care in Hypertensive Patients with Physical Disabilities: A Path Analysis Using a Multi-Mediation Model. International Journal of Environmental Research and Public Health. 2021; 18(7):3363. https://doi.org/10.3390/ijerph18073363
Chicago/Turabian StyleNam, Hye Jin, and Ju Young Yoon. 2021. "Linking Health Literacy to Self-Care in Hypertensive Patients with Physical Disabilities: A Path Analysis Using a Multi-Mediation Model" International Journal of Environmental Research and Public Health 18, no. 7: 3363. https://doi.org/10.3390/ijerph18073363
APA StyleNam, H. J., & Yoon, J. Y. (2021). Linking Health Literacy to Self-Care in Hypertensive Patients with Physical Disabilities: A Path Analysis Using a Multi-Mediation Model. International Journal of Environmental Research and Public Health, 18(7), 3363. https://doi.org/10.3390/ijerph18073363