
Interventions to Improve Adherence to Antiretroviral Therapy (ART) in Sub-Saharan Africa: An Updated Systematic Review

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
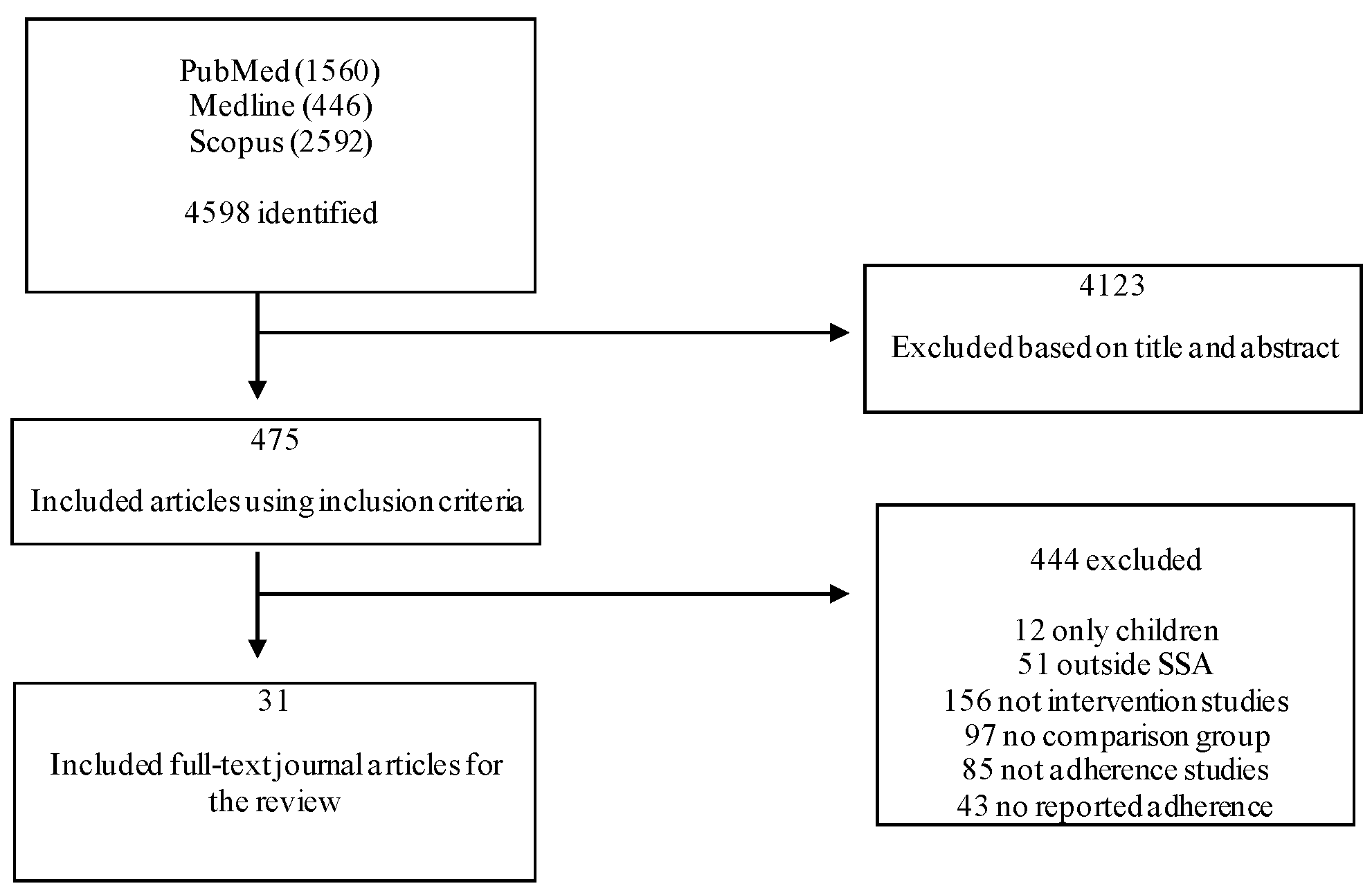
2.3. Study Selection
2.4. Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Risk of Bias Assessment
4. Discussion
4.1. Effectiveness of Interventions
4.2. Adherence in Key Affected Populations
4.3. Assessment of Adherence
4.4. Other Results
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fauci, A.S.; Marston, H.D.; Folkers, G.K. An HIV cure: Feasibility, discovery, and implementation. JAMA 2014, 312, 335–336. [Google Scholar] [CrossRef] [PubMed]
- Mills, E.J.; Nachega, J.B.; Buchan, I.; Orbinski, J.; Attaran, A.; Singh, S.; Rachlis, B.; Wu, P.; Cooper, C.; Thabane, L.; et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: A meta-analysis. JAMA 2006, 296, 679–690. [Google Scholar] [CrossRef]
- Langebeek, N.; Gisolf, E.H.; Reiss, P.; Vervoort, S.C.; Hafsteinsdóttir, T.B.; Richter, C.; Sprangers, M.A.; Nieuwkerk, P.T. Predictors and correlates of adherence to combination antiretroviral therapy (ART) for chronic HIV infection: A meta-analysis. BMC Med. 2014, 12, 142. [Google Scholar] [CrossRef]
- Weiser, S.D.; Palar, K.; Frongillo, E.A.; Tsai, A.C.; Kumbakumba, E. Longitudinal assessment of associations between food insecurity, antiretroviral adherence and HIV treatment outcomes in rural Uhganda. AIDS 2014, 28, 115. [Google Scholar] [CrossRef] [PubMed]
- Aberg, J.A.; Gallant, J.E.; Ghanem, K.G.; Emmanuel, P.; Zingman, B.S.; Horberg, M.A. Primary care guidelines for the management of persons infected with HIV: 2013 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 58, e1–e34. [Google Scholar] [CrossRef]
- Paterson, D.L.; Swindells, S.; Mohr, J.; Brester, M.; Vergis, E.N.; Squier, C.; Wagener, M.M.; Singh, N. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann. Intern. Med. 2000, 133, 21–30. [Google Scholar] [CrossRef]
- de Olalla Garcia, P.; Knobel, H.; Carmona, A.; Guelar, A.; López-Colomés, J.L.; Caylà, J.A. Impact of adherence and highly active antiretroviral therapy on survival in HIV-infected patients. J. Acquir. Immune Defic. Syndr. 2002, 30, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Bangsberg, D.R.; Perry, S.; Charlebois, E.D.; Clark, R.A.; Roberston, M.; Zolopa, A.R.; Moss, A. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. Aids 2001, 15, 1181–1183. [Google Scholar] [CrossRef] [PubMed]
- Hansana, V.; Sanchaisuriya, P.; Durham, J.; Sychareun, V.; Chaleunvong, K.; Boonyaleepun, S.; Schelp, F.P. Adherence to antiretroviral therapy (ART) among people living with HIV (PLHIV): A cross-sectional survey to measure in Lao PDR. BMC Public Health 2013, 13, 617. [Google Scholar] [CrossRef]
- Byrd, K.K.; Hou, J.G.; Bush, T.; Hazen, R.; Kirkham, H.; Delpino, A.; Weidle, P.J.; Shankle, M.D.; Camp, N.M.; Suzuki, S.; et al. Adherence and viral suppression among participants of the patient-centered human immunodeficiency virus (HIV) care model project: A collaboration between community-based pharmacists and HIV clinical providers. Clin. Infect. Dis. 2020, 70, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.S.; Chen, Y.Q.; McCauley, M.; Gamble, T.; Hosseinipour, M.C.; Kumarasamy, N.; Hakim, J.G.; Kumwenda, J.; Grinsztejn, B.; Pilotto, J.H.; et al. Antiretroviral therapy for the prevention of HIV-1 transmission. N. Engl. J. Med. 2016, 375, 830–839. [Google Scholar] [CrossRef] [PubMed]
- Rodger, A.J.; Cambiano, V.; Bruun, T.; Vernazza, P.; Collins, S.; Van Lunzen, J.; Corbelli, G.M.; Estrada, V.; Geretti, A.M.; Beloukas, A.; et al. Sexual activity without condoms and risk of HIV transmission in serodifferent couples when the HIV-positive partner is using suppressive antiretroviral therapy. JAMA 2016, 316, 171–181. [Google Scholar] [CrossRef] [PubMed]
- May, M.T.; Gompels, M.; Delpech, V.; Porter, K.; Orkin, C.; Kegg, S.; Hay, P.; Johnson, M.; Palfreeman, A.; Gilson, R.; et al. Impact on life expectancy of HIV-1 positive individuals of CD4+ cell count and viral load response to antiretroviral therapy. AIDS 2014, 28, 1193. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. 90-90-90 Treatment Target. 2020. Available online: https://www.unaids.org/en/90-90-90 (accessed on 20 November 2020).
- Kharsany, A.B.; Karim, Q.A. HIV Infection and AIDS in Sub-Saharan Africa: Current Status, Challenges and Opportunities. Open AIDS J. 2016, 10, 34–48. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. HIV/AIDS. 2020. Available online: https://www.afro.who.int/health-topics/hivaids (accessed on 10 January 2021).
- Amico, K.R.; Orrell, C. Antiretroviral therapy adherence support: Recommendations and future directions. J. Int. Assoc. Provid. AIDS Care (JIAPAC) 2013, 12, 128–137. [Google Scholar] [CrossRef]
- Bärnighausen, T.; Chaiyachati, K.; Chimbindi, N.; Peoples, A.; Haberer, J.; Newell, M.L. Interventions to increase antiretroviral adherence in sub-Saharan Africa: A systematic review of evaluation studies. Lancet Infect. Dis. 2011, 11, 942–951. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Riva, J.J.; Malik, K.M.; Burnie, S.J.; Endicott, A.R.; Busse, J.W. What is your research question? An introduction to the PICOT format for clinicians. J. Can. Chiropr. Assoc. 2012, 56, 167. [Google Scholar]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]; The Cochrane Collaboration, 2011; Available online: www.handbook.cochrane.org (accessed on 14 November 2011).
- Heestermans, T.; Browne, J.L.; Aitken, S.C.; Vervoort, S.C.; Klipstein-Grobusch, K. Determinants of adherence to antiretroviral therapy among HIV-positive adults in sub-Saharan Africa: A systematic review. BMJ Glob. Health 2016, 1, e000125. [Google Scholar] [CrossRef]
- Mbuagbaw, L.; Sivaramalingam, B.; Navarro, T.; Hobson, N.; Keepanasseril, A.; Wilczynski, N.J.; Haynes, R.B.; Patient Adherence Review (PAR) Team. Interventions for enhancing adherence to antiretroviral therapy (ART): A systematic review of high quality studies. AIDS Patient Care STDS 2015, 29, 248–266. [Google Scholar] [CrossRef]
- Achieng, L.; Musangi, H.; Ong’uti, S.; Ombegoh, E.; Bryant, L.; Mwiindi, J.; Smith, N.; Keiser, P. An observational cohort comparison of facilitators of retention in care and adherence to anti-eetroviral therapy at an HIV treatment center in Kenya. PLoS ONE 2012, 7, e32727. [Google Scholar] [CrossRef]
- Atanga, P.N.; Ndetan, H.T.; Fon, P.N.; Meriki, H.D.; Muffih, T.P.; Achidi, E.A.; Hoelscher, M.; Kroidl, A. Using a composite adherence tool to assess ART response and risk factors of poor adherence in pregnant and breastfeeding HIV-positive Cameroonian women at 6 and 12 months after initiating option B+. BMC Pregnancy Child. 2018, 18, 418. [Google Scholar] [CrossRef] [PubMed]
- Bajunirwe, F.; Ayebazibwe, N.; Mulogo, E.; Eng, M.; McGrath, J.; Kaawa-Mafigiri, D.; Mugyenyi, P.; Seth, A.J. Effectiveness of a mobile antiretroviral pharmacy and HIV care intervention on the continuum of HIV care in rural Uganda. BioRxiv 2019, 533950. [Google Scholar] [CrossRef]
- Bhana, A.; Mellins, C.A.; Petersen, I.; Alicea, S.; Myeza, N.; Holst, H.; Abrams, E.; John, S.; Chhagan, M.; Nestadt, D.F.; et al. The VUKA family program: Piloting a family-based psychosocial intervention to promote health and mental health among HIV infected early adolescents in South Africa. AIDS Care 2014, 26, 1–11. [Google Scholar] [CrossRef]
- Boeke, C.E.; Nabitaka, V.; Rowan, A.; Guerra, K.; Nawaggi, P.; Mulema, V.; Bigira, V.; Magongo, E.; Mucheri, P.; Musoke, A.; et al. Results from a proactive follow-up intervention to improve linkage and retention among people living with HIV in Uganda: A pre-/post-study. BMC Health Serv. Res. 2018, 18, 949. [Google Scholar] [CrossRef]
- Boruett, P.; Kagai, D.; Njogo, S.; Nguhiu, P.; Awuor, C.; Gitau, L.; Chalker, J.; Ross-Degnan, D.; Wahlström, R.; Tomson, G. Facility-level intervention to improve attendance and adherence among patients on anti-retroviral treatment in Kenya—A quasi-experimental study using time series analysis. BMC Health Serv. Res. 2013, 13, 242. [Google Scholar] [CrossRef] [PubMed]
- Chime, O.H.; Arinze-Onyia, S.U.; Obionu, C.N. Do peer support groups have an effect on medication adherence? A study among people living with HIV/AIDS in Enugu State, Nigeria. Proc. Singap. Healthc. 2018, 27, 256–264. [Google Scholar] [CrossRef]
- Chung, M.H.; Richardson, B.A.; Tapia, K.; Benki-Nugent, S.; Kiarie, J.N.; Simoni, J.M.; Overbaugh, J.; Attwa, M.; John-Stewart, G.C. A randomized controlled trial comparing the effects of counseling and alarm device on HAART adherence and virologic outcomes. PLoS Med. 2011, 8, e1000422. [Google Scholar] [CrossRef] [PubMed]
- Coker, M.; Etiebet, M.A.; Chang, H.; Awwal, G.; Jumare, J.; Maiyaki Musa, B.; Babashani, M.; GHabib, A.; Dakum, P.; GAbimiku, A.; et al. Socio-demographic and adherence factors associated with viral load suppression in HIV-infected adults initiating therapy in northern Nigeria: A randomized controlled trial of a peer support intervention. Curr. HIV Res. 2015, 13, 279–285. [Google Scholar] [CrossRef]
- Fatti, G.; Meintjes, G.; Shea, J.; Eley, B.; Grimwood, A. Improved survival and antiretroviral treatment outcomes in adults receiving community-based adherence support: 5-year results from a multicentre cohort study in South Africa. J. Acquir. Immune Defic. Syndr. 2012, 61, e50–e58. [Google Scholar] [CrossRef] [PubMed]
- Gorman, S.E.; Martinez, J.M.; Olson, J. An assessment of HIV treatment outcomes among utilizers of semi-mobile clinics in rural Kenya. AIDS Care 2015, 27, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Hickey, M.D.; Salmen, C.R.; Omollo, D.; Mattah, B.; Fiorella, K.J.; Geng, E.H.; Bacchetti, P.; Blat, C.; Ouma, G.B.; Zoughbie, D.; et al. Implementation and Operational Research: Pulling the Network Together: Quasiexperimental Trial of a Patient-Defined Support Network Intervention for Promoting Engagement in HIV Care and Medication Adherence on Mfangano Island, Kenya. J. Acquir. Immune Defic. Syndr. 2015, 69, e127–e134. [Google Scholar] [CrossRef] [PubMed]
- Holstad, M.M.; Essien, E.J.; Ekong, E.; Higgins, M.; Teplinskiy, I.; Adewuyi, M.F. Motivational groups support adherence to antiretroviral therapy and use of risk reduction behaviors in HIV positive Nigerian women: A pilot study. Afr. J. Reprod. Health 2012, 16, 14–26. [Google Scholar] [PubMed]
- Igumbor, J.O.; Scheepers, E.; Ebrahim, R.; Jason, A.; Grimwood, A. An evaluation of the impact of a community-based adherence support programme on ART outcomes in selected government HIV treatment sites in South Africa. AIDS Care 2011, 23, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Jobanputra, K.; Parker, L.A.; Azih, C.; Okello, V.; Maphalala, G.; Kershberger, B.; Khogali, M.; Lujan, J.; Antierens, A.; Teck, R.; et al. Factors associated with virological failure and suppression after enhanced adherence counselling, in children, adolescents and adults on antiretroviral therapy for HIV in Swaziland. PLoS ONE 2015, 10, e0116144. [Google Scholar] [CrossRef]
- Jones, D.L.; Zulu, I.; Vamos, S.; Cook, R.; Chitalu, N.; Weiss, S.M. Determinants of engagement in HIV treatment and care among Zambians new to antiretroviral therapy. J. Assoc. Nurses AIDS Care 2013, 24, e1–e12. [Google Scholar] [CrossRef]
- Jones, A.S.; Coetzee, B.; Kagee, A.; Fernandez, J.; Cleveland, E.; Thomas, M.; Petrie, K.J. The Use of a Brief, Active Visualisation Intervention to Improve Adherence to Antiretroviral Therapy in Non-adherent Patients in South Africa. AIDS Behav. 2018, 26, 1–9. [Google Scholar] [CrossRef]
- Kalichman, S.C.; Mathews, C.; Banas, E.; Kalichman, M.O. Stigma management intervention to improve antiretroviral therapy adherence: Phase-I test of concept trial, Cape Town South Africa. Glob. Public Health 2018, 1, 1–6. [Google Scholar] [CrossRef]
- Kunutsor, S.; Walley, J.; Katabira, E.; Muchuro, S.; Balidawa, H.; Namagala, E.; Ikoona, E. Improving clinic attendance and adherence to antiretroviral therapy through a treatment supporter intervention in Uganda: A randomized controlled trial. AIDS Behav. 2011, 15, 1795–1802. [Google Scholar] [CrossRef]
- Kiweewa, F.M.; Wabwire, D.; Nakibuuka, J.; Mubiru, M.; Bagenda, D.; Musoke, P.; Fowler, M.G.; Antelman, G. Noninferiority of a task-shifting HIV care and treatment model using peer counselors and nurses among Ugandan women initiated on ART: Evidence from a randomized trial. J. Acquir. Immune Defic. Syndr. 2013, 63, e125–e132. [Google Scholar] [CrossRef]
- Maduka, O.; Tobin-West, C.I. Adherence counseling and reminder text messages improve uptake of antiretroviral therapy in a tertiary hospital in Nigeria. Niger. J. Clin. Pract. 2013, 16, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Mbuagbaw, L.; Thabane, L.; Ongolo-Zogo, P.; Lester, R.T.; Mills, E.J.; Smieja, M.; Dolovich, L.; Kouanfack, C. The Cameroon Mobile Phone SMS (CAMPS) trial: A randomized trial of text messaging versus usual care for adherence to antiretroviral therapy. PLoS ONE 2012, 7, e46909. [Google Scholar] [CrossRef] [PubMed]
- Moosa, M.Y.; Jeenah, F.Y. Treating depression in HIV-positive patients affects adherence. South. Afr. J. HIV Med. 2012, 13, 144–149. [Google Scholar] [CrossRef]
- Obua, C.; Kayiwa, J.; Waako, P.; Tomson, G.; Balidawa, H.; Chalker, J.; Ross-Degnan, D.; Wahlstrom, R. Improving adherence to antiretroviral treatment in Uganda with a low-resource facility-based intervention. Glob. Health Action 2014, 7, 24198. [Google Scholar] [CrossRef] [PubMed]
- Orrell, C.; Cohen, K.; Mauff, K.; Bangsberg, D.R.; Maartens, G.; Wood, R. A randomised controlled trial of real-time electronic adherence monitoring with text message dosing reminders in people starting first-line antiretroviral therapy. J. Acquir. Immune Defic. Syndr. 2015, 70, 495–502. [Google Scholar] [CrossRef]
- Peltzer, K.; Ramlagan, S.; Jones, D.; Weiss, S.M.; Fomundam, H.; Chanetsa, L. Efficacy of a lay health worker led group antiretroviral medication adherence training among non-adherent HIV-positive patients in KwaZulu-Natal, South Africa: Results from a randomized trial. Sahara J. 2012, 9, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Robbins, R.N.; Mellins, C.A.; Leu, C.S.; Rowe, J.; Warne, P.; Abrams, E.J.; Witte, S.; Stein, D.J.; Remien, R.H. Enhancing Lay Counselor Capacity to Improve Patient Outcomes with Multimedia Technology. AIDS Behav. 2015, 19 (Suppl. 2), 163–176. [Google Scholar] [CrossRef]
- Selke, H.M.; Kimaiyo, S.; Sidle, J.E.; Vedanthan, R.; Tierney, W.M.; Shen, C.; Denski, C.D.; Katschke, A.R.; Wools-Kaloustian, K. Task-shifting of antiretroviral delivery from health care workers to persons living with HIV/AIDS: Clinical outcomes of a community-based program in Kenya. J. Acquir. Immune Defic. Syndr. 2010, 55, 483–490. [Google Scholar] [CrossRef]
- Serrano, C.; Laporte, R.; Ide, M.; Nouhou, Y.; De Truchis, P.; Rouveix, E.; Adamou, A.; Pauly, V.; Mattei, J.F.; Gastaut, J.A. Family nutritional support improves survival, immune restoration and adherence in HIV patients receiving ART in developing country. Asia Pac. J. Clin. Nutr. 2010, 19, 68–75. [Google Scholar]
- Tirivayi, N.; Koethe, J.R.; Groot, W. Clinic-Based Food Assistance is Associated with Increased Medication Adherence among HIV-Infected Adults on Long-Term Antiretroviral Therapy in Zambia. J. AIDS Clin. Res. 2012, 3, 171. [Google Scholar] [CrossRef]
- Willis, N.; Milanzi, A.; Mawodzeke, M.; Dziwa, C.; Armstrong, A.; Yekeye, I.; Mtshali, P.; James, V. Effectiveness of community adolescent treatment supporters (CATS) interventions in improving linkage and retention in care, adherence to ART and psychosocial well-being: A randomised trial among adolescents living with HIV in rural Zimbabwe. BMC Public Health 2019, 19, 117. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Camacho-Minano, M.J.; LaVoi, N.M.; Barr-Anderson, D.J. Interventions to promote physical activity among young and adolescent girls: A systematic review. Health Educ. Res. 2011, 26, 1025–1049. [Google Scholar] [CrossRef] [PubMed]
- Hariton, E.; Locascio, J.J. Randomised controlled trials—The gold standard for effectiveness research. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 1716. [Google Scholar] [CrossRef]
- Evans, D. Hierarchy of evidence: A framework for ranking evidence evaluating healthcare interventions. J. Clin. Nurs. 2003, 12, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Bondemark, L.; Ruf, S. Randomized controlled trial: The gold standard or an unobtainable fallacy? Eur. J. Orthod. 2015, 37, 457–461. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. HIV/AIDS. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/hiv-aids (accessed on 15 January 2021).
- Margolis, A.M.; Heverling, H.; Pham, P.A.; Stolbach, A. A review of the toxicity of HIV medications. J. Med. Toxicol. 2014, 10, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.Y.; Hessol, N.A.; Vittinghoff, E.; Amico, K.R.; Kroboth, E.; Fuchs, J.; Irvin, R.; Sineath, R.C.; Sanchez, T.; Sullivan, P.S.; et al. Medication adherence among men who have sex with men at risk for HIV infection in the United States: Implications for pre-exposure prophylaxis implementation. AIDS Patient Care STDS 2014, 28, 622–627. [Google Scholar] [CrossRef]
- Ortego, C.; Huedo-Medina, T.B.; Llorca, J.; Sevilla, L.; Santos, P.; Rodríguez, E.; Warren, M.R.; Vejo, J. Adherence to highly active antiretroviral therapy (HAART): A meta-analysis. AIDS Behav. 2011, 15, 1381–1396. [Google Scholar] [CrossRef] [PubMed]
- Sangeda, R.Z.; Mosha, F.; Prosperi, M.; Aboud, S.; Vercauteren, J.; Camacho, R.J.; Lyamuya, E.F.; Van Wijngaerden, E.; Vandamme, A.M. Pharmacy refill adherence outperforms self-reported methods in predicting HIV therapy outcome in resource-limited settings. BMC Public Health 2014, 14, 1035. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, X.; Qiao, S.; Shen, Z.; Zhou, Y. Comparing self-reported medication adherence measures with hair antiretroviral concentration among people living with HIV in Guangxi, China. AIDS Res. Ther. 2020, 17, 8. [Google Scholar] [CrossRef]
- Gill, C.J.; Hamer, D.H.; Simon, J.L.; Thea, D.M.; Sabin, L.L. No room for complacency about adherence to antiretroviral therapy in sub-Saharan Africa. AIDS 2005, 19, 1243. [Google Scholar] [CrossRef]
- Crutzen, R.; Göritz, A.S. Social desirability and self-reported health risk behaviors in web-based research: Three longitudinal studies. BMC Public Health 2010, 10, 1–10. [Google Scholar] [CrossRef]
- Castillo-Mancilla, J.R.; Haberer, J.E. Adherence measurements in HIV: New advancements in pharmacologic methods and real-time monitoring. Curr. HIV AIDS Rep. 2018, 15, 49–59. [Google Scholar] [CrossRef]
- Grossberg, R.; Zhang, Y.; Gross, R. A time-to-prescription-refill measure of antiretroviral adherence predicted changes in viral load in HIV. J. Clin. Epidemiol. 2004, 57, 1107–1110. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.D.; Cantrell, R.A.; Mulenga, L.B.; Tambatamba, B.C.; Reid, S.E.; Levy, J.W.; Limbada, M.; Taylor, A.; Saag, M.S.; Vermund, S.H.; et al. Simple adherence assessments to predict virologic failure among HIV-infected adults with discordant immunologic and clinical responses to antiretroviral therapy. AIDS Res. Hum. Retrovir. 2008, 24, 1031–1035. [Google Scholar] [CrossRef]
- Warne, P.; Robbins, R.; Anderson, P.; Gouse, H.; Joska, J.; Leu, C.S.; Mtingeni, Y.; Henry, M.; Rios, J.L.; Castillo-Mancilla, J.; et al. Utility of Dried Blood Spot-Derived ARV Biomarkers as an Objective Measure of Treatment Adherence in South Africa; IAPAC Adherence: Miami, FL, USA, 2015. [Google Scholar]
- Samet, J.H.; Sullivan, L.M.; Traphagen, E.T.; Ickovics, J.R. Measuring adherence among HIV-infected persons: Is MEMS consummate technology? AIDS Behav. 2001, 5, 21–30. [Google Scholar] [CrossRef]
- Haberer, J.E. Actionable adherence monitoring to optimise intervention. Lancet HIV 2017, 4, e5–e6. [Google Scholar] [CrossRef]
- Garrison, L.E.; Haberer, J.E. Technological methods to measure adherence to antiretroviral therapy and preexposure prophylaxis. Curr. Opin. HIV Aids 2017, 12, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Pearson, C.R.; Simoni, J.M.; Hoff, P.; Kurth, A.E.; Martin, D.P. Assessing antiretroviral adherence via electronic drug monitoring and self-report: An examination of key methodological issues. AIDS Behav. 2007, 11, 161. [Google Scholar] [CrossRef] [PubMed]
- Bachman DeSilva, M.; Gifford, A.L.; Keyi, X.; Li, Z.; Feng, C.; Brooks, M.; Harrold, M.; Yueying, H.; Gill, C.J.; Wubin, X.; et al. Feasibility and acceptability of a real-time adherence device among HIV-positive IDU patients in China. AIDS Res. Treat. 2013, 2013, 957862. [Google Scholar] [CrossRef]
- Jimmy, B.; Jose, J. Patient medication adherence: Measures in daily practice. Oman Med. J. 2011, 26, 155. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.Y.; Fresco, P. Medication Adherence Measures: An Overview. Biomed. Res. Int. 2015, 2015, 217047. [Google Scholar] [CrossRef] [PubMed]
- Musayón-Oblitas, Y.; Carcamo, C.; Gimbel, S. Counseling for improving adherence to antiretroviral treatment: A systematic review. Aids Care 2019, 31, 4–13. [Google Scholar] [CrossRef]
- Zuge, S.S.; Paula, C.C.; Padoin, S.M. Effectiveness of interventions for adherence to antiretroviral therapy in adults with HIV: A systematic review. Rev. Esc. Enferm. Usp. 2020, 54, e03627. [Google Scholar] [CrossRef]
- Chaiyachati, K.H.; Ogbuoji, O.; Price, M.; Suthar, A.B.; Negussie, E.K.; Bärnighausen, T. Interventions to improve adherence to antiretroviral therapy: A rapid systematic review. AIDS 2014, 28, S187–S204. [Google Scholar] [CrossRef] [PubMed]
- NACA. National HIV/AIDS Strategic Framework 2017–2021. 2017. Available online: https://www.childrenandaids.org/sites/default/files/2017-11/NATIONAL-HIV-AND-AIDS-STRATEGIC-FRAMEWORK.pdf (accessed on 22 February 2021).
- UNAIDS. UNAIDS DATA 2017. 2017. Available online: https://www.unaids.org/sites/default/files/media_asset/20170720_Data_book_2017_en.pdf (accessed on 22 February 2021).


{kind=link}
| Author | Study Design | Intervention Category | Intervention Type | Study Country | Intervention Setting | Outcome | Adherence Measurement | Follow-Up Duration | Findings |
|---|---|---|---|---|---|---|---|---|---|
| Achieng et al. (2012) | Prospective cohort | Structural | Community health worker’s home visits, pharmacy counseling, community-based support groups, and unannounced pill counts by clinicians. | Kenya | Community-based | Time to treatment failure as defined by a detectable HIV-1 viral load | Pill count | 1 year | Time to treatment failure was longer in support groups. Better adherence and improved pill counts in support groups. |
| Atanga et al. (2018) | Prospective cohort | Structural | Option B+ | Cameroon | Hospital-based (outpatient) | Adherence |
| 1 year | Improvement in adherence was seen in the intervention group from 6 months to 12 months with 92.7% viral suppression. Low adherence was associated with treatment failure. |
| Bajunirwe et al. (2019) | Pre-post study | Structural, affective | Mobile ART pharmacy and counseling | Uganda | Community-based | Adherence, waiting time, viral suppression | Self-report | 1 year | No improvement in waiting time. Number of missed doses significantly declined 12 months post-intervention. Proportion of detectable viral load in patients decreased post-intervention. |
| Bhana et al. (2014) | Pilot randomized controlled trial | Affective | Counseling by lay counselors to pre-adolescents and their families (VUKA) vs. SOC | South Africa | Hospital-based (outpatient) | Adherence, treatment knowledge, care-giver communication, illness stigma | Self-report | 3 months | Greater improvements in ART adherence in VUKA post-intervention. |
| Boeke et al. (2018) | Pre-post study | Affective | Lay workers counseling | Uganda | Hospital-based (outpatient) | Adherence, linkage to care, retention | Appointment scheduling | 1 year 6 months | Adherence of patients to appointment schedules was improved. |
| Boruett et al. (2013) | Quasi-experimental, (cohort) | Behavioral | Clinic appointment diary, modifying self-report adherence questions, staff training, visiting support facilities and use of monitoring data vs. SOC | Kenya | Hospital-based | Adherence to medication and clinic appointment, |
| 11 months | There was maximum adherence (100%) in both groups and at baseline and pot-intervention. No change was observed. |
| Chime et al. (2018) | Cross-sectional | Affective | Peer Support groups vs. standard of care | Nigeria | Hospital-based (outpatient) | Adherence | Self-report | No post-intervention | Better adherence was seen in the intervention group compared to the control group. |
| Chung (2011) | Randomized controlled trial | Affective, behavioral | Counseling vs. alarm device vs. counseling + alarm, vs. SOC | Kenya | Hospital-based | Adherence, Viral load, CD4 count, mortality, | Pill count | 1 year 6 months | Adherence was significantly improved and treatment failure decreased post-intervention (18 months follow-up) whereas no significant impact on adherence and viral failure was observed for alarm use. |
| Coker et al. (2015) | Three-arm Randomized controlled trial | Behavioral, structural (combination) | Alarm daily reminder + follow up calls from peer educators + adherence support (CBAS) Vs. CBAS + home-based treatment partner + SOC | Nigeria | Community-based | Viral suppression |
| 9 months | There was no significant change in viral suppression between both (intervention and control) groups post-intervention. |
| Fatti et al. (2012) | Observational multicohort | Structural | Community-based adherence support (CBAS) | South Africa | Community-based | Viral suppression, Patient retention, and mortality rate |
| 5 years | There was significant difference in viral suppression between intervention and control groups 6 months post-intervention. |
| Gorman et al. (2015) | Retrospective cohort | Structural | Semi-mobile clinics | Kenya | Hospital-based (outpatient) | Adherence, CD4 count, mortality, HIV treatment retention | Pill count | 5 years | There was no change in adherence and CD4 count between intervention group and control group |
| Hickey et al. (2015) | Quasi experimental study (pre-post) | Structural | Microclinics vs. SOC | Kenya | Community-based | Linkage to care and ART concentration in hair |
| 6 months | The intervention group had less NVP hair concentration than control group. Microclinic could possibly improve ART adherence. |
| Holstad et al. (2012) | Quasi-experimental, two group post-test only design | Affective, Cognitive | Motivational interviewing (MI) vs. Health promotion program (HPP) | Nigeria | Hospital-based (outpatient) | Adherence, knowledge of HIV, condom use, safe sex |
| 6 months | Higher mean adherence in MI group compared to HPP post-intervention. |
| Igumbor et al. (2011) | Retrospective cohort | Affective | Adherence Treatment supporter (patient advocate) | South Africa | Community-based | Virologic outcome |
| 6 months | There was improved viral suppression in intervention group (<400 copies/mL) at 6 months; improved drug pickup rate of >95% and increased retention in care. |
| Jobanputra et al. (2015) | Retrospective cohort | Affective | Enhanced adherence counseling by lay counselors vs. SOC | Swaziland | Hospital-based (outpatient) | Viral suppression, CD4 count | Plasma viral load | 6 moths | No change in odds of viral re-suppression between EAC group and SOC post-intervention. |
| Jones et al. (2013) | Randomized controlled trial | Cognitive | Group patient education vs. individual patient education | Zambia | Hospital-based (outpatient) | Adherence to medication and clinic visits |
| 6 months | Participants of group intervention had enhanced adherence, but following crossover, gains were not sustained to the individual intervention. |
| Jones et al. (2018) | Randomized controlled trial (RCT) | Cognitive | Active visualization | South Africa | Hospital-based (outpatient) | Adherence measured by viral load | Plasma viral load | 2 months | There was change in viral load scores and higher suppression in intervention group |
| Kalichman et al. (2018) | Randomized controlled trial (RCT) | Behavioral | Mobile phone counseling vs. a contact matched control | South Africa | Hospital-based (outpatient) | Adherence | Self-report using VAS | 2 weeks | Intervention group significantly improved in ART adherence post-intervention |
| Kunutsor et al. (2011) | Two-arm Randomized controlled trial | Affective | Treatment supporter (TS) vs. SOC | Uganda | Hospital-outpatient (Rural) | Adherence and clinic attendance for refills | Pill count | 7 months | TS participants had greater optimal adherence. |
| Kiweewa et al. (2013) | Randomized controlled trial | Affective | Peer support counseling | Uganda | Hospital-based (outpatient) | Adherence, virologic suppression | Pill count | 1 year | No change in adherence and viral suppression between intervention and control groups. |
| Maduka and Tobin-West (2013) | Randomized Controlled Trial | Affective, behavioral | Adherence counseling, mobile-phone text messages, Standard of Care | Nigeria | Hospital-based (Urban) | Adherence, Immunological outcome | Self-report | 4 months | The intervention group had higher adherence and CD4 count than control group post-intervention. |
| Mbuagbaw et al. (2012) | Randomized controlled trial | Behavioral | Text messages vs. standard of care | Cameroon | Hospital-based (outpatient) | Adherence |
| 6 months | No significant effect was seen between groups post-intervention. |
| Moosa and Jeenah (2012) | Prospective Randomized Controlled Trial | Affective, | Interpersonal psychotherapy vs. pharmacotherapy | South Africa | Hospital-based | Adherence |
| 6 months | Adherence improved greater in the intervention group compared to the control group |
| Obua et al. (2014) | Cohort | Behavioral | Appointment system, fast-tracking, longer prescription | Uganda | Hospital-based-outpatient | Adherence |
| 1 year | Reduced missed appointments improved adherence |
| Orrell et al. (2015) | Randomized Controlled Trial | Behavioral | Text messages vs. standard of care | South Africa | Hospital-outpatient | Adherence, viral load treatment interruption count | Electronic adherence monitoring device (EAMD) | 1 year | Although not statistically significant, mean ART adherence increased more in intervention group. However, viral suppression was more in control group. |
| Peltzer et al. (2012) | Two-armed Randomized Controlled Trial (RCT) | Cognitive | Medication Adherence Training + structured three session group intervention vs. Standard of Care (SOC) | South Africa | Hospital-bases (outpatient) | Adherence, Immunologic outcome, depression level | Self-report | 3 months | Intervention group had more increase in ART adherence and CD4 count. |
| Robbins et al. (2015) | Randomized controlled trial | Combination (cognitive and affective) | Media education (masivukeni) vs. standard of care counseling | South Africa | Hospital-based (outpatient) | Adherence, |
| 6 weeks | Intervention group experienced more increase in adherence while control group decreased. |
| Selke et al. (2012) | Prospective cluster randomized controlled clinical trial | Structural | Community-based care by personal digital assistant vs. SOC | Kenya | Community-based | Adherence, Viral load, CD4 count, |
| 1 year | No statistical significance between intervention and control arms at 6 months and 12 months |
| Serrano et al. (2010) | Retrospective cohort | Biological | Family nutritional support + nutritional advice vs. SOC | Niger | Hospital-based (outpatient) | Adherence |
| 6 months | Increased mean adherence post-intervention and improved CD4 count. |
| Tirivayi et al. (2012) | Retrospective cohort | Biological vs. SOC | Food ration (Food assistance) | Zambia | Hospital-based | Adherence, weight gain, CD4 count | Pill count (medication possession ratio) | 6 months | Intervention arm had higher ART adherence however, there was no change in CD4 count and weight. |
| Willis et al. (2019) | Randomized controlled trial (RCT) | Affective, behavioral | Community adolescent treatment supporter (CATS), pill boxes, monthly support group vs. SOC | Zimbabwe | Community-based | Adherence, psychological wellbeing, quality of life | Self-report | 1 year | The intervention arm had more likelihood of adhering to ART than the control arm. |
| Categories | Description | Examples |
|---|---|---|
| Affective | Using emotional support to affect ART adherence | Peer support (social support) Treatment with antidepressants counseling |
| Behavioral | Using direct behavior modification to affect ART adherence | Reminder devices (like pill boxes, alarms, mobile-phone text messages, pager messages)Cash incentives Directly Observed Therapy (DOT) |
| Biological | Using improved physical ability to take ART to affect ART adherence | Vitamin/micronutrient supplements Food rations/assistance |
| Cognitive | Using teaching, clarification or instruction to affect ART adherence | Patient education Media education materials (such as audio, video, or reading materials) |
| Combination | Using a combination of one more intervention categories to affect ART adherence | Peer support, Patient education Food rations |
| Structural | Using changes in the delivery structure or additional service structures to affect ART adherence | ART delivery in community centers Income-generating activities for ART patients Community mobilization |
| Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Total n (%) | Bias | |
|---|---|---|---|---|---|---|---|---|---|
| Achieng et al. (2012) | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 (29%) | High |
| Atanga et al. (2018) | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 3 (43%) | Low |
| Bajunirwe et al. (2019) | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 (29%) | High |
| Bhana et al. (2014) | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (14%) | High |
| Boeke et al. (2018) | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 3 (43%) | Low |
| Boruett et al. (2013) | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 3 (43%) | Low |
| Chime et al. (2018) | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 3 (43%) | Low |
| Chung (2011) | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 2 (29%) | High |
| Coker et al. (2015) | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 5 (71%) | Low |
| Fatti et al. (2012) | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 (29%) | High |
| Gorman et al. (2015) | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 (29%) | High |
| Hickey et al. (2015) | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 (29%) | High |
| Holstad et al. (2012) | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 (29%) | High |
| Igumbor et al. (2011) | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 (29%) | High |
| Jobanputra et al. (2015) | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 (29%) | High |
| Jones et al. (2013) | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 4 (57%) | Low |
| Jones et al. (2018) | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 4 (57%) | Low |
| Kalichman et al. (2018) | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 5 (71%) | Low |
| Kunutsor et al. (2011) | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (14%) | High |
| Kiweewa et al. (2013) | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 4 (57%) | Low |
| Maduka and Tobin-West (2013) | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 6 (86%) | Low |
| Mbuagbaw et al. (2012) | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 6 (86%) | Low |
| Moosa and Jeenah (2012) | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 (14%) | High |
| Obua et al. (2014) | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 3 (43%) | Low |
| Orrell et al. (2015) | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 5 (71%) | Low |
| Peltzer et al. (2012) | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 3 (43%) | Low |
| Robbins et al. (2015) | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 3 (43%) | Low |
| Selke et al. (2012) | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 4 (57%) | Low |
| Serrano et al. (2010) | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 2 (29%) | High |
| Tirivayi et al. (2012) | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 3 (43%) | Low |
| Willis et al. (2019) | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 3 (43%) | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damulak, P.P.; Ismail, S.; Abdul Manaf, R.; Mohd Said, S.; Agbaji, O. Interventions to Improve Adherence to Antiretroviral Therapy (ART) in Sub-Saharan Africa: An Updated Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 2477. https://doi.org/10.3390/ijerph18052477
Damulak PP, Ismail S, Abdul Manaf R, Mohd Said S, Agbaji O. Interventions to Improve Adherence to Antiretroviral Therapy (ART) in Sub-Saharan Africa: An Updated Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(5):2477. https://doi.org/10.3390/ijerph18052477
Chicago/Turabian StyleDamulak, Panmial Priscilla, Suriani Ismail, Rosliza Abdul Manaf, Salmiah Mohd Said, and Oche Agbaji. 2021. "Interventions to Improve Adherence to Antiretroviral Therapy (ART) in Sub-Saharan Africa: An Updated Systematic Review" International Journal of Environmental Research and Public Health 18, no. 5: 2477. https://doi.org/10.3390/ijerph18052477
APA StyleDamulak, P. P., Ismail, S., Abdul Manaf, R., Mohd Said, S., & Agbaji, O. (2021). Interventions to Improve Adherence to Antiretroviral Therapy (ART) in Sub-Saharan Africa: An Updated Systematic Review. International Journal of Environmental Research and Public Health, 18(5), 2477. https://doi.org/10.3390/ijerph18052477