
Community-Level Experiences, Understandings, and Responses to COVID-19 in Low- and Middle-Income Countries: A Systematic Review of Qualitative and Ethnographic Studies



Abstract
1. Introduction
2. Materials and Methods

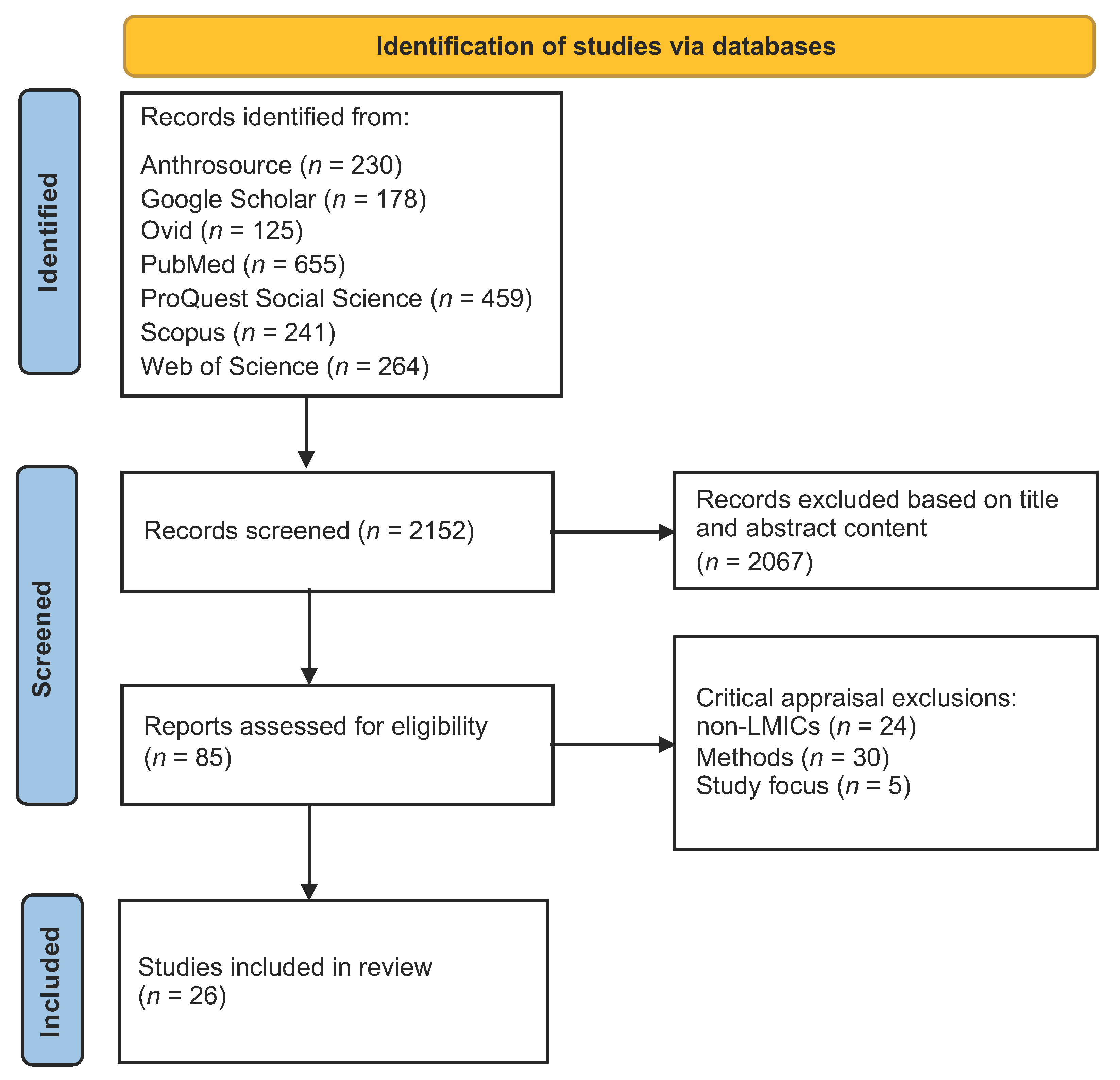{kind=link}
{kind=link}
| Citation | Country | COVID-19 Focus | Target Pop. | Article Title and Key Outcomes | Approaches |
|---|---|---|---|---|---|
| Adom et al. [57] | Ghana | Stigma and mental distress | HCWs and patients | The psychological distress and mental health disorders from COVID-19 stigmatization in Ghana—Stigma and psychological distress among HCWs, patients, and others; psychosocial recommendations for policy change | Phenomenology |
| Ali [58] | Pakistan | COVID-19 burials | Local community | Rituals of containment: many pandemics, body politics, and social dramas during COVID-19 in Pakistan—Ethnography of funeral rites in the context of COVID-19 government restrictions; changes in burial traditions; social consequences; entanglement of science, religion and politics | Social drama, symbolic ownership of the “viral body” by the state, liminality and grief, death traditions |
| Ali et al. [59] | Pakistan | Mental health, perceptions | Local community | When COVID-19 enters in a community setting: an exploratory qualitative study of community perspectives on COVID-19 affecting mental well-being—Anxiety and fear, social, financial and religious crises and distress. Coping: becoming closer to God and family, participating in mental health sessions, and resetting lives | Qualitative, descriptive |
| Amir [60] | Uganda | Stigma and mental distress | Recovered COVID-19 patients | COVID-19 and its related stigma: A qualitative study among survivors in Kampala, Uganda—Narratives of stigma experiences, social rejection, labeling and distress | Qualitative, descriptive, narrative |
| Asiimwe et al. [61] | Ghana | Perceptions of contact tracing | Contact tracers, contacts, and supervisors | Stakeholders’ perspective of, and experience with, contact tracing for COVID-19 in Ghana: A qualitative study among contact tracers, supervisors, and contacts—Perceptions of utility and effectiveness of COVID-19 contact tracing among implementing bureaucrats and recipients; generally positive experiences and expressed concerns of stigma associated with home visits | Phenomenology, narrative, Lipsky’s street-level bureaucrats theory |
| Bahagia et al. [62] | Indonesia | Local wisdom, food security and livelihoods | Community leaders | Local wisdom to overcome the COVID-19 pandemic of Urug and Cipatat Kolot societies in Bogor, West Java, Indonesia—Food redistribution, collective action through nujuh bulanan, instigating taboos, Indigenous knowledge that combats “life perturbations” | Qualitative, ethnography of local knowledge (ceremonies, taboos, rituals), descriptive |
| Bhatt et al. [63] | Nepal | Perceptions, understanding, and prevention | Local community | Perceptions and experiences of the public regarding the COVID-19 pandemic in Nepal: a qualitative study using phenomenological analysis—Knowledge measures, social isolation, inadequate PPE, disorganized public sector | Phenomenology, lived experience |
| Ekoh et al. [64] | Nigeria | Effects of social restrictions | Above 60-aged community | Digital and physical social exclusion of older people in rural Nigeria in the time of COVID-19—The elderly are digitally and socially excluded due to pandemic restrictions, leading to loneliness and lack of coping | Qualitative, descriptive |
| Ghani and Sitohang [65] | Indonesia | Knowledge and responses of community | Remote Indigenous community | How people in remote areas react to the COVID-19 pandemic in the early phase—Hoaxes predominate and circulate widely; with limited access to reliable information, there is a need to improve access to reliable information and quell hoaxes | Digital vicious cycle, “illusory truth effect”, bullet theory of communication |
| Jones [66] | Sierra Leone | Experiences of state-led COVID-19 measures | Urban and rural communities | An ethnographic examination of people’s reactions to state-led COVID-19 measures in Sierra Leone—Adaptation, non-compliance, passive, and active resistance; heterogeneous responses by communities | Adaptive capacity, compliance, passive, active resistance theories; social and financial capital |
| Kumari et al. [67] | India | Psychosocial functioning | Peripartum women | Impact of COVID-19 on psychosocial functioning of peripartum women: a qualitative study comprising focus group discussions and in-depth interviews—Peripartum women experienced distress, anxiety due to pandemic confinement, and social restrictions during and after pregnancy | Qualitative, descriptive |
| Kwaghe et al. [68] | Nigeria | Stigma, trauma | Frontline HCWs | Stigmatization, psychological and emotional trauma among frontline health care workers treated for COVID-19 in Lagos State, Nigeria: a qualitative study—Knowledge assessed for biomedical understanding; experienced stigma and social reactions from family and community; insights into improving health care quality based on experiences | Colaizzi’s phenomenological method |
| Newton et al. [69] | Ghana | Health-seeking behavior | Above 60-aged community | Understanding older adults’ functioning and health-seeking behavior during the COVID-19 pandemic in Ghana—Reporting physical and emotional health during the pandemic; challenges of loneliness and health-seeking restrictions and health provider attitudes | Qualitative Thematic Analysis, descriptive |
| Nicoletti et al. [70] | Bolivia | Patient experiences | Rural patients with epilepsy | The impact of COVID-19 pandemic on frail health systems of low- and middle-income countries: The case of epilepsy in the rural areas of the Bolivian Chaco—Patients with epilepsy in remote Bolivia experienced drug stockouts and lack of access to health care; 75% had inconsistent medication use during COVID-19 lockdowns | Qualitative, descriptive |
| Okediran et al. [71] | Nigeria | Experiences and perceptions | Frontline HCWs | The experiences of healthcare workers during the COVID-19 crisis in Lagos, Nigeria: a qualitative study—Four themes identified around responsibilities, challenges and coping strategies, experiences of distress and pleasure, and recommended needs for further material and social support | Qualitative, descriptive |
| Østebø et al. [72] | Ethiopia | Religious and secular perspectives | Local community | Religion and the “secular shadow”: responses to COVID-19 in Ethiopia—Conflations of science and religion, tradition and modernity in the Ethiopian context as local perceptions are considered in the development of public health interventions, exploring epistemic tensions | Qualitative, ethnographic, Latour, coexisting epistemologies, modernity |
| Prajitha et al. [73] | India | Government responses | Government bureaucrats | Strategies and challenges in Kerala’s response to the initial phase of COVID-19 pandemic: a qualitative descriptive study—Five themes emerged in reflecting on government responses, recognizing key components of social capital, a robust public health system, participation and volunteerism, health system preparedness, and challenges | Qualitative, descriptive, social capital, SDH |
| Prasetyo et al. [74] | Indonesia | Civil society participation | Task Force members | Civil Society participation in efforts to prevent the spread of COVID-19—Four task forces engaged: public education, controlling mobility via gate system, hand washing, and food needs/suspected patient monitoring, etc. Lack of funds and lack of public awareness were the main obstacles | Civil society engagement |
| Prasetyono et al. [75] | Indonesia | Leadership and local governance | Village heads | Patron-client relationship between village heads and their residents during the COVID-19 pandemic—Village leaders influence public opinion and awareness, consolidate volunteers and information, facilitate social assistance. Patron-client relationship between village head and residents, seen as a “father protector” | Qualitative, patron–client theories, power relations in bureaucracy |
| Samuelsen and Toé [76] | Burkina Faso | Ruptures in politics and life | Local community | COVID-19 temporalities: Ruptures of everyday life in urban Burkina Faso: Investigated community responses to government-led restrictions as prevention prior to the advent of COVID-19 in Burkina Faso, placed within the socio-economic, political, and fragile security contexts at the time | Qualitative, anthropology, Giddens “time-space distanciation”, outbreak narratives |
| Sari et al. [77] | Indonesia | Social protection with village fund | Community and leaders | The Effectiveness of Tri Hita Karana-based traditional village management in COVID-19 prevention in Bali—Experience in managing the village fund for social protection during COVID-19, using traditional Tri Hita Karana philosophy. Local wisdom provides positive outcomes for village resource distribution and social protection | Tri Hita Karana Hindu philosophy |
| Sharma et al. [78] | India | Information, media, andpsychosocial experiences | Local community | Panic during COVID-19 pandemic! A qualitative investigation into the psychosocial experiences of a sample of Indian people—Misinformation causes panic and anxiety; quarantines and social restrictions created cognitive dissonance | Qualitative, descriptive, social psychology, grounded theory |
| Sukmawan [79] | Indonesia | Traditional rituals | Local community | Tradition-responsive approach as a non-medical treatment in mitigating the COVID-19 pandemic in Tengger, East Java, Indonesia—Nambak lelakon, an adaptation of traditional tolak bala ritual in East Java, used to maintain and protect human life through the collective non-medical mitigation of COVID-19. Use of this ritual instills harmony in the community and is a form of prayer and surrender to God | Qualitative, psychosocial, religious |
| Sumesh and Gogoi [80] | India | Stigma, discrimination | Recovered COVID-19 patients | Collecting the “Thick Descriptions”: A pandemic ethnography of the lived experiences of COVID-19-induced stigma and social discrimination in India—Embodied experience of stigma; former patients discriminated against and criminalized; social process of stigma analyzed | Pandemic ethnography, lived experience, grounded theory, Geertz, Goffman, narrative |
| Tan and Lasco [81] | Philippines | Local knowledge | Traditional community | ‘Hawa’ and ‘resistensiya’: local health knowledge and the COVID-19 pandemic in the Philippines—Ethnographic study of “contagion” and “immunity” framing in illness understanding and explanatory models for COVID-19; multiple ontologies/traditional knowledge | Ethnography, postcolonialism, risk theory, political economy |
| Wibisono et al. [82] | Indonesia | Religious exclusion and xenophobia | Muslim community | Turning religion from cause to reducer of panic during the COVID-19 pandemic—Explored ways to reduce social exclusion and reactions via religious cohesion in a traditional community | Collaborative auto-ethnography, Weber’s verstehen, Geertz |
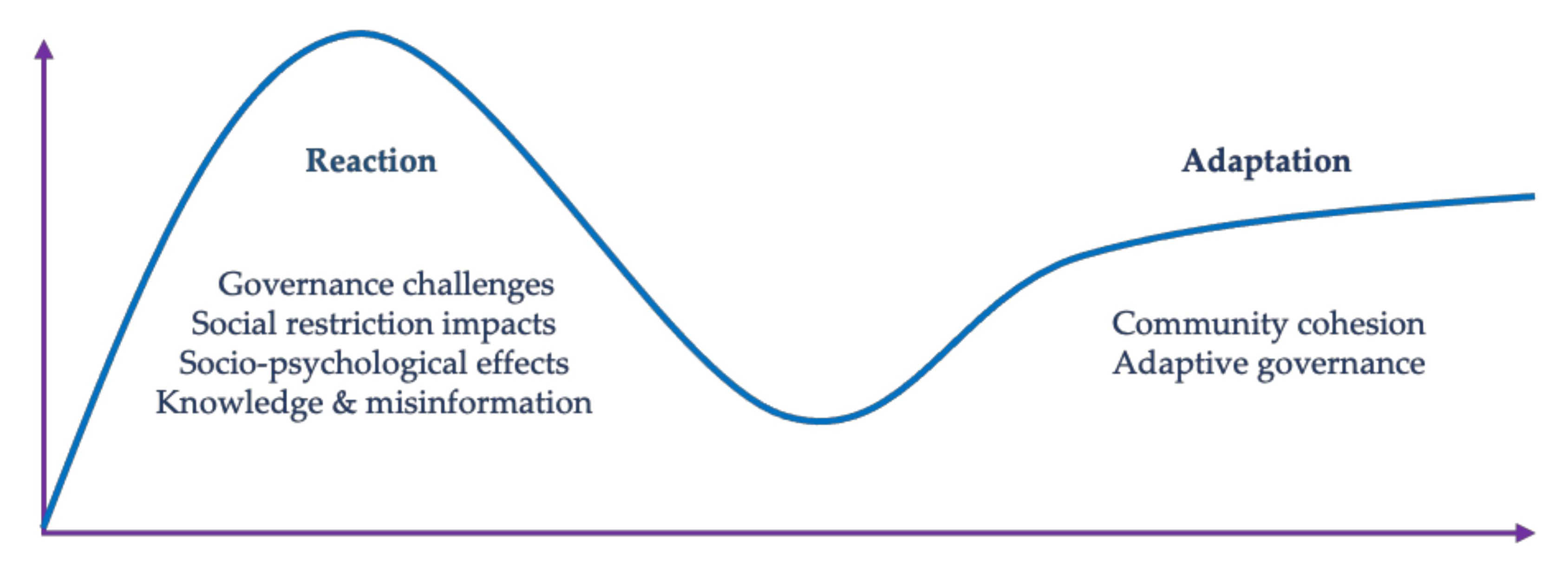
3. Results
3.1. Reactive Responses
3.1.1. COVID-19 Biomedical Knowledge and Misinformation
Believe it or not. This afternoon, did anyone hear the thunder when it was hot (not raining)? There was a true incident from Popay today. A baby was born this afternoon, and before the attendants could cut the umbilical cord, it spoke and said, “To avoid the coronavirus, you must boil an egg”. Immediately after, a strong thunderclap was heard and the baby began crying [65].
3.1.2. Social and Psychological Effects
3.1.3. Impacts of Social and Mobility Restrictions
3.1.4. Pandemic Governance and Health System Challenges
3.2. Adaptive Responses
Community Cohesion and Adaptive Governance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wade, D.T.; Halligan, P.W. The biopsychosocial model of illness: A model whose time has come. Clin. Rehabil. 2017, 31, 995–1004. [Google Scholar] [CrossRef]
- Trout, L.J.; Kleinman, A. COVID-19 Requires a social medicine response. Front. Sociol. 2020, 5, 579991. [Google Scholar] [CrossRef] [PubMed]
- Hopman, J.; Allegranzi, B.; Mehtar, S. Managing COVID-19 in low-and middle-income countries. JAMA 2020, 323, 1549. [Google Scholar] [CrossRef]
- WHO. Critical Preparedness, Readiness and Response Actions for COVID-19: Interim Guidance, 22 March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. Novel Coronavirus (2019-nCoV): Strategic Preparedness and Response Plan; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- JHU. COVID-19 Dashboard; Center for Systems Science and Engineering, Johns Hopkins University: Baltimore, MD, USA, 2021. [Google Scholar]
- WHO. WHO Coronavirus (COVID-19) Dashboard; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Team, V.; Manderson, L. How COVID-19 reveals structures of vulnerability. Med. Anthropol. 2020, 39, 671–674. [Google Scholar] [CrossRef]
- Chao, S. Health, Harm, Habitus: Techniques of the Body in COVID-19. Thesis Eleven: Critical Theory and Historical Sociology. Available online: https://thesiseleven.com/2020/07/07/health-harm-habitus-techniques-of-the-body-in-covid-19/ (accessed on 10 September 2021).
- Friedler, A. Sociocultural, behavioural and political factors shaping the COVID-19 pandemic: The need for a biocultural approach to understanding pandemics and (re)emerging pathogens. Glob. Public Health 2021, 16, 17–35. [Google Scholar] [CrossRef]
- Zakar, R.; Yousaf, F.; Zakar, M.Z.; Fischer, F. Sociocultural challenges in the implementation of COVID-19 public health measures: Results from a qualitative study in Punjab, Pakistan. Front. Public Health 2021, 9, 703825. [Google Scholar] [CrossRef]
- Shadmi, E.; Chen, Y.; Dourado, I.; Faran-Perach, I.; Furler, J.; Hangoma, P.; Hanvoravongchai, P.; Obando, C.; Petrosyan, V.; Rao, K.D.; et al. Health equity and COVID-19: Global perspectives. Int. J. Equity Health 2020, 19, 104. [Google Scholar] [CrossRef]
- Gill, I.; Schellekens, P. COVID-19 is a developing country pandemic. In Future Development; The Brookings Institution: Washington, WA, USA, 2021. [Google Scholar]
- Economist. There Have been 7m–13m Excess Deaths Worldwide during the Pandemic. Available online: https://www.economist.com/briefing/2021/05/15/there-have-been-7m-13m-excess-deaths-worldwide-during-the-pandemic (accessed on 15 September 2021).
- Economist. COVID-19 Global Excess Deaths Model; The Economist. Available online: https://www.economist.com/graphic-detail/coronavirus-excess-deaths-estimates (accessed on 15 September 2021).
- WHO. COVID-19 Weekly Epidemiological and Operational Updates. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 1 September 2021).
- Bell, G. Pandemic passages: An anthropological account of life and liminality during COVID-19. Anthropol. Action 2021, 28, 79–84. [Google Scholar] [CrossRef]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Lupton, D. Contextualising COVID-19: Sociocultural perspectives on contagion. In The COVID-19 Crisis: Social Perspectives; Lupton, D., Willis, K., Eds.; Routledge: London, UK, 2020. [Google Scholar]
- Manderson, L.; Levine, S. COVID-19, risk, fear, and fall-out. Med. Anthropol. 2020, 39, 367–370. [Google Scholar] [CrossRef]
- Sciortino, R. COVID-19: Learning from past funding initiatives and their dismissal in Southeast Asia. Etropic: Electron. J. Stud. Trop. 2021, 20, 182–201. [Google Scholar] [CrossRef]
- Venables, E.; Pellecchia, U. Engaging anthropology in an Ebola outbreak. Anthropol. Action 2017, 24, 1–8. [Google Scholar] [CrossRef]
- Abramowitz, S. Epidemics (Especially Ebola). Annu. Rev. Anthropol. 2017, 46, 421–445. [Google Scholar] [CrossRef]
- Richardson, E.T.; Barrie, M.B.; Kelly, J.D.; Dibba, Y.; Koedoyoma, S.; Farmer, P.E. Biosocial approaches to the 2013-2016 Ebola pandemic. Health Hum. Rights 2016, 18, 115–128. [Google Scholar] [PubMed]
- Guarner, J. Three emerging coronaviruses in two decades the story of SARS, MERS, and now COVID-19. Am. J. Clin. Pathol. 2020, 153, 420–421. [Google Scholar] [CrossRef]
- Fidler, D.P. Germs, governance, and global public health in the wake of SARS. J. Clin. Investig. 2004, 113, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Crawford, R.; Rutz, D.C.; Evans, D.P. ‘Between combat boots and Birkenstocks’–Lessons from HIV/AIDS, SARS, H1N1 and Ebola. Public Health 2016, 141, 186–191. [Google Scholar] [CrossRef]
- Eaton, L.A.; Kalichman, S.C. Social and behavioral health responses to COVID-19: Lessons learned from four decades of an HIV pandemic. J. Behav. Med. 2020, 43, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Adams, V.; Nading, A. Medical anthropology in the time of COVID-19. Med. Anthropol. Q. 2020, 34, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Higgins, R.; Martin, E.; Vesperi, M.D. An anthropology of the COVID-19 pandemic. Anthropol. Now 2020, 12, 2–6. [Google Scholar] [CrossRef]
- Daniels, K.; Hanefeld, J.; Marchal, B. Social sciences: Vital to improving our understanding of health equity, policy and systems. Int. J. Equity Health 2017, 16. [Google Scholar] [CrossRef]
- Campbell, D. Anthropology’s contribution to public health policy development. Mcgill J. Med. 2011, 13, 76. [Google Scholar] [CrossRef]
- Santana, F.N.; Hammond Wagner, C.; Berlin Rubin, N.; Bloomfield, L.S.P.; Bower, E.R.; Fischer, S.L.; Santos, B.S.; Smith, G.E.; Muraida, C.T.; Wong-Parodi, G. A path forward for qualitative research on sustainability in the COVID-19 pandemic. Sustain. Sci. 2021, 16, 1061–1067. [Google Scholar] [CrossRef]
- Rahman, S.A.; Tuckerman, L.; Vorley, T.; Gherhes, C. Resilient research in the field: Insights and lessons from adapting qualitative research projects during the COVID-19 pandemic. Int. J. Qual. Methods 2021, 20, 160940692110161. [Google Scholar] [CrossRef]
- UTS. Adapting Research Methodologies in the COVID-19 Pandemic: Resources for Researchers; University of Washington: Seattle, WA, USA, 2020. [Google Scholar]
- Lupton, D. Doing Fieldwork in a Pandemic (Crowd-Sourced Document). 2020. Revised Version. Available online: https://docs.google.com/document/d/1clGjGABB2h2qbduTgfqribHmog9B6P0NvMgVuiHZCl8/edit?ts=5e88ae0a# (accessed on 5 September 2021).
- Tremblay, S.; Castiglione, S.; Audet, L.-A.; Desmarais, M.; Horace, M.; Peláez, S. Conducting qualitative research to respond to COVID-19 challenges: Reflections for the present and beyond. Int. J. Qual. Methods 2021, 20, 160940692110096. [Google Scholar] [CrossRef]
- Sah, L.; Singh, D.R.; Sah, R.K. Conducting qualitative interviews using virtual communication tools amid COVID-19 pandemic: A learning opportunity for future research. J. Nepal. Med. Assoc. 2020, 58, 1103. [Google Scholar] [CrossRef] [PubMed]
- Vindrola-Padros, C.; Chisnall, G.; Cooper, S.; Dowrick, A.; Djellouli, N.; Symmons, S.M.; Martin, S.; Singleton, G.; Vanderslott, S.; Vera, N.; et al. Carrying out rapid qualitative research during a pandemic: Emerging lessons from COVID-19. Qual. Health Res. 2020, 30, 2192–2204. [Google Scholar] [CrossRef]
- Teti, M.; Schatz, E.; Liebenberg, L. Methods in the time of COVID-19: The vital role of qualitative inquiries. Int. J. Qual. Methods 2020, 19, 160940692092096. [Google Scholar] [CrossRef]
- Nichter, M.; Hedges, K.; Cartwright, E. Call to Action: Influence of Medical Anthropology for COVID-19 Response; Anthropological Responses to Health Emergencies SIG: Tuscon, AZ, USA, 2020. [Google Scholar]
- Lupton, D. Social Research for a COVID and Post-COVID World: An Initial Agenda. Available online: https://medium.com/@deborahalupton/social-research-for-a-covid-and-post-covid-world-an-initial-agenda-796868f1fb0e (accessed on 1 August 2021).
- Ward, P.R. A sociology of the COVID-19 pandemic: A commentary and research agenda for sociologists. J. Sociol. 2020, 56, 726–735. [Google Scholar] [CrossRef]
- Novick, G. Is there a bias against telephone interviews in qualitative research? Res. Nurs. Health 2008, 31, 391–398. [Google Scholar] [CrossRef]
- Denzin, N.K.; Lincoln, Y.S. The Sage Handbook of Qualitative Research, 5th ed.; Los Angeles Sage: Los Angeles, CA, USA, 2017. [Google Scholar]
- JBI. Joanna Briggs Institute Critical Appraisal Tools; University of Adelaide: Adelaide, Australia, 2015. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 89. [Google Scholar] [CrossRef]
- OED. Reaction. Available online: https://www-oed-com./view/Entry/158836?redirectedFrom=reaction#eid (accessed on 5 September 2021).
- OED. Adaptation. Available online: https://www-oed-com/view/Entry/2115?redirectedFrom=adaptation#eid (accessed on 5 September 2021).
- Keck, M.; Sakdapolrak, P. What is social resilience? Lessons learned and ways forward. Erdkd. Arch. Sci. Geogr. 2013, 67, 5–19. [Google Scholar] [CrossRef]
- Ungar, M. Resilience across cultures. Br. J. Soc. Work 2006, 38, 218–235. [Google Scholar] [CrossRef]
- Bryce, C.; Ring, P.; Ashby, S.; Wardman, J.K. Resilience in the face of uncertainty: Early lessons from the COVID-19 pandemic. J. Risk Res. 2020, 23, 880–887. [Google Scholar] [CrossRef]
- Meyer, A.D. Adapting to environmental jolts. Adm. Sci. Q. 1982, 27, 515. [Google Scholar] [CrossRef]
- Weick, K.E.; Sutcliffe, K.M. Managing the Unexpected: Resilient Performance in an Age of Uncertainty, 2nd ed.; John Wiley: New York, NY, USA; Jossey-Bass: San Francisco, CA, USA, 2007. [Google Scholar]
- Evans-Pritchard, E.E. Witchcraft, Oracles and Magic among the Azande; Clarendon Press: Oxford, UK, 1937. [Google Scholar]
- Panter-Brick, C. Health, risk, and resilience: Interdisciplinary concepts and applications. Annu. Rev. Anthropol. 2014, 43, 431–448. [Google Scholar] [CrossRef]
- Adom, D.; Mensah, J.A.; Osei, M. The psychological distress and mental health disorders from COVID-19 stigmatization in Ghana. Soc. Sci. Humanit. Open 2021, 4, 100186. [Google Scholar] [CrossRef] [PubMed]
- Ali, I. Rituals of containment: Many pandemics, body politics, and social dramas during COVID-19 in Pakistan. Front. Sociol. 2021, 6, 648149. [Google Scholar] [CrossRef]
- Ali, N.A.; Feroz, A.S.; Akber, N.; Feroz, R.; Nazim Meghani, S.; Saleem, S. When COVID-19 enters in a community setting: An exploratory qualitative study of community perspectives on COVID-19 affecting mental well-being. BMJ Open 2021, 11, e049851. [Google Scholar] [CrossRef] [PubMed]
- Amir, K. COVID-19 and its related stigma: A qualitative study among survivors in Kampala, Uganda. Stigma Health 2021, 6, 272–276. [Google Scholar] [CrossRef]
- Asiimwe, N.; Tabong, P.T.-N.; Iro, S.A.; Noora, C.L.; Opoku-Mensah, K.; Asampong, E. Stakeholders perspective of, and experience with contact tracing for COVID-19 in Ghana: A qualitative study among contact tracers, supervisors, and contacts. PLoS ONE 2021, 16, e0247038. [Google Scholar] [CrossRef]
- Bahagia, B.; Bambang, H.; Rimun, W.; Zuzy, A. Local wisdom to overcome COVID-19 pandemic of Urug and Cipatat Kolot societies in Bogor, West Java, Indonesia. Forum Geogr. 2020, 34, 2. [Google Scholar] [CrossRef]
- Bhatt, N.; Bhatt, B.; Gurung, S.; Dahal, S.; Jaishi, A.R.; Neupane, B.; Budhathoki, S.S. Perceptions and experiences of the public regarding the COVID-19 pandemic in Nepal: A qualitative study using phenomenological analysis. BMJ Open 2020, 10, e043312. [Google Scholar] [CrossRef]
- Ekoh, P.C.; George, E.O.; Ezulike, C.D. Digital and physical social exclusion of older people in rural Nigeria in the time of COVID-19. J. Gerontol. Soc. Work 2021, 64, 629–642. [Google Scholar] [CrossRef] [PubMed]
- Ghani, M.; Sitohang, M. How people in remote areas react to the COVID-19 pandemic in the early phase. Masy. Indones. Maj. Ilmu-Ilmu Sos. Indones. 2020, 46, 168–179. [Google Scholar] [CrossRef]
- Jones, J. An ethnographic examination of people’s reactions to state-led COVID-19 measures in Sierra Leone. Eur. J. Dev. Res. 2021, 899, 1–18. [Google Scholar] [CrossRef]
- Kumari, A.; Ranjan, P.; Sharma, K.A.; Sahu, A.; Bharti, J.; Zangmo, R.; Bhatla, N. Impact of COVID-19 on psychosocial functioning of peripartum women: A qualitative study comprising focus group discussions and in-depth interviews. Int. J. Gynecol. Obstet. 2021, 152, 321–327. [Google Scholar] [CrossRef]
- Kwaghe, A.V.; Ilesanmi, O.S.; Amede, P.O.; Okediran, J.O.; Utulu, R.; Balogun, M.S. Stigmatization, psychological and emotional trauma among frontline health care workers treated for COVID-19 in Lagos State, Nigeria: A qualitative study. BMC Health Serv. Res. 2021, 21, 855. [Google Scholar] [CrossRef]
- Newton, A.; Awuviry-Newton, K.; Oppong Nkansah, J.; Abekah-Carter, K. Understanding older adults’ functioning and health-seeking behaviour during the COVID-19 pandemic in Ghana: A descriptive qualitative study. Health Soc. Care Community 2021, 00, 1–9. [Google Scholar] [CrossRef]
- Nicoletti, A.; Todaro, V.; Cicero, C.E.; Giuliano, L.; Zappia, M.; Cosmi, F.; Vilte, E.; Bartoloni, A.; Crespo Gómez, E.B. The impact of COVID-19 pandemic on frail health systems of low-and middle-income countries: The case of epilepsy in the rural areas of the Bolivian Chaco. Epilepsy Behav. 2021, 118, 107917. [Google Scholar] [CrossRef]
- Okediran, J.O.; Ilesanmi, O.S.; Fetuga, A.A.; Onoh, I.; Afolabi, A.A.; Ogunbode, O.; Olajide, L.; Kwaghe, A.V.; Balogun, M.S. The experiences of healthcare workers during the COVID-19 crisis in Lagos, Nigeria: A qualitative study. Germs 2020, 10, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Østebø, T.; Tronvoll, K.; Marit Tolo, Ø. Religion and the ‘Secular Shadow’: Responses to COVID-19 in Ethiopia. Religion 2021, 51, 339–358. [Google Scholar] [CrossRef]
- Prajitha, K.C.; Rahul, A.; Chintha, S.; Soumya, G.; Maheswari Suresh, M.; Nalina Kumari Kesavan Nair, A.; Valamparampil, M.J.; Reghukumar, A.; Venkitaraman, S.; Anish, T.S.N. Strategies and challenges in Kerala’s response to the initial phase of COVID-19 pandemic: A qualitative descriptive study. BMJ Open 2021, 11, e051410. [Google Scholar] [CrossRef] [PubMed]
- Prasetyo, K.; Arif, L. Civil society participation in efforts to prevent the spread COVID-19. J. Adm. Publik: Public Adm. J. 2021, 11, 22–31. [Google Scholar] [CrossRef]
- Prasetyono, D.W.; Hidayat, E.; Marta, R.F.; Kurniawati, L.S.M.W.; Chinmi, M. Patron-client relationship between village heads and their residents during the COVID-19 pandemic. J. Sos. Dan. Pembang. 2020, 36, 501–510. [Google Scholar] [CrossRef]
- Samuelsen, H.; Toé, L.P. COVID-19 temporalities: Ruptures of everyday life in urban Burkina Faso. Med. Anthropol. Theory 2021, 8, 1–21. [Google Scholar] [CrossRef]
- Mirna Sari, N.P.; Romadhon Sukadi, B.D.N.; Yasintha, P.N. The effectiveness of Tri Hita Karana based traditional village management in COVID-19 prevention in Bali. J. Transform. 2021, 7, 56–80. [Google Scholar] [CrossRef]
- Sharma, G.D.; Ghura, A.S.; Mahendru, M.; Erkut, B.; Kaur, T.; Bedi, D. Panic during COVID-19 pandemic! A qualitative investigation into the psychosocial experiences of a sample of Indian people. Front. Psychol. 2020, 11, 575491. [Google Scholar] [CrossRef]
- Sukmawan, S. Tradition-responsive approach as non-medical treatment in mitigating the COVID-19 pandemic in Tengger, East Java, Indonesia. In Proceedings of the 1st International Seminar on Cultural Sciences, ISCS 2020; EAI: Malang, Indonesia, 2021. [Google Scholar]
- Sumesh, S.S.; Gogoi, N. Collecting the ‘Thick Descriptions’: A pandemic ethnography of the lived experiences of COVID-19 induced stigma and social discrimination in India. J. Loss Trauma 2021, 27, 1–14. [Google Scholar] [CrossRef]
- Tan, M.L.; Lasco, G. ‘Hawa’ and ‘resistensiya’: Local health knowledge and the COVID-19 pandemic in the Philippines. Anthropol. Med. 2021, 19, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Wibisono, M.Y.; Truna, D.S.; Rahman, M.T. Turning religion from cause to reducer of panic during the COVID-19 pandemic. HTS Teol. Stud./Theol. Stud. 2021, 77, 4. [Google Scholar] [CrossRef]
- Baer, H.A.; Ida Susser, M.S.H.A.B.; Singer, M.; Susser, I.; Susser, P.A.I. Medical Anthropology and the World System; Praeger: Westport, CT, USA, 2003. [Google Scholar]
- Herring, D.A.; Swedlund, A.C. Plagues and epidemics in anthropological perspective. In Plagues and Epidemics: Infected Spaces Past and Present; Herring, D.A., Swedlund, A.C., Eds.; Taylor & Francis Group: London, UK, 2010. [Google Scholar]
- Altiparmakis, A.; Bojar, A.; Brouard, S.; Foucault, M.; Kriesi, H.; Nadeau, R. Pandemic politics: Policy evaluations of government responses to COVID-19. West Eur. Politics 2021, 44, 1159–1179. [Google Scholar] [CrossRef]
- Hakim, M.S. SARS-CoV-2, COVID-19, and the debunking of conspiracy theories. Rev. Med. Virol. 2021, 31, e2222. [Google Scholar] [CrossRef] [PubMed]
- Douglas, K.M. COVID-19 conspiracy theories. Group Process. Intergroup Relat. 2021, 24, 270–275. [Google Scholar] [CrossRef]
- Sturm, T.; Albrecht, T. ‘Constituent Covid-19 apocalypses: Contagious conspiracism, 5G, and viral vaccinations’. Anthropol. Med. 2021, 28, 122–139. [Google Scholar] [CrossRef]
- Pummerer, L.; Böhm, R.; Lilleholt, L.; Winter, K.; Zettler, I.; Sassenberg, K. Conspiracy theories and their societal effects during the COVID-19 pandemic. Soc. Psychol. Personal. Sci. 2021. [Google Scholar] [CrossRef]
- Earnshaw, V.A.; Eaton, L.A.; Kalichman, S.C.; Brousseau, N.M.; Hill, E.C.; Fox, A.B. COVID-19 conspiracy beliefs, health behaviors, and policy support. Transl. Behav. Med. 2020, 10, 850–856. [Google Scholar] [CrossRef]
- Cuan-Baltazar, J.Y.; Muñoz-Perez, M.J.; Robledo-Vega, C.; Pérez-Zepeda, M.F.; Soto-Vega, E. Misinformation of COVID-19 on the Internet: Infodemiology study. JMIR Public Health Surveill. 2020, 6, e18444. [Google Scholar] [CrossRef]
- Larson, H.J. Blocking information on COVID-19 can fuel the spread of misinformation. Nature 2020, 580, 306. [Google Scholar] [CrossRef]
- Aghagoli, G.; Siff, E.J.; Tillman, A.C.; Feller, E.R. COVID-19: Misinformation can kill. Rhode Isl. Med. J. (2013) 2020, 103, 12–14. [Google Scholar]
- Dairaini, I. Data Transparency and Misinformation of COVID-19 in Indonesia. Politik Nasional. 2020. Available online: http://lipi.go.id/publikasi/data-transparency-and-misinformation-of-covid-19-in-indonesia/34527 (accessed on 15 November 2021).
- Tasnim, S.; Hossain, M.M.; Mazumder, H. Impact of Rumors and Misinformation on COVID-19 in Social Media. J. Prev. Med. Public Health 2020, 53, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Nasir, N.M.; Baequni, B.; Nurmansyah, M.I. Misinformation related to COVID-19 in Indonesia. J. Adm. Kesehat. Indones. 2020, 8, 51–59. [Google Scholar] [CrossRef]
- Malecki, K.; Keating, J.A.; Safdar, N. Crisis communication and public perception of COVID-19 risk in the era of social media. Clin. Infect. Dis. 2020, 72, 697–702. [Google Scholar] [CrossRef]
- Lunn, P.; Belton, C.; Lavin, C.; McGowan, F.; Timmons, S.; Robertson, D. Using Behavioural Science to Help Fight the Coronavirus; ESRI Working Paper No. 656 March 2020; Economic and Social Research Institute: Dublin, Ireland, 2020. [Google Scholar]
- Briggs, C.L. Beyond the linguistic/medical anthropology divide: Retooling anthropology to face COVID-19. Med. Anthropol. 2020, 39, 563–572. [Google Scholar] [CrossRef]
- Ramaci, T.; Barattucci, M.; Ledda, C.; Rapisarda, V. Social stigma during COVID-19 and its impact on HCWs outcomes. Sustainability 2020, 12, 3834. [Google Scholar] [CrossRef]
- Mahmud, A.; Islam, M.R. Social stigma as a barrier to COVID-19 responses to community well-being in Bangladesh. Int. J. Community Well-Being 2020, 4, 315–321. [Google Scholar] [CrossRef]
- Kleinman, A.; Lee, S. SARS and the problem of social stigma. In China, Prelude to Pandemic? Kleinman, A., Watson, J., Eds.; Stanford University Press: Stanford, CA, USA, 2006; pp. 173–195. [Google Scholar]
- Das, V. Stigma, contagion, defect: Issues in the anthropology of public health. In Proceedings of the Stigma and Global Health: Developing a Research Agenda, National Institutes of Health; National Institutes of Health: Bethesda, MD, USA, 2013. [Google Scholar]
- Barrett, R.; Brown, P.J. Stigma in the time of influenza: Social and institutional responses to pandemic emergencies. J. Infect. Dis. 2008, 197, S34–S37. [Google Scholar] [CrossRef]
- Yang, L.; Kleinman, A.; Link, B.; Phelan, J.; Lee, S.; Good, B. Culture and stigma: Adding moral experience to stigma theory. Soc. Sci. Med. (1982) 2007, 64, 1524–1535. [Google Scholar] [CrossRef] [PubMed]
- Keusch, G.T.; Wilentz, J.; Kleinman, A. Stigma and global health: Developing a research agenda. Lancet 2006, 367, 525–527. [Google Scholar] [CrossRef]
- Briggs, C.L. Communicability, racial discourse, and disease. Annu. Rev. Anthropol. 2005, 34, 269–291. [Google Scholar] [CrossRef]
- Flowers, P.; Davis, M.; Lohm, D.; Waller, E.; Stephenson, N. Understanding pandemic influenza behaviour: An exploratory biopsychosocial study. J. Health Psychol. 2016, 21, 759–769. [Google Scholar] [CrossRef] [PubMed]
- Quesada, J.; Hart, L.K.; Bourgois, P. Structural vulnerability and health: Latino migrant laborers in the United States. Med. Anthropol. 2011, 30, 339–362. [Google Scholar] [CrossRef] [PubMed]
- Morsy, S. The missing link in medical anthropology: The political economy of health. Rev. Anthropol. 1979, 6, 349–363. [Google Scholar] [CrossRef]
- Kentikelenis, A.; Rochford, C. Power asymmetries in global governance for health: A conceptual framework for analyzing the political-economic determinants of health inequities. Glob. Health 2019, 15 (Suppl. 1), 1–10. [Google Scholar] [CrossRef]
- Wilkinson, A.; Parker, M.; Martineau, F.; Leach, M. Engaging ‘communities’: Anthropological insights from the West African Ebola epidemic. Philos. Trans. R. Soc. B Biol. Sci. 2017, 372, 20160305. [Google Scholar] [CrossRef]
- Wald, P. Contagious: Cultures, Carriers, and the Outbreak Narrative; Duke University Press: Durham, NC, USA, 2008. [Google Scholar] [CrossRef]
- Singer, M.; Rylko-Bauer, B. The syndemics and structural violence of the COVID-19 pandemic: Anthropological insights on a crisis. Open Anthropol. Res. 2021, 1, 7–32. [Google Scholar] [CrossRef]
- Ali, I. From normal to viral body: Death rituals during ordinary and extraordinary Covidian times in Pakistan. Front. Sociol. 2021, 5, 133. [Google Scholar] [CrossRef]
- Madhi, S.A.; Gray, G.E.; Ismail, N.; Izu, A.; Mendelson, M.; Cassim, N.; Stevens, W.; Venter, F. COVID-19 lockdowns in low- and middle-income countries: Success against COVID-19 at the price of greater costs. South Afr. Med. J. 2020, 110, 724. [Google Scholar] [CrossRef]
- Hrynick, T.A.; Ripoll Lorenzo, S.; Carter, S.E. COVID-19 response: Mitigating negative impacts on other areas of health. BMJ Glob. Health 2021, 6, e004110. [Google Scholar] [CrossRef] [PubMed]
- TB PPM. One Year of COVID-19 and its Impact on Private Provider Engagement for TB; StobTB: Geneva, Switzerland, 2021. [Google Scholar]
- GFATM. The Impact of COVID-19 on HIV, TB and Malaria Services and Systems for Health: A Snapshot from 502 Health Facilities across Africa and Asia; Global Fund to Fight AIDS, Tuberculosis and Malaria: Geneva, Switzerland, 2021. [Google Scholar]
- Fronteira, I.; Sidat, M.; Magalhães, J.P.; De Barros, F.P.C.; Delgado, A.P.; Correia, T.; Daniel-Ribeiro, C.T.; Ferrinho, P. The SARS-CoV-2 pandemic: A syndemic perspective. One Health 2021, 12, 100228. [Google Scholar] [CrossRef] [PubMed]
- Antulov-Fantulin, N.; Biller-Andorno, N.; Böttcher, L.; Berezowski, J.; Burton-Jeangros, C.; Blanchet, K.; Clausin, M.; Escher, G.; Flahault, A.; Fukuda, K.; et al. Building societal resilience to COVID-19 and future pandemics: A synthesis of the literature and a governance framework for action. 2021. Pre-print. [Google Scholar] [CrossRef]
- Wenham, C. What went wrong in the global governance of covid-19? BMJ 2021, 372, 303. [Google Scholar] [CrossRef] [PubMed]
- Nederveen Pieterse, J.; Lim, H.; Khondker, H. Covid-19 and Governance: Crisis Reveals; Taylor & Francis Group: Abingdon, UK, 2021. [Google Scholar]
- Shrestha, N.; Mishra, S.R.; Ghimire, S.; Gyawali, B.; Marahatta, S.B.; Maskey, S.; Baral, S.; Shrestha, N.; Yadav, R.; Pokharel, S.; et al. Health system preparedness for COVID-19 and its impacts on frontline health-care workers in Nepal: A qualitative study among frontline health-care workers and policy-makers. Disaster Med. Public Health Prep. 2021, 204, 1–9. [Google Scholar] [CrossRef]
- Rajan, D.; Koch, K.; Rohrer, K.; Bajnoczki, C.; Socha, A.; Voss, M.; Nicod, M.; Ridde, V.; Koonin, J. Governance of the Covid-19 response: A call for more inclusive and transparent decision-making. BMJ Glob. Health 2020, 5, e002655. [Google Scholar] [CrossRef]
- Turner, V. Dramas, Fields, and Metaphors: Symbolic Action in Human Society; Cornell University Press: New York, NY, USA, 1974. [Google Scholar]
- Foster, G.M. Disease etiologies in non-western medical systems. Am. Anthropol. 1976, 78, 773–782. [Google Scholar] [CrossRef]
- Hasher, L.; Goldstein, D.; Toppino, T. Frequency and the conference of referential validity. J. Verbal Learn. Verbal Behav. 1977, 16, 107–112. [Google Scholar] [CrossRef]
- Link, B.G.; Phelan, J.C. Conceptualizing stigma. Annu. Rev. Sociol. 2001, 27, 363–385. [Google Scholar] [CrossRef]


| Topic | Inclusion Criteria (Met All) | Exclusion Criteria (Met Any) |
|---|---|---|
| Scope | Focus on COVID-19 impacts using social research methods Primary qualitative data collection from community or participatory settings Research conducted in LMICs | Studies conducted in non-LMICs Quantitative methodology Emphasis on virtual, digital, or distance data collection, such as phone or teleconferencing interviews or online surveys Methodologically low rigor |
| Type | Peer-reviewed journal articles publishing data from empirical studies | Grey literature, systematic reviews, published protocols, or commentaries |
| Language | English terms used for database search | Non-English articles |
| Timeline | Published after December 2019 through August 2021 | Data collected prior to December 2019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raymond, C.B.; Ward, P.R. Community-Level Experiences, Understandings, and Responses to COVID-19 in Low- and Middle-Income Countries: A Systematic Review of Qualitative and Ethnographic Studies. Int. J. Environ. Res. Public Health 2021, 18, 12063. https://doi.org/10.3390/ijerph182212063
Raymond CB, Ward PR. Community-Level Experiences, Understandings, and Responses to COVID-19 in Low- and Middle-Income Countries: A Systematic Review of Qualitative and Ethnographic Studies. International Journal of Environmental Research and Public Health. 2021; 18(22):12063. https://doi.org/10.3390/ijerph182212063
Chicago/Turabian StyleRaymond, Christopher B., and Paul R. Ward. 2021. "Community-Level Experiences, Understandings, and Responses to COVID-19 in Low- and Middle-Income Countries: A Systematic Review of Qualitative and Ethnographic Studies" International Journal of Environmental Research and Public Health 18, no. 22: 12063. https://doi.org/10.3390/ijerph182212063
APA StyleRaymond, C. B., & Ward, P. R. (2021). Community-Level Experiences, Understandings, and Responses to COVID-19 in Low- and Middle-Income Countries: A Systematic Review of Qualitative and Ethnographic Studies. International Journal of Environmental Research and Public Health, 18(22), 12063. https://doi.org/10.3390/ijerph182212063