
Maternal Perinatal Characteristics in Patients with Severe Preeclampsia: A Case-Control Nested Cohort Study

 ,
, 
 and
and 
Abstract
:1. Introduction
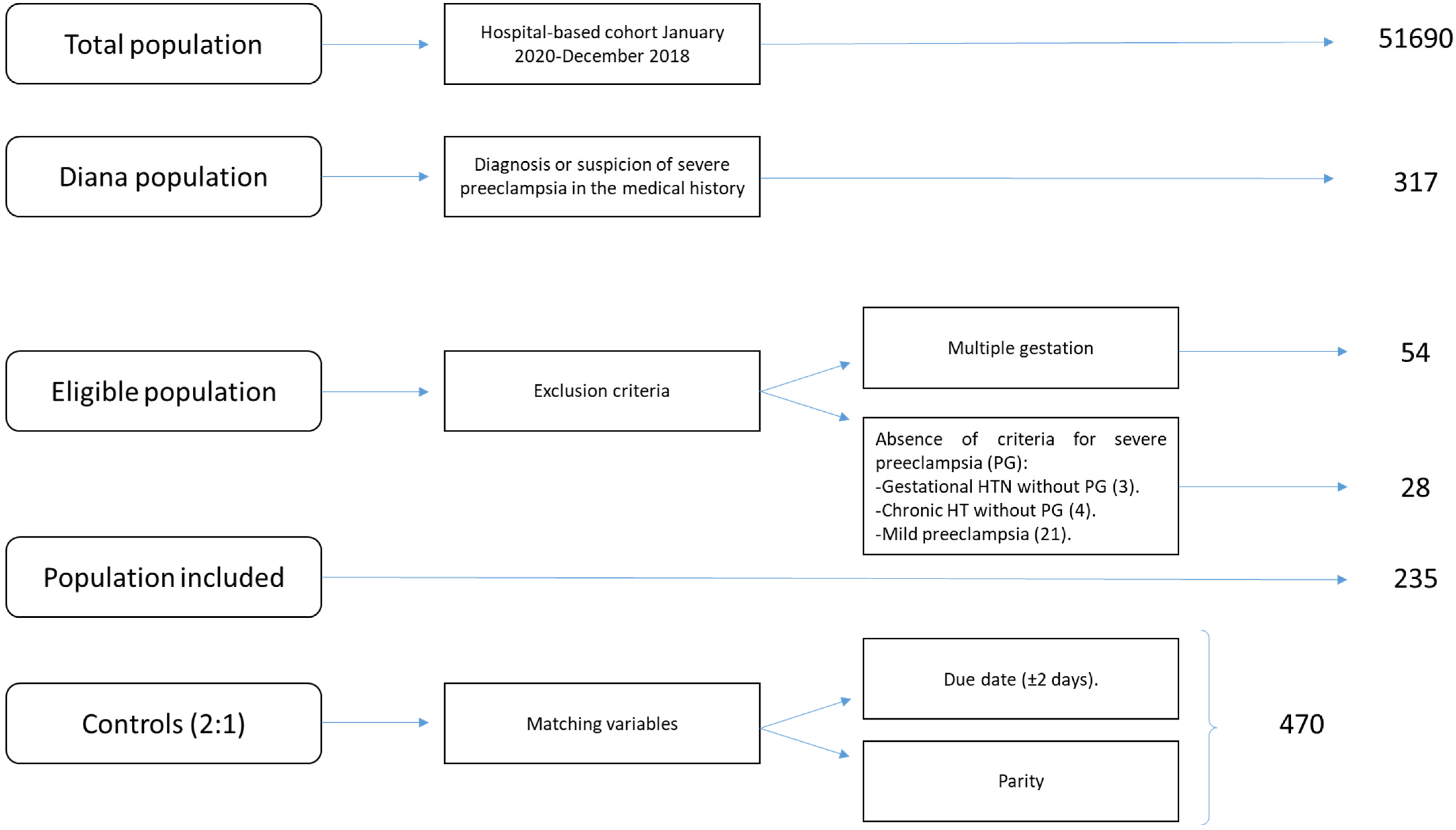
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins. Gestational Hypertension and Preeclampsia. Obstet. Gynecol. 2020, 135, e237–e253. [Google Scholar] [CrossRef]
- Payne, B.; Magee, L.A.; von Dadelszen, P. Assessment, surveillance and prognosis in pre-eclampsia. Best Pr. Res. Clin. Obs. Gynaecol. 2011, 25, 449. [Google Scholar] [CrossRef] [PubMed]
- Magee, L.A.; Pels, A.; Helewa, M.; Rey, E.; von Dadelszen, P.; Audibert, F.; Bujold, E.; Côté, A.-M.; Douglas, M.J.; Eastabrook, G.; et al. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy: Executive summary. J. Obs. Gynaecol. Can. 2014, 36, 416. [Google Scholar] [CrossRef]
- Abalos, E.; Cuesta, C.; Grosso, A.L.; Chou, D.; Say, L. Global and regional estimates of preeclampsia and eclampsia: A systematic review. Eur. J. Obs. Gynecol. Reprod. Biol. 2013, 170, 1. [Google Scholar] [CrossRef]
- Ananth, C.V.; Keyes, K.M.; Wapner, R.J. Pre-eclampsia rates in the United States, 1980–2010: Age-period-cohort analysis. BMJ 2013, 347, f6564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartch, E.; Medcalf, K.E.; Park, A.L.; Ray, J.G. Clinical Risk factors for preeclampsia determined in early pregnancy: Systematic review and meta-analysis of large cohort studies. BMJ. 2016, 353, i1753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology [STROBE] statement: Guidelines for reporting observational studies. Gac. Sanit. 2008, 22, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Sibai, B.M.; Taslimi, M.M.; El-Nazer, A.; Amon, E.; Mabie, B.C.; Ryan, G.M. Maternal-perinatal outcome associated with the syndrome of hemolysis, elevated liver enzymes, and low platelets in severe preeclampsia-eclampsia. Am. J. Obs. Gynecol. 1986, 155, 501–509. [Google Scholar] [CrossRef]
- Liu, C.M.; Cheng, P.J.; Chang, S.D. Maternal Complications and Perinatal Outcomes Associated with Gestational Hypertension and Severe Preeclampsia in Taiwanese Women. J. Med. Assoc. 2008, 107, 129–138. [Google Scholar] [CrossRef] [Green Version]
- Turgut, A.; Demirci, O.; Demirci, E.; Uludoğan, M. Comparison of maternal and neonatal outcomes in women with HELLP syndrome and women with severe preeclampsia without HELLP syndrome. J. Prenat. Med. 2010, 4, 51–58. [Google Scholar] [PubMed]
- Ngwenya, S.; Jones, B.; Mwembe, D. Determinants of adverse maternal and perinatal outcomes in severe preeclampsia and eclampsia in a low-resource setting, Mpilo Central Hospital, Bulawayo, Zimbabwe. BMC Res. Notes 2019, 12, 298. [Google Scholar] [CrossRef] [Green Version]
- Yücesoy, G.; Özkan, S.; Bodur, H.; Tan, T.; Çalışkan, E.; Vural, B.; Çorakçı, A. Maternal and perinatal outcome in pregnancies complicated with hypertensive disorder of pregnancy: A seven year experience of a tertiary care center. Arch. Gynecol. Obs. 2005, 273, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Jantasing, S.; Tanawattanacharoen, S. Perinatal Outcomes in Severe Preeclamptic Women between 24-33+6 Weeks’ Gestation. J. Med. Assoc. Thai. 2008, 91, 25–30. [Google Scholar] [PubMed]
- Li, X.; Zhang, W.; Lin, J.; Liu, H.; Yang, Z.; Teng, Y.; Duan, S.; Lin, X.; Xie, Y.; Li, Y.; et al. Risk factors for adverse maternal and perinatal outcomes in women with preeclampsia: Analysis of 1396 cases. J. Clin. Hypertens. 2018, 20, 1049–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kongwattanakul, K.; Saksiriwuttho, P.; Chaiyarach, S.; Thepsuthammarat, K. Incidence, characteristics, maternal complications, and perinatal outcomes associated with preeclampsia with severe features and HELLP síndrome. Int. J. Women’s Health 2018, 10, 371–377. [Google Scholar] [CrossRef] [Green Version]
- Kwiatkowski, S.; Dołegowska, B.; Kwiatkowska, E.; Rzepka, R.; Marczuk, N.; Loj, B.; Torbè, A. Maternal endothelial damage as a disorder shared by early preeclampsia, late preeclampsia and intrauterine growth restriction. J. Perinat. Med. 2017, 45, 793–802. [Google Scholar] [CrossRef]
- Chappell, L.C.; Brocklehurst, P.; Green, M.E.; Hunter, R.; Hardy, P.; Juszczak, E.; Linsell, L.; Chiocchia, V.; Greenland, M.; Placzek, A.; et al. Planned early delivery or expectant management for late preterm pre-eclampsia (PHOENIX): A randomised controlled trial. Lancet 2019, 394, 1181. [Google Scholar] [CrossRef] [Green Version]
- Magee, L.A.; Yong, P.J.; Espinosa, V.; Côté, A.M.; Chen, I.; Von Dadelszen, P. Expectant Management of Severe Preeclampsia Remote from Term: A Structured Systematic Review. Hypertens. Pregnancy 2009, 28, 312–347. [Google Scholar] [CrossRef]
- Haddad, B.; Sibai, B.M. Expectant management in pregnancies with severe pre-eclampsia. Semin. Perinatol. 2009, 33, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Guerrier, G.; Oluyide, B.; Keramarou, M.; Grais, R.F. Factors associated with severe preeclampsia and eclampsia in Jahun, Nigeria. Int. J. Womens Health 2013, 5, 509–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nankali, A.; Malek-Khosravi, S.H.; Zangeneh, M.; Rezaei, M.; Hemati, Z.; Kohzadi, M. Maternal Complications Associated with Severe Preeclampsia. J. Obstet. Gynecol. India 2013, 63, 112–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Overall | Cases (SP) | Controls | p Value | |
|---|---|---|---|---|
| N, % | 705 | 235 (33.3%) | 470 (66.7%) | |
| Maternal features: | ||||
| Maternal age at birth, mean ± SD | 33.62 ± 5.88 | 33.50 ± 6.32 | 33.69 ± 5.65 | 0.78 |
| Maternal age > 35 years, n, % | 334 (47.4%) | 164 (69.8%) | 170 (36.2%) | <0.001 |
| Maternal age > 40 years, n, % | 131 (18.6%) | 68 (28.9%) | 63 (13.4%) | <0.001 |
| Nuliparous, n, % | 341 (48.3%) | 112 (47.7%) | 229 (48.7%) | 0.67 |
| Delivery features: | ||||
| Elective C-Section, n, % | 113 (16%) | 95 (40.4%) | 18 (3.8%) | <0.001 |
| Global C-Section, n, % | 239 (33.9%) | 141 (60%) | 98 (20.9%) | <0.001 |
| Days of maternal admission, mean ± SD | 5.64 ± 4.7 | 9.73 ± 6.09 | 3.58± 1.39 | <0.001 |
| Maternal mortality, n, % | 0 | 0 | 0 | |
| Neonatal features: | ||||
| Gestational age at delivery (weeks), mean ± SD | 37.41 ± 3.36 | 34.77 ± 3.97 | 38.74 ± 1.95 | <0.001 |
| Prematurity, n, % | 179 (25.8%) | 137 (58.3%) | 45 (9.6%) | <0.001 |
| Male, n, % | 359 (50.9%) | 108 (46%) | 251 (53.4%) | 0.62 |
| Birth weight, mean ± SD | 2879 ± 833 | 2218± 905 | 3210± 552 | <0.001 |
| pH at birth, mean ± SD | 7.26 ± 0.08 | 7.23 ± 0.09 | 7.27 ± 0.08 | <0.001 |
| Unknown pH, mean ± SD | 37 (5.2%) | 20 (8.5%) | 17 (3.6%) | |
| Apgar at 1st minute, mean ± SD | 8.17 ± 1.72 | 7.18 ± 2.31 | 8.65 ± 1.13 | <0.001 |
| Apgar at 5 min, mean ± SD | 9.28 ± 1.52 | 8.55 ± 2.16 | 9.64 ± 0.88 | <0.001 |
| Apgar Unknown n, % | 4 (0.5%) | 3 (1.2%) | 0 (0%) | |
| Perinatal morbidity and mortality | ||||
| pH < 7 at birth, n, % | 14 (1.9%) | 12 (5.1%) | 2 (0.4%) | <0.001 |
| Apgar at 5 min < 7, n, % | 27 (3.8%) | 22 (9.4%) | 5 (1.1%) | <0.001 |
| Perinatal mortality, n, % | 15 (2.1%) | 14 (6%) | 1 (0.2%) | <0.001 |
| Intrauterine mortality, n, % | 10 (1.4%) | 9 (3.8%) | 1 (0.2%) | <0.001 |
| Overall n = 235 | |
|---|---|
| Maternal features | |
| Chronic hypertension, n,% | 43 (18.3%) |
| Previous preeclampsia, n,% | 24 (10.2%) |
| Diabetes Mellitus, n,% | 6 (2.6%) |
| Chronic hypothyroidism, n,% | 24 (10.2%) |
| Chronic kidney disease, n,% | 18 (7.7%) |
| Chronic renal failure (GFR < 60 mL/min/1.732), n,% | 3 (1.3%) |
| Antiphospholipid syndrome, n, % | 6 (2.6%) |
| BMI > 30 | 53 (22.6%) |
| Nationality, n,% | |
| European | 140 (59.6%) |
| African | 13 (5.5%) |
| Latin American | 78 (33.2%) |
| Other | 4 (1.7%) |
| IVF, n,% | 29 (12.3%) |
| Obstetric features: | |
| Gestational hypertension, n,% | 63 (26.8%) |
| Gestational hypothyroidism, n,% | 25 (10.6%) |
| Gestational diabetes, n,% | 20 (8.5%) |
| GA at diagnosis of severe preeclampsia (weeks), mean ± SD | 34.40 ± 4.46 |
| Form of presentation of severe preeclampsia, n,% | |
| Early onset (GA < 34 weeks) | 91 (38.7%) |
| Puerperal preeclampsia | 53 (22.6%) |
| Magnesium Sulfate, n,% | 158 (67.2%) |
| Lung maturation with corticosteroid therapy, n,% | 105 (44.7%) |
| PE Severity features | |
| Maximum systolic blood pressure (mmHg), mean ± SD | 180 ± 16 |
| Maximum diastolic blood pressure (mmHg), mean ± SD | 104 ± 12 |
| HELLP syndrome, n,% | 22 (9.4%) |
| Eclampsia, n,% | 9 (3.8%) |
| Acute lung edema, n,% | 3 (1.3%) |
| Acute renal failure (plasma creatinine > 1.1 mg/dL), n,% | 51 (21.7%) |
| Oliguria (<400 mL/day or <0.5 mL/kg / h), n,% | 17 (7.2%) |
| Hematoma of the liver, n,% | 2 (0.9%) |
| Abruptio placentae, n,% | 3 (1.3%) |
| Acute cerebrovascular accident, n,% | 3 (1.3%) |
| PRESS syndrome, n,% | 1 (0.2%) |
| Thrombocytopenia (<100,000 platelets), n,% | 34 (14.5%) |
| Need for transfusion of packed red blood cells, n,% | 21 (8.9%) |
| Neonatal Features | |
| Restricted intrauterine growth (CIR), n,% | 56 (23.8%) |
| Newborn admission to NICU, n,% | 67 (28.5%) |
| Postpartum features: | |
| HBP at discharge, n,% | 227 (96.6%) |
| Number of antihypertensive drugs at discharge, n,% | |
| No antihypertensive drug | 8 (3.4%) |
| 1 antihypertensive drug | 97 (41.3%) |
| 2 antihypertensive drugs | 109 (46.4%) |
| 3 or more antihypertensive drugs | 21 (8.9%) |
| Renal failure at discharge, n,% | 9 (3.8%) |
| Persistence of renal failure 12 weeks after delivery, n,% | 3/9 (33.3%) |
| Positive proteinuria at 12 weeks, n,% | 167 (71.1%) |
| Postpartum hemoglobin (g/dL, mean ± SD) | 10.76 ± 1.74 |
| Loss to follow-up after hospital discharge, n,% | 27 (11.5%) |
| Diagnosis | Discharge | p | At 12 Weeks | p | |
|---|---|---|---|---|---|
| Plasma creatinine (mg/dL), mean ± SD | 0.87 ± 0.55 | 0.67 ± 0.25 | * | 0.68 ± 0.19 | ǂ |
| 24 h urine creatinine clearance (ml/min), mean ± SD | 113.14 ± 41.96 | 117.37 ± 33.85 | 113.03 ± 31.44 | ® | |
| Proteinuria at diagnosis of PE (gr/day), mean ± SD | 2.82 ± 2.92 | 0.97 ± 1.057 | * | 0.14 ± 0.26 | ǂ |
| Uric acid at diagnosis of PE (mg/dL), mean ± SD | 7.24 ± 1.76 | 5.71± 1.45 | * | ||
| GPT (ALT) at diagnosis of PE (IU/L), mean ± SD | 61.96 ± 116.03 | 29.12 ± 24.22 | * | ||
| Platelets/µcL at diagnosis of PE, mean ± SD | 167,485 ± 72,230 | 287,536 ± 100,015 | * | ||
| Peripartum LDH (IU/L), mean ± SD | 344.97 ± 300.83 | 240.12 ± 64.61 | * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aracil Moreno, I.; Rodríguez-Benitez, P.; Ruiz-Minaya, M.; Bernal Claverol, M.; Ortega Abad, V.; Hernández Martin, C.; Pintado Recarte, P.; Yllana, F.; Oliver-Barrecheguren, C.; Álvarez-Mon, M.; et al. Maternal Perinatal Characteristics in Patients with Severe Preeclampsia: A Case-Control Nested Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 11783. https://doi.org/10.3390/ijerph182211783
Aracil Moreno I, Rodríguez-Benitez P, Ruiz-Minaya M, Bernal Claverol M, Ortega Abad V, Hernández Martin C, Pintado Recarte P, Yllana F, Oliver-Barrecheguren C, Álvarez-Mon M, et al. Maternal Perinatal Characteristics in Patients with Severe Preeclampsia: A Case-Control Nested Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(22):11783. https://doi.org/10.3390/ijerph182211783
Chicago/Turabian StyleAracil Moreno, Irene, Patrocinio Rodríguez-Benitez, Maria Ruiz-Minaya, Mireia Bernal Claverol, Virginia Ortega Abad, Concepción Hernández Martin, Pilar Pintado Recarte, Fátima Yllana, Cristina Oliver-Barrecheguren, Melchor Álvarez-Mon, and et al. 2021. "Maternal Perinatal Characteristics in Patients with Severe Preeclampsia: A Case-Control Nested Cohort Study" International Journal of Environmental Research and Public Health 18, no. 22: 11783. https://doi.org/10.3390/ijerph182211783
APA StyleAracil Moreno, I., Rodríguez-Benitez, P., Ruiz-Minaya, M., Bernal Claverol, M., Ortega Abad, V., Hernández Martin, C., Pintado Recarte, P., Yllana, F., Oliver-Barrecheguren, C., Álvarez-Mon, M., Ortega, M. A., & De Leon-Luis, J. A. (2021). Maternal Perinatal Characteristics in Patients with Severe Preeclampsia: A Case-Control Nested Cohort Study. International Journal of Environmental Research and Public Health, 18(22), 11783. https://doi.org/10.3390/ijerph182211783