
Nutrition, Physical Activity, and New Technology Programs on Obesity Prevention in Primary Education: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Screening
2.4. Data Extraction
2.5. Assessment of the Methodological Quality of the Studies
3. Results
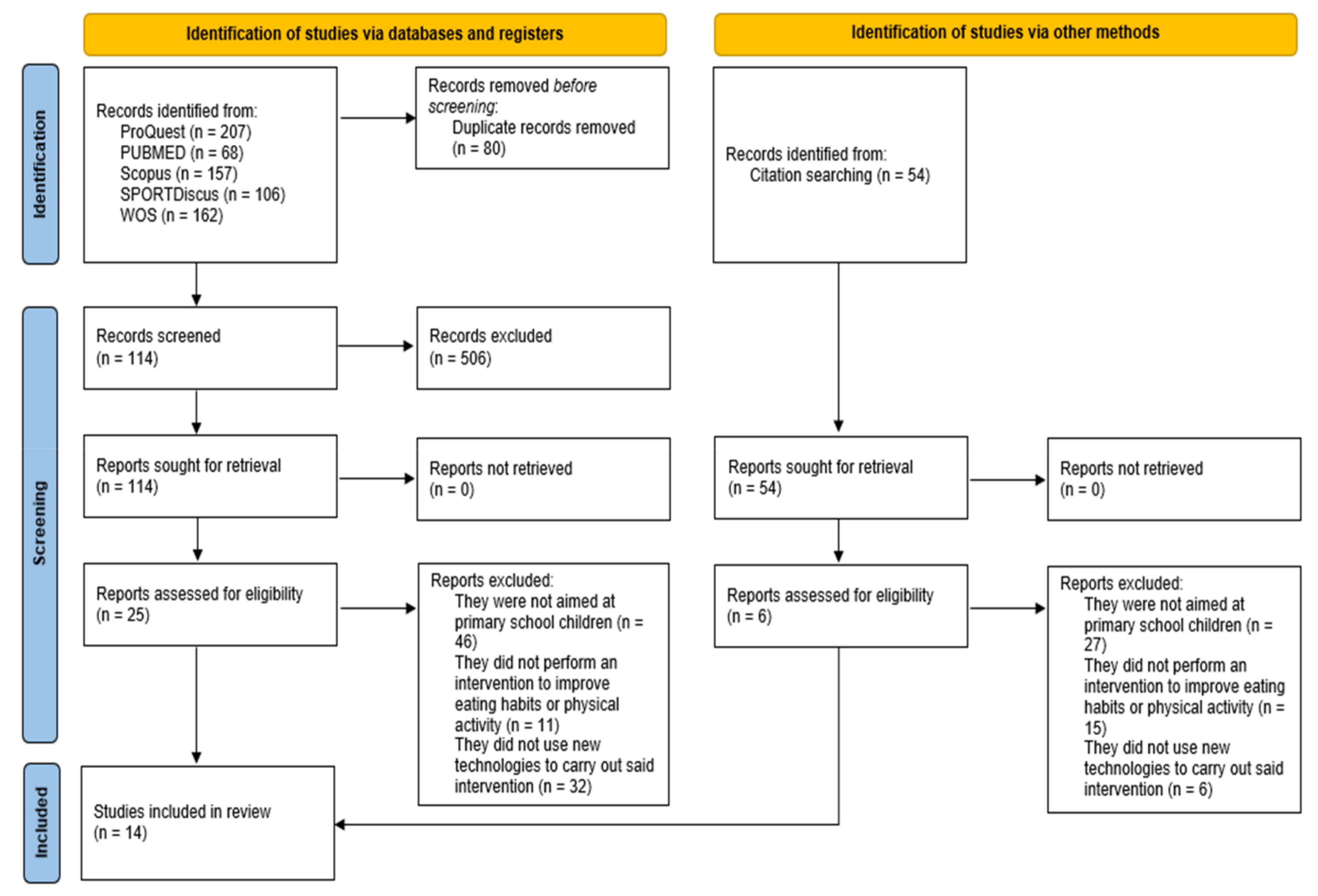
3.1. Database Searches
3.2. Description of Included Studies
3.3. Effects of Interventions on Nutrition
3.4. Effects of Interventions on Physical Activity
3.5. Effects of Interventions on Body Mass Index
3.6. Effects of the Use of New Technologies
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weihe, P.; Weihrauch-Blüher, S. Metabolic Syndrome in Children and Adolescents: Diagnostic Criteria, Therapeutic Options and Perspectives. Curr. Obes. Rep. 2019, 8, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R. Obesity in Children and Young People: A Crisis in Public Health. Obes. Rev. 2004, 5, 4–85. [Google Scholar] [CrossRef] [PubMed]
- Whitlock, E.P.; Williams, S.B.; Gold, R.; Smith, P.R.; Shipman, S.A. Screening and Interventions for Childhood Overweight: A Summary of Evidence for the US Preventive Services Task Force. Pediatrics 2005, 116, e125–e144. [Google Scholar] [CrossRef]
- Gurnani, M.; Birken, C.; Hamilton, J. Childhood Obesity: Causes, Consequences, and Management. Pediatr. Clin. N. Am. 2015, 62, 821–840. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.B.; Beets, M.W.; Brazendale, K.; Blair, S.N.; Pate, R.R.; Andersen, L.B.; Anderssen, S.A.; Grøntved, A.; Hallal, P.C.; Kordas, K.; et al. Associations of Vigorous-Intensity Physical Activity with Biomarkers in Youth. Med. Sci. Sports Exerc. 2017, 49, 1366–1374. [Google Scholar] [CrossRef]
- Aubert, S.; Barnes, J.D.; Abdeta, C.; Nader, P.A.; Adeniyi, A.F.; Aguilar-Farias, N.; Tenesaca, D.S.A.; Bhawra, J.; Brazo-Sayavera, J.; Cardon, G.; et al. Global Matrix 3.0 Physical Activity Report Card Grades for Children and Youth: Results and Analysis From 49 Countries. J. Phys. Act. Health 2018, 15, S251–S273. [Google Scholar] [CrossRef] [PubMed]
- Straatmann, V.S.; Almquist, Y.B.; Oliveira, A.J.; Veiga, G.V.; Rostila, M.; Lopes, C.S. Stability and Bidirectional Relationship between Physical Activity and Sedentary Behaviours in Brazilian Adolescents: Longitudinal Findings from a School Cohort Study. PLoS ONE 2019, 14, e0211470. [Google Scholar] [CrossRef]
- Wyszyńska, J.; Ring-Dimitriou, S.; Thivel, D.; Weghuber, D.; Hadjipanayis, A.; Grossman, Z.; Ross-Russell, R.; Dereń, K.; Mazur, A. Physical Activity in the Prevention of Childhood Obesity: The Position of the European Childhood Obesity Group and the European Academy of Pediatrics. Front. Pediatr. 2020, 8, 662. [Google Scholar] [CrossRef]
- Westerterp, K.R. Control of Energy Expenditure in Humans. Eur. J. Clin. Nutr. 2017, 71, 340–344. [Google Scholar] [CrossRef] [PubMed]
- Piirtola, M.; Kaprio, J.; Waller, K.; Heikkilä, K.; Koskenvuo, M.; Svedberg, P.; Silventoinen, K.; Kujala, U.M.; Ropponen, A. Leisure-Time Physical Inactivity and Association with Body Mass Index: A Finnish Twin Study with a 35-Year Follow-Up. Int. J. Epidemiol. 2017, 46, 116–127. [Google Scholar] [CrossRef]
- Whiting, S.; Buoncristiano, M.; Gelius, P.; Abu-Omar, K.; Pattison, M.; Hyska, J.; Duleva, V.; Musić Milanović, S.; Zamrazilová, H.; Hejgaard, T.; et al. Physical Activity, Screen Time, and Sleep Duration of Children Aged 6–9 Years in 25 Countries: An Analysis within the WHO European Childhood Obesity Surveillance Initiative (COSI) 2015–2017. Obes. Facts 2021, 14, 32–44. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Bruno, L.E. A Fundamental Approach for Treating Pediatric Dynapenia in Kids. ACSMs Health Fit. J. 2017, 21, 18–24. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. Physical Activity, Sedentary Time, and Obesity in an International Sample of Children. Med. Sci. Sports Exerc. 2015, 47, 2062–2069. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Barnes, J.D.; González, S.A.; Katzmarzyk, P.T.; Onywera, V.O.; Reilly, J.J.; Tomkinson, G.R. Global Matrix 2.0: Report Card Grades on the Physical Activity of Children and Youth Comparing 38 Countries. J. Phys. Act. Health 2016, 13, S343–S366. [Google Scholar] [CrossRef] [PubMed]
- Riddoch, C.J.; Bo Andersen, L.; Wedderkopp, N.; Harro, M.; Klasson-Heggebø, L.; Sardinha, L.B.; Cooper, A.R.; Ekelund, U. Physical Activity Levels and Patterns of 9- and 15-Yr-Old European Children. Med. Sci. Sports Exerc. 2004, 36, 86–92. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Mâsse, L.C.; Tilert, T.; Mcdowell, M. Physical Activity in the United States Measured by Accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Telama, R.; Yang, X.; Viikari, J.; Välimäki, I.; Wanne, O.; Raitakari, O. Physical Activity from Childhood to Adulthood: A 21-Year Tracking Study. Am. J. Prev. Med. 2005, 28, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Ronto, R.; Wu, J.H.; Singh, G.M. The Global Nutrition Transition: Trends, Disease Burdens and Policy Interventions. Public Health Nutr. 2018, 21, 2267–2270. [Google Scholar] [CrossRef]
- Cuadrado-Soto, E.; Peral-Suarez, Á.; Aparicio, A.; Perea, J.M.; Ortega, R.M.; López-Sobaler, A.M. Sources of Dietary Sodium in Food and Beverages Consumed by Spanish Schoolchildren between 7 and 11 Years Old by the Degree of Processing and the Nutritional Profile. Nutrients 2018, 10, 1880. [Google Scholar] [CrossRef]
- Filgueiras, A.R.; Pires de Almeida, V.B.; Koch Nogueira, P.C.; Alvares Domene, S.M.; Eduardo da Silva, C.; Sesso, R.; Sawaya, A.L. Exploring the Consumption of Ultra-Processed Foods and Its Association with Food Addiction in Overweight Children. Appetite 2019, 135, 137–145. [Google Scholar] [CrossRef]
- Maalouf, J.; Cogswell, M.E.; Bates, M.; Yuan, K.; Scanlon, K.S.; Pehrsson, P.; Gunn, J.P.; Merritt, R.K. Sodium, Sugar, and Fat Content of Complementary Infant and Toddler Foods Sold in the United States, 2015. Am. J. Clin. Nutr. 2017, 105, 1443–1452. [Google Scholar] [CrossRef]
- Alonso, F.J.; Carranza, M.D.; Rueda, J.D.; Naranjo, J. Composición Corporal En Escolares de Primaria y Su Relación Con El Hábito Nutricional y La Práctica Reglada de Actividad Deportiva. Rev. Andal. Med. Deporte 2014, 7, 137–142. [Google Scholar] [CrossRef][Green Version]
- Hardy, L.L.; Bell, J.; Bauman, A.; Mihrshahi, S. Association between Adolescents’ Consumption of Total and Different Types of Sugar-Sweetened Beverages with Oral Health Impacts and Weight Status. Aust. N. Z. J. Public Health 2018, 42, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of Ultra-Processed Foods and Health Status: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2021, 125, 308. [Google Scholar] [CrossRef]
- Nishtar, S.; Gluckman, P.; Armstrong, T. Ending Childhood Obesity: A Time for Action. Lancet 2016, 387, 825–827. [Google Scholar] [CrossRef]
- Gasser, C.E.; Mensah, F.K.; Russell, M.; Dunn, S.E.; Wake, M. Confectionery Consumption and Overweight, Obesity, and Related Outcomes in Children and Adolescents: A Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2016, 103, 1344–1356. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, C.E.; Iii, V.L.F.; Nicklas, T.A. Association of Candy Consumption with Body Weight Measures, Other Health Risk Factors for Cardiovascular Disease, and Diet Quality in US Children and Adolescents: NHANES 1999–2004. Food Nutr. Res. 2011, 55, 5794. [Google Scholar] [CrossRef]
- Pourshahidi, L.K.; Kerr, M.A.; McCaffrey, T.A.; Livingstone, M.B.E. Influencing and Modifying Children’s Energy Intake: The Role of Portion Size and Energy Density. Proc. Nutr. Soc. 2014, 73, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.B.; Arnberg, K.; Trolle, E.; Michaelsen, K.F.; Bro, R.; Pipper, C.B.; Mølgaard, C. The Effects of Water and Dairy Drinks on Dietary Patterns in Overweight Adolescents. Int. J. Food Sci. Nutr. 2016, 67, 314–324. [Google Scholar] [CrossRef]
- Tak, N.I.; Velde, S.J.T.; Singh, A.S.; Brug, J. The Effects of a Fruit and Vegetable Promotion Intervention on Unhealthy Snacks during Mid-Morning School Breaks: Results of the Dutch Schoolgruiten Project. J. Hum. Nutr. Diet. 2010, 23, 609–615. [Google Scholar] [CrossRef]
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Penalvo, J.L.; Mozaffarian, D. Effectiveness of School Food Environment Policies on Children’s Dietary Behaviors: A Systematic Review and Meta-Analysis. PLoS ONE 2018, 13, e0194555. [Google Scholar] [CrossRef]
- Davies, A.; Shi, Y.; Bauman, A.; Allman-Farinelli, M. Validity of New Technologies That Measure Bone-Related Dietary and Physical Activity Risk Factors in Adolescents and Young Adults: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 5688. [Google Scholar] [CrossRef]
- Cugelman, B.; Thelwall, M.; Dawes, P. Online Interventions for Social Marketing Health Behavior Change Campaigns: A Meta-Analysis of Psychological Architectures and Adherence Factors. J. Med. Internet Res. 2011, 13, e1367. [Google Scholar] [CrossRef]
- Durant, N.H. Not Just Fun and Games: Harnessing Technology to Address Childhood Obesity. Child. Obes. 2010, 6, 283–284. [Google Scholar] [CrossRef]
- Fox, S.; Duggan, M. Mobile Health 2012; Pew Research Center: Internet, Science & Tech: Washington, DC, USA, 2012. [Google Scholar]
- Turner-McGrievy, G.M.; Hales, S.B.; Schoffman, D.E.; Valafar, H.; Brazendale, K.; Weaver, R.G.; Beets, M.W.; Wirth, M.D.; Shivappa, N.; Mandes, T.; et al. Choosing between Responsive-Design Websites versus Mobile Apps for Your Mobile Behavioral Intervention: Presenting Four Case Studies. Transl. Behav. Med. 2017, 7, 224–232. [Google Scholar] [CrossRef]
- Wantland, D.J.; Portillo, C.J.; Holzemer, W.L.; Slaughter, R.; McGhee, E.M. The Effectiveness of Web-Based vs. Non-Web-Based Interventions: A Meta-Analysis of Behavioral Change Outcomes. J. Med. Internet Res. 2004, 6, e116. [Google Scholar] [CrossRef] [PubMed]
- Lu, A.S.; Kharrazi, H.; Gharghabi, F.; Thompson, D. A Systematic Review of Health Videogames on Childhood Obesity Prevention and Intervention. Games Health J. 2013, 2, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Araújo, A.C.D.; Knijnik, J.; Ovens, A.P. How Does Physical Education and Health Respond to the Growing Influence in Media and Digital Technologies? An Analysis of Curriculum in Brazil, Australia and New Zealand. J. Curric. Stud. 2021, 53, 563–577. [Google Scholar] [CrossRef]
- Kelishadi, R.; Heidari-Beni, M. Prevention and Control of Childhood Obesity: The Backbone in Prevention of Non Communicable Disease. Adv. Exp. Med. Biol. 2019, 1121, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Yi, D.Y.; Kim, S.C.; Lee, J.H.; Lee, E.H.; Kim, J.Y.; Kim, Y.J.; Kang, K.S.; Hong, J.; Shim, J.O.; Lee, Y.; et al. Clinical Practice Guideline for the Diagnosis and Treatment of Pediatric Obesity: Recommendations from the Committee on Pediatric Obesity of the Korean Society of Pediatric Gastroenterology Hepatology and Nutrition. Korean J. Pediatr. 2019, 62, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Shamah Levy, T.; Morales Ruán, C.; Amaya Castellanos, C.; Salazar Coronel, A.; Jiménez Aguilar, A.; Méndez Gómez Humarán, I. Effectiveness of a Diet and Physical Activity Promotion Strategy on the Prevention of Obesity in Mexican School Children. BMC Public Health 2012, 12, 152. [Google Scholar] [CrossRef]
- Williamson, D.A.; Champagne, C.M.; Harsha, D.; Han, H.; Martin, C.K.; Newton, R.L.; Sothern, M.; Stewart, T.M.; Webber, L.S.; Ryan, D. Effect of an Environmental School-Based Obesity Prevention Program on Changes in Body Fat and Body Weight: A Randomized Trial. Obesity 2012, 20, 1653–1661. [Google Scholar] [CrossRef]
- Grydeland, M.; Bergh, I.H.; Bjelland, M.; Lien, N.; Andersen, L.F.; Ommundsen, Y.; Klepp, K.-I.; Anderssen, S.A. Intervention Effects on Physical Activity: The HEIA Study—A Cluster Randomized Controlled Trial. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.M.; Meyer, A.; Kay, C.; Allensworth, D.; Gazmararian, J.A. A Holistic School-Based Intervention for Improving Health-Related Knowledge, Body Composition, and Fitness in Elementary School Students: An Evaluation of the HealthMPowers Program. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 78. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, D.B.; Ali, K.; Silva, C.; Gonçalves, S.; Machado, P.P.P. Use of Text Messaging Services to Promote Health Behaviors in Children. J. Nutr. Educ. Behav. 2015, 47, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.; Fassnacht, D.B.; Ali, K.; Gonçalves, S.; Conceição, E.; Vaz, A.; Crosby, R.D.; Machado, P.P.P. Promoting Health Behaviour in Portuguese Children via Short Message Service: The Efficacy of a Text-Messaging Programme. J. Health Psychol. 2015, 20, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Grutzmacher, S.K.; Duru, E.B.; Speirs, K.E.; Worthington, L.; Munger, A.L.; Lachenmayr, L.A. Using Text Messages to Engage Low-Income Parents in School-Based Nutrition Education. J. Hunger Environ. Nutr. 2018, 13, 335–339. [Google Scholar] [CrossRef]
- Min, J.; Tan, Z.; Abadie, L.; Townsend, S.; Xue, H.; Wang, Y. An Evaluation of the Effectiveness of the National Aeronautics and Space Administration Mission-X Child Health Promotion Program in the United States. Am. J. Health Promot. 2018, 32, 1333–1339. [Google Scholar] [CrossRef]
- Bartelink, N.H.M.; van Assema, P.; Kremers, S.P.J.; Savelberg, H.H.C.M.; Oosterhoff, M.; Willeboordse, M.; van Schayck, O.C.P.; Winkens, B.; Jansen, M.W.J. Can the Healthy Primary School of the Future Offer Perspective in the Ongoing Obesity Epidemic in Young Children? A Dutch Quasi-Experimental Study. BMJ Open 2019, 9, e030676. [Google Scholar] [CrossRef]
- Wadolowska, L.; Hamulka, J.; Kowalkowska, J.; Ulewicz, N.; Hoffmann, M.; Gornicka, M.; Bronkowska, M.; Leszczynska, T.; Glibowski, P.; Korzeniowska-Ginter, R. Changes in Sedentary and Active Lifestyle, Diet Quality and Body Composition Nine Months after an Education Program in Polish Students Aged 11−12 Years: Report from the ABC of Healthy Eating Study. Nutrients 2019, 11, 331. [Google Scholar] [CrossRef]
- Espinosa-Curiel, I.E.; Pozas-Bogarin, E.E.; Lozano-Salas, J.L.; Martínez-Miranda, J.; Delgado-Pérez, E.E.; Estrada-Zamarron, L.S. Nutritional Education and Promotion of Healthy Eating Behaviors Among Mexican Children Through Video Games: Design and Pilot Test of FoodRateMaster. JMIR Serious Games 2020, 8, e16431. [Google Scholar] [CrossRef]
- Mack, I.; Reiband, N.; Etges, C.; Eichhorn, S.; Schaeffeler, N.; Zurstiege, G.; Gawrilow, C.; Weimer, K.; Peeraully, R.; Teufel, M.; et al. The Kids Obesity Prevention Program: Cluster Randomized Controlled Trial to Evaluate a Serious Game for the Prevention and Treatment of Childhood Obesity. J. Med. Internet Res. 2020, 22, e15725. [Google Scholar] [CrossRef]
- Xu, H.; Ecker, O.; Zhang, Q.; Du, S.; Liu, A.; Li, Y.; Hu, X.; Li, T.; Guo, H.; Li, Y.; et al. The Effect of Comprehensive Intervention for Childhood Obesity on Dietary Diversity among Younger Children: Evidence from a School-Based Randomized Controlled Trial in China. PLoS ONE 2020, 15, e0235951. [Google Scholar] [CrossRef]
- Sánchez-Martínez, F.; Brugueras, S.; Serral, G.; Valmayor, S.; Juarez, O.; Jose Lopez, M.; Ariza, C. Three-Year Follow-Up of the POIBA Intervention on Childhood Obesity: A Quasi-Experimental Study. Nutrients 2021, 13, 453. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Ramírez, S.; Mundo-Rosas, V.; Jiménez-Aguilar, A.; Shamah-Levy, T. Methodology for the Analysis of Dietary Data from the Mexican National Health and Nutrition Survey 2006. Salud Publica Mex. 2009, 51 (Suppl. 4), S523–S529. [Google Scholar] [CrossRef] [PubMed]
- Hernández, B.; Gortmaker, S.L.; Laird, N.M.; Colditz, G.A.; Parra-Cabrera, S.; Peterson, K.E. Validity and reproducibility of a questionnaire on physical activity and non-activity for school children in Mexico City. Salud Publica Mex. 2000, 42, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Parcel, G.S.; Edmundson, E.; Perry, C.L.; Feldman, H.A.; O’Hara-Tompkins, N.; Nader, P.R.; Johnson, C.C.; Stone, E.J. Measurement of Self-Efficacy for Diet-Related Behaviors among Elementary School Children. J. Sch. Health 1995, 65, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Carskadon, M.A.; Acebo, C. A Self-Administered Rating Scale for Pubertal Development. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 1993, 14, 190–195. [Google Scholar] [CrossRef]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The Multistage 20 Metre Shuttle Run Test for Aerobic Fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef]
- Golan, M.; Weizman, A. Reliability and Validity of the Family Eating and Activity Habits Questionnaire. Eur. J. Clin. Nutr. 1998, 52, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Manz, K.; Schlack, R.; Poethko-Müller, C.; Mensink, G.; Finger, J.; Lampert, T.; KiGGS Study Group. Physical activity and electronic media use in children and adolescents: Results of the KiGGS study: First follow-up (KiGGS wave 1). Bundesgesundheitsblatt Gesundh. Gesundh. 2014, 57, 840–848. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Sample | Design | Length | Intervention | Variables | Instruments | ICT |
|---|---|---|---|---|---|---|---|
| Shamah-Levy et al. (2012) [43] | 1020 (♀ 50.7%, ♂ 49.3%) (10–11 years old) | Blind cluster-randomized field trial | 3 weeks (6 months follow-up) | Students: Nutrition and PA workshops, creation of puppet theatre, activation sessions and active participation games at playtime breaks. Teachers: Workshops to raise awareness about healthy eating and PA. Families: Calendars with healthy school breakfast recipes. School: Training of workers to recommend vegetables, fruit and water, delivery of water bottles, banners and public address announcements to promote the consumption of fruits, vegetables, water and PA. | BMI; Food intake; PA KDPA; PAS; HES | ES + S; FFQ; PAQ; MCQ; DCQ | Video |
| Williamson et al. (2012) [44] | 2060 (♀ 58.5%, ♂ 41.5%) (9–12 years old) | Longitudinal, cluster randomized 3-arm controlled | 28 months | Primary Prevention (PP): Environmental modification programme to promote healthy diet, PA and prevention programme for families. Primary + Secondary Prevention (PP + SP): Primary prevention + Classroom curriculum + counselling and education on the Internet. | Body fat; BMIz; FI; PA SST | IS + S; Digital video camera; SAPAC; DSS | Website |
| Grydeland et al. (2013) [45] | 700 (♀ 57%, ♂ 43%) (11 years old) | Cluster randomized controlled trial | 20 months | Students: Lessons on nutrition, consumption of fruits and vegetables, active breaks in the classroom, active transport campaigns, pedometers and computer-tailored individual advice. Families: Information sheets about nutrition and PA. School: Teacher training in the SPARK Physical Education teacher-training program. | BMI; A | ES + S; PCS; ActiGraph; 7164/GT1 | Computer tailored programme |
| Burke et al. (2014) [46] | 40 schools (8–11 years old) | Pretest-post-test | 3 years | The programme is integrated into the curriculum to improve health, PA and nutrition-education knowledge and behaviours. In addition, there are classroom exercises with the DVD, assemblies, classroom lessons, and family-based reinforcement activities. | HKB; BMI; Cardiovascular fitness; SSLP | Ad-hoc Questionnaire ES + S; PACER CITT | Video |
| Fassnacht et al. (2015) [47] | 49 (♀ 53%, ♂ 47%) (8–10 years old) | Pretest-post-test | 8 weeks. | All children participated in 2 educational group sessions that focused on health behaviours. The monitoring group also reported daily behaviours using SMS and received supportive feedback. | BMIz; Health behaviour; Daily fruit & vegetable intake; PA | ES + S; Questionnaire; Pedometer | SMS |
| Silva et al. (2015) [48] | 139 (♀ 47.5%, ♂ 52.5%) (8–10 years old) | Pretest-post-test | 8 weeks (4 weeks follow-up) | Two educational sessions of nutrition, PA, and screen-time and monitoring of the experimental group by SMS. | FVI; PA + CT; Daily steps; BMI; SP | FFQ; FEAHQ; Pedometer Plus;ES + S; SSQ | SMS |
| Grutzmacher et al. (2018) [49] | 23 schools | Pretest-post-test | 4 years | Text2BHealthy schools and control schools received standard classroom-based nutrition education from FSNE educators and classroom teachers trained by FSNE educators. Parents from Text2BHealthy schools receive 2 text messages each week during the school year and 2–3 messages each month during the summer. | FPB; HNE; DC; CBRE; PAB; ST | Ad-hoc Survey | SMS |
| Jungwon Min et al. (2018) [50] | 409 (♀ 52.3%, ♂ 47.7%) (6–13 years old) | Pretest-post-test | 6 weeks | Activity from website was completed in about 30 to 50 min per class time. The participants could repeat the activities with the teacher 2 or more times within a week. | Obesity-related behaviours; Health knowledge | Questionnaire | Website |
| Bartelink et al. (2019) [51] | 1676 (♀ 52.6%, ♂ 47.4%) (4–12 years old) | Longitudinal quasi-experimental | 2 years | Partial HPSF (PA): E-health programme for parents, structured PA sessions after lunch. Full HPSF (PA + Nutrition): Partial HPSF + Improved their health policy, provided water bottles and provided an educational lunch once a week. | BMIz; Socioeconomic status; Children’s; PA; behaviours Children’s dietary behaviours Children’s lunch intake | ES + S; Parent questionnaire; Accelerometer; Child questionnaire; Child lunch questionnaire | E-health program |
| Wadolowska et al. (2019) [52] | 646 (♀ 53.4%, ♂ 46.6%) (11–12 years old) | Pretest-posttest | 3 weeks (9 months follow-up) | The programme consisted of 5 topics, each topic included various forms of education from fun to “scientific” cognition. Each topic lasted approx. 180 min (4 h of school lessons) and was run by a minimum of 3–4 researchers. | Diet, sedentary and active lifestyle; Nutrition knowledge Sociodemographic characteristic | Short Form of the Food; Frequency; Questionnaire for Polish Children | Website |
| Espinosa-Curiel et al. (2020) [53] | 60 (♀ 47%, ♂ 53%) (8–10 years old) | Pretest-post-test | 6 weeks | 12 sessions of at least 25 min of play. | Food knowledge Dietary intake Parent perception | FKQ; FFQa; PPQ | Serious video game |
| Mack et al. (2020) [54] | 82 (♀ 48%, ♂ 52%) (9–12 years old) | Cluster randomized controlled trial | 2 weeks (4 weeks follow-up) | Intervention group: played the game (45 min) twice over a 2-week period, with a different selection of game modules played at each of the two sessions. Control group: Received basic information about a healthy lifestyle via a brochure. | Maintenance of knowledge Acceptance of the game; Emotions during game play Changes in dietary behaviour; PA; Media consumption | Knowledge questionnaire Questionnaire Self-assessment manikin Ernährungsmusterindex; KIGGS | Serious video game |
| Xu et al. (2020) [55] | 4846 (7–13 years old) | Randomized controlled trial | 12 months | Nutrition-education intervention (NE): Food notebook, courses for students (6), parents (2) and teachers (4), poster and class meetings. PA intervention (PA): Course for parents, 20 min of “Happy 10” per day and class meetings. Mixed group (CNP): All of the above. | BMI; DC; DDS9; DDS28; FVS | ES + S; Parent questionnaire; 24hDR | Video |
| Sánchez-Martínez et al. (2021) [56] | 4139 (8–9 years old) | Pretest-posttest | 9 lessons of 55 min. Reinforcement: 2 lessons of 50 min. and 1 of 60 min. (1 and 3 years follow-up) | Individual: Class on nutrition and registration of PA in 1 month. Family: Workshops to improve food and PA on weekends and attendance at more than 4 events at weekends. School: Review of the school menu, improvement in the availability of healthy food in the cafeteria and promotion of the opening of spaces. | BMI; TST; Physical fitness | P-HDWE; P-HDWM; Eurofit battery | Digital platform “Edu Natura” |
| Study | Results | Conclusion | |||
|---|---|---|---|---|---|
| N | PA | BMI | ICT | ||
| Shamah-Levy et al. (2012) [38] |  |  |  |  | The intervention strategy is effective in maintaining the BMI of schoolchildren. |
| Williamson et al. (2012) [39] |  |  |  |  | This school-based environmental-modification programme had modest beneficial effects on changes in percentage of body fat. Addition of a classroom/internet programme to the environmental programme did not enhance weight/fat-gain prevention, but did enhance physical activity and social support in overweight children. |
| Grydeland et al. (2013) [40] |  |  |  |  | An implementation of the HEIA intervention components in the school system may have a beneficial effect on public health by increasing overall physical activity among adolescents and possibly among girls and low-active adolescents in particular. |
| Burke et al. (2014) [41] |  |  |  |  | The HealthMPowers programme is effective in producing positive change in school policies and practices, student knowledge and behaviours, and student fitness and BMI, supporting the use of holistic interventions to address childhood obesity. |
| Fassnacht et al. (2015) [42] |  |  |  |  | The current SMS intervention was a useful tool to monitor and promote improved health behaviours in children. |
| Silva et al. (2015) [43] |  |  |  |  | The present findings suggest that the SMS-based monitoring and feedback systems have the potential for promoting better health behaviours in children. |
| Grutzmacher et al. (2018) [44] |  |  |  |  | Text2BHealthy resulted in improvements in a number of fruit and vegetable -consumption practices of parents and their children. |
| Jungwon Min et al. (2018) [45] |  |  |  |  | NASA MX programme was shown to improve children’s health knowledge and PA in the United States. |
| Bartelink et al. (2019) [46] |  |  |  |  | Full HPSF is effective in promoting positive health behaviours in children at T1 and T2 compared with control schools. Focusing on both nutrition and PA components seems to be more effective in promoting healthy behaviours than focusing exclusively on PA. |
| Wadolowska et al. (2019) [47] |  |  |  |  | In conclusion, diet-related and lifestyle-related school-based education from an almost one-year perspective can reduce central adiposity in pre-teenagers, despite a decrease in physical activity and the tendency to increase screen time. |
| Espinosa-Curiel et al. (2020) [48] |  |  |  |  | Health games such as FoodRateMaster are viable tools to help young children increase their food knowledge and improve dietary behaviours. |
| Mack et al. (2020) [49] |  |  |  |  | The Kids Obesity Prevention programme sustainably increased knowledge in the areas of nutrition and coping with stress, and children were able to apply the dietary energy density principle (DED-P). |
| Xu et al. (2020) [50] |  |  |  |  | Though the comprehensive obesity intervention did not improve the overall dietary diversity per day, positive intervention effects were observed in the consumption of breakfast and some other foods. |
| Sánchez-Martínez et al. (2021) [51] |  |  |  |  | School-based interventions are a good strategy to tackle the global rise in childhood obesity. Multilevel and multicomponent school-based interventions, including a family component, could improve children’s health habits, especially those regarding food and nutrition, and the taking part in physical activity. They could also be helpful in preventing the appearance of new cases of childhood obesity, though they may not have an immediate effect on adiposity outcomes. |
 ), non-significant difference (
), non-significant difference (  ), Not measured for outcomes (
), Not measured for outcomes (  ).
).Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navidad, L.; Padial-Ruz, R.; González, M.C. Nutrition, Physical Activity, and New Technology Programs on Obesity Prevention in Primary Education: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 10187. https://doi.org/10.3390/ijerph181910187
Navidad L, Padial-Ruz R, González MC. Nutrition, Physical Activity, and New Technology Programs on Obesity Prevention in Primary Education: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(19):10187. https://doi.org/10.3390/ijerph181910187
Chicago/Turabian StyleNavidad, Lorenzo, Rosario Padial-Ruz, and Mar Cepero González. 2021. "Nutrition, Physical Activity, and New Technology Programs on Obesity Prevention in Primary Education: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 19: 10187. https://doi.org/10.3390/ijerph181910187
APA StyleNavidad, L., Padial-Ruz, R., & González, M. C. (2021). Nutrition, Physical Activity, and New Technology Programs on Obesity Prevention in Primary Education: A Systematic Review. International Journal of Environmental Research and Public Health, 18(19), 10187. https://doi.org/10.3390/ijerph181910187