
The Containment Scouts: First Insights into an Initiative to Increase the Public Health Workforce for Contact Tracing during the COVID-19 Pandemic in Germany


Abstract
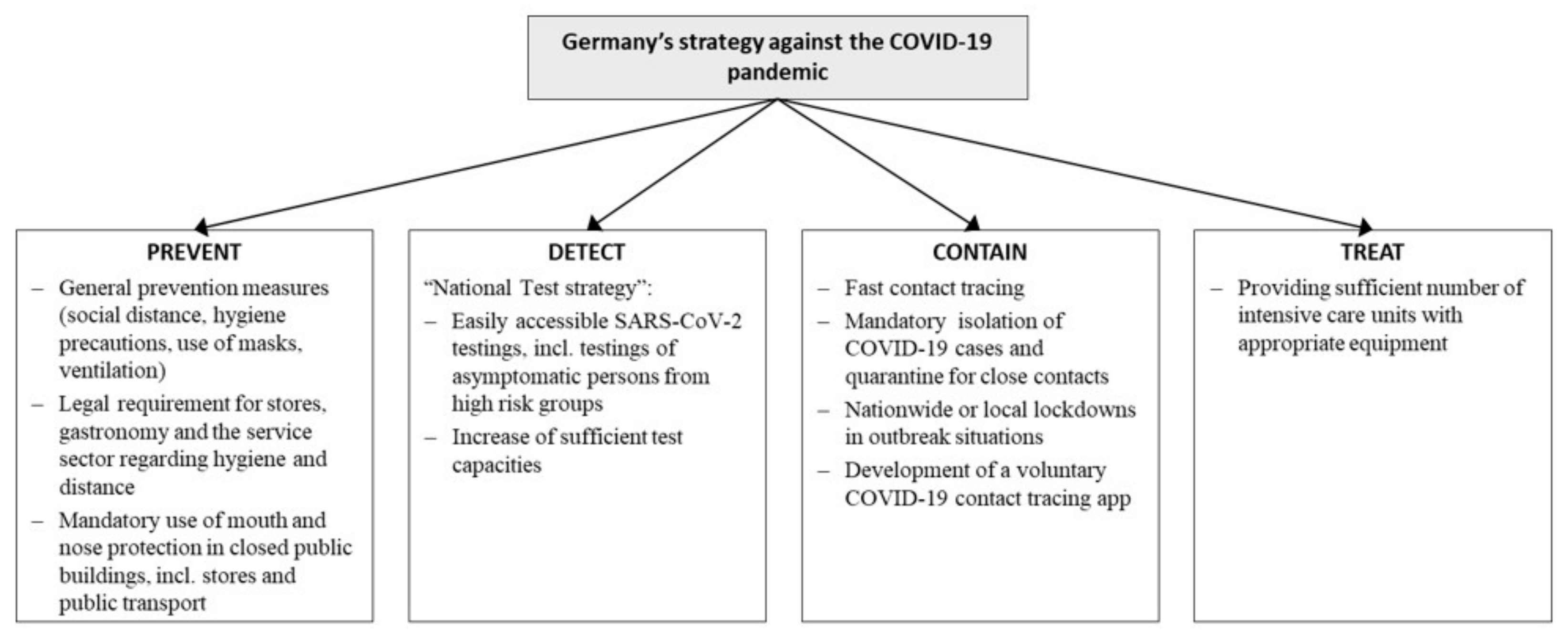
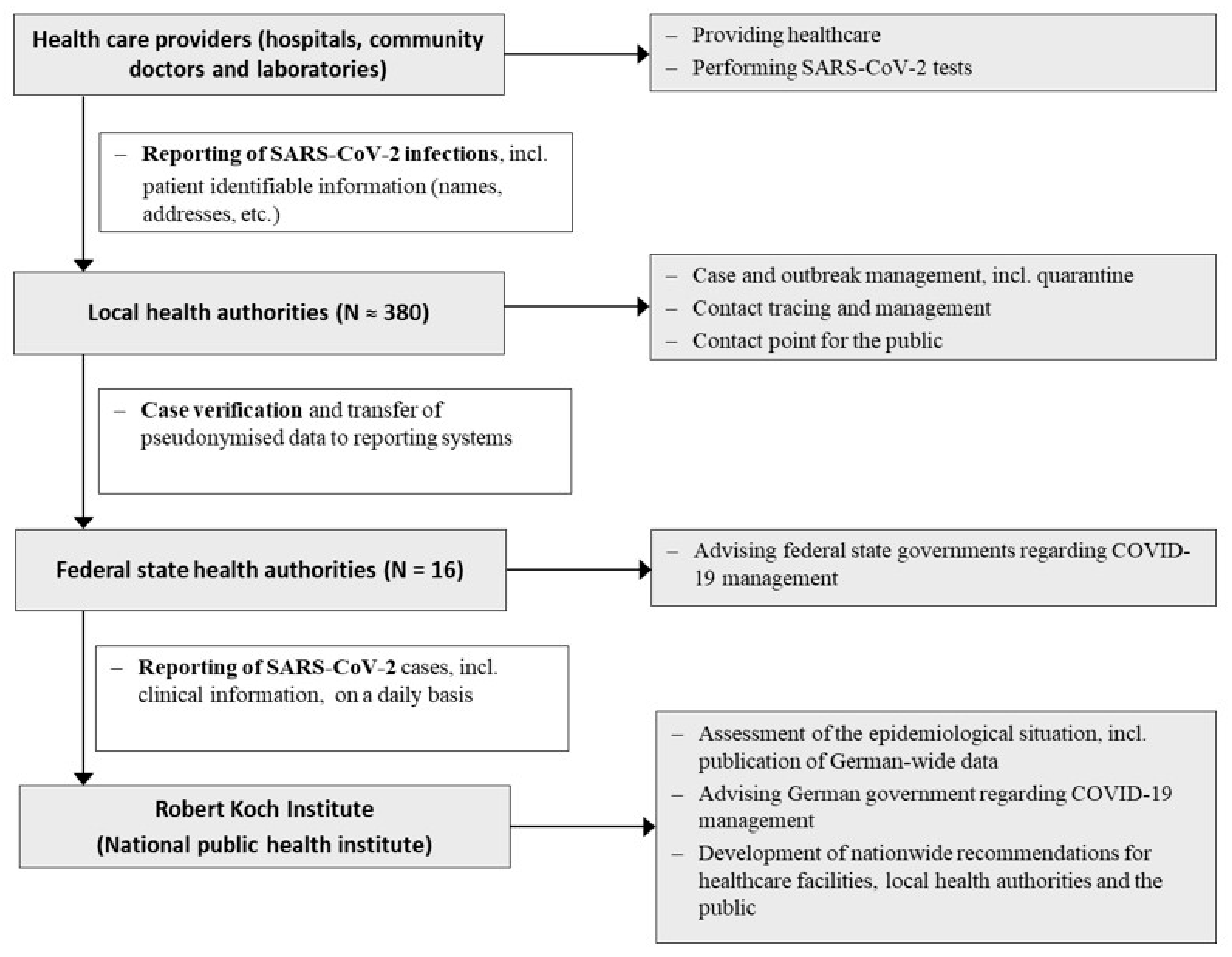
:1. Introduction
2. Methods
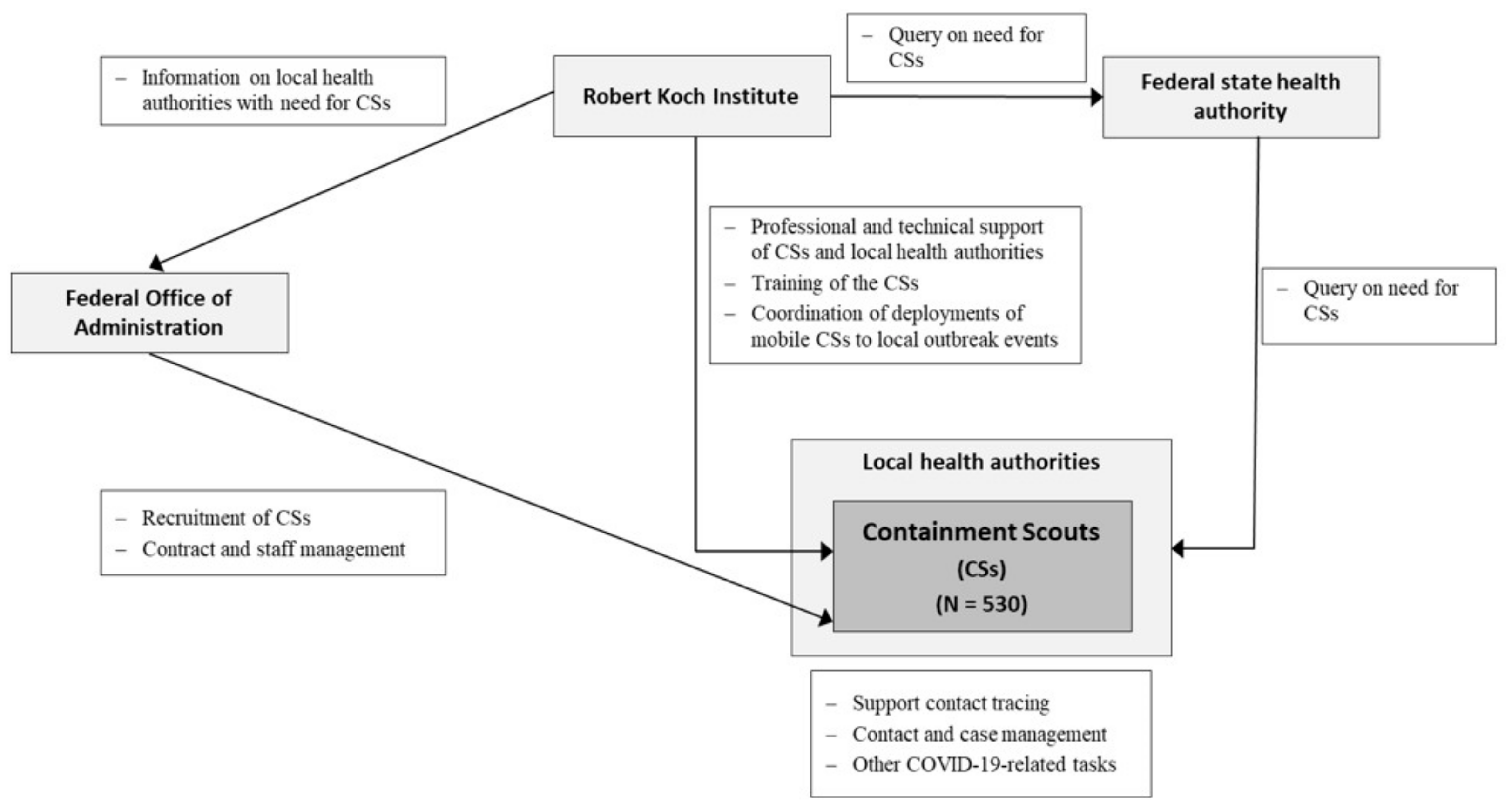
2.1. Management and Funding
2.2. Project Participation and Coordination
2.3. Containment Scouts: Job Description, Job Profile, and Training Materials
2.4. Mobile Containment Scouts
2.5. Surveys: First Assessments of the CSI
3. Results
3.1. Recruitment of the CSs and Continuous Exchange between Project Participants
3.2. Professional Background and Further Perspectives
3.3. Continued Professional Support
3.4. Task and Performance Assessment
3.5. Support of the Mobile Containment Scouts
3.6. Project Extension
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Busse, R.; Klazinga, N.; Panteli, D.; Quentin, W. Improving Healthcare Quality in Europe: Characteristics, Effectiveness and Implementation of Different Strategies; European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2019; pp. 3–18. [Google Scholar]
- Iacobucci, G. Covid-19: Underfunding of health workforce left many European nations vulnerable, says commission. BMJ 2021, 372, n724. [Google Scholar] [CrossRef] [PubMed]
- OECD. Health Workforce Policies in OECD Countries: Right Jobs, Right Skills, Right Places; OECD Publishing: Paris, France, 2016. [Google Scholar] [CrossRef]
- Deutsches Ärzteblatt. Die Kollegen Brauchen Dringend Unterstützung. Available online: https://www.aerzteblatt.de/nachrichten/111073/Die-Kollegen-brauchen-dringend-Unterstuetzung (accessed on 3 June 2021).
- Robert Koch-Institut. Ergänzung zum Nationalen Pandemieplan—COVID-19—Neuartige Coronaviruserkrankung. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Ergaenzung_Pandemieplan_Covid.pdf?__blob=publicationFile (accessed on 3 June 2021).
- European Centre for Disease Prevention and Control. Contact Tracing: Public Health Management of Persons, Including Healthcare Workers, Having Had Contact with COVID-19 Cases in the European Union—Second Update. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Contact-tracing-Public-health-management-persons-including-healthcare-workers-having-had-contact-with-COVID-19-cases-in-the-European-Union%E2%80%93second-update.pdf (accessed on 10 June 2021).
- Hernández-Quevedo, C.; Scarpetti, G.; Webb, E.; Shuftan, N.; Williams, G.A.; Birk, H.O.; Jervelund, S.S.; Krasnik, A.; Vrangbæk, K. Effective contact tracing and the role of apps: Lessons from Europe. Eurohealth 2020, 26, 40–44. [Google Scholar]
- World Health Organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.%20pdf (accessed on 10 June 2021).
- COVID-19 Contact Tracing: Challenges and Future Directions. Available online: https://www.preprints.org/manuscript/202006.0240/v2 (accessed on 10 June 2021).
- World Health Organization. Contact Tracing in the Context of COVID-19. Interim Guidance. Available online: https://apps.who.int/iris/bitstream/handle/10665/332049/WHO-2019-nCoV-Contact_Tracing-2020.1-eng.pdf?sequence=1&isAllowed=y (accessed on 2 June 2021).
- Land Berlin. Beamte helfen Gesundheitsämtern bei Kontaktnachverfolgung. Available online: https://www.berlin.de/aktuelles/berlin/6351566-958092-beamte-helfen-gesundheitsaemtern-bei-kon.html (accessed on 28 June 2021).
- Deutsches Ärzteblatt. Medizinstudierende an Gesundheitsämter Vermitteln. Available online: https://www.aerzteblatt.de/nachrichten/121480/Medizinstudierende-an-Gesundheitsaemter-vermitteln (accessed on 14 June 2021).
- Gerlinger, T.; Schmidt, P.F.; Lückenbach, C. Öffentliche Gesundheitsdienste in der COVID-19-Pandemie: Strategien und Praktiken in ausgewählten europäischen Nachbarländern. Bundesgesundheitsbla 2021, 64, 472–480. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe; European Commission Directorate-General Sante; Europea Observatory on Healt Systems and Policies. COVID-19 Health System Response Monitor. Available online: https://www.covid19healthsystem.org/searchandcompare.aspx (accessed on 31 May 2021).
- Williams, G.A.; Maier, C.B.; Scarpetti, G.; Giulio de Belvis, A.; Fattore, G.; Morsella, A.; Pastorino, G.; Poscia, A.; Ricciardi, W.; Silenzi, A. What strategies are countries using to expand health workforce surge capacity during the COVID-19 pandemic? Eurohealth 2020, 26, 51–57. [Google Scholar]
- WHO Regional Office for Europe; European Commission Directorate-General Sante; Europea Observatory on Healt Systems and Policies. How do Measures for Isolation, Quarantine, and Contact Tracing Differ among Countries? Available online: https://analysis.covid19healthsystem.org/index.php/2020/05/19/how-do-measures-for-isolation-quarantine-and-contact-tracing-differ-among-countries/ (accessed on 26 July 2021).
- Rajan, S.; Cylus, J.; Mckee, M. Successful find-test-trace-isolate-support systems: How to win at snakes and ladders. Eurohealth 2020, 26, 34–39. [Google Scholar] [CrossRef]
- Burns, K.F.; Strickland, C.J.; Horney, J.A. Public Health Student Response to COVID-19. J. Community Health 2021, 46, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Leser, K.A.; Hay, M.C.; Henebry, B.; Virden, J.; Patel, M.; Luttrell-Freeman, J.; Bailer, J. An Academic-Health Department Community Partnership to Expand Disease Investigation and Contact Tracing Capacity and Efficiency during the COVID-19 Pandemic. J. Public Health Manag. Pract. 2021. [Google Scholar] [CrossRef] [PubMed]
- Shelby, T.; Hennein, R.; Schenck, C.; Clark, K.; Meyer, A.J.; Goodwin, J.; Weeks, B.; Bond, M.; Niccolai, L.; Davis, J.L.; et al. Implementation of a volunteer contact tracing program for COVID-19 in the United States: A qualitative focus group study. PLoS ONE 2021, 16, e0251033. [Google Scholar] [CrossRef] [PubMed]
- Pelton, M.; Medina, D.; Sood, N.; Bogale, K.; Buzzelli, L.; Blaker, J.; Nye, D.; Nguyen, P.D.H.; Giglio, M.; Smiley, C.; et al. Efficacy of a student-led community contact tracing program partnered with an academic medical center during the coronavirus disease 2019 pandemic. Ann. Epidemiol. 2021, 56, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Koetter, P.; Pelton, M.; Gonzalo, J.; Du, P.; Exten, C.; Bogale, K.; Buzzelli, L.; Connolly, M.; Edel, K.; Hoffman, A.; et al. Implementation and process of a COVID-19 contact tracing initiative: Leveraging health professional students to extend the workforce during a pandemic. Am. J. Infect. Control. 2020, 48, 1451–1456. [Google Scholar] [CrossRef]
- Celentano, J.; Sachdev, D.; Hirose, M.; Ernst, A.; Reid, M. Mobilizing a COVID-19 Contact Tracing Workforce at Warp Speed: A Framework for Successful Program Implementation. Am. J. Trop Med. Hyg. 2021, 104, 1616–1619. [Google Scholar] [CrossRef]
- Murray, A.; Majwa, P.; Roberton, T.; Burnham, G. Report of the Real Time Evaluation of Ebola Control Programs in Guinea, Sierra Leone and Liberia 2015. Available online: https://www.alnap.org/help-library/report-of-the-real-time-evaluation-of-ebola-control-programs-in-guinea-sierra-leone-and (accessed on 28 August 2021).
- Centers for Disease Control and Prevention. Training Case Investigators and Contact Tracers. Available online: https://www.cdc.gov/coronavirus/2019-ncov/php/contact-tracing/contact-tracing-plan/training-investigators.html (accessed on 27 May 2021).
- Niccolai, L.; Shelby, T.; Weeks, B.; Schenck, C.; Goodwin, J.; Hennein, R.; Rossini, M.; Vazquez, J.; van Rhijn, D.; Meek, J.; et al. Community Trace: Rapid Establishment of a Volunteer Contact Tracing Program for COVID-19. Am. J. Public Health 2021, 111, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Bundesministerium für Gesundheit. Pakt für den Öffentlichen Gesundheitsdienst. Available online: https://www.bundesgesundheitsministerium.de/service/begriffe-von-a-z/o/oeffentlicher-gesundheitsheitsdienst-pakt.html (accessed on 31 May 2021).
- Deutsches Ärzteblatt. Ärztetag: Politik Liegt bei Mutterschutz und Gesundheitsämtern Zurück. Available online: https://www.aerzteblatt.de/nachrichten/sw/%D6ffentlicher%20Gesundheitsdienst?s=&p=1&n=1&nid=123605 (accessed on 20 May 2021).

{kind=link}
{kind=link}
{kind=link}
| Category | Level of Experience or Knowledge | Subject Area | % | N |
|---|---|---|---|---|
| 1 | Graduated or current student in medical or health subjects | e.g., human medicine, public health, health management | 36.0 | 103 |
| 2 | People with health-related professional background | e.g., trained (health) nurses, paramedics | 8.4 | 24 |
| 3 | Graduated or current student in non-health-related subjects | e.g., sociology, pedagogy, sports science | 53.1 | 152 |
| 4 | Not graduated or current student, or no professional health-related background | e.g., office administrator | 2.4 | 7 |
| Categorisation of contacts of SARS-CoV-2 positive cases | Could the CT value of SARS-CoV-2 cases be considered for the assessment of contact person categorisation? |
| Dealing with choir rehearsals indoors or outdoors—In case of a COVID-19 infection, should everyone who participated in the choir rehearsal be considered a contact person? | |
| Do both criteria (distance <1.5m and 15 min and longer contact) have to be met to fulfil quarantine requirements or is one criterion already sufficient? | |
| People who have been classified as category I contact person and have tested negative for SARS-CoV-2 must remain in quarantine for 14 days after the last contact with the confirmed case. Does the last contact with the confirmed case count as day 1 of quarantine? | |
| Case management | Should previous cases be reclassified as contacts after repeated exposure? |
| How does one deal with cases that remain positive over a long period of time? | |
| Contact categorisation and case management of medical staff | The hospital has several employees who, after having a SARS-CoV-2 infection, now have SARS-CoV-2 antibodies (Roche test). To what extent can this be included in the contact person categorisation? |
| How are medical staff categorised without adequate protective equipment but with simple face masks? | |
| Infectiousness | When do people who are positive for SARS-CoV-2 become infectious? |
| For a few weeks, I have observed that in families with members who are positive for SARS-CoV-2, all family members fall ill on most occasions. This was not the case in spring/summer. Is it possible that the virus has changed and has therefore become even more contagious? | |
| Travellers returning from risk areas | What is the procedure for people who return from countries where infection rates are not known/not credible? |
| How does one categorise people who return from travel abroad who had contact with people who tested positive for SARS-CoV-2 in a double-decker bus? | |
| Corona Warn App | Should people who receive a high-risk-alert by the Corona Warn App (i.e., contact with an infected person) be tested for SARS-CoV-2? If so, will the RKI adapt its recommendations accordingly? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Said, D.; Brinkwirth, S.; Taylor, A.; Markwart, R.; Eckmanns, T. The Containment Scouts: First Insights into an Initiative to Increase the Public Health Workforce for Contact Tracing during the COVID-19 Pandemic in Germany. Int. J. Environ. Res. Public Health 2021, 18, 9325. https://doi.org/10.3390/ijerph18179325
Said D, Brinkwirth S, Taylor A, Markwart R, Eckmanns T. The Containment Scouts: First Insights into an Initiative to Increase the Public Health Workforce for Contact Tracing during the COVID-19 Pandemic in Germany. International Journal of Environmental Research and Public Health. 2021; 18(17):9325. https://doi.org/10.3390/ijerph18179325
Chicago/Turabian StyleSaid, Dunja, Simon Brinkwirth, Angelina Taylor, Robby Markwart, and Tim Eckmanns. 2021. "The Containment Scouts: First Insights into an Initiative to Increase the Public Health Workforce for Contact Tracing during the COVID-19 Pandemic in Germany" International Journal of Environmental Research and Public Health 18, no. 17: 9325. https://doi.org/10.3390/ijerph18179325
APA StyleSaid, D., Brinkwirth, S., Taylor, A., Markwart, R., & Eckmanns, T. (2021). The Containment Scouts: First Insights into an Initiative to Increase the Public Health Workforce for Contact Tracing during the COVID-19 Pandemic in Germany. International Journal of Environmental Research and Public Health, 18(17), 9325. https://doi.org/10.3390/ijerph18179325