
Emotional Intelligence as a Mediator between Subjective Sleep Quality and Depression during the Confinement Due to COVID-19



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Analysis of Data
3. Results
3.1. Preliminary Analyses
3.2. Mediation Analysis
4. Discussion
- -
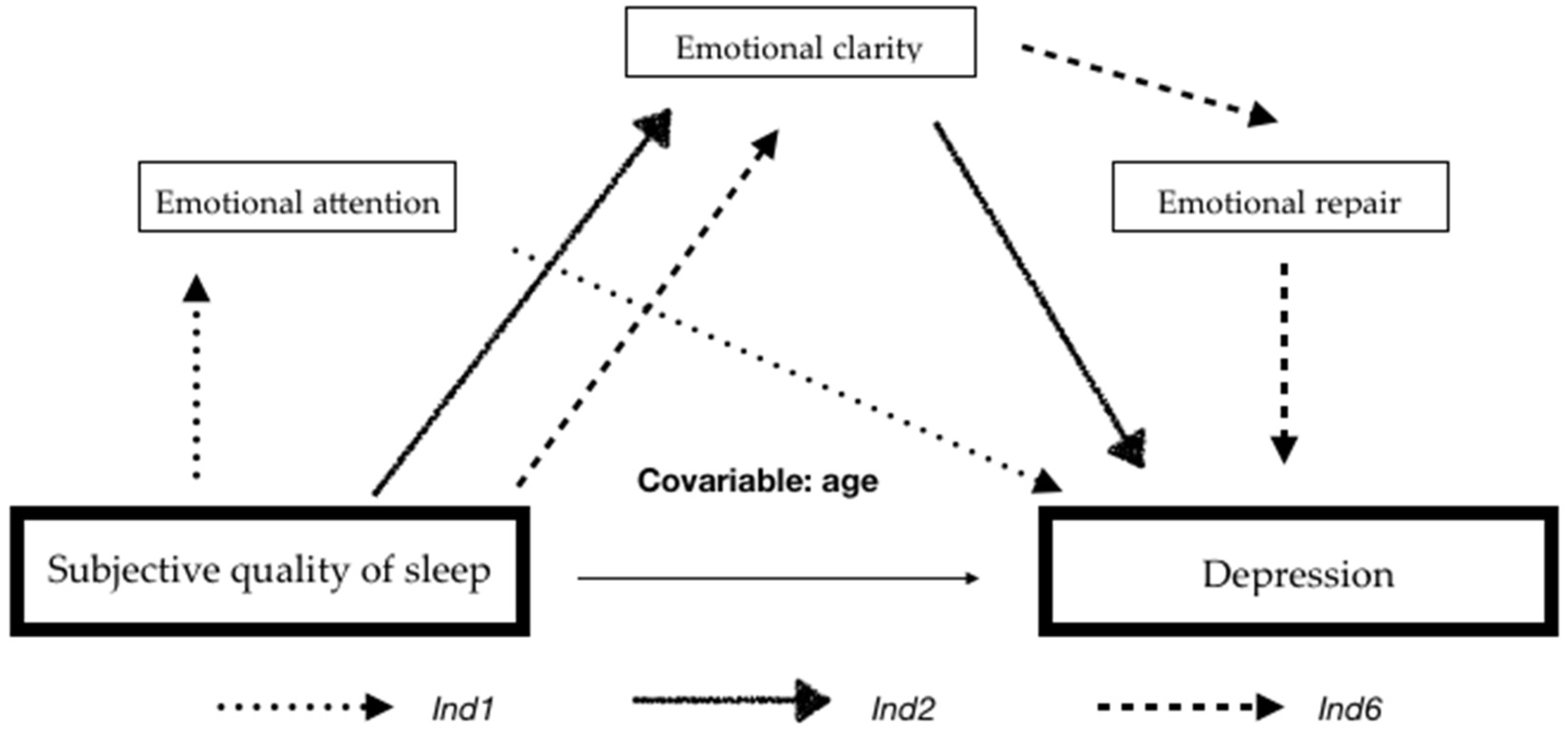
- Firstly, poor sleep quality plus high emotional attention lead to more depressive symptoms. This effect was expected since both poor sleep quality and high emotional attention lead to higher levels of depression. Thus, both factors together have the potential to induce similar effects.
- -
- Secondly, poor subjective sleep quality, along with low levels of emotional clarity, lead to higher levels of depression. The explanation could be similar to the previous case, that is, poor sleep quality is related to more depressive symptoms, and low levels of emotional clarity are also related to more depressive symptoms, indicating that both factors together may also influence levels of depression.
- -
- Thirdly, poor subjective sleep quality, along with low clarity and emotional recovery, implies higher levels of depression. This relationship is also predictable since low levels of clarity and emotional repair, as well as poor perceived sleep quality, are closely related to a high number of depressive symptoms.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ozamiz-Etxebarria, N.; Dosil-Santamaria, M.; Picaza-Gorrochategui, M.; Idoiaga-Mondragon, N. Stress, Anxiety, and Depression Levels in the Initial Stage of the COVID-19 Outbreak in a Population Sample in the Northern Spain. Cad. Saúde Pública 2020, 36, e00054020. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y. Prevalence and Predictors of PTSS during COVID-19 Outbreak in China Hardest-Hit Areas: Gender Differences Matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef]
- Shigemura, J.; Ursano, R.J.; Morganstein, J.C.; Kurosawa, M.; Benedek, D.M. Public Responses to the Novel 2019 Coronavirus (2019-nCoV) in Japan: Mental Health Consequences and Target Populations. Psychiatry Clin. Neurosci. 2020, 74, 281–282. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public. Health. 2020, 17, 1729. [Google Scholar] [CrossRef]
- González Casas, D.; Mercado García, E.; Corchado Castillo, A.I.; De la Paz Elez, P. COVID-19 y Su Asociación Con Síntomas Depresivos En Población Española. Rev. Habanera Cienc. Médicas 2020, 19. [Google Scholar]
- Sandín, B.; Valiente, R.M.; García-Escalera, J.; Chorot, P. Impacto Psicológico de La Pandemia de COVID-19: Efectos Negativos y Positivos En Población Española Asociados al Periodo de Confinamiento Nacional. Rev. Psicopatología Psicol. Clínica 2020, 25, 1–22. [Google Scholar]
- Liljenberg, B.; Almwvist, M.; Hetta, J.; Roos, B.-E.; Agren, H. Affective Disturbance and Insomnia: A Population Study. Eur. J. Psychiatry 1989, 3, 91–98. [Google Scholar]
- Feinberg, M.; Gillin, J.C.; Carroll, B.J.; Greden, J.F.; Zis, A.P. EEG Studies of Sleep in the Diagnosis of Depression. Biol. Psychiatry 1982, 305–317. [Google Scholar]
- Royuela, A.; Macías, J. Calidad de Sueño En Pacientes Ansiosos y Depresivos. Psiquiatr. Biológica 1997, 4, 225–230. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Miró, E.; Martínez, P.; Arriaza, R. Influencia de La Cantidad y La Calidad Subjetiva de Sueño En La Ansiedad y El Estado de Ánimo Deprimido. SaludMent. 2006, 29, 30–37. [Google Scholar]
- Benca, R.M.; Obermeyer, W.H.; Thisted, R.A.; Gillin, J.C. Sleep and Psychiatric Disorders: A Meta-Analysis. Arch. Gen. Psychiatry 1992, 49, 651–668. [Google Scholar] [CrossRef]
- Moo-Estrella, J.; Pérez-Benítez, H.; Solís-Rodríguez, F.; Arankowsky-Sandoval, G. Evaluation of Depressive Symptoms and Sleep Alterations in College Students. Arch. Med. Res. 2005, 36, 393–398. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Zulley, J. Correlates of Global Sleep Dissatisfaction in the German Population. Sleep 2001, 24, 780–787. [Google Scholar]
- Cano, M. del C.; Miró, E.; Espinosa, L.; Buela-Casal, G. Parámetros Subjetivos de Sueño y Estado de Ánimo Disfórico. Rev. Psicopatología Psicol. Clínica 2004, 9, 35–48. [Google Scholar]
- Pilcher, J.J.; Ginter, D.R.; Sadowsky, B. Sleep Quality versus Sleep Quantity: Relationships between Sleep and Measures of Health, Well-Being and Sleepiness in College Students. J. Psychosom. Res. 1997, 42, 583–596. [Google Scholar] [CrossRef]
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of Knowledge, Attitude, Anxiety & Perceived Mental Healthcare Need in Indian Population during COVID-19 Pandemic. Asian J. Psychiatry 2020, 51, 102083. [Google Scholar]
- Mayer, J.D.; Salovey, P. What is emotional intelligence? In Emotional Development and Emotional Intelligence: Educational Implications, 2nd ed.; Basic: New York, NY, USA, 1997; pp. 3–31. [Google Scholar]
- Barraza-López, R.J.; Muñoz-Navarro, N.A.; Behrens-Pérez, C.C. Relación Entre Inteligencia Emocional y Depresión-Ansiedad y Estrés En Estudiantes de Medicina de Primer Año. Rev. Chil. Neuro-Psiquiatr. 2017, 55, 18–25. [Google Scholar] [CrossRef]
- Montenegro, J. La Inteligencia Emocional y Su Efecto Protector Ante La Ansiedad, Depresión y El Estrés Académico En Estudiantes Universitarios. TZHOECOEN 2020, 12, 449–461. [Google Scholar] [CrossRef]
- Rodríguez, U.; Suárez, Y. Relación Entre Inteligencia Emocional, Depresión y Rendimiento Académico En Estudiantes de Psicología. Psicogente 2012, 15, 348–359. [Google Scholar]
- Royuela, A.; Macías, J.A. Propiedades Clinimétricas de La Versión Castellana Del Cuestionario de Pittsburgh. Vigilia-Sueño 1997, 9, 81–94. [Google Scholar]
- Salovey, P.; Mayer, J.D.; Goldman, S.L.; Turvey, C.; Palfai, T.P. Emotional attention, clarity, and repair: Exploring emotional intelligence using the Trait Meta-Mood Scale. In Emotion, Disclosure, and Health; American Psychological Assn.: Washington, DC, USA, 1995; pp. 125–154. [Google Scholar]
- Fernández-Berrocal, P.; Extremera, N.; Ramos, N. Validity and Reliability of the Spanish Modified Version of the Trait Meta-Mood Scale. Psychol. Rep. 2004, 94, 751–755. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory The Psychological Corporation. San Antonio TX 1996. Available online: https://www.nctsn.org/measures/beck-depression-inventory-second-edition (accessed on 17 August 2021).
- Sanz, J.; García-Vera, M.P. Rendimiento diagnóstico y estructura factorial del Inventario de depresión de Beck-II (BDI-II). Anales de Psicología 2013, 29, 66–75. [Google Scholar]
- Salguero Noguera, J.M.; Iruarrizaga Díez, I. Relaciones Entre Inteligencia Emocional Percibida y Emocionalidad Negativa: Ansiedad, Ira y Tristeza/Depresión. Ansiedad Estrés 2006, 12, 207–221. [Google Scholar]
- Extremera, N.; Fernández-Berrocal, P.; Ruiz-Aranda, D.; Cabello, R. Inteligencia Emocional, Estilos de Respuesta y Depresión. Ansiedad Estrés 2006, 12, 191–205. [Google Scholar]
- Montesó-Curto, P.; Aguilar-Martín, C. Depresión Según La Edad y El Género: Análisis En Una Comunidad. Aten. Primaria 2014, 46, 167–172. [Google Scholar] [CrossRef] [PubMed][Green Version]



{kind=link}
{kind=link}
| Instruments | Men | Women | Overall | Spearman’s Rho Correlations | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | 1 | 2 | 3 | 4 | |
| 1. Subjective sleep quality | 1.11 | 0.61 | 1.57 | 0.81 | 1.43 | 0.78 | - | |||
| 2. Emotional Attention | 21.25 | 7.12 | 23.63 | 7.30 | 22.86 | 7.31 | 0.194 ** | - | ||
| 3. Emotional Clarity | 25.51 | 7.46 | 25.20 | 7.86 | 25.30 | 7.72 | −0.143 * | 0.450 ** | - | |
| 4. Emotional Repair | 26.21 | 7.67 | 25.78 | 7.25 | 25.92 | 7.37 | −0.048 | 0.333 ** | 0.618 ** | - |
| 5. Depression | 6.51 | 6.91 | 10.10 | 8.51 | 8.95 | 8.19 | 0.528 ** | 0.200 ** | −0.198 ** | −0.176 * |
| Path | Coefficient | SE | Boot LLCI | Boot ULCI | t | p |
|---|---|---|---|---|---|---|
| Total effect (c) | 4.448 | 0.701 | 3.065 | 5.832 | 6.346 | 0.000 |
| Direct effect (c′) | 3.377 | 0.689 | 2.018 | 4.737 | 4.901 | 0.000 |
| a1 | 1.473 | 0.707 | 0.0775 | 2.868 | 2.082 | 0.039 |
| a2 | −2.625 | 0.665 | −3.938 | −1.312 | −3.945 | 0.000 |
| a3 | 0.190 | 0.593 | −0.979 | 1.360 | 0.321 | 0.748 |
| b1 | 0.353 | 0.078 | 0.199 | 0.508 | 4.521 | 0.000 |
| b2 | −0.218 | 0.089 | −0.393 | −0.043 | −2.462 | 0.015 |
| b3 | −0.186 | 0.086 | −0.356 | −0.017 | −2.166 | 0.032 |
| d21 | 0.514 | 0.068 | 0.379 | 0.649 | 7.499 | 0.000 |
| d31 | 0.078 | 0.067 | −0.054 | 0.211 | 1.169 | 0.244 |
| d32 | 0.574 | 0.063 | 0.449 | 0.699 | 9.083 | 0.000 |
| Indirect effects | Effect | SE | Boot LLCI | Boot ULCI | ||
| Total indirect effect | 1.071 | 0.375 | 0.401 | 1.861 | ||
| Ind1: a1b1 | 0.521 | 0.292 | 0.015 | 1.159 | ||
| Ind2: a2b2 | 0.573 | 0.259 | 0.126 | 1.141 | ||
| Ind6: a2d32b3 | 0.281 | 0.146 | 0.052 | 0.619 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salguero-Alcañiz, M.P.; Merchán-Clavellino, A.; Alameda-Bailén, J.R. Emotional Intelligence as a Mediator between Subjective Sleep Quality and Depression during the Confinement Due to COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 8837. https://doi.org/10.3390/ijerph18168837
Salguero-Alcañiz MP, Merchán-Clavellino A, Alameda-Bailén JR. Emotional Intelligence as a Mediator between Subjective Sleep Quality and Depression during the Confinement Due to COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(16):8837. https://doi.org/10.3390/ijerph18168837
Chicago/Turabian StyleSalguero-Alcañiz, María Pilar, Ana Merchán-Clavellino, and Jose Ramón Alameda-Bailén. 2021. "Emotional Intelligence as a Mediator between Subjective Sleep Quality and Depression during the Confinement Due to COVID-19" International Journal of Environmental Research and Public Health 18, no. 16: 8837. https://doi.org/10.3390/ijerph18168837
APA StyleSalguero-Alcañiz, M. P., Merchán-Clavellino, A., & Alameda-Bailén, J. R. (2021). Emotional Intelligence as a Mediator between Subjective Sleep Quality and Depression during the Confinement Due to COVID-19. International Journal of Environmental Research and Public Health, 18(16), 8837. https://doi.org/10.3390/ijerph18168837