
Identifying Risk and Resilience Factors Impacting Mental Health among Black and Latinx Adults following Nocturnal Tornadoes in the U.S. Southeast



Abstract
:1. Introduction
1.1. Tornado Warnings, Exposure, and Mental Health
1.2. Resilience Factors and Mental Health
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.3. Analyses
3. Results
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carter, L.; Terando, A.; Dow, K.; Hiers, K.; Kunkel, K.E.; Lascurain, A.; Marcy, D.; Osland, M.; Schramm, P. Chapter 19: Southeast. In Impacts, Risks, and Adaptation in the United States: Fourth National Climate Assessment, Volume II; Reidmiller, D.R., Avery, C.W., Easterling, D.R., Kunkel, K.E., Lewis, K.L.M., Maycock, T.K., Stewart, B.C., Eds.; U.S. Global Change Research Program: Washington, DC, USA, 2018; pp. 743–808. [Google Scholar]
- Roach, J. AccuWeather Estimates the Total Damage from the Tennessee Tornadoes will Approach $2 Billion. 2020. Available online: https://www.accuweather.com/en/severe-weather/accuweather-estimates-the-total-damage-from-the-tennessee-tornadoes-will-approach-2-billion/697185 (accessed on 20 March 2021).
- NOAA, Cited 2021. Available online: https://www.weather.gov/ohx/20200303 (accessed on 17 May 2021).
- Ashley, W.S. Spatial and Temporal Analysis of Tornado Fatalities in the United States: 1880–2005. Weather. Forecast. 2007, 22, 1214–1228. [Google Scholar] [CrossRef]
- Ashley, W.S.; Krmenec, A.J.; Schwantes, R. Vulnerability due to Nocturnal Tornadoes. Weather. Forecast. 2008, 23, 795–807. [Google Scholar] [CrossRef]
- Ellis, K.N.; Mason, L.R.; Hurley, K. In the dark: Public perceptions of and National Weather Service forecaster considerations for nocturnal tornadoes in Tennessee. Bull. Am. Meteorol. Soc. 2020, 101, E1677–E1684. [Google Scholar] [CrossRef]
- Mason, L.R.; Ellis, K.N.; Winchester, B.; Schexnayder, S. Tornado Warnings at Night: Who Gets the Message? Weather Clim. Soc. 2018, 10, 561–568. [Google Scholar] [CrossRef]
- El Sayed, A.M.; Galea, S. Climate change and population health. In Global Climate Change and Human Health: From Science to Practice; Luber, G., Lemery, J., Eds.; WILEY: Hoboken, NJ, USA, 2015. [Google Scholar]
- Mason, L.R.; Sharma, B.B.; Walters, J.E.; Ekenga, C.C. Mental Health and Weather Extremes in a Southeastern U.S. City: Exploring Group Differences by Race. Int. J. Environ. Res. Public Health 2020, 17, 3411. [Google Scholar] [CrossRef] [PubMed]
- Rataj, E.; Kunzweiler, K.; Garthus-Niegel, S. Extreme weather events in developing countries and related injuries and mental health disorders—A systematic review. BMC Public Health 2016, 16, 1020. [Google Scholar] [CrossRef] [Green Version]
- Galea, S.; Nandi, A.; Vlahov, D. The Epidemiology of Post-Traumatic Stress Disorder after Disasters. Epidemiol. Rev. 2005, 27, 78–91. [Google Scholar] [CrossRef] [Green Version]
- Goldmann, E.; Galea, S. Mental Health Consequences of Disasters. Annu. Rev. Public Health 2014, 35, 169–183. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, A.C.; Norris, F.H. Definitions and Concepts in Disaster Research. Methods for Disaster Mental Health Research; The Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Houston, J.B.; Spialek, M.L.; Stevens, J.; First, J.; Mieseler, V.L.; Pfefferbaum, B. 2011 Joplin, Missouri tornado experience, mental health reactions, and service utilization: Cross-sectional assessments at approximately 6 months and 2.5 years post-event. PLoS Curr. 2015, 7. [Google Scholar] [CrossRef]
- Norris, F.H. Disaster research methods: Past progress and future directions. J. Trauma. Stress 2006, 19, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Ahern, J.; Galea, S. Social context and depression after a disaster: The role of income inequality. J. Epidemiol. Community Health 2006, 60, 766–770. [Google Scholar] [CrossRef] [Green Version]
- Bethel, J.W.; Burke, S.C.; Britt, A.F. Disparity in disaster preparedness between racial/ ethnic groups. Disaster Health 2013, 1, 110–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenman, D.P.; Glik, D.; Gonzalez, L.; Maranon, R.; Zhou, Q.; Tseng, C.H.; Asch, S.M. Improving Latino disaster preparedness using social networks. Am. J. Prev. Med. 2009, 37, 512–517. [Google Scholar] [CrossRef]
- Lim, J.; Loveridge, S.; Shupp, R.; Skidmore, M. Double danger in the double wide: Dimensions of poverty, housing quality and tornado impacts. Reg. Sci. Urban. Econ. 2017, 65, 1–15. [Google Scholar] [CrossRef]
- Prohaska, A. Still struggling: Intersectionality, vulnerability, and long-term recovery after the Tuscaloosa, Alabama USA Tornado. Crit. Policy Stud. 2020, 4, 466–487. [Google Scholar] [CrossRef]
- Reid, M. Disasters and Social Inequalities. Sociol. Compass 2013, 7, 984–997. [Google Scholar] [CrossRef]
- Emrich, C.T.; Cutter, S.L. Social Vulnerability to Climate-Sensitive Hazards in the Southern United States. Weather Clim. Soc. 2011, 3, 193–208. [Google Scholar] [CrossRef]
- Lindell, M.K.; Perry, R.W. The protective action decision model: Theoretical modifications and additional evidence. Risk Anal. Int. J. 2012, 32, 616–632. [Google Scholar] [CrossRef]
- Purtle, J. Racial and Ethnic Disparities in Post-Disaster Mental Health: Examining the Evidence through a Lens of Social Justice. Wash. Lee J. Civ. Rts. Soc. Just. 2012, 19, 31–55. Available online: https://scholarlycommons.law.wlu.edu/crsj/vol19/iss1/7 (accessed on 21 July 2021).
- Kuo, S.S. Speaking in tongues: Mandating multilingual disaster warnings in the public interest. Wash. LeeJ. Civ. Rts. Soc. Just. 2007, 14, 3–47. Available online: https://scholarlycommons.law.wlu.edu/crsj/vol14/iss1/4 (accessed on 21 July 2021).
- Spence, P.R.; Lachlan, K.A.; Griffin, D.R. Crisis Communication, Race, and Natural Disasters. J. Black Stud. 2007, 37, 539–554. [Google Scholar] [CrossRef]
- Cruz, J.; White, P.C.L.; Bell, A.; Coventry, P.A. Effect of Extreme Weather Events on Mental Health: A Narrative Synthesis and Meta-Analysis for the UK. Int. J. Env. Res. Public Health 2020, 17, 8581. [Google Scholar] [CrossRef]
- Munro, A.; Kovats, R.S.; Rubin, G.J.; Waite, T.D.; Bone, A.; Armstrong, B.; Beck, C.R.; Amlot, R.; Leonardi, G.; Oliver, I. Effect of evacuation and displacement on the association between flooding and mental health outcomes: A cross-sectional analysis of UK survey data. Lancet Planet. Health 2017, 1, e134–e141. [Google Scholar] [CrossRef]
- Tunstall, S.; Tapsell, S.; Green, C.; Floyd, P.; George, C. The health effects of flooding: Social research results from England and Wales. J. Water Health 2006, 4, 365–380. [Google Scholar] [CrossRef] [PubMed]
- Neria, Y.; Nandi, A.; Galea, S. Post-traumatic stress disorder following disasters: A systematic review. Psychol. Med. 2008, 38, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Brewin, C.R.; Andrews, B.; Valentine, J.D. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J. Consult. Clin. Psychol. 2000, 68, 748. [Google Scholar] [CrossRef] [PubMed]
- Lowe, S.R.; McGrath, J.A.; Young, M.N.; Kwok, R.K.; Engel, L.S.; Galea, S.; Sandler, D.P. Cumulative Disaster Exposure and Mental and Physical Health Symptoms Among a Large Sample of Gulf Coast Residents. J. Trauma Stress 2019, 32, 196–205. [Google Scholar] [CrossRef]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniasty, K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981-2001. Psychiatry 2002, 65, 207–239. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, R.M.; Gillezeau, C.N.; Liu, B.; Lieberman-Cribbin, W.; Taioli, E. Longitudinal Impact of Hurricane Sandy Exposure on Mental Health Symptoms. Int. J. Environ. Res. Public Health 2017, 14, 957. [Google Scholar] [CrossRef]
- Davidson, T.M.; Price, M.; McCauley, J.L.; Ruggiero, K.J. Disaster impact across cultural groups: Comparison of Whites, African Americans, and Latinos. Am. J. Community Psychol. 2013, 52, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Panter-Brick, C.; Leckman, J.F. Editorial Commentary: Resilience in child development--interconnected pathways to wellbeing. J. Child Psychol. Psychiatry Allied Discip. 2013, 54, 333–336. [Google Scholar] [CrossRef]
- Norris, F.H.; Stevens, S.P.; Pfefferbaum, B.; Wyche, K.F.; Pfefferbaum, R.L. Community Resilience as a Metaphor, Theory, Set of Capacities, and Strategy for Disaster Readiness. Am. J. Community Psychol. 2008, 41, 127–150. [Google Scholar] [CrossRef] [PubMed]
- Constantine, M.G.; Alleyne, V.L.; Caldwell, L.D.; McRae, M.B.; Suzuki, L.A. Coping responses of Asian, Black, and Latino/Latina New York City residents following the September 11, 2001 terrorist attacks against the United States. Cult. Divers. Ethn. Minority Psychol. 2005, 11, 293–308. [Google Scholar] [CrossRef]
- Constantine, M.G.; Gainor, K.A.; Ahluwalia, M.K.; Berkel, L.A. Independent and Interdependent Self-Construals, Individualism, Collectivism, and Harmony Control in African Americans. J. Black Psychol. 2003, 29, 87–101. [Google Scholar] [CrossRef]
- Ferreira, R.J.; Adolph, V.; Hall, M.; Buttell, F. Predictors of Individual Resilience: Gender Differences among African Americans. J. Evid. Based Soc. Work. 2019, 16, 347–362. [Google Scholar] [CrossRef]
- Schuster, M.A.; Stein, B.D.; Jaycox, L.H.; Collins, R.L.; Marshall, G.N.; Elliott, M.N.; Zhou, A.J.; Kanouse, D.E.; Morrison, J.L.; Berry, S.H. A National Survey of Stress Reactions after the September 11, 2001, Terrorist Attacks. N. Engl. J. Med. 2001, 345, 1507–1512. [Google Scholar] [CrossRef]
- Mitchell, S.J.; Ronzio, C.R. Violence and Other Stressful Life Events as Triggers of Depression and Anxiety: What Psychosocial Resources Protect African American Mothers? Matern. Child. Health J. 2011, 15, 1272–1281. [Google Scholar] [CrossRef]
- Utsey, S.O.; Giesbrecht, N.; Hook, J.; Stanard, P.M. Cultural, sociofamilial, and psychological resources that inhibit psychological distress in African Americans exposed to stressful life events and race-related stress. J. Couns. Psychol. 2008, 55, 49–62. [Google Scholar] [CrossRef]
- Osofsky, H.J.; Osofsky, J.D.; Hansel, T.C. Deepwater Horizon oil spill: Mental health effects on residents in heavily affected areas. Disaster Med. Public Health Prep. 2011, 5, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Galea, S.; Bucciarelli, A.; Vlahov, D. What predicts psychological resilience after disaster? The role of demographics, resources, and life stress. J. Consult. Clin. Psychol. 2007, 75, 671–682. [Google Scholar] [CrossRef]
- First, J.M.; Yu, M.; Houston, J.B. Development and Validation of the Disaster Adaptation and Resilience Scale (DARS): Development and Validation of an Individual-level Protection Measure. Disasters 2021. Advance online publication. [Google Scholar] [CrossRef]
- Jongen, C.; Langham, E.; Bainbridge, R.; McCalman, J. Instruments for Measuring the Resilience of Indigenous Adolescents: An Exploratory Review. Front. Public Health 2019, 7, 194. Available online: https://www.frontiersin.org/article/10.3389/fpubh.2019.00194 (accessed on 20 July 2021). [CrossRef] [Green Version]
- Raghavan, S.; Sandanapitchai, P. The relationship between cultural variables and resilience to psychological trauma: A systematic review of the literature. Traumatology 2020. Advance online publication. [Google Scholar] [CrossRef]
- Ungar, M. Social ecologies and their contribution to resilience. In The Social Ecology of Resilience: A Handbook of Theory and Practice; Ungar, M., Ed.; Springer: New York, NY, USA, 2012; pp. 13–31. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A language and environment for statistical computing. In R Foundation for Statistical Computing; 2016; Available online: https://www.R-project.org/ (accessed on 5 July 2021).
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Little, T.D. Longitudinal Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Walters, J.E.; Mason, L.R.; Ellis, K.; Winchester, B. Staying safe in a tornado: A qualitative inquiry into public knowledge, access, and response to tornado warnings. Weather. Forecast. 2020, 35, 67–81. [Google Scholar] [CrossRef]
- Sutter, D.; Simmons, K.M. Tornado fatalities and mobile homes in the United States. Nat. Hazards 2010, 53, 125–137. [Google Scholar] [CrossRef]
- Shenesey, J.W.; Langhinrichsen-Rohling, J. Perceived resilience: Examining impacts of the deepwater horizon oil spill one-year post-spill. Psychol. Trauma: Theory Res. Pract. Policy 2015, 7, 252–258. [Google Scholar] [CrossRef]
- Windle, G. What is resilience? A review and concept analysis. Rev. Clin. Gerontol. 2011, 21, 152–169. [Google Scholar] [CrossRef]
- Abramson, D.M.; Grattan, L.M.; Mayer, B.; Colten, C.E.; Arosemena, F.A.; Bedimo-Rung, A.; Lichtveld, M. The resilience activation framework: A conceptual model of how access to social resources promotes adaptation and rapid recovery in post-disaster settings. J. Behav. Health Serv. Res. 2015, 42, 42–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobfoll, S.E.; Stevens, N.R.; Zalta, A.K. Expanding the Science of Resilience: Conserving Resources in the Aid of Adaptation. Psychol. Inq. 2015, 26, 174–180. [Google Scholar] [CrossRef] [Green Version]
- McKnight-Eily, L.R.; Okoro, C.A.; Strine, T.W.; Verlenden, J.; Hollis, N.D.; Njai, R.; Mitchell, E.W.; Board, A.; Puddy, R.; Thomas, C. Racial and Ethnic Disparities in the Prevalence of Stress and Worry, Mental Health Conditions, and Increased Substance Use Among Adults During the COVID-19 Pandemic—United States, April and May 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Teo, M.; Goonetilleke, A.; Deilami, K.; Ahankoob, A.; Lawie, M. Engaging Residents from Different Ethnic and Language Backgrounds in Disaster Preparedness. Int. J. Disaster Risk Reduct. 2019, 39, 101–245. [Google Scholar] [CrossRef]
- Klaiman, T.; Knorr, D.; Fitzgerald, S.; DeMara, P.; Thomas, C.; Heake, G.; Hausman, A. Locating and Communicating with At-Risk Populations About Emergency Preparedness: The Vulnerable Populations Outreach Model. Disaster Med. Public Health Prep. 2010, 4, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Clay, L.; Goetschius, J.; Papas, M.; Kendra, J. Influence of Mental Health on Disaster Preparedness: Findings from the Behavioral Risk Factor Surveillance System, 2007–2009. J. Homel. Secur. Emerg. Manag. 2014, 11, 375–392. [Google Scholar] [CrossRef]
- Maxwell, S.E.; Cole, D.A. Bias in cross-sectional analyses of longitudinal mediation. Psychol. Methods 2007, 12, 23–44. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Variables | N | % |
|---|---|---|
| Gender | ||
| Female | 150 | 67.9 |
| Male | 68 | 30.8 |
| Transgender | 2 | 0.90 |
| Non-binary | 1 | 0.50 |
| Race/Ethnicity | ||
| Black/African American/Afro-Caribbean | 150 | 67.9 |
| Hispanic/Latino | 71 | 32.2 |
| Age | ||
| 18–29 | 125 | 56.6 |
| 30–49 | 68 | 30.8 |
| 50–69 | 24 | 10.9 |
| Over 70 | 4 | 1.8 |
| Income | ||
| Less than $15,000 | 47 | 21.5 |
| $15,000 to $29,999 | 34 | 15.5 |
| $30,000 to $44,999 | 40 | 18.3 |
| $45,000 to $59,999 | 32 | 14.6 |
| $60,000 to $74,999 | 20 | 9.1 |
| $75,000 to $104,999 | 24 | 11.0 |
| $105,000 to $119,000 | 22 | 10.0 |
| Education | ||
| Grade School | 4 | 1.8 |
| Some High School | 16 | 7.2 |
| High School Graduate | 63 | 28.5 |
| Some College | 59 | 26.7 |
| College Graduate | 52 | 23.5 |
| Advanced Degree | 27 | 12.2 |
| Housing Structure | ||
| Mobile Home | 31 | 14.1 |
| House detached from other buildings | 101 | 45.9 |
| House attached to other buildings | 38 | 17.3 |
| Apartment building | 48 | 21.7 |
| Boat, RV, Van, etc. | 2 | 0.90 |
| Barriers to Tornado Warning Alerts | ||
| Language barriers | 25 | 11.3 |
| Being asleep | 104 | 47.1 |
| No access to smart phone for alerts | 41 | 18.6 |
| No access to NOAA weather radio | 33 | 14.9 |
| Family, friends, neighbors were asleep | 58 | 26.2 |
| Did not hear sirens | 61 | 27.6 |
| Tornado Exposure | ||
| Property damage in tornado | 87 | 39.4 |
| Injured from tornado | 35 | 6.31 |
| Knew people with property damage from tornado | 146 | 66.0 |
| Believed self or loved one would be killed or harmed by tornado | 149 | 67.4 |
| Felt helplessness, fear, or horror during tornado | 153 | 69.2 |
| Viewed damaged areas, debris, people injured after tornado | 175 | 79.2 |
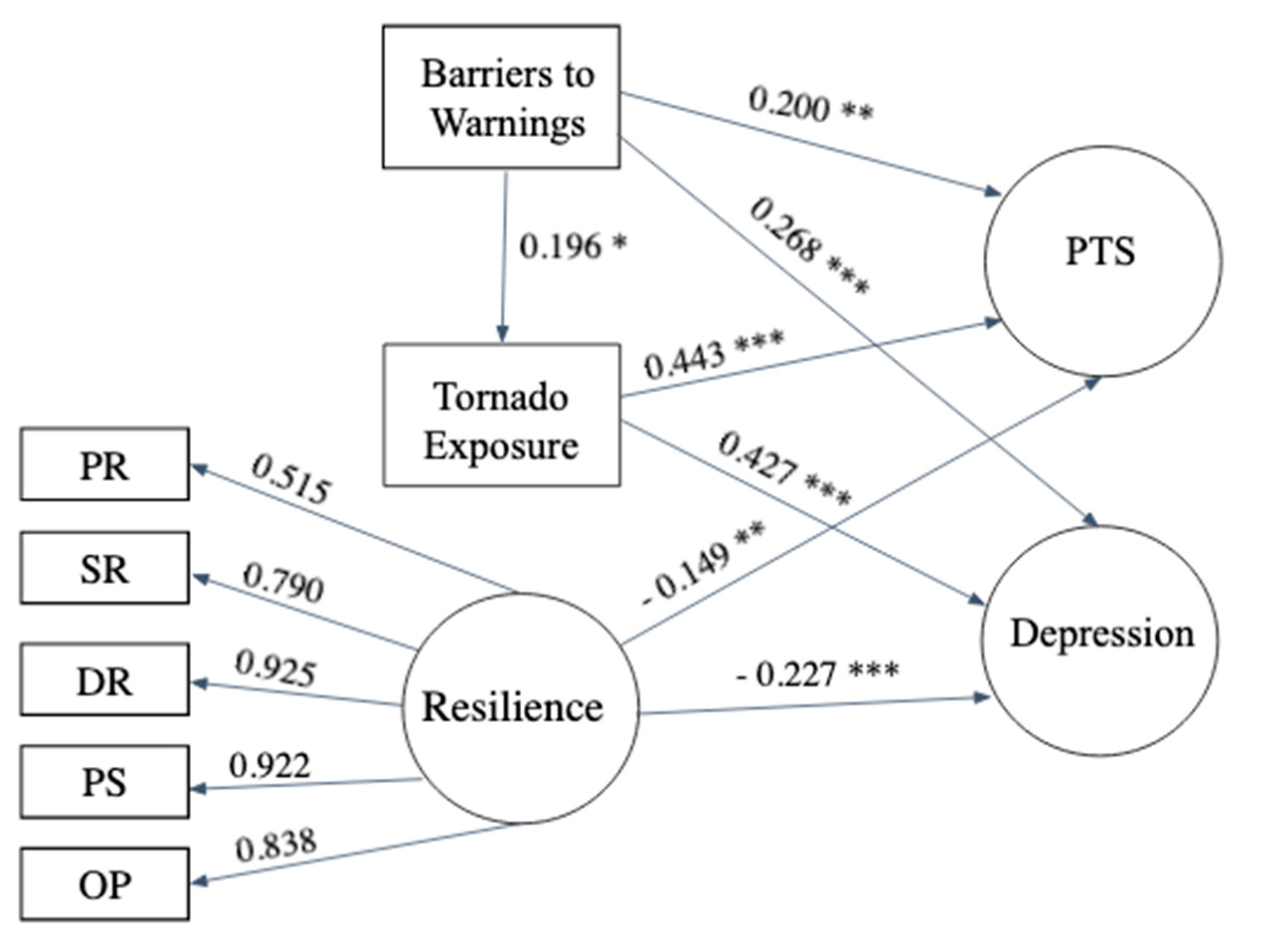
| Regression Paths | Unstandardized Estimate | Standard Error | Standard Estimate |
|---|---|---|---|
| Tornado Exposure (R2 = 0.038) | |||
| Barriers to Warnings | 0.238 | 0.032 | 0.196 * |
| Post-traumatic Stress (R2 = 0.293) | |||
| Barriers to Warnings | 0.224 | 0.065 | 0.199 ** |
| Tornado Exposure | 0.117 | 0.022 | 0.443 *** |
| Resilience | −0.177 | 0.081 | −0.149 ** |
| Depression (R2 = 0.350) | |||
| Barriers to Warnings | 0.315 | 0.074 | 0.268 *** |
| Tornado Exposure | 0.118 | 0.019 | 0.427 *** |
| Resilience | −0.285 | 0.068 | −0.229 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
First, J.M.; Ellis, K.; Held, M.L.; Glass, F. Identifying Risk and Resilience Factors Impacting Mental Health among Black and Latinx Adults following Nocturnal Tornadoes in the U.S. Southeast. Int. J. Environ. Res. Public Health 2021, 18, 8609. https://doi.org/10.3390/ijerph18168609
First JM, Ellis K, Held ML, Glass F. Identifying Risk and Resilience Factors Impacting Mental Health among Black and Latinx Adults following Nocturnal Tornadoes in the U.S. Southeast. International Journal of Environmental Research and Public Health. 2021; 18(16):8609. https://doi.org/10.3390/ijerph18168609
Chicago/Turabian StyleFirst, Jennifer M., Kelsey Ellis, Mary Lehman Held, and Florence Glass. 2021. "Identifying Risk and Resilience Factors Impacting Mental Health among Black and Latinx Adults following Nocturnal Tornadoes in the U.S. Southeast" International Journal of Environmental Research and Public Health 18, no. 16: 8609. https://doi.org/10.3390/ijerph18168609
APA StyleFirst, J. M., Ellis, K., Held, M. L., & Glass, F. (2021). Identifying Risk and Resilience Factors Impacting Mental Health among Black and Latinx Adults following Nocturnal Tornadoes in the U.S. Southeast. International Journal of Environmental Research and Public Health, 18(16), 8609. https://doi.org/10.3390/ijerph18168609