Abstract
This review was undertaken to identify the perceived barriers and facilitators of nurses’ and physicians’ willingness to work during a respiratory disease outbreak. This mixed-methods systematic review involved the extraction of data from the electronic databases PubMed, Web of Science, CINAHL, and PsycINFO and from a manual search of articles published between 2003 and April 2021. The quality of the included studies was assessed using a mixed-method appraisal tool. A total of 29 studies were eligible for inclusion: 21 quantitative and 8 qualitative. Using the Integrated Behavioral Model, perceived barriers and facilitators were identified under seven categories: demographics, attitude, perceived norm, personal agency, knowledge and skills to perform the behavior, environmental constraints, and habit. The results of this study broaden the understanding of various factors that affect nurses’ and physicians’ willingness to work during a respiratory disease outbreak. These findings will facilitate the modification of current pandemic workplace staffing strategies and practices and will inform preparedness planning for similar situations in the future.
1. Introduction
During a disease outbreak, increased capacity in terms of personnel, equipment, supplies, and structure is needed to address surge capacity across health facilities [1]. Although all resources are important, adequate staffing and availability of healthcare is necessary to address patient and community needs during a respiratory disease outbreak, such as the most recent coronavirus disease (COVID-19) pandemic. It is essential to secure sufficient numbers of healthcare workers, including nurses and physicians, during a respiratory disease outbreak [2], as it is the workers and not the facility beds, ventilators, or other equipment that actually provide frontline care. Nurses and physicians are usually expected to sacrifice their own health and well-being for the benefit of patients during a public health emergency such as the COVID-19 pandemic [3]. Many ethical and societal factors contribute to the notion or the need to sacrifice and can vary between providers and facilities. However, through research focused on the severe acute respiratory syndrome (SARS) outbreak [4], the H1N1 influenza pandemic [5], and the COVID-19 pandemic [6], researchers have demonstrated that nurses or physicians may refuse to participate in caring for patients who are infected or suspected to be infected with novel diseases during outbreaks. For example, in a recent study, approximately 23% of psychiatrists and nurses in China expressed unwillingness to care for patients infected with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes COVID-19 [7]. In an Australian study, about 39% of the nurses reported that they were unwilling to provide care for patients in intensive care units during the COVID-19 pandemic [8].
Willingness refers to “an individual’s openness to opportunity” [9] (p. 896) and is the most influential predictor of individuals performing a specific behavior [10]. The willingness of nurses and physicians to work refers to their intention or wanting to provide care for patients during the pandemic [8]. We acknowledge that facility surge capacity and the unavailability of needed supplies have complicated healthcare professionals’ work experiences, optimism, rates of burnout, and other aspects of pandemic care; however, the healthcare personnel’s willingness to work can affect public access to healthcare and the quality of the care in a disaster [11]. Thus, it is necessary to understand the willingness of healthcare personnel to engage in patient care amid extreme challenges, such as respiratory disease outbreaks, to inform future pandemic planning [12]. To date, there is limited literature on nurses’ and physicians’ willingness to provide patient care during a respiratory disease outbreak.
Researchers have identified several factors associated with healthcare workers’ willingness to work during an influenza pandemic. For example, personal characteristics (e.g., gender and occupation), knowledge and skill-related factors (e.g., clinical knowledge of influenza pandemics, confidence in personal skills, role-specific knowledge, and having pandemic response training), perceived safety factors (e.g., perceived personal safety, awareness of pandemic risk, and knowledge of the peak phase of the influenza emergency), concern for family and loved ones, and personal obligations have affected healthcare workers’ willingness to work during an influenza pandemic [13,14]. Healthcare team members have a duty to provide direct patient care, and therefore are at higher risk of getting infected with a respiratory virus because of the time expended in implementing bedside care [3]. Nurses and physicians provide considerable personal, hands-on patient care. The factors that influence the willingness of nurses and physicians to provide such care may differ from factors that other inter-professional healthcare team members consider important.
There is a critical need to identify barriers and facilitators to nurses’ and physicians’ willingness to work during a disease outbreak. The identification of these factors can help healthcare systems, leaders, stakeholders, and policymakers to address barriers and facilitators in order to support adequate availability of the requisite care during a respiratory disease outbreak [13,15,16]. A literature review identified factors related to healthcare workers’ willingness to work during an influenza pandemic through an analysis of quantitative studies [13]. However, it is valuable to review both qualitative and quantitative studies as it enriches the evidence, which in turn provides broad perspectives and strong rationale for improved decision making [17]. Therefore, we undertook a mixed-method systematic review to provide a rich and highly practical understanding of a complex issue [18]: the willingness of healthcare workers to work during a pandemic. Understanding the factors related to nurses’ and physicians’ willingness to engage in patient care during a respiratory disease outbreak will facilitate the modification of current pandemic workplace practices and may serve to inform future pandemic planning.
2. Materials and Methods
We followed a mixed-methods systematic review procedure that was described by Pluye and Hong [18]. In addition, we used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist [19] and the Enhancing Transparency in Reporting the Synthesis of Qualitative Research Guidance (ENTREQ) [20] to structure reporting and guide the synthesis of study findings.
Prior to conducting the literature search, we searched the International Prospective Register of Systematic Reviews and Cochrane Library for related work on our topic and ascertained that there were no similar systematic reviews. A systematic search of the literature was conducted during April 2021, using the PubMed, Web of Science, CINAHL, and PsycINFO electronic databases. We used specific search strategies because of the differences in the search process across databases. Table S1 lists the search strategies that were undertaken. Key search terms were related to population (i.e., nurse, physician, healthcare worker, healthcare provider), willingness to work (i.e., willingness, willing* and work, report to work, respon* and work), and respiratory disease outbreaks (i.e., pandemic, healthcare disaster, respiratory infectious disease epidemic, and disease outbreak*). The ancestry approach was conducted to identify other articles that met the inclusion criteria and contributed to the aim of this review. The literature searches were conducted in consultation with a medical librarian.
The inclusion criteria for the present review specified studies that: (1) focused on nurses’ and/or physicians’ willingness to work during a respiratory disease outbreak, (2) were original research published in a peer-reviewed scholarly journal, and (3) were published in English. Studies were excluded if they were theoretical, discussion, or review articles or if they focused on non-respiratory diseases, such as Ebola virus.
The PRISMA framework guided the article search and review processes as shown in Figure 1. The initial database search yielded 2021 articles. A manual search identified 3 additional articles. After excluding duplicates, 1585 articles remained. Following title and abstract review by two researchers (HJL and EK) independently, 1416 articles were excluded, as they did not meet the inclusion criteria. A total of 169 articles were included for full-text review, of which 140 articles were excluded. A final sample of 29 studies were included in this review; 8 articles were qualitative studies and 21were quantitative studies.
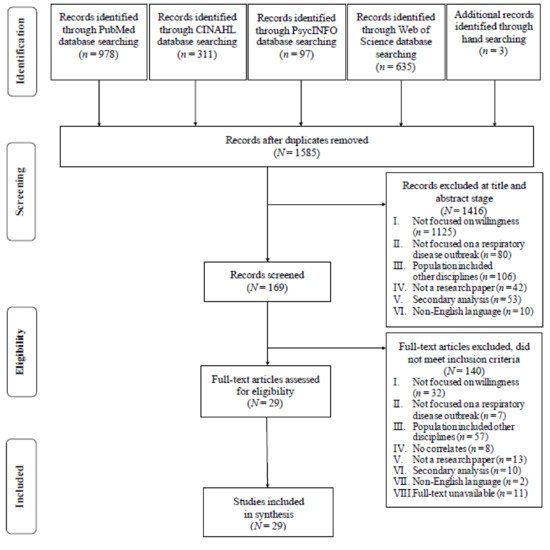
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Flowchart of Article Selection for Analysis.
The quality of the selected articles was appraised using the mixed-method appraisal tool (MMAT), which evaluates the methodological quality of qualitative, quantitative, and mixed-methods studies [21]. Each study was reviewed using MMAT for clarity of the research question and the sufficiency of the collected data to address the research question. Then, according to each study design, the quality of the study was evaluated with five questions that had three possible responses (yes, no, or cannot tell). Using a blinded process, two researchers (HJL and EK) evaluated the quality of each manuscript that was included. When the reviewer ratings were discordant, the reviewers discussed their findings until reaching a consensus on the quality of all articles.
In the data extraction process, one researcher (HJL) extracted data and another researcher (EK) validated the data extraction. Data from the 29 included studies were organized using a matrix of the following characteristics: first author, year of publication, country, type of study, study aim, sample and setting, and main results (Table 1).

Table 1.
Summary of Studies Reviewed.
Data synthesis was based on a sequential explanatory synthesis [18]. To enable this synthesis, results of quantitative studies were pooled in evidence tables based on identified perceived barriers and facilitators of nurses’ and/or physicians’ willingness to work. Findings of qualitative studies were integrated using a qualitative thematic analysis (Table 2). After themes were identified, the theme was compared with the barriers and facilitators identified during quantitative synthesis.
Table 2.
Reciprocal translation table.
3. Results
3.1. Study Characteristics
A total of 29 articles were included in this review: 8 qualitative research articles and 21 quantitative research papers. The included manuscripts were published between 2003 and 2021. As shown in Table 1, studies were conducted in various countries, including Australia (n = 4) [8,22,23,24], Bangladesh (n = 1) [25], Canada (n = 1) [26], China (n = 7) [2,7,27,28,29,30,31], Georgia (n = 1) [32], Hong Kong (n = 1) [33], Nigeria (n = 1) [34], Pakistan (n = 1) [35], Philippines (n = 1) [36], Qatar (n = 1) [37], South Korea (n = 2) [38,39], Taiwan (n = 3) [4,40,41], Turkey (n = 1) [42], USA (n = 3) [5,43,44], and Yemen (n = 1) [15]. Among the 29 studies reviewed, 19 studies included nurses only [4,5,8,22,27,28,29,30,31,33,36,37,38,39,40,41,42,43,44], 6 included physicians only [23,24,25,26,34,35], and 4 included both nurses and physicians [2,7,15,32]. A total of 19 studies were conducted during an outbreak or pandemic, such as the SARS outbreak (n = 2) [4,41], the H1N1 influenza pandemic (n = 3) [5,33,43], the Middle East respiratory syndrome (MERS) outbreak (n = 1) [39], and the COVID-19 pandemic (n = 13) [2,7,8,25,27,28,29,30,31,35,36,37,42]. One study was conducted to evaluate the high possibility of an avian influenza (AI) outbreak [40]. The other studies were conducted using hypothetical influenza pandemic scenarios. One study [33] was conducted in a community setting, whereas the others were conducted in the hospital setting. MMAT ratings were higher than 80% for most of the studies reviewed. No study was excluded based on the quality rating. Table S2 displays the MMAT ratings for all included studies.
3.2. Summary of Evidence
We integrated the findings of the reviewed studies using the Integrated Behavioral Model (IBM), which is a theoretical construct that presenting how individual motivational factors affect the willingness to perform a specific behavior [10]. In this review, we summarized the perceived barriers and facilitators of nurses’ and/or physicians’ willingness to work in seven categories adopted from the IBM: demographics, attitude, perceived norm, personal agency, knowledge and skills to perform the behavior, environmental constraints, and habit (Figure 2). The attitude represented instrumental attitude, which is determined by beliefs about the outcomes of the behavior. Perceived norms include social identity, which is the social pressure one feels to perform or not perform a particular behavior. In this review, social responsibility and professionalism, which includes putting the patient’s interests ahead of their own [38], are perceived as societal norms among healthcare workers. Personal agency refers to an individual’s capability to perform a behavior for given purposes, which comprises self-efficacy and perceived control over behavioral performance. Knowledge and skills to perform the behavior included respiratory disease outbreak-response training. Environmental constraints refer to physical constraints that hinder a behavior. In this review, we divided environmental constraints into physical constraints and emotional constraints in a respiratory disease outbreak situation. Lastly, when the behavior is habitual and the person has previously performed such behavior, that particular behavior is more likely to occur [10]. This review replaced habit with the past experience of participants.
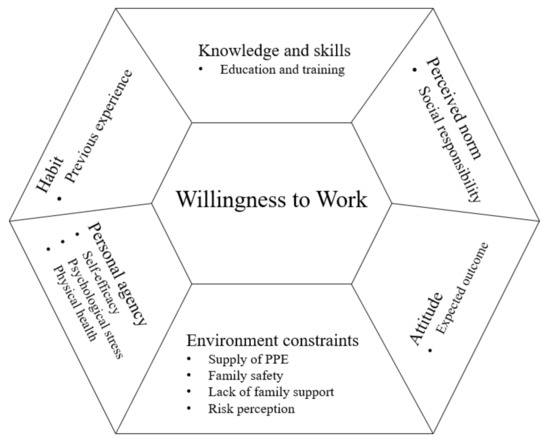
Figure 2.
Barriers and Facilitators of Nurses and Physicians’ Willingness to Work During a Respiratory Disease Outbreak.
3.2.1. Demographics
Gender, age, professional experience, education level, occupation, and participating in religious activities influenced nurses’ and physicians’ willingness to work during a respiratory disease outbreak. Three research teams concluded that, compared with women, men were more likely to be willing to work if an influenza pandemic occurred [25,26,34]. Research teams evaluated findings related to chronological age. The younger that the physicians were, the more willing they were to work during the COVID-19 pandemic [25]. Similarly, nurses who were older than 40 years were less willing to work compared with nurses aged 20–29 years [28]. In terms of the duration of professional experience, nurses who had worked for 11–15 years were less willing to participate in frontline pandemic work than nurses with 21 or more years of experience [31]. The findings of another research study supported the finding that senior nurses were more likely to report willingness to combat COVID-19 at the professional frontline [28]. Nurses with higher levels of education were more willing to work during the pandemic [29]. When analyzed by occupation, nurses were less willing to work than physicians in case of a hypothetical influenza pandemic [32]. Among physicians-in-training and more senior physicians, those who were no longer in training reported greater unwillingness to work during the COVID-19 pandemic [25]. In addition, regardless of the religion practiced, nurses who engaged in religious activities were more likely to be willing to work during a possible avian flu pandemic [40].
3.2.2. Attitude
Nurses’ and physicians’ willingness to work was affected by the expected outcomes of providing care during a respiratory disease outbreak, such as infection, overwork (e.g., workload inequities, care assignments with mismatched needs and resources available, or exploitation), quarantine, and incentives. Researchers determined that nurses hesitated to participate in caring for patients suffering from MERS due to fear of infection [39]. During the H1N1 influenza pandemic, community nurses who were more fearful of infection reported greater unwillingness to work [33]. Similarly, general practitioners were hesitant to care for patients during a possible pandemic as they prioritized family safety and did not want to carry a virus to their families [23]. The nurses who thought COVID-19 affected their workload had a lower level of willingness to work [29]. Moreover, nurses’ willingness to work significantly decreased when there was a need to quarantine during and after providing care for patients infected with respiratory viruses [4,5,41].
A research team that studied the impact of incentives on willingness concluded that when double wages were provided, when accommodation was provided, and when vaccines and medicines were provided, not only to nurses themselves but also to their families, the willingness of nurses to work decreased [43]. In contrast, the nurse participant of one study stated that she would not participate in the next outbreak because she was not adequately compensated after taking care of patients with MERS [39]. General practitioners who were not currently in clinical practice stated that professional risk and liability played an important role in their willingness to provide care during a possible influenza pandemic [24].
3.2.3. Perceived Norm
Eleven studies identified social responsibility as a facilitator of nurses’ and physicians’ willingness to work [2,23,24,27,29,30,36,38,39,42,44]. Nurses with higher scores of social responsibility were more likely to report their willingness to work if a respiratory outbreak occurred [38,44]. Nurses and physicians have been reported to have a strong sense of responsibility to care for patients infected during a pandemic [2,39]. Furthermore, the physicians believed that refusal to work during a pandemic was an abandonment of their responsibilities to both their patients and colleagues [23,24]. Some nurses learned about the difficulties that healthcare workers and patients were experiencing during the COVID-19 pandemic from news broadcasts and social media, which was antecedent to their decision to volunteer to support the COVID-19 care sites to extend help [27].
3.2.4. Personal Agency
Nurses and physicians with high self-efficacy were more likely to work during an influenza pandemic [15]. Those who were confident in their knowledge of the risks of COVID-19 and how to protect themselves and their patients from infection reported that they would care for COVID-19 patients [7,25,31,37].
Stress and other psychological issues that nurses experienced during a respiratory disease outbreak reduced the nurses’ willingness to work [28,29,33,38]. Multiple research teams have determined an inverse relationship between high levels of stress among nurses and willingness to work during an outbreak [33,38]. The nurses who felt anxious and depressed during the COVID-19 outbreak reported a lower level of intention to respond to calls for work during subsequent waves of COVID-19 [28,29]. Moreover, the perceived physical health of nurses influenced their willingness to work. Nurses who felt energetic and spirited or in stable conditions of health were more likely to volunteer to work in the COVID-19 medical sites [28].
3.2.5. Knowledge and Skills to Perform the Behavior
Training to improve knowledge and skills that nurses and physicians can use to address patient needs with a disease outbreak was associated with their willingness to work. For example, after providing a 4 h online and a 4-day field training about the influenza pandemic for nurses, the confidence and willingness of nurses to work during a pandemic significantly increased [22]. Psychiatrists and nurses who completed a training program had a greater likelihood of accepting an assignment that included infected patients [7]. Having protective equipment training had a positive effect on nurses’ intention to respond during the COVID-19 pandemic [28,29]. Nurses in intensive care units (ICUs) who perceived that they received enough information from the organization regarding SARS-CoV-2 transmission, restrictions due to the risks of COVID-19, use of personal protective equipment (PPE), availability of relevant education, and access to mental health services were more willing to provide nursing care during the pandemic [8]. The ICU nurses’ intention to work was unassociated with the actual preparedness of the ICU to manage COVID-19 surges [8]. Nurses who perceived that they were well-prepared against emergency situations such as the COVID-19 pandemic reported a high level of intention to work [29]. When physicians noted inadequate training regarding care of COVID-19 patients, they were more reluctant to treat patients with the illness [35].
3.2.6. Environmental Constraints
The availability of adequate PPE (e.g., masks, disposable gowns, and gloves) was identified as an important factor in willingness to work. For instance, inadequate supply of PPE prevented nurses and physicians from being willing to work during respiratory disease outbreaks [5,23,24,35,40,43]. General practitioners stated that they would stop working in an expected pandemic if PPE was unavailable [24]. However, some general practitioners stated that they would work regardless of whether PPE was provided adequately [24]. When nurses agreed with infection control principles, they were more likely to report to work during an outbreak [4,41]. Similarly, physicians who believed that using PPE would keep healthcare workers safe from getting COVID-19 tended to have greater willingness to work [25].
Nurses having family at risk for illness or death were less likely to work in an influenza pandemic [5,43]. Emergency nurses with children in the home [44] and female physicians who needed to care for family [26] were significantly less likely to report to work during an expected outbreak. Furthermore, physicians who had an elderly relative at home expressed their reluctance to treat COVID-19 patients [35]. Similarly, worries about family care and lack of family support were barriers affecting nurses’ willingness to work during the COVID-19 pandemic [31]. Nurses reported increased willingness to volunteer to work in the COVID-19 pandemic when their families had a supportive attitude toward working in the COVID-19 medical sites [28].
Fear about an outbreak was negatively associated with nurses’ willingness to work during a threatened outbreak [40], and increased worry among nurses about an outbreak was related to a decreased likelihood of reporting to work [44]. Furthermore, frightening news reports about a pandemic as well as a hypothetical situation where a 30-year-old healthcare colleague died from workplace disease exposure reduced nurses’ willingness to work [5,43]. In contrast, low self-perceived risk of a SARS-CoV-2 infection in the workplace was a predictor of nurses’ and physicians’ willingness to work during the COVID-19 pandemic [25,31].
3.2.7. Habit
The lived experience of caring for patients who were infected or suspected of being infected with the pathogen implicated in an outbreak positively affected the willingness of nurses and physicians to work. Five studies determined that prior experience in caring for patients infected or suspected of being infected during a respiratory disease outbreak was positively associated with willingness to work in the same or a similar future outbreak [7,15,29,38,39]. Past experiences increased the confidence of working during an outbreak, which in turn increased the willingness to work [39]. However, one research team determined that physicians who treated confirmed or suspected COVID-19 patients had less willingness to continue their work during the COVID-19 pandemic, whereas physicians who had the experience of treating patients during previous pandemics (e.g., H5N1 or H1N1) had greater willingness to work with COVID-19 patients [25].
4. Discussion
This mixed-methods systematic review identified barriers and facilitators that influence the willingness of nurses and physicians to work during a respiratory disease outbreak. Key barriers included attitude toward expected negative outcomes resulting from working during the outbreak; environmental constraints, including inadequate supply of PPE; concern of family; and perceived risk. Key facilitators were perceived norms (e.g., social responsibility or duty as nurses and physicians); personal agency, including self-efficacy, knowledge, and skills improved through training; and habits influenced by previous experiences.
The perceived norm, a duty as nurses and physicians, was an important role in their willingness to sacrifice themselves in a respiratory disease outbreak. However, their duty was grounded in a reciprocity for their acceptance of greater risk for the public good [45]. For example, nurses and physicians who provide direct care to infected patients should be prioritized in the allocation of scarce medical resources such as PPE during the COVID-19 pandemic [46]. In the same line with reciprocity, the environmental constraints were major barriers of willingness to work in a respiratory disease outbreak. In addition, nurses’ and physicians’ attitudes toward the negative expected outcomes of providing care during a respiratory disease outbreak, including infection and quarantine, decreased their willingness to work. In order to facilitate nurses’ and physicians’ willingness to work in an outbreak, it is essential to support their safety and their ability to protect themselves from infection. For a safe workplace, provision of adequate PPE is essential. The British Medical Association, Canadian Nurses Association Code of Ethics, and Royal College of Nursing highlight the reciprocal duty of employers and governments to protect nurses and physicians by providing necessary and sufficient protective equipment and supplies during disasters, outbreaks, and pandemics to minimize the healthcare workers’ risk of infection [47,48,49]. Recently during the COVID-19 pandemic, there was a global lack of adequate PPE for frontline healthcare workers [50]. In March 2020 (in the early days of the COVID-19 pandemic), there was a massive personnel recruitment in the National Health System in the UK due to concerns that physicians would quit their jobs due to fear of inadequate supplies of PPE [51]. The supply and management of adequate PPE is a task for the government and not one for individual facilities or workers because the antecedent of most PPE shortages during the COVID-19 pandemic was mainly due to insufficient stockpiles and limited manufacturing capacity [52]. For example, after a SARS outbreak, the government of Taiwan developed a stockpiling system of PPE that could maintain a minimum stockpile for addressing the surge in demand for PPE in the early stages of a pandemic [53], and this strategy was helpful in coping with the COVID-19 pandemic [54]. The South Korean government took several steps to actively resolve the shortage of PPE in healthcare settings and the community. The government purchased 80% of the masks from domestic manufacturers, banned exports of PPE, and limited the price of masks and the amount of masks that an individual could buy every week [55]. India, which relied on imports for the supply of PPE, started producing and manufacturing PPE with various government institutes and some private manufacturers, given the poor quality of imported PPE [56]. National agencies are encouraged to check and improve the government stockpiling and manufacturing system with regard to PPE based on the lessons learned from the ongoing COVID-19 pandemic. A proactive approach will support worker safety and reduce the situational constraints that hinder willingness to work.
In addition, this review identified that training to cope with an outbreak facilitated willingness to work during a respiratory disease outbreak. Providing nurses and physicians not only with adequate PPE but also with sufficient information and resources may help alleviate fears related to working during a disease outbreak. Furthermore, the training increased the confidence of nurses and physicians to work in the COVID-19 pandemic situation, which positively affected their willingness to work [7]. In this review, confidence and self-efficacy as a personal agency facilitated their willingness to work. In a study in Australia, field and online training increased nurses’ willingness to work in the outbreak, as did knowledge about how to deal with an outbreak situation [22]. According to a review on implementing disaster and pandemic training programs for medical students, a program including 1-day training improved disaster and pandemic preparedness, attitude toward working in disaster and pandemic situations, and knowledge and skills [57]. In addition, a 1 h computer-based simulation training enhanced nurses’ self-efficacy and working skill in a disaster [58]. Simulation-based training is increasingly used in disaster management not only to educate caregivers with the required knowledge and skills but also to give them experience in handling a disaster situation, which is one of facilitators of nurses’ and physicians’ willingness to work [58]. In pandemics, there can be a lack of training about the specific infection and PPE best practices for healthcare workers, and some trainings may not be mandatory [59]. We suggest that organizations provide an outbreak-specific simulation training for nurses and physicians to improve their outbreak situation-related knowledge, skills, and confidence, which will support their willingness to work. Such trainings provide important information and serve as a reliable source of knowledge during a time when myths and rumors may be prevalent, and therefore participation in such trainings should be obligatory.
Most of the studies we reviewed had several limitations. First, the studies including both nurses and physicians did not explore the differences among the two groups of professionals. Occupation or role-related barriers and facilitators of willingness to work during a pandemic should be determined to develop an effective workforce strategy. Second, most of the studies that were analyzed in this review used quantitative methodology. However, willingness is an individual perception that is influenced by various factors [9]; therefore, it may be best to explore this concept with mixed-methods or fully qualitative work. The qualitative studies enriched the evidence that professional responsibility facilitated a willingness to work. Finally, there is insufficient evidence to report with confidence that researchers have obtained a comprehensive understanding of the various barriers and facilitators of willingness to work in a pandemic situation. For example, in this review, the results of qualitative and quantitative studies on the impact of rewards were inconsistent and limited, which makes it difficult to describe the influence of a reward on the willingness to work during an outbreak. To determine best practices for compensation and support for working during a pandemic, we suggest the need for additional research on how and what type of compensation affects the willingness to work in a respiratory infectious disease outbreak. Such research should be approached from the perspective that fair work deserves fair pay and that the increase in stress, workload, and responsibility during a pandemic undoubtedly warrants additional compensation.
There are several limitations of this review. As the literature search was limited to records published in English, we may have missed important and relevant studies published in other languages. This review included studies with low MMAT quality scores. However, the results were derived by synthesizing and analyzing results across 29 studies, most of which had quality ratings of 80% or higher. Although this review included studies conducted during an actual respiratory disease outbreak situation and those conducted with hypothetical prompts, we did not analyze situation-related influencing factors. Additionally, there are different healthcare systems in each country according to their socio-economic situation. For example, government healthcare support and spending, as well as individual or family funds available to support health needs, vary between OECD and non-OECD nations; the funding models are one source of disparity that impacts health indicators such as life expectancy and infant mortality [60]. The nature of the different healthcare systems may affect nurses’ and physicians’ willingness to work. However, this review did not consider differences among the healthcare systems. Therefore, in order to develop more specific interventions, we suggest that future studies consider health system differences between countries along with the factors that influence willingness to work, whether such studies are conducted in the context of an actual outbreak situation or a hypothetical situation. Nevertheless, this review broadens the understanding of perceived facilitators and barriers for willingness to work among nurses and physicians in a respiratory disease outbreak.
5. Conclusions
This review provides an understanding of the barriers and facilitators affecting nurses’ and physicians’ willingness to work during a respiratory disease outbreak. Individual workers across different health systems and settings will have variability in the resources afforded them to carry out healthcare, and they will approach care with differing professional lived experiences. Regardless of the evidence-based policies and programming on the willingness to work that are studied and implemented, it is important to respect and respond to nurses’ and physicians’ concerns about their safety and preparedness when providing care during a respiratory disease outbreak. The environmental constraints that could harm the health of nurses and physicians and concerns regarding family wellbeing had a negative impact on the willingness to work. Factors that have a positive effect on the willingness to work include a sense of social responsibility and self-efficacy in terms of adequate knowledge and skills needed to provide care for patients during an outbreak. Establishing a working environment that is safe from infection by facilitating the consistent availability of proper PPE is a prerequisite for supporting worker well-being and willingness to work. Even in usual non-pandemic situations, education and training for nurses and physicians should be regularly implemented in preparation for an unexpected respiratory disease outbreak.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/ijerph18136841/s1, Table S1: Literature search strategy, Table S2: Mixed Method Appraisal Tool (MMAT) in selected studies (N = 29).
Author Contributions
Conceptualization, H.J.L.; methodology, H.J.L. and E.K.; validation, H.J.L. and E.K.; formal analysis, H.J.L.; data curation, H.J.L.; writing—original draft preparation, H.J.L. and E.K.; writing—review and editing, S.E.L. and B.L.M.; visualization, H.J.L.; supervision, S.E.L.; project administration, S.E.L.; funding acquisition, S.E.L. and H.J.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Faculty-Student Research Grant 2020 [6-2020-0049] from Yonsei University College of Nursing.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Kaji, A.; Koenig, K.L.; Bey, T. Surge Capacity for Healthcare Systems: A Conceptual Framework. Acad. Emerg. Med. 2006, 13, 1157–1159. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Zhu, J.; Stone, T.; Petrini, M. The ethics of refusing to care for patients during the coronavirus pandemic: A Chinese perspective. Nurs. Inq. 2021, 28, 12380. [Google Scholar] [CrossRef]
- Tzeng, H.-M. SARS infection control in Taiwan: Investigation of nurses’ professional obligation. Outcomes Manag. 2003, 7, 186–193. [Google Scholar]
- Martin, S.D. Nurses’ ability and willingness to work during pandemic flu. J. Nurs. Manag. 2010, 19, 98–108. [Google Scholar] [CrossRef] [PubMed]
- McQuoid-Mason, D.J. COVID-19: What should employers do if employed health professionals such as doctors and nurses refuse to treat COVID-19 patients despite being provided with the required personal protective equipment? S. Afr. J. Bioeth. Law 2020, 13, 87. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, J.; Yang, Y.; Wang, Z.; Wang, G.; Hashimoto, K.; Zhang, K.; Liu, H. Knowledge and attitudes of medical staff in Chinese psychiatric hospitals regarding COVID-19. Brain Behav. Immun. Health 2020, 4, 100064. [Google Scholar] [CrossRef]
- Lord, H.; Loveday, C.; Moxham, L.; Fernandez, R. Effective communication is key to intensive care nurses’ willingness to provide nursing care amidst the COVID-19 pandemic. Intensiv. Crit. Care Nurs. 2021, 62, 102946. [Google Scholar] [CrossRef]
- Pomery, E.A.; Gibbons, F.X.; Reis-Bergan, M.; Gerrard, M. From Willingness to Intention: Experience Moderates the Shift from Reactive to Reasoned Behavior. Pers. Soc. Psychol. Bull. 2009, 35, 894–908. [Google Scholar] [CrossRef]
- Montaño, D.E.; Kasprzyk, D. Theory of reasoned action, theory of planned behavior, and the integrated behavioral model. In Health Behavior: Theory, Research and Practice, 5th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass/Wiley: San Francisco, CA, USA, 2015; pp. 95–124. [Google Scholar]
- Chaffee, M. Willingness of Health Care Personnel to Work in a Disaster: An Integrative Review of the Literature. Disaster Med. Public Health Prep. 2009, 3, 42–56. [Google Scholar] [CrossRef]
- Ives, J.; Greenfield, S.; Parry, J.M.; Draper, H.; Gratus, C.; Petts, J.I.; Sorell, T.; Wilson, S. Healthcare workers’ attitudes to working during pandemic influenza: A qualitative study. BMC Public Health 2009, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Aoyagi, Y.; Beck, C.R.; Dingwall, R.; Nguyen-Van-Tam, J.S. Healthcare workers’ willingness to work during an influenza pandemic: A systematic review and meta-analysis. Influenza Other Respir. Viruses 2015, 9, 120–130. [Google Scholar] [CrossRef]
- Devnani, M. Factors Associated with the Willingness of Health Care Personnel to Work During an Influenza Public Health Emergency: An Integrative Review. Prehospital Disaster Med. 2012, 27, 551–566. [Google Scholar] [CrossRef]
- Al-Hunaishi, W.; Hoe, V.C.; Chinna, K. Factors associated with healthcare workers willingness to participate in disasters: A cross-sectional study in Sana’a, Yemen. BMJ Open 2019, 9, e030547. [Google Scholar] [CrossRef] [PubMed]
- Seale, H.; Leask, J.; Po, K.; MacIntyre, C.R. “Will they just pack up and leave?”—Attitudes and intended behaviour of hospital health care workers during an influenza pandemic. BMC Health Serv. Res. 2009, 9, 30. [Google Scholar] [CrossRef] [PubMed]
- Newman, T.B. The power of stories over statistics. BMJ 2003, 327, 1424–1427. [Google Scholar] [CrossRef]
- Pluye, P.; Hong, Q.N. Combining the Power of Stories and the Power of Numbers: Mixed Methods Research and Mixed Studies Reviews. Annu. Rev. Public Health 2014, 35, 29–45. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Hope, K.; Massey, P.D.; Osbourn, M.; Durrheim, D.N.; Kewley, C.D.; Turner, C. Senior Clinical Nurses Effectively Contribute to the Pandemic Influenza Public Health Response. Aust. J. Adv. Nurs. 2011, 28, 47–53. [Google Scholar]
- Anikeeva, O.; Braunack-Mayer, A.; Street, J. How will Australian general practitioners respond to an influenza pandemic? A qualitative study of ethical values. Med. J. Aust. 2008, 189, 148–150. [Google Scholar] [CrossRef] [PubMed]
- Shaw, K.A.; Chilcott, A.; Hansen, E.; Winzenberg, T. The GP’s response to pandemic influenza: A qualitative study. Fam. Pract. 2006, 23, 267–272. [Google Scholar] [CrossRef]
- Rafi, A.; Hasan, M.T.; Azad, D.T.; Alam, S.F.; Podder, V.; Hossain, S.; Akther, S.M.Q.; Ashraf, F.; Hossain, G. Willingness to work during initial lockdown due to COVID-19 pandemic: Study based on an online survey among physicians of Bangladesh. PLoS ONE 2021, 16, e0245885. [Google Scholar] [CrossRef]
- Dickinson, J.A.; Bani-Adam, G.; Williamson, T.; Berzins, S.; Pearce, C.; Ricketson, L.; Medd, E. Alberta family physicians’ willingness to work during an influenza pandemic: A cross-sectional study. Asia Pac. Fam. Med. 2013, 12, 3. [Google Scholar] [CrossRef]
- Cui, S.; Zhang, L.; Yan, H.; Shi, Q.; Jiang, Y.; Wang, Q.; Chu, J. Experiences and Psychological Adjustments of Nurses Who Voluntarily Supported COVID-19 Patients in Hubei Province, China. Psychol. Res. Behav. Manag. 2020, 13, 1135–1145. [Google Scholar] [CrossRef]
- Gan, X.; Shi, Z.; Chair, S.Y.; Cao, X.; Wang, Q. Willingness of Chinese nurses to practice in Hubei combating the coronavirus disease 2019 epidemic: A cross-sectional study. J. Adv. Nurs. 2020, 76, 1250–2137. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, P.; Chen, J.; Ruan, L.; Zeng, Q.; Gong, Y. Intention to response, emergency preparedness and intention to leave among nurses during COVID-19. Nurs. Open 2020, 7, 1867–1875. [Google Scholar] [CrossRef]
- Liu, Y.; Bd, Z.Z.; Han, Y.; Liu, Y.; Liu, F.; Hu, D. Experiences of front-line nurses combating coronavirus disease-2019 in China: A qualitative analysis. Public Health Nurs. 2020, 37, 757–763. [Google Scholar] [CrossRef]
- Luo, Y.; Feng, X.; Zheng, M.; Zhang, D.; Xiao, H.; Li, N. Willingness to participate in front-line work during the COVID-19 pandemic: A cross-sectional study of nurses from a province in South-West China. J. Nurs. Manag. 2021. [Google Scholar] [CrossRef]
- Butsashvili, M.; Triner, W.; Kamkamidze, G.; Kajaia, M.; McNutt, L.-A. Knowledge and anticipated behavior of health care workers in response to an outbreak of pandemic influenza in Georgia. J. Infect. Dev. Ctries. 2007, 1, 329–332. [Google Scholar] [CrossRef]
- Wong, E.L.Y.; Wong, S.Y.S.; Kung, K.; Cheung, A.W.L.; Gao, T.T.; Griffiths, S.M. Will the community nurse continue to function during H1N1 influenza pandemic: A cross-sectional study of Hong Kong community nurses? BMC Health Serv. Res. 2010, 10, 107. [Google Scholar] [CrossRef]
- Adam, V.Y.; Okukpon, P.O. Human pandemic influenza: An assessment of the knowledge, attitudes and prevention practices of doctors in a tertiary health facility in Southern Nigeria. Niger. Postgrad. Med. J. 2014, 21, 235–240. [Google Scholar]
- Ayub, M.; Arshad, D.; Maqbool, N.; Zahid, M.; Malik, R.S.; Rizvi, Z.A.; Arshad, U.; Khan, S.U. Physicians’ Attitudes Towards Treating Patients in the Context of COVID-19 Pandemic in Pakistan. Cureus 2020, 12, 10331. [Google Scholar] [CrossRef] [PubMed]
- Sadang, J.M. The Lived Experience of Filipino Nurses’ Work in COVID-19 Quarantine Facilities: A Descriptive Phenomenological Study. Pac. Rim Int. J. Nurs. Res. 2021, 25, 154–164. [Google Scholar]
- Nashwan, A.J.; Abujaber, A.A.; Mohamed, A.S.; Villar, R.C.; Al-Jabry, M.M. Nurses’ willingness to work with COVID-19 patients: The role of knowledge and attitude. Nurs. Open 2021, 8, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Oh, N.; Hong, N.; Ryu, D.H.; Bae, S.G.; Kam, S.; Kim, K.-Y. Exploring Nursing Intention, Stress, and Professionalism in Response to Infectious Disease Emergencies: The Experience of Local Public Hospital Nurses During the 2015 MERS Outbreak in South Korea. Asian Nurs. Res. 2017, 11, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y. Nurses’ experiences of care for patients with Middle East respiratory syndrome-coronavirus in South Korea. Am. J. Infect. Control 2018, 46, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, H.-M.; Yin, C.-Y. Nurses’ Fears and Professional Obligations Concerning Possible Human-to-Human Avian Flu. Nurs. Ethics 2006, 13, 455–470. [Google Scholar] [CrossRef]
- Tzeng, H.-M. Nurses’ Professional Care Obligation and Their Attitudes Towards SARS Infection Control Measures in Taiwan During and After the 2003 Epidemic. Nurs. Ethics 2004, 11, 277–289. [Google Scholar] [CrossRef]
- Şimşek, D.C.; Günay, U. Experiences of nurses who have children when caring for COVID-19 patients. Int. Nurs. Rev. 2021, 68, 219–227. [Google Scholar] [CrossRef]
- Martin, S.D.; Brown, L.; Reid, W.M. Predictors of Nurses’ Intentions to Work During the 2009 Influenza A (H1N1) Pandemic. Am. J. Nurs. 2013, 113, 24–31. [Google Scholar] [CrossRef]
- Bell, M.A.; Dake, J.A.; Price, J.H.; Jordan, T.R.; Rega, P. A National Survey of Emergency Nurses and Avian Influenza Threat. J. Emerg. Nurs. 2014, 40, 212–217. [Google Scholar] [CrossRef]
- McGuire, A.L.; Aulisio, M.P.; Davis, F.D.; Erwin, C.; Harter, T.D.; Jagsi, R.; Klitzman, R.; Macauley, R.; Racine, E.; Wolf, S.M.; et al. Ethical Challenges Arising in the COVID-19 Pandemic: An Overview from the Association of Bioethics Program Directors (ABPD) Task Force. Am. J. Bioeth. 2020, 20, 15–27. [Google Scholar] [CrossRef]
- Aulisio, M.P.; May, T. Why healthcare workers ought to be Prioritized in ASMR during the SARS-CoV-2 pandemic. Am. J. Bioeth. 2020, 20, 125–128. [Google Scholar] [CrossRef]
- British Medical Association. COVID-19: Refusing to Treat Where PPE Is Inadequate. 2020. Available online: https://www.bma.org.uk/advice-and-support/covid-19/ppe/covid-19-refusing-to-treat-where-ppe-is-inadequate#:~:text=You%20are%20under%20no%20obligation,way%20of%20delivering%20the%20care (accessed on 28 May 2021).
- Royal College of Nursing. Guidance for Members: Refusal to Treat due to Lack of Adequate PPE During the Pandemic. 2020. Available online: https://www.rcn.org.uk/professional-development/publications/rcn-refusal-to-treat-covid-19-uk-pub-009231 (accessed on 28 May 2021).
- Wright, D.; Peterson, W.; Gifford, W.; Canadian Nurses Association. Nurses’ Ethical Considerations During a Pandemic. 2020. Available online: https://cna-aiic.ca/-/media/cna/covid-19/nurses-ethical-considerations-during-a-pandemic_e.pdf (accessed on 28 May 2021).
- Ranney, M.L.; Griffeth, V.; Jha, A.K. Critical Supply Shortages—The Need for Ventilators and Personal Protective Equipment during the Covid-19 Pandemic. N. Engl. J. Med. 2020, 382, e41. [Google Scholar] [CrossRef]
- Campbell, D.; Stewart, H. Doctors Threaten to Quit NHS Over Shortage of Protective Kit. The Guardian, 24 March 2020. Available online: https://www.theguardian.com/world/2020/mar/24/doctors-threaten-to-quit-over-protective-equipment-shortage (accessed on 28 May 2021).
- Ernst & Young. International Benchmark Survey of COVID-19 Crisis Management. 2020. Available online: https://assets.ey.com/content/dam/ey-sites/ey-com/fr_fr/topics/health/ey-international-benchmark-crisis-management-en.pdf?download (accessed on 28 May 2021).
- Chen, Y.-J.; Chiang, P.-J.; Cheng, Y.-H.; Huang, C.-W.; Kao, H.-Y.; Chang, C.-K.; Huang, H.-M.; Liu, P.-Y.; Wang, J.-H.; Chih, Y.-C.; et al. Stockpile Model of Personal Protective Equipment in Taiwan. Health Secur. 2017, 15, 170–174. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Hossain, M.; Singh, A. Addressing the shortage of personal protective equipment during the COVID-19 pandemic in India-A public health perspective. AIMS Public Health 2020, 7, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; An, J.A.-R.; Min, P.-K.; Bitton, A.; Gawande, A.A. How South Korea Responded to the Covid-19 Outbreak in Daegu. NEJM Catal. 2020, 1. [Google Scholar] [CrossRef]
- Gauttam, P.; Patel, N.; Singh, B.; Kaur, J.; Chattu, V.; Jakovljevic, M. Public Health Policy of India and COVID-19: Diagnosis and Prognosis of the Combating Response. Sustainability 2021, 13, 3415. [Google Scholar] [CrossRef]
- Ashcroft, J.; Byrne, M.H.V.; Brennan, P.A.; Davies, R.J. Preparing medical students for a pandemic: A systematic review of student disaster training programmes. Postgrad. Med. J. 2021, 97, 368–379. [Google Scholar] [CrossRef]
- Jonson, C.-O.; Pettersson, J.; Rybing, J.; Nilsson, H.; Prytz, E. Short simulation exercises to improve emergency department nurses’ self-efficacy for initial disaster management: Controlled before and after study. Nurse Educ. Today 2017, 55, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Houghton, C.; Meskell, P.; Delaney, H.; Smalle, M.; Glenton, C.; Booth, A.; Chan, X.H.S.; Devane, D.; Biesty, L.M. Barriers and facilitators to healthcare workers’ adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: A rapid qualitative evidence synthesis. Cochrane Database Syst. Rev. 2020, 2020, CD013582. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Sugahara, T.; Timofeyev, Y.; Rancic, N. Predictors of (in)efficiencies of Healthcare Expenditure among the Leading Asian Economies—Comparison of OECD and Non-OECD Nations. Risk Manag. Healthc. Policy 2020, 13, 2261–2280. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).