Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
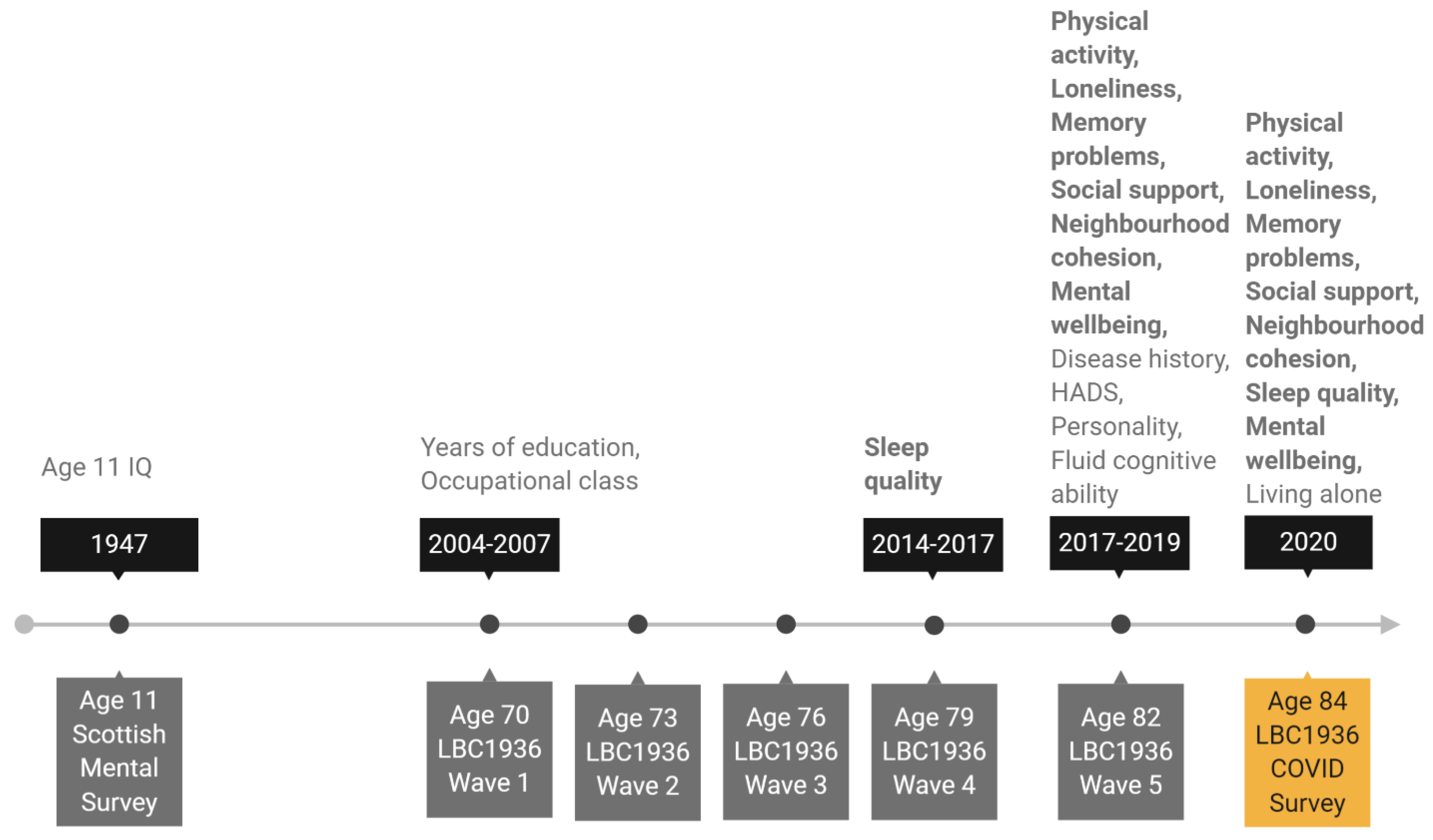
2.2. LBC1936 Study Assessments
2.3. LBC1936 COVID-19 Questionnaire
3. Measures
3.1. Physical Activity and Sleep Quality
3.2. Psychosocial Variables
3.3. Covariates
3.4. Analytical Sample
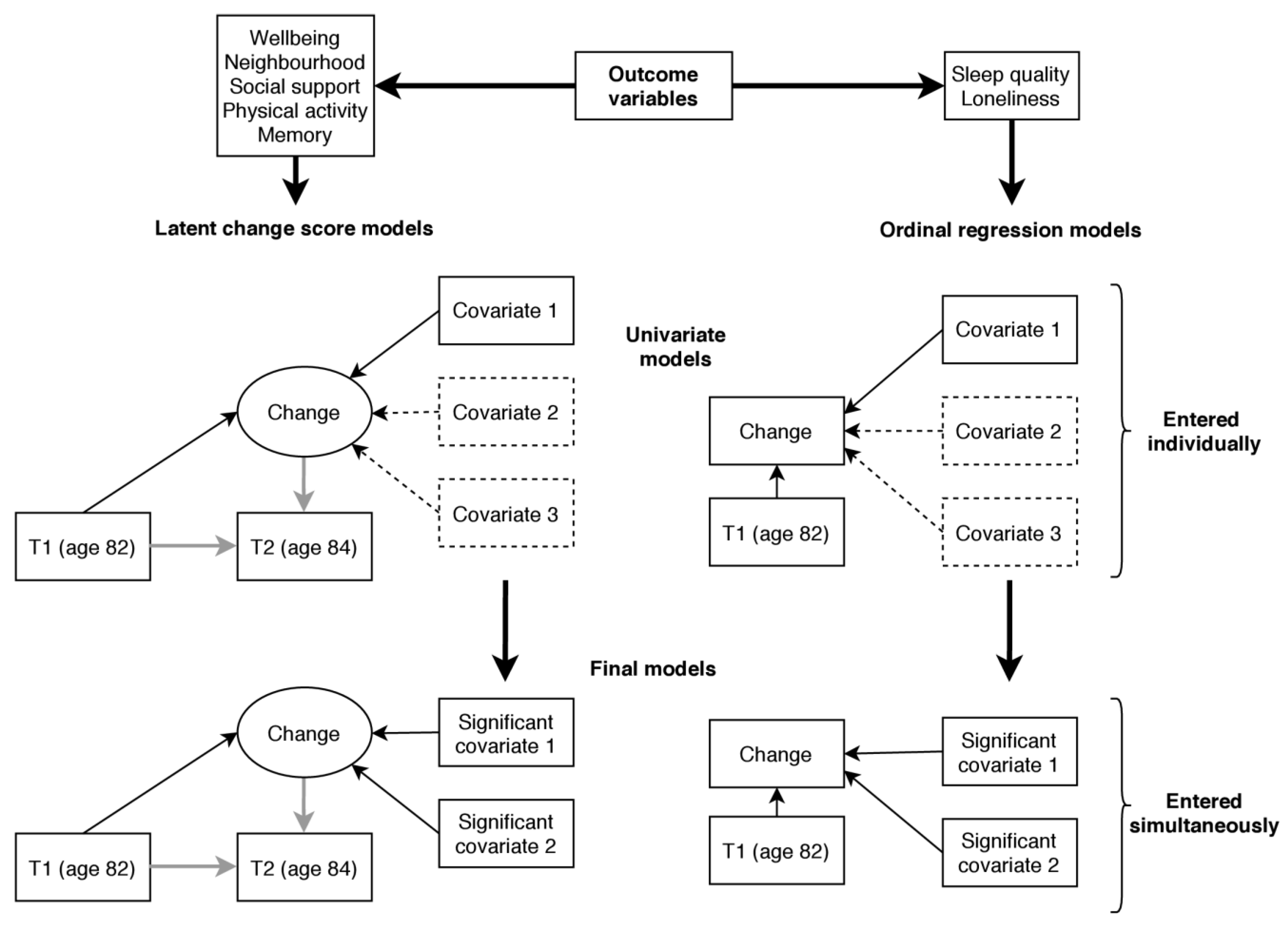
3.5. Analysis
4. Results
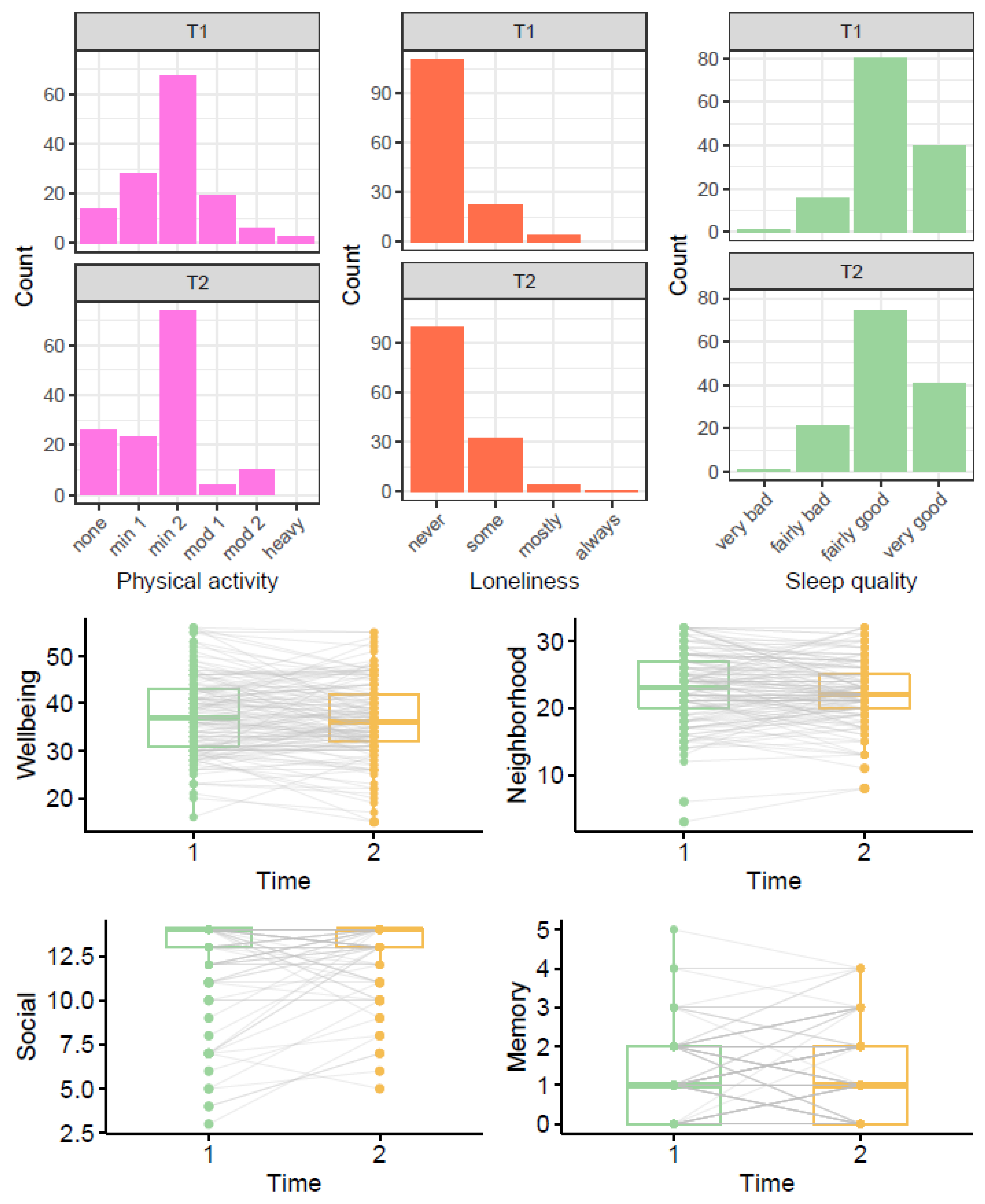
4.1. Descriptive Results
4.2. Correlations between Outcomes
4.3. Predictors of Change
4.4. Subsidiary Analysis
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheval, B.; Sivaramakrishnan, H.; Maltagliati, S.; Fessler, L.; Forestier, C.; Sarrazin, P.; Orsholits, D.; Chalabaev, A.; Sander, D.; Ntoumanis, N. Relationships Between Changes in Self-reported Physical Activity and Sedentary Behaviours and Health during the Coronavirus (COVID-19) Pandemic in France and Switzerland. SportRxiv Prepr. 2020. [Google Scholar] [CrossRef]
- Guan, H.; Okely, A.D.; Aguilar-Farias, N.; del Pozo Cruz, B.; Draper, C.E.; El Hamdouchi, A.; Florindo, A.A.; Jáuregui, A.; Katzmarzyk, P.T.; Kontsevaya, A.; et al. Promoting healthy movement behaviours among children during the COVID-19 pandemic. Lancet Child Adolesc. Health 2020, 4, 416–418. [Google Scholar] [CrossRef]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity, eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef]
- Beck, F.; Leger, D.; Fressard, L.; Peretti-Watel, P.; Verger, P. The Coconel Group. Covid-19 health crisis and lockdown associated with high level of sleep complaints and hypnotic uptake at the population level. J. Sleep Res. 2020, e13119. [Google Scholar] [CrossRef]
- Lee, C.M.; Cadigan, J.M.; Rhew, I.C. Increases in loneliness among young adults during the COVID-19 pan-demic and association with increases in mental health problems. J. Adolesc. Health 2020, 67, 714–717. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Cloonan, S.A.; Taylor, E.C.; Miller, M.A.; Dailey, N.S. Three months of loneliness during the COVID-19 lockdown. Psychiatry Res. 2020, 293, 113392. [Google Scholar] [CrossRef]
- Borkowska, M.; Laurence, J. Coming together or coming apart? Changes in social cohesion during the Covid-19 pandemic in England. Eur. Soc. 2020, 1–19. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Ettman, C.K.; Abdalla, S.M.; Cohen, G.H.; Sampson, L.; Vivier, P.M.; Galea, S. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw. Open 2020, 3, e2019686. [Google Scholar] [CrossRef]
- Tull, M.T.; Edmonds, K.A.; Scamaldo, K.; Richmond, J.R.; Rose, J.P.; Gratz, K.L. Psychological Outcomes Asso-ciated with Stay-at-Home Orders and the Perceived Impact of COVID-19 on Daily Life. Psychiatry Res. 2020, 289, 113098. [Google Scholar] [CrossRef] [PubMed]
- El-Zoghby, S.M.; Soltan, E.M.; Salama, H.M. Impact of the COVID-19 Pandemic on Mental Health and Social Support among Adult Egyptians. J. Community Health 2020, 45, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Sahoo, S.; Mehra, A.; Avasthi, A.; Tripathi, A.; Subramanyan, A.; Pattojoshi, A.; Rao, G.P.; Saha, G.; Mishra, K.K. Psychological impact of COVID-19 lockdown: An online survey from India. Indian J. Psychiatry 2020, 62, 354. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus Disease 2019 (COVID-19): Situation Report—89 (18 April 2020)—World. Available online: https://reliefweb.int/report/world/coronavirus-disease-2019-covid-19-situation-report-89-18-april-2020 (accessed on 3 June 2020).
- Papaioannou, A.G.; Schinke, R.J.; Chang, Y.K.; Kim, Y.H.; Duda, J.L. Physical activity, health and well-being in an imposed social distanced world. Int. J. Sport Exerc. Psychol. 2020, 18, 414–419. [Google Scholar] [CrossRef]
- Webb, L. COVID-19 lockdown: A perfect storm for older people’s mental health. J. Psychiatr. Ment. Health Nurs. 2020. [Google Scholar] [CrossRef]
- Bidzan-Bluma, I.; Bidzan, M.; Jurek, P.; Bidzan, L.; Knietzsch, J.; Stueck, M.; Bidzan, M. A Polish and German Population Study of Quality of Life, Well-Being, and Life Satisfaction in Older Adults during the COVID-19 Pan-demic. Front. Psychiatry 2020, 11, 585813. [Google Scholar] [CrossRef]
- Thorp, A.A.; Owen, N.; Neuhaus, M.; Dunstan, D.W. Sedentary behaviors and subsequent health outcomes in adults: A systematic review of longitudinal studies, 1996–2011. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef]
- Blondell, S.J.; Hammersley-Mather, R.; Veerman, J.L. Does physical activity prevent cognitive decline and de-mentia? A systematic review and meta-analysis of longitudinal studies. BMC Public Health 2014, 14, 510. [Google Scholar] [CrossRef]
- Steptoe, A.; Deaton, A.; Stone, A.A. Subjective wellbeing, health, and ageing. Lancet 2015, 385, 640–648. [Google Scholar] [CrossRef]
- Covassin, N.; Singh, P. Sleep duration and cardiovascular disease risk: Epidemiologic and experimental evi-dence. Sleep Med. Clin. 2016, 11, 81–89. [Google Scholar] [CrossRef]
- Cox, S.R.; Ritchie, S.J.; Allerhand, M.; Hagenaars, S.; Radakovic, R.; Breen, D.P.; Davies, G.; Riha, R.L.; Harris, S.E.; Starr, J.M.; et al. Sleep and cognitive aging in the eighth decade of life. Sleep 2019, 42, zsz019. [Google Scholar] [CrossRef] [PubMed]
- Boss, L.; Kang, D.-H.; Branson, S. Loneliness and cognitive function in the older adult: A systematic review. Int. Psychogeriatr. 2015, 27, 541–553. [Google Scholar] [CrossRef]
- Bu, F.; Steptoe, A.; Fancourt, D. Loneliness during lockdown: Trajectories and predictors during the COVID-19 pandemic in 35,712 adults in the UK. medRxiv 2020. [Google Scholar] [CrossRef]
- Rimfeld, K.; Malancini, M.; Allegrini, A.; Packer, A.E.; McMillan, A.; Ogden, R.; Webster, L.; Shakeshaft, N.G.; Schofield, K.L.; Pingault, J. Genetic correlates of psychological responses to the COVID-19 crisis in young adult twins in Great Britain. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Whatley, M.C.; Siegel, A.L.; Schwartz, S.T.; Silaj, K.M.; Castel, A.D. Younger and Older Adults’ Mood and Ex-pectations Regarding Aging during COVID-19. Gerontol. Geriatr. Med. 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Zacher, H.; Rudolph, C.W. Individual differences and changes in subjective wellbeing during the early stages of the COVID-19 pandemic. Am. Psychol. 2020. [Google Scholar] [CrossRef]
- Van Tilburg, T.G.; Steinmetz, S.; Stolte, E.; van der Roest, H.; de Vries, D.H. Loneliness and mental health dur-ing the COVID-19 pandemic: A study among Dutch older adults. J. Gerontol. Ser. B 2020, gbaa111. [Google Scholar] [CrossRef]
- Golden, J.; Conroy, R.M.; Lawlor, B.A. Social support network structure in older people: Underlying dimensions and association with psychological and physical health. Psychol. Health Med. 2009, 14, 280–290. [Google Scholar] [CrossRef]
- Jean-Pierre, P.; Winters, P.C.; Ahles, T.A.; Antoni, M.; Armstrong, F.D.; Penedo, F.; Lipshultz, S.E.; Miller, T.L.; Fiscella, K. Prevalence of Self-Reported Memory Problems in Adult Cancer Survivors: A National Cross-Sectional Study. J. Oncol. Pract. 2012, 8, 30–34. [Google Scholar] [CrossRef]
- Ha, J.; Pai, M. Subjective Memory Problems and Availability of Emotional Support. Res. Aging 2018, 40, 978–1007. [Google Scholar] [CrossRef]
- Mol, M.; Carpay, M.; Ramakers, I.; Rozendaal, N.; Verhey, F.; Jolles, J. The effect of perceived forgetfulness on quality of life in older adults; a qualitative review. Int. J. Geriatr. Psychiatry 2006, 22, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Scottish Council for Research in Education. The Trend of Scottish Intelligence; University of London Press: London, UK, 1949. [Google Scholar]
- Deary, I.J.; Whiteman, M.C.; Starr, J.M.; Whalley, L.J.; Fox, H.C. The Impact of Childhood Intelligence on Later Life: Following Up the Scottish Mental Surveys of 1932 and 1947. J. Personal. Soc. Psychol. 2004, 86, 130–147. [Google Scholar] [CrossRef] [PubMed]
- Deary, I.J.; Gow, A.J.; Pattie, A.; Starr, J.M. Cohort Profile: The Lothian Birth Cohorts of 1921 and 1936. Int. J. Epidemiol. 2011, 41, 1576–1584. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.M.; Pattie, A.; Deary, I.J. Cohort Profile Update: The Lothian Birth Cohorts of 1921 and 1936. Int. J. Epidemiol. 2018, 47, 1042–1042r. [Google Scholar] [CrossRef] [PubMed]
- Qualtrics, Provo, UT, USA. 2020. Available online: https://www.qualtrics.com (accessed on 3 June 2020).
- Bysse, D.J.; Reynolds, C.F., III; Monk, T.H. The Pittsburgh Sleep Quality Index (PSQI): A new instrument for psychiatric research and practice. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef]
- Grundy, E.; Murphy, M. Marital status and family support for the oldest-old in Great Britain. In Human Longevity, Individual Life Duration, and the Growth of the Oldest-Old Population; Springer: Dordrecht, The Netherlands, 2007; pp. 415–436. [Google Scholar]
- Buckner, J.C. The development of an instrument to measure neighborhood cohesion. Am. J. Community Psychol. 1988, 16, 771–791. [Google Scholar] [CrossRef]
- Office of Population Censuses and Surveys. Classification of Occupations 1980; Her Majesty’s Stationary Office: London, UK, 1980. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Goldberg, L.R. A broad-bandwidth, public domain, personality inventory measuring the lower-level facets of several five-factor models. Personal. Psychol. Eur. 1999, 7, 7–28. [Google Scholar]
- Wechsler, D. WMS-IIIUK Administration and Scoring Manual; Psychological Corporation: London, UK, 1998. [Google Scholar]
- McArdle, J.J.; Hamagami, F. Advanced studies of individual differences linear dynamic models for longitudinal data analysis. In New Developments and Techniques in Structural Equation Modeling; Lawrence Erlbaum: Mahwah, NJ, USA, 2001; pp. 203–246. [Google Scholar]
- Newsom, J.T. Longitudinal Structural Equation Modeling: A Comprehensive Introduction; Routledge: New York, NY, USA, 2015. [Google Scholar]
- Schochet, P.Z. An Approach for Addressing the Multiple Testing Problem in Social Policy Impact Evaluations. Eval. Rev. 2009, 33, 539–567. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B Stat. Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Muthen, L.K.; Muthen, B. Mplus Version 8 User’s Guide; Muthen & Muthen: Los Angeles, CA, USA, 2017; ISBN 978-0-9829983-2-8. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Conroy, D.; Nicholls, E. All in this together? Psychologist 2020. Available online: https://thepsychologist.bps.org.uk/all-together (accessed on 29 December 2020).
- Clouston, S.A.P.; Brewster, P.; Kuh, D.; Richards, M.; Cooper, R.; Hardy, R.; Rubin, M.S.; Hofer, S.M. The Dynamic Relationship Between Physical Function and Cognition in Longitudinal Aging Cohorts. Epidemiol. Rev. 2013, 35, 33–50. [Google Scholar] [CrossRef]
- Gajewski, P.D.; Falkenstein, M. Physical activity and neurocognitive functioning in aging—A condensed updated review. Eur. Rev. Aging Phys. Act. 2016, 13, 1. [Google Scholar] [CrossRef]
- Gow, A.J.; Bastin, M.E.; Maniega, S.M.; Hernández, M.C.V.; Morris, Z.; Murray, C.; Royle, N.A.; Starr, J.M.; Deary, I.J.; Wardlaw, J.M. Neuroprotective lifestyles and the aging brain: Activity, atrophy, and white matter integrity. Neurology 2012, 79, 1802–1808. [Google Scholar] [CrossRef]
- Rogers, N.T.; Marshall, A.; Roberts, C.H.; Demakakos, P.; Steptoe, A.; Scholes, S. Physical activity and trajectories of frailty among older adults: Evidence from the English Longitudinal Study of Ageing. PLoS ONE 2017, 12, e0170878. [Google Scholar] [CrossRef]
- Tajvar, M.; Fletcher, A.; Grundy, E. Exploring associations between social support and mental health in older people: A systematic narrative review. Ageing Dev. Ctries. 2016, 1, 1–120. [Google Scholar]
- Brooke, J.; Jackson, D. Older people and COVID-19: Isolation, risk and ageism. J. Clin. Nurs. 2020, 29, 2044–2046. [Google Scholar] [CrossRef] [PubMed]
- Kroencke, L.; Geukes, K.; Utesch, T.; Kuper, N.; Back, M. Neuroticism and emotional risk during the COVID-19 pandemic. J. Res. Personal. 2020, 89, 104038. [Google Scholar] [CrossRef] [PubMed]
- Weyers, S.; Dragano, N.; Moebus, S.; Beck, E.-M.; Stang, A.; Möhlenkamp, S.; Jöckel, K.-H.; Erbel, R.; Siegrist, J. Low socio-economic position is associated with poor social networks and social support: Results from the Heinz Nixdorf Recall Study. Int. J. Equity Health 2008, 7, 13. [Google Scholar] [CrossRef]
- Krause, N.; Borawski-Clark, E. Social class differences in social support among older adults. Gerontologist 1995, 35, 498–508. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Bu, F.; Steptoe, A.; Fancourt, D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. Public Health 2020, 186, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Corley, J.; Cox, S.R.; Deary, I.J. Healthy cognitive ageing in the Lothian Birth Cohort studies: Marginal gains not magic bullet. Psychol. Med. 2017, 48, 187–207. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Hiam, L.; Sowemimo, A.; Devakumar, D.; McKee, M. Ethnicity and covid-19. BMJ 2020, 369, m2282. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| T1 | T2 | p | |
|---|---|---|---|
| Sleep quality | 0.597 1 | ||
| -very bad | 1 (0.7%) | 1 (0.7%) | |
| -fairly bad | 16 (11.7%) | 21 (15.3%) | |
| -fairly good | 80 (58.4%) | 74 (54.0%) | |
| -very good | 40 (29.2%) | 41 (29.9%) | |
| Physical activity | 0.012 1 | ||
| -only household chores | 14 (10.2%) | 26 (19.0%) | |
| -outdoor activities 1–2x per week | 28 (20.4%) | 23 (16.8%) | |
| -outdoor activities > 2x per week | 67 (48.9%) | 74 (54.0%) | |
| -moderate exercise 1–2x per week | 19 (13.9%) | 4 (2.9%) | |
| -moderate exercise > 2x per week | 6 (4.4%) | 10 (7.3%) | |
| -keep-fit/heavy exercise several times per week | 3 (2.2%) | 0 (0.0%) | |
| Loneliness | 0.059 1 | ||
| -none/almost none of the time | 111 (81.0%) | 100 (73.0%) | |
| -some of the time | 22 (16.1%) | 32 (23.4%) | |
| -most of the time | 4 (2.9%) | 4 (2.9%) | |
| -all or almost all the time | 0 (0.0%) | 1 (0.7%) | |
| Memory problems | 0.192 1 | ||
| -Mean (SD) | 1.212 (1.046) | 1.321 (1.156) | |
| Wellbeing | 0.076 2 | ||
| -Mean (SD) | 37.453 (8.369) | 36.453 (8.230) | |
| Social support | 0.032 1 | ||
| -Mean (SD) | 12.759 (2.490) | 13.095 (1.802) | |
| Neighborhood cohesion | 0.108 2 | ||
| -Mean (SD) | 22.920 (5.377) | 22.372 (4.756) |
| Sleep | Physical | Loneliness | Memory | Wellbeing | Social Support | |
|---|---|---|---|---|---|---|
| Sleep | ||||||
| Physical activity | −0.161 | |||||
| Loneliness | −0.102 | −0.095 | ||||
| Memory | 0.035 | −0.023 | 0.100 | |||
| Wellbeing | 0.030 | −0.035 | −0.220 ** | −0.223 ** | ||
| Social support | −0.099 | −0.064 | −0.096 | −0.169 * | 0.174 * | |
| Neighbourhood | −0.018 | −0.119 | −0.006 | −0.038 | 0.138 | 0.135 |
| Change Variable | Covariate | Est | 95% CI | p | FDR p |
|---|---|---|---|---|---|
| Wellbeing a | Emotional stability * | 0.221 | 0.094, 0.348 | 0.001 | 0.003 |
| Living with others | 0.252 | −0.031, 0.536 | 0.081 | 0.081 | |
| History of CVD * | −0.376 | −0.634, −0.118 | 0.004 | 0.006 | |
| Neighbourhood a | Intellect | 0.147 | 0.022,0.272 | 0.021 | 0.025 |
| History of CVD | −0.310 | −0.580, −0.039 | 0.025 | 0.025 | |
| Social support a | Intellect | 0.118 | 0.003, 0.232 | 0.044 | 0.088 |
| Occupational class | |||||
| managerial | 0.195 | −0.063, 0.453 | 0.138 | 0.184 | |
| skilled non-manual | −0.052 | −0.461, 0.357 | 0.804 | 0.804 | |
| manual | 0.575 | 0.192, 0.959 | 0.003 | 0.012 | |
| Physical activity a | Intellect | 0.035 | −0.102, 0.173 | 0.615 | 0.718 |
| Extraversion | 0.162 | 0.035, 0.289 | 0.012 | 0.084 | |
| Age 11 IQ | 0.143 | 0.017, 0.269 | 0.026 | 0.091 | |
| Fluid g | 0.137 | −0.014, 0.287 | 0.075 | 0.175 | |
| Occupational class | |||||
| managerial | −0.018 | −0.289, 0.254 | 0.899 | 0.899 | |
| skilled non−manual | 0.235 | −0.232, 0.702 | 0.324 | 0.454 | |
| manual | −0.302 | −0.682, 0.077 | 0.118 | 0.206 | |
| Memory a | Depression | −0.159 | −0.316, −0.002 | 0.047 | − |
| Loneliness b | Anxiety | 1.222 | 1.049, 1.424 | 0.010 | 0.010 |
| Living with others * | 0.149 | 0.061, 0.364 | <0.001 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okely, J.A.; Corley, J.; Welstead, M.; Taylor, A.M.; Page, D.; Skarabela, B.; Redmond, P.; Cox, S.R.; Russ, T.C. Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936. Int. J. Environ. Res. Public Health 2021, 18, 210. https://doi.org/10.3390/ijerph18010210
Okely JA, Corley J, Welstead M, Taylor AM, Page D, Skarabela B, Redmond P, Cox SR, Russ TC. Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936. International Journal of Environmental Research and Public Health. 2021; 18(1):210. https://doi.org/10.3390/ijerph18010210
Chicago/Turabian StyleOkely, Judith A., Janie Corley, Miles Welstead, Adele M. Taylor, Danielle Page, Barbora Skarabela, Paul Redmond, Simon R. Cox, and Tom C. Russ. 2021. "Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936" International Journal of Environmental Research and Public Health 18, no. 1: 210. https://doi.org/10.3390/ijerph18010210
APA StyleOkely, J. A., Corley, J., Welstead, M., Taylor, A. M., Page, D., Skarabela, B., Redmond, P., Cox, S. R., & Russ, T. C. (2021). Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936. International Journal of Environmental Research and Public Health, 18(1), 210. https://doi.org/10.3390/ijerph18010210