Response of Different Treatment Protocols to Treat Chronic Non-Bacterial Osteomyelitis (CNO) of the Mandible in Adult Patients: A Systematic Review

 ,
,  ,
, 
Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Study Selection
2.4. Data Collection Process and Items
2.5. Risk of Bias within Studies
3. Results
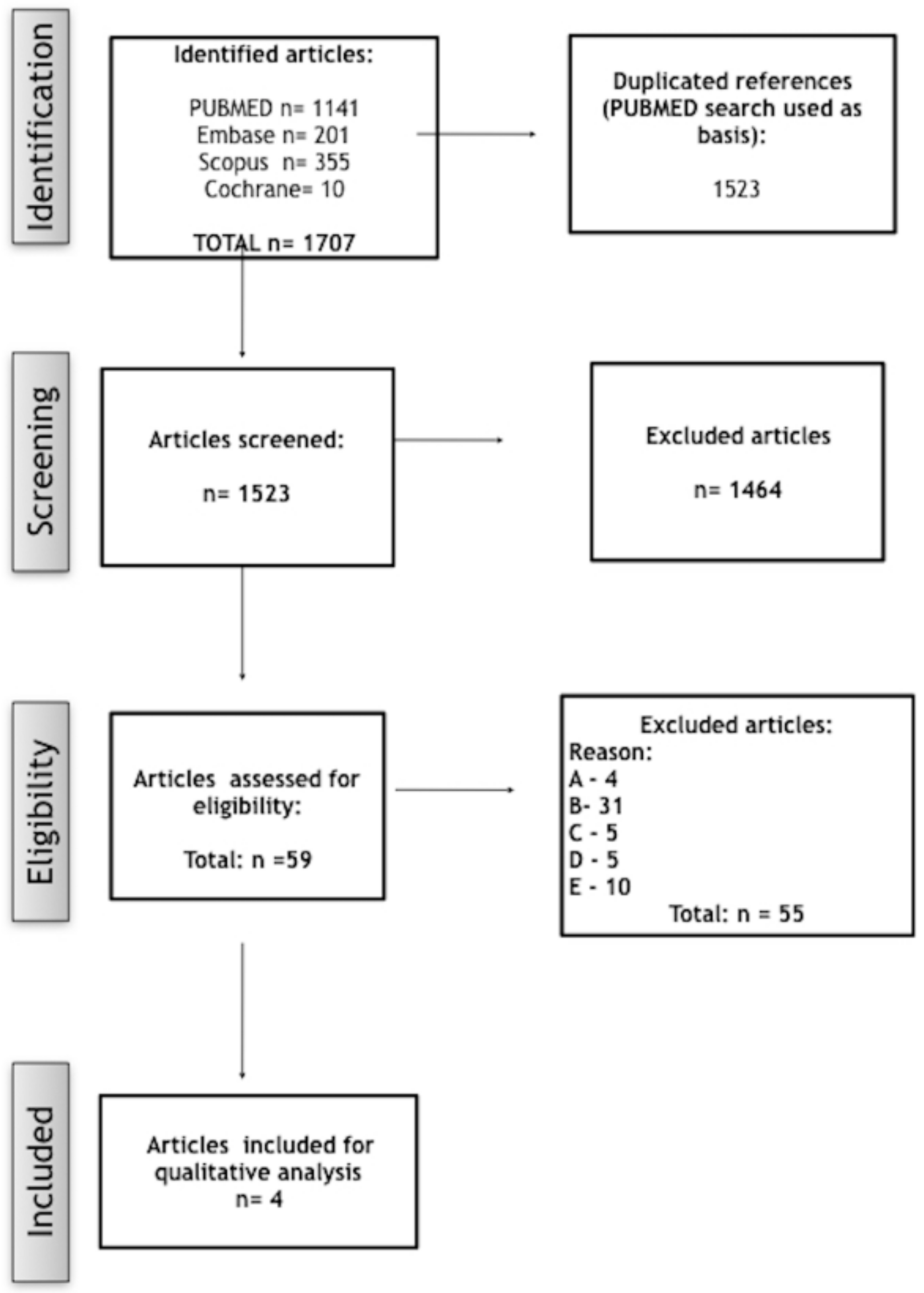
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
4. Discussion
4.1. Follow-Up
4.2. Surgical Therapy
4.3. Pharmacological Therapy
4.4. Antibiotics
4.5. Antiresorptive Drugs
4.6. Use of NSAIDs
4.7. Nomenclature Recommendation
4.8. Limitations of the Review
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Baltensperger, M.M. Osteomyelitis of the Jaws: With 47 Tables; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Agarwal, A.; Kumar, N.; Tyagi, A.; De, N. Primary chronic osteomyelitis in the mandible: A conservative approach. BMJ Case Rep. 2014. [Google Scholar] [CrossRef]
- Kudva, A.; Kamath, A.T.; Dhara, V.; Ravindranath, V. Chronic recurrent osteomyelitis: A surgeon’s enigma. J. Oral. Pathol. Med. Off. Publ. Int. Assoc. Oral. Pathol. Am. Acad. Oral. Pathol. 2019, 48, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Rustemeyer, J.; Siegmund, B.J.; Okcu, Y.; Busch, A. Total mandibular reconstruction following diffuse sclerosing osteomyelitis. Oral. Maxillofac. Surg. 2019, 23, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Urade, M.; Noguchi, K.; Takaoka, K.; Moridera, K.; Kishimoto, H. Diffuse sclerosing osteomyelitis of the mandible successfully treated with pamidronate: A long-term follow-up report. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2012, 114, e9–e12. [Google Scholar] [CrossRef] [PubMed]
- Morbach, H.; Dick, A.; Beck, C.; Stenzel, M.; Müller-Hermelink, H.K.; Raab, P.; Girschick, H.J. Association of chronic non-bacterial osteomyelitis with Crohn’s disease but not with CARD15 gene variants. Rheumatol. Int. 2010, 30, 617–621. [Google Scholar] [CrossRef]
- Buch, K.; Thuesen, A.C.B.; Brøns, C.; Schwarz, P. Chronic Non-bacterial Osteomyelitis: A Review. Calcif. Tissue Int. 2018. [Google Scholar] [CrossRef]
- Gamble, J.G.; Rinsky, L.A. Chronic recurrent multifocal osteomyelitis: A distinct clinical entity. J. Pediatr. Orthop. 1986, 6, 579–584. [Google Scholar] [CrossRef]
- Hofmann, S.R.; Kubasch, A.S.; Ioannidis, C.; Rösen-Wolff, A.; Girschick, H.J.; Morbach, H.; Hedrich, C.M. Altered expression of IL-10 family cytokines in monocytes from CRMO patients result in enhanced IL-1β expression and release. Clin. Immunol. 2015, 161, 300–307. [Google Scholar] [CrossRef]
- Hofmann, S.R.; Roesen-Wolff, A.; Hahn, G.; Hedrich, C.M. Update: Cytokine Dysregulation in Chronic Nonbacterial Osteomyelitis (CNO). Int. J. Rheumatol. 2012, 2012, 310206. [Google Scholar] [CrossRef]
- Hofmann, S.R.; Schwarz, T.; Möller, J.C.; Morbach, H.; Schnabel, A.; Rösen-Wolff, A.; Girschick, H.J.; Hedrich, C.M. Chronic non-bacterial osteomyelitis is associated with impaired Sp1 signaling, reduced IL10 promoter phosphorylation, and reduced myeloid IL-10 expression. Clin. Immunol. 2011, 141, 317–327. [Google Scholar] [CrossRef]
- Scianaro, R.; Insalaco, A.; Bracci Laudiero, L.; De Vito, R.; Pezzullo, M.; Teti, A.; De Benedetti, F.; Prencipe, G. Deregulation of the IL-1β axis in chronic recurrent multifocal osteomyelitis. Pediatr. Rheumatol. Online J. 2014, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Taddio, A.; Zennaro, F.; Pastore, S.; Cimaz, R. An Update on the Pathogenesis and Treatment of Chronic Recurrent Multifocal Osteomyelitis in Children. Paediatr. Drugs 2017, 19, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Taddio, A.; Ferrara, G.; Insalaco, A.; Pardeo, M.; Gregori, M.; Finetti, M.; Pastore, S.; Tommasini, A.; Ventura, A.; Gattorno, M. Dealing with Chronic Non-Bacterial Osteomyelitis: A practical approach. Pediatr. Rheumatol. Online J. 2017, 15, 87. [Google Scholar] [CrossRef] [PubMed]
- Jacobsson, S.; Dahlén, G.; Möller, A.J. Bacteriologic and serologic investigation in diffuse sclerosing osteomyelitis (DSO) of the mandible. Oral. Surg. Oral. Med. Oral. Pathol. 1982, 54, 506–512. [Google Scholar] [CrossRef]
- Skrabl-Baumgartner, A.; Singer, P.; Greimel, T.; Gorkiewicz, G.; Hermann, J. Chronic non-bacterial osteomyelitis: A comparative study between children and adults. Pediatr. Rheumatol. Online J. 2019, 17, 49. [Google Scholar] [CrossRef]
- Van de Meent, M.M.; Pichardo, S.E.C.; Rodrigues, M.F.; Verbist, B.M.; Van Merkesteyn, J.P.R. Radiographic characteristics of chronic diffuse sclerosing osteomyelitis/tendoperiostitis of the mandible: A comparison with chronic suppurative osteomyelitis and osteoradionecrosis. J. Cranio-Maxillo-Fac. Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-Fac. Surg. 2018, 46, 1631–1636. [Google Scholar] [CrossRef]
- Van Merkesteyn, J.P.; Groot, R.H.; Bras, J.; McCarroll, R.S.; Bakker, D.J. Diffuse sclerosing osteomyelitis of the mandible: A new concept of its etiology. Oral. Surg. Oral. Med. Oral. Pathol. 1990, 70, 414–419. [Google Scholar] [CrossRef]
- Yoshii, T.; Nishimura, H.; Yoshikawa, T.; Furudoi, S.; Yoshioka, A.; Takenono, I.; Ohtsuka, Y.; Komori, T. Therapeutic possibilities of long-term roxithromycin treatment for chronic diffuse sclerosing osteomyelitis of the mandible. J. Antimicrob. Chemother. 2001, 47, 631–637. [Google Scholar] [CrossRef]
- Kim, S.M.; Lee, S.K. Chronic non-bacterial osteomyelitis in the jaw. J. Korean Assoc. Oral. Maxillofac. Surg. 2019, 45, 68–75. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Jacobsson, S.; Hollender, L. Treatment and prognosis of diffuse sclerosing osteomyelitis (DSO) of the mandible. Oral. Surg. Oral. Med. Oral. Pathol. 1980, 49, 7–14. [Google Scholar] [CrossRef]
- Kuijpers, S.C.C.; De Jong, E.; Hamdy, N.A.T.; Van Merkesteyn, J.P.R. Initial results of the treatment of diffuse sclerosing osteomyelitis of the mandible with bisphosphonates. J. Cranio-Maxillo-fac. Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-fac. Surg. 2011, 39, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Montonen, M.; Kalso, E.; Pylkkären, L.; Lindströrm, B.M.; Lindqvist, C. Disodium clodronate in the treatment of diffuse sclerosing osteomyelitis (DSO) of the mandible. Int. J. Oral. Maxillofac. Surg. 2001, 30, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Jacobsson, S. Diffuse sclerosing osteomyelitis of the mandible. Int. J. Oral. Surg. 1984, 13, 363–385. [Google Scholar] [CrossRef]
- McPhillips, A.; Wolford, L.M.; Rodrigues, D.B. SAPHO syndrome with TMJ involvement: Review of the literature and case presentation. Int. J. Oral. Maxillofac. Surg. 2010, 39, 1160–1167. [Google Scholar] [CrossRef]
- Müller-Richter, U.D.A.; Roldán, J.C.; Mörtl, M.; Behr, M.; Reichert, T.E.; Driemel, O. SAPHO syndrome with ankylosis of the temporomandibular joint. Int. J. Oral. Maxillofac. Surg. 2009, 38, 1335–1341. [Google Scholar] [CrossRef]
- Zemann, W.; Feichtinger, M.; Pau, M.; Kärcher, H. Primary osteomyelitis of the mandibular condyle--a rare case. Oral. Maxillofac. Surg. 2011, 15, 109–111. [Google Scholar] [CrossRef]
- Reichardt, L.F.; Pitak-Arnnop, P.; Hemprich, A.; Dhanuthai, K.; Pausch, N.C. Chronic refractory osteomyelitis as a part of synovitis, acne, pustulosis, hyperostosis and osteitis (SAPHO) syndrome: A diagnostic challenge. ANZ J. Surg. 2011, 81, 642–643. [Google Scholar] [CrossRef]
- Kriauciunas, A.; Gleiznys, A.; Gleiznys, D.; Janužis, G. The Influence of Porphyromonas Gingivalis Bacterium Causing Periodontal Disease on the Pathogenesis of Rheumatoid Arthritis: Systematic Review of Literature. Cureus 2019, 11, e4775. [Google Scholar] [CrossRef]
- Urasaki, Y.; Nori, M.; Iwata, S.; Sasaki, T.; Hosono, O.; Kawasaki, H.; Tanaka, H.; Dang, N.H.; Ikeda, E.; Morimoto, C. Roxithromycin specifically inhibits development of collagen induced arthritis and production of proinflammatory cytokines by human T cells and macrophages. J. Rheumatol. 2005, 32, 1765–1774. [Google Scholar]
- Ianaro, A.; Ialenti, A.; Maffia, P.; Sautebin, L.; Rombolà, L.; Carnuccio, R.; Iuvone, T.; D’Acquisto, F.; Di Rosa, M. Anti-inflammatory activity of macrolide antibiotics. J. Pharmacol. Exp. Ther. 2000, 292, 156–163. [Google Scholar] [PubMed]
- Scaglione, F.; Rossoni, G. Comparative anti-inflammatory effects of roxithromycin, azithromycin and clarithromycin. J. Antimicrob. Chemother. 1998, 41, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Kodama, Y.; Tanaka, R.; Kurokawa, A.; Ohnuki, H.; Sultana, S.; Hayashi, T.; Iizuka, T.; Takagi, R. Severe destruction of the temporomandibular joint with complete resorption of the condyle associated with synovitis, acne, pustulosis, hyperostosis, and osteitis syndrome. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2013, 116, e128–e133. [Google Scholar] [CrossRef] [PubMed]
- Otto, S.; Troeltzsch, M.; Burian, E.; Mahaini, S.; Probst, F.; Pautke, C.; Ehrenfeld, M.; Smolka, W. Ibandronate treatment of diffuse sclerosing osteomyelitis of the mandible: Pain relief and insight into pathogenesis. J. Cranio-Maxillo-fac. Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-fac. Surg. 2015, 43, 1837–1842. [Google Scholar] [CrossRef] [PubMed]
- Kuroshima, S.; Sasaki, M.; Sawase, T. Medication-related osteonecrosis of the jaw: A literature review. J. Oral. Biosci. 2019, 61, 99–104. [Google Scholar] [CrossRef]
- Montonen, M.; Li, T.-F.; Lukinmaa, P.-L.; Sakai, E.; Hukkanen, M.; Sukura, A.; Konttinen, Y.T. RANKL and cathepsin K in diffuse sclerosing osteomyelitis of the mandible. J. Oral. Pathol. Med. Off. Publ. Int. Assoc. Oral. Pathol. Am. Acad. Oral. Pathol. 2006, 35, 620–625. [Google Scholar] [CrossRef]
- Hallmer, F.; Korduner, M.; Møystad, A.; Bjørnland, T. Treatment of diffuse sclerosing osteomyelitis of the jaw with denosumab shows remarkable results-A report of two cases. Clin. Case Rep. 2018, 6, 2434–2437. [Google Scholar] [CrossRef]
- Otto, S.; Burian, E.; Troeltzsch, M.; Kaeppler, G.; Ehrenfeld, M. Denosumab as a potential treatment alternative for patients suffering from diffuse sclerosing osteomyelitis of the mandible-A rapid communication. J. Cranio-Maxillo-fac. Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-fac. Surg. 2018, 46, 534–537. [Google Scholar] [CrossRef]
- Concha, S.; Hernández-Ojeda, A.; Contreras, O.; Mendez, C.; Talesnik, E.; Borzutzky, A. Chronic nonbacterial osteomyelitis in children: A multicenter case series. Rheumatol. Int. 2019. [Google Scholar] [CrossRef]
- Girschick, H.; Finetti, M.; Orlando, F.; Schalm, S.; Insalaco, A.; Ganser, G.; Nielsen, S.; Herlin, T.; Koné-Paut, I.; Martino, S.; et al. PRINTO and the Eurofever registry. The multifaceted presentation of chronic recurrent multifocal osteomyelitis: A series of 486 cases from the Eurofever international registry. Rheumatol. Oxf. Engl. 2018. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| P | #1 | ((mandible) OR mandibular) OR jaw | 180,180 |
| I | #2 | (((((((((osteomyelitis [MeSH Terms]) OR "diffuse sclerosing osteomyelitis") OR "chronic non-bacterial osteomyelitis") OR CNO) OR DSO) OR PCO) OR SAPHO) OR CRMO)) | 28,673 |
| O | #3 | ((((treatment) OR therapy) OR follow-up) OR outcome) | 10,715,195 |
| P+I+O | #1+ #2+ #3 | ((((((((((((osteomyelitis [MeSH Terms]) OR "diffuse sclerosing osteomyelitis") OR "chronic non-bacterial osteomyelitis") OR CNO) OR DSO) OR PCO) OR SAPHO) OR CRMO)))) AND (((mandible) OR mandibular) OR jaw)) AND ((((treatment) OR therapy) OR follow-up) OR outcome) | 1141 |
| Authors | Country | Study design | Patients (n) | Term | Gender | Age | Symptoms |
|---|---|---|---|---|---|---|---|
| Jacobsson and Hollender. [23] | Sweden | Retrospective study | 11 | DSO | F (7), M (4) | 22–53 | Pain, swelling, trismus, ankylosis from TMJ |
| Kuijpers et al. [24] | Netherlands | Retrospective study | 6 | DSO | F (5), M (1) | 23–78 | |
| Montonen et al. [25] | Finland | Prospective, randomized, double-blind and placebo controlled. | 10 | DSO | F (8), M (2) | 31–77 | Pain |
| Yoshii et al. [19] | Japan | Retrospective study | 9 | DSOM | F (5), M (4) | 19–70 | Pain, swelling, trismus |
| Authors | Imaging | Previous Treatment | Treatment | Therapeutic Regime | Outcome | Follow-Up |
|---|---|---|---|---|---|---|
| Jacobsson and Hollender. [23] | Radiographic and scintigraphic examinations | Short- and long-term antibiotic therapy, decortication, tooth extraction | Decortication (7), excision, resection, antibiotics, cortisone | Predinisolone 20/5 mg (12 d), penicillin (3 months) | Long-term antibiotic therapy decreased the interval between exacerbations and pain/decortication ceased the symptoms for 6–12 months | 3–19 y |
| Kuijpers et al. [24] | Panoramic radiograph, CT | Analgesics (acetaminophen, NSAIDs), antibiotics (e.g., doxycycline, amoxicillin, vibramycin, clindamycin), physiotherapy, corticosteroids and/or surgery | Bisphosphonate (intravenous dose of 15 mg pamidronate, 3–5 d) | - | Symptoms decreased or disappeared | 18–46 months |
| Montonen et al. [25] | Radiological examinations, scintigraphy and orthopantomography | Conservative or surgical therapy | Bisphosphonate | Disodiumclodronate (300 to 900 mg) or placebo intravenously | There was a greater pain relief after 6 em of treatment with bisphosphonate | 12 months |
| Yoshii et al. [19] | Radiographic imaging | Surgical treatment | Long-term roxithromycin | 300 mg, oral, daily, 68 d–66 months | Pain was reduced and ceased completely in 7 of 9 patients | 12 months |
| Risk of bias assessment | Jacobsson et al. | Kuijpers et al. | Montonen et al. | Yoshii et al. | Total |
|---|---|---|---|---|---|
| A clearly stated aim | 1 | 0 | 2 | 1 | 4 |
| Inclusion of consecutive patients | 1 | 1 | 2 | 2 | 6 |
| Prospective collection of data | 0 | 1 | 2 | 0 | 3 |
| Endpoints appropriate to the aim of the study | 1 | 1 | 1 | 1 | 4 |
| Unbiased assessment of the study endpoint | 0 | 0 | 2 | 1 | 3 |
| Follow-up period appropriate to the aim of the study | 1 | 1 | 2 | 1 | 5 |
| Loss to follow-up less than 5% | 2 | 1 | 2 | 2 | 7 |
| Prospective calculation of the study size | 0 | 0 | 0 | 0 | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timme, M.; Bohner, L.; Huss, S.; Kleinheinz, J.; Hanisch, M. Response of Different Treatment Protocols to Treat Chronic Non-Bacterial Osteomyelitis (CNO) of the Mandible in Adult Patients: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 1737. https://doi.org/10.3390/ijerph17051737
Timme M, Bohner L, Huss S, Kleinheinz J, Hanisch M. Response of Different Treatment Protocols to Treat Chronic Non-Bacterial Osteomyelitis (CNO) of the Mandible in Adult Patients: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(5):1737. https://doi.org/10.3390/ijerph17051737
Chicago/Turabian StyleTimme, Maximilian, Lauren Bohner, Sebastian Huss, Johannes Kleinheinz, and Marcel Hanisch. 2020. "Response of Different Treatment Protocols to Treat Chronic Non-Bacterial Osteomyelitis (CNO) of the Mandible in Adult Patients: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 5: 1737. https://doi.org/10.3390/ijerph17051737
APA StyleTimme, M., Bohner, L., Huss, S., Kleinheinz, J., & Hanisch, M. (2020). Response of Different Treatment Protocols to Treat Chronic Non-Bacterial Osteomyelitis (CNO) of the Mandible in Adult Patients: A Systematic Review. International Journal of Environmental Research and Public Health, 17(5), 1737. https://doi.org/10.3390/ijerph17051737