Preconception Care among Pregnant Women in an Urban and a Rural Health Facility in Kenya: A Quantitative Study


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Study Participants
3.2. Uptake and Determinants of PCC
4. Discussion
4.1. Strengths
4.2. Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Meeting to Develop a Global Consensus on Preconception Care to Reduce Maternal and Childhood Mortality and Morbidity: World Health Organization Headquarters, Geneva, 6–7 February 2012; Meeting Report, 2013; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Say, L.; Chou, D.; Gemmill, A.; Tunçalp, Ö.; Moller, A.-B.; Daniels, J.; Gülmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob Health 2014, 2, e323–e333. [Google Scholar] [CrossRef]
- Jack, B.W.; Atrash, H.; Coonrod, D.V.; Moos, M.-K.; O’Donnell, J.; Johnson, K. The clinical content of preconception care: An overview and preparation of this supplement. Am. J. Obstet. Gynecol. 2008, 199, S266–S279. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Public Health and Sanitation. National Reproductive Health Strategy 2009–2015; Ministry of Public Health and Sanitation: Nairobi, Kenya, 2009. [Google Scholar]
- Demographic, K. Health Survey 2014: Key Indicators; Kenya National Bureau of Statistics (KNBS) and ICF Macro: Nairobi, Kenya, 2014. [Google Scholar]
- Defo, B.K. The importance for the MDG4 and MDG5 of addressing reproductive health issues during the second decade of life: Review and analysis from times series data of 51 African countries. Afr. J. Reprod. Health 2011, 15, 9–30. [Google Scholar] [PubMed]
- Frey, K.A.; Files, J.A. Preconception healthcare: What women know and believe. Matern. Child Health J. 2006, 10, S73–S77. [Google Scholar] [CrossRef] [PubMed]
- Ezegwui, H.U.; Dim, C.; Dim, N.; Ikeme, A.C. Preconception care in South Eastern Nigeria. J. Obstet. Gynaecol. 2008, 28, 765–768. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, J.; Patel, D.; Barrett, G.; Howden, B.; Copas, A.; Ojukwu, O.; Pandya, P.; Shawe, J. How do women prepare for pregnancy? Preconception experiences of women attending antenatal services and views of health professionals. PLoS ONE 2014, 9, e103085. [Google Scholar] [CrossRef] [PubMed]
- Ekem, N.N.; Lawani, L.O.; Onoh, R.C.; Iyoke, C.A.; Ajah, L.O.; Onwe, E.O.; Onyebuchi, A.K.; Okafor, L.C. Utilisation of preconception care services and determinants of poor uptake among a cohort of women in Abakaliki Southeast Nigeria. J. Obstet. Gynaecol. 2018, 38, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Idris, S.H.; Sambo, M.N.; Ibrahim, M.S. Barriers to utilisation of maternal health services in a semi-urban community in northern Nigeria: The clients’ perspective. Niger. Med. J. J. Niger. Med. Assoc. 2013, 54, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Statistics, K.N.B. Kenya Demographic and Health Survey 2014; Kenya National Bureau of Statistics: Nairobi, Kenya, 2015. [Google Scholar]
- Nairobi City County. The Project on Integrated Urban Development Master Plan for the City of Nairobi in the Republic of Kenya; Nairobi City County Nairobi: Nairobi, Kenya, 2014. [Google Scholar]
- Ndegwa, E. Murang’a County Council Integrated Regional Development Plan (2013–2017); Kenya Open Data: Nairobi, Kenya, 2013. [Google Scholar]
- Kawakatsu, Y.; Sugishita, T.; Oruenjo, K.; Wakhule, S.; Kibosia, K.; Were, E.; Honda, S. Determinants of health facility utilization for childbirth in rural western Kenya: Cross-sectional study. BMC Pregnancy Childbirth 2014, 14, 265. [Google Scholar] [CrossRef] [PubMed]
- Jalang’o, R.; Thuita, F.; Barasa, S.O.; Njoroge, P. Determinants of contraceptive use among postpartum women in a county hospital in rural KENYA. BMC Public Health 2017, 17, 604. [Google Scholar] [CrossRef] [PubMed]
- Banke-Thomas, A.; Banke-Thomas, O.; Kivuvani, M.; Ameh, C.A. Maternal health services utilisation by Kenyan adolescent mothers: Analysis of the Demographic Health Survey 2014. Sex. Reprod. Healthc. 2017, 12, 37–46. [Google Scholar] [PubMed]
- Ayalew, Y.; Mulat, A.; Dile, M.; Simegn, A. Women’s knowledge and associated factors in preconception care in adet, west gojjam, northwest Ethiopia: A community based cross sectional study. Reprod. Health 2017, 14, 15. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preconception Care: Maximizing the Gains for Maternal and Child Health; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Okonofua, F.; Ntoimo, L.; Ogungbangbe, J.; Anjorin, S.; Imongan, W.; Yaya, S. Predictors of women’s utilization of primary health care for skilled pregnancy care in rural Nigeria. BMC Pregnancy Childbirth 2018, 18, 106. [Google Scholar] [CrossRef] [PubMed]
- Sinai, I.; Anyanti, J.; Khan, M.; Daroda, R.; Oguntunde, O. Demand for Women’s Health Services in Northern Nigeria: A Review of the Literature. Afr. J. Reprod. Health 2017, 21, 96–108. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; WHO Press: Geneva, Switzerland, 2013. [Google Scholar]


{kind=link}
{kind=link}
| AKUH, N n (%) or Mean ± S.D | Maragua n (%) or Mean ± S.D | p-Value (Chi-Square/t-Test) | |
|---|---|---|---|
| Age: | |||
| Mean | 30.1 ± 4.0 | 26.8 ± 5.4 | |
| <30 years | 42 (43.3) | 68 (70.1) | |
| ≥30 years | 55 (56.7) | 29 (29.9) | <0.01 |
| Marital status: | |||
| Married | 84 (86.6) | 60 (61.9) | 0.01 |
| Single | 12 (12.4) | 31 (32.0) | |
| Divorced | 0 (0.0) | 1 (1.0) | |
| Widowed | 1 (1.0) | 5 (5.2) | |
| Education: | |||
| Primary | 0 (0.0) | 18 (18.6) | <0.01 |
| Secondary | 3 (3.1) | 54 (55.7) | |
| Tertiary | 94 (96.9) | 24 (24.7) | |
| None | 0 (0.0) | 1 (1.0) | |
| Occupation: | |||
| Student | 5 (5.2) | 3 (3.1) | <0.01 |
| Unemployed | 8 (8.2) | 21 (21.6) | |
| Farmer | 0 (0.0) | 21 (21.6) | |
| Business | 17(17.5) | 33 (34.0) | |
| Professional | 67 (69.1) | 19 (19.6) | |
| Parity: | |||
| Primigravida | 33 (34.0) | 38 (39.2) | 0.46 |
| Multigravida | 64 (66.0) | 59 (60.8) | |
| Prior poor pregnancy outcomes: Yes No Miscarriages Molar pregnancy Ectopic pregnancy Preterm birth Stillbirth Birth defects | (n = 64) 43 (67.2) 21 (32.8) 21 (32.8) 1 (1.6) 1 (1.6) 5 (7.8) 2 (3.1) 0 (0.0) | (n = 59) 34 (57.6) 25 (42.4) 17 (28.8) 0 (0.0) 6 (10.2) 3 (5.1) 4 (6.8) 2 (3.4) | 0.19 |
| Caesarian section delivery | (n = 64) | (n = 59) | 0.28 |
| 16 (25.0) | 17 (28.8) | ||
| Medical conditions during prior pregnancy (such as diabetes, hypertension, cholestasis in pregnancy etc.) | (n = 64) | (n = 59) | 0.95 |
| 4 (6.3) | 8 (13.6) | ||
| Preexisting medical conditions | |||
| Diabetes | 1 (1.0) | 3 (3.1) | 0.23 |
| High blood pressure | 2 (2.1) | 1 (1.0) | |
| Heart disease | 0 (0.0) | 0 (0.0) | |
| Asthma | 4 (4.1) | 5 (5.2) | |
| Epilepsy | 1 (1.0) | 1 (1.0) | |
| HIV | 4 (4.1) | 8 (8.2) | |
| None | 85 (87.6) | 79 (81.4) |
| AKUH, N n (%) or Mean ± S.D | Maragua n (%) or Mean ± S.D | p-Value (Chi-Square/t-Test) | |
|---|---|---|---|
| Last time seen by health professional other than for ANC | |||
| Within 3 months before pregnancy | 43 (44.3) | 11 (11.3) | <0.01 |
| Within 6 months before pregnancy | 16 (16.5) | 6 (6.2) | |
| Within 12 months before pregnancy | 7 (7.2) | 8 (8.2) | |
| More than a year before pregnancy | 17 (17.5) | 38 (39.2) | |
| Never | 14 (14.4) | 34 (35.1) | |
| Purpose of visit to health care professional | |||
| Regular health check up | 25 (25.8) | 1 (1.0) | <0.01 |
| Sick and needed medical care | 35 (36.1) | 54 (55.7) | |
| To discuss pregnancy plans and preparation | 23 (23.7) | 8 (8.2) | |
| Not applicable (i.e., had never seen health professional before) | 14 (14.4) | 34 (35.1) | |
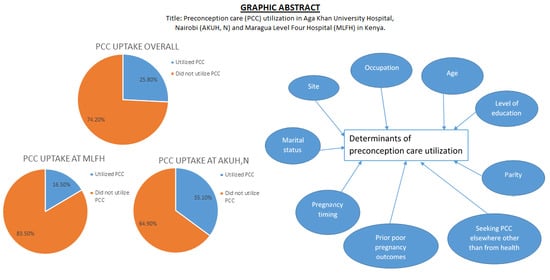
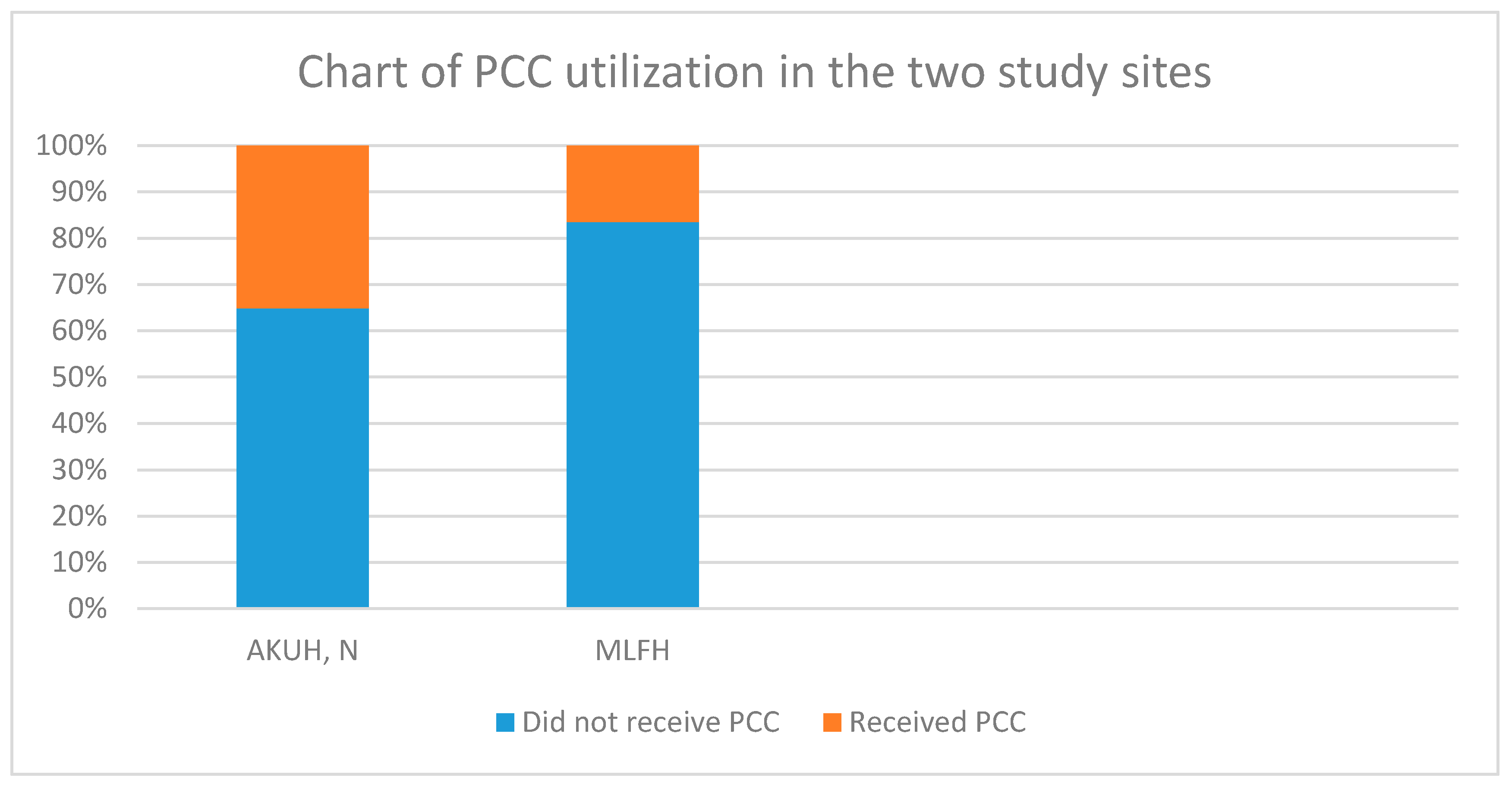
| Received PCC: Yes | 34 (35.1) | 16 (16.5) | <0.01 |
| No | 63 (64.9) | 81 (83.5) | |
| Sought PCC elsewhere other than from health provider: | |||
| No | 60 (61.9) | 71 (73.2) | 0.19 |
| Yes | 37 (38.1) | 26 (26.8) | |
| Family | 16 (16.5) | 12 (12.4) | |
| Friend | 16 (16.5) | 18 (18.6) | |
| Radio/ Television | 0 (0.0) | 0 (0.0) | |
| Social media | 8 (8.2) | 4 (4.1) | |
| Traditional healer | 0 (0.0) | 0(0.0) | |
| Other (Internet, google) | 8 (8.2) | 3 (3.1) | |
| Challenges to accessing medical care | |||
| Distance | 2 (2.1) | 2 (2.1) | <0.01 |
| Financial | 4 (4.1) | 28 (28.9) | |
| Other (time) | 2 (2.1) | 0 (0.0) | |
| None | 89 (91.8) | 67 (69.1) | |
| About becoming pregnant | |||
| Right time | 79 (81.4) | 59 (60.8) | <0.01 |
| Okay, but not right time | 17 (17.5) | 29 (29.9) | |
| Wrong time | 1 (1.0) | 9 (9.3) | |
| Possible to prepare for pregnancy | |||
| Yes | 91 (93.8) | 65 (67.0) | <0.01 |
| No | 6 (6.2) | 32 (33.0) | |
| There is enough information about PCC | |||
| Yes | 38 (39.2) | 6 (6.2) | <0.01 |
| No | 59 (60.8) | 91 (93.8) |
| Characteristic (n = Number of Respondents) | PCC Received (%) | Odds Ratio (95% Confidence Interval) | p-Value |
|---|---|---|---|
| Age: <30 years | 20/110 (18.1) | ||
| ≥30 years | 30/84 (35.7) | 2.5 (1.3–4.8) | 0.01 |
| Site: AKUH, N | 34/97 (35.1) | ||
| MLFH | 16/97 (16.5) | 0.3 (0.2–0.7) | <0.01 |
| Marital status: Not Married | 7/50 (14.0) | ||
| Married | 43/144 (29.9) | 2.6 (1.1–6.3) | 0.03 |
| Education: Below tertiary | 9/76 (11.4) | ||
| Tertiary | 41/118 (34.7) | 4.0 (1.8–8.8) | <0.01 |
| Occupation: | |||
| No formal employment | 16/108 (14.8) | ||
| Formal employment | 34/86 (39.5) | 3.8 (1.9–7.5) | <0.01 |
| Parity: Primigravida | 10/71 (14.1) | ||
| Multigravida | 40/123 (32.5) | 3.0 (1.4–6.3) | 0.01 |
| Prior poor pregnancy outcomes | |||
| No | 10/17 (58.8) | 3.1 (1.6–6.0) | <0.01 |
| Yes | 30/106 (28.3) | ||
| Miscarriages | 26/38 (42.1) | 2.6 (1.2–5.5) | 0.01 |
| Preterm birth | 3/8 (37.5) | 1.8 (0.4–7.7) | 0.44 |
| Stillbirth | 2/6 (33.3) | 1.5 (0.3–8.2) | 0.67 |
| Birth defects | 1/2 (50.0) | 2.9 (0.2–47.5) | 0.43 |
| Preexisting medical conditions: | |||
| No | 42/164 (25.6) | ||
| Yes | 8/30 (26.7) | 1.1 (0.4–2.3) | 0.90 |
| Sought PCC elsewhere (not health provider): | |||
| No | 23/131 (17.6) | ||
| Yes | 27/63 (42.9) | 3.5 (1.8–6.9) | <0.01 |
| Challenges to accessing medical care: | |||
| No | 40/156 (25.6) | ||
| Yes | 10/38 (26.3) | 1.0 (0.5–2.3) | 0.94 |
| About becoming pregnant | |||
| Not right time | 8/56 (14.3) | ||
| Right time | 42/138 (30.4) | 2.6 (1.1–6.0) | 0.02 |
| There is enough information about PCC: | |||
| No | 34/150 (22.7) | ||
| Yes | 16/44 (36.4) | 2.0 (0.9–4.0) | 0.07 |
| Variables | Adjusted Odds Ratio (95% Confidence Interval) | p-Value |
|---|---|---|
| Site | 1.32 (0.479–3.612) | 0.60 |
| Age | 1.18 (0.552–2.511) | 0.67 |
| Marital status | 1.58 (0.587–4.227) | 0.37 |
| Education | 3.08 (0.955–9.940) | 0.06 |
| Occupation | 2.20 (0.951–5.083) | 0.07 |
| Parity | 1.68 (0.607–4.652) | 0.32 |
| Prior poor pregnancy outcomes | 2.39 (0.978–5.861) | 0.06 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okemo, J.; Temmerman, M.; Mwaniki, M.; Kamya, D. Preconception Care among Pregnant Women in an Urban and a Rural Health Facility in Kenya: A Quantitative Study. Int. J. Environ. Res. Public Health 2020, 17, 7430. https://doi.org/10.3390/ijerph17207430
Okemo J, Temmerman M, Mwaniki M, Kamya D. Preconception Care among Pregnant Women in an Urban and a Rural Health Facility in Kenya: A Quantitative Study. International Journal of Environmental Research and Public Health. 2020; 17(20):7430. https://doi.org/10.3390/ijerph17207430
Chicago/Turabian StyleOkemo, Joan, Marleen Temmerman, Mukaindo Mwaniki, and Dorothy Kamya. 2020. "Preconception Care among Pregnant Women in an Urban and a Rural Health Facility in Kenya: A Quantitative Study" International Journal of Environmental Research and Public Health 17, no. 20: 7430. https://doi.org/10.3390/ijerph17207430
APA StyleOkemo, J., Temmerman, M., Mwaniki, M., & Kamya, D. (2020). Preconception Care among Pregnant Women in an Urban and a Rural Health Facility in Kenya: A Quantitative Study. International Journal of Environmental Research and Public Health, 17(20), 7430. https://doi.org/10.3390/ijerph17207430