Effect of Fluoride Concentration in Drinking Water on Dental Fluorosis in Southwest Saudi Arabia

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Rodríguez, I.; Jaudenes, J.R.; Hardisson, A.; Paz, S.; Rubio, C.; Gutiérrez, A.J.; Burgos, A.; Revert, C. Potentiometric determination of fluoride concentration in beers. Biol. Trace Elem. Res. 2018, 181, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Akuno, M.H.; Nocella, G.; Milia, E.P.; Gutierrez, L. Factors influencing the relationship between fluoride in drinking water and dental fluorosis: A ten-year systematic review and meta-analysis. J. Water Health 2019, 17, 845–862. [Google Scholar] [CrossRef] [PubMed]
- Bakhurji, E.A.; Alqahtani, Y.S. Fluoride Concentration of Water Supply in Eastern Saudi Arabia: A Preliminary Study. Saudi J. Med. Med. Sci. 2018, 6, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.O.; Jones, K.; Tomar, S.L. An economic evaluation of community water fluoridation. J. Public Health Dent. 2001, 61, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Nowak, B.; Sicilio, L.; Kizior, C.; Tedder, G.; Zimmerman, N.; Bobo, N. Advocating for Oral Health Through Fluoridation. NASN Sch. Nurse 2019, 34, 288–294. [Google Scholar] [CrossRef]
- Till, C.; Green, R.; Grundy, J.G.; Hornung, R.; Neufeld, R.; Martinez-Mier, E.A.; Ayotte, P.; Muckle, G.; Lanphear, B. Community water fluoridation and urinary fluoride concentrations in a national sample of pregnant women in Canada. Environ. Health Perspect. 2018, 126, 107001. [Google Scholar] [CrossRef]
- de Souza, C.F.M.; de Oliveira Paredes, S.; Forte, F.D.S.; Sampaio, F.C. The fluoride content of bottled water commercialized in two cities of northeastern Brazil. J. Oral Sci. 2009, 8, 206–209. [Google Scholar]
- Maraqa, M.A.; Ghoudi, K. Survey of public attitude towards bottled and tap water quality in the UAE. Global NEST J. 2015, 17, 607–617. [Google Scholar]
- Aldosari, A.M.; Akpata, E.S.; Khan, N.; Wyne, A.H.; Al-Meheithif, A. Fluoride levels in drinking water in the central province of Saudi Arabia. Ann. Saudi Med. 2003, 23, 20–23. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services Federal Panelon Community Water Fluoridation. U.S. Public health servicerecommendation for fluoride concentration in drinking water for theprevention of dental caries. Public Health Rep. 2015, 130, 318–331. [Google Scholar] [CrossRef]
- Elsherbini, M.S.; Alsughier, Z.; Elmoazen, R.A.; Habibullah, M.A. Prevalence and severity of dental fluorosis among primary school children in AlRass, Saudi Arabia. Int. J. Med. Health Res. 2018, 4, 45–49. [Google Scholar]
- Fawell, J.; Bailey, K.; Chilton, J.; Dahi, E.; Fewtrell, L.; Magara, Y. Fluoride in Drinking-Water; World Health Organization: Geneva, Switzerland, 2006; Volume 208, pp. 693–713. [Google Scholar]
- Wei, W.; Gao, Y.; Wang, C.; Zhao, L.; Sun, D. Excessive fluoride induces endoplasmic reticulum stress and interferes enamel proteinases secretion. Environ. Toxicol. 2013, 28, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Ahiropoulos, V. Fluoride content of bottled waters available in Northern Greece. Int. J. Paediatr. Dent. 2006, 16, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.O.; Regnier, E.; Griffin, P.M.; Huntley, V. Effectiveness of fluoride in preventing caries in adults. J. Dent. Res. 2007, 86, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Gurbuz, F.; Akpınar, Ş.; Ozcan, S.; Acet, Ö.; Odabaşı, M. Reducing arsenic and groundwater contaminants down to safe level for drinking purposes via Fe3+-attached hybrid column. Environ. Monit. Assess. 2019, 191, 722. [Google Scholar] [CrossRef]
- Dhar, V.; Bhatnagar, M. Physiology and toxicity of fluoride. Indian J. Dent. Res. 2009, 20, 350. [Google Scholar] [CrossRef]
- Al-Zahrani, K.H.; Baig, M. Water in the Kingdom of Saudi Arabia: Sustainable management options. J. Anim. Plant. Sci. 2011, 21, 601–606. [Google Scholar]
- WHO/UNICEF. WHO/UNICEF Joint Monitoring Programme. Available online: http://www.wssinfo.org/ (accessed on 9 November 2019).
- Al-Othman, A.A.; Ahmed, I. Hydrogeological framework and its implication on water level rise in Eastern Al Riyadh, Saudi Arabia. Environ. Earth Sci. 2012, 67, 1493–1502. [Google Scholar] [CrossRef]
- Al-Khateeb, T.L.; Darwish, S.K.; Bastawi, A.E.; O’Mullane, D.M. Dental caries in children residing in communities in Saudi Arabia with differing levels of natural fluoride in the drinking water. Community Dent. Health 1990, 7, 165–990. [Google Scholar]
- Al Dosari, A.M.; Wyne, A.H.; Akpata, E.S.; Khan, N.B. Caries prevalence and its relation to water fluoride levels among schoolchildren in the central province of Saudi Arabia. Int. Dent. J. 2004, 54, 424–428. [Google Scholar] [CrossRef]
- Akpata, E.S.; Fakiha, Z.; Khan, N. Dental fluorosis in 12–15-year-old rural children exposed to fluorides from well drinking water in the hail region of Saudi Arabia. Community Dent Oral Epidemiol. 1997, 25, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Alshahrani, I.; Tikare, S.; Meer, Z.; Mustafa, A.; Abdulwahab, M.; Sadatullah, S. Prevalence of dental caries among male students aged 15–17 years in southern Asir, Saudi Arabia. Saudi Dent. J. 2018, 30, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.Q.; Moheet, I.A.; Farooq, F.A.; ArRejaie, A.S.; AlAbbad, M.A.; Khabeer, A. Prevalence of dental fluorosis in school going children of Dammam, Saudi Arabia. J. Dent. Allied Sci. 2015, 4, 69–72. [Google Scholar] [CrossRef]
- Elfaki, N.K.; Elsheikh, A.S.; Assiry, A.A.; Alsunbul, F. Dental Fluorosis Prevails among Primary-Schools’ Students in Najran City-Saudi Arabia. Merit Res. J. Med. Med. Sci. 2018, 6, 121–125. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
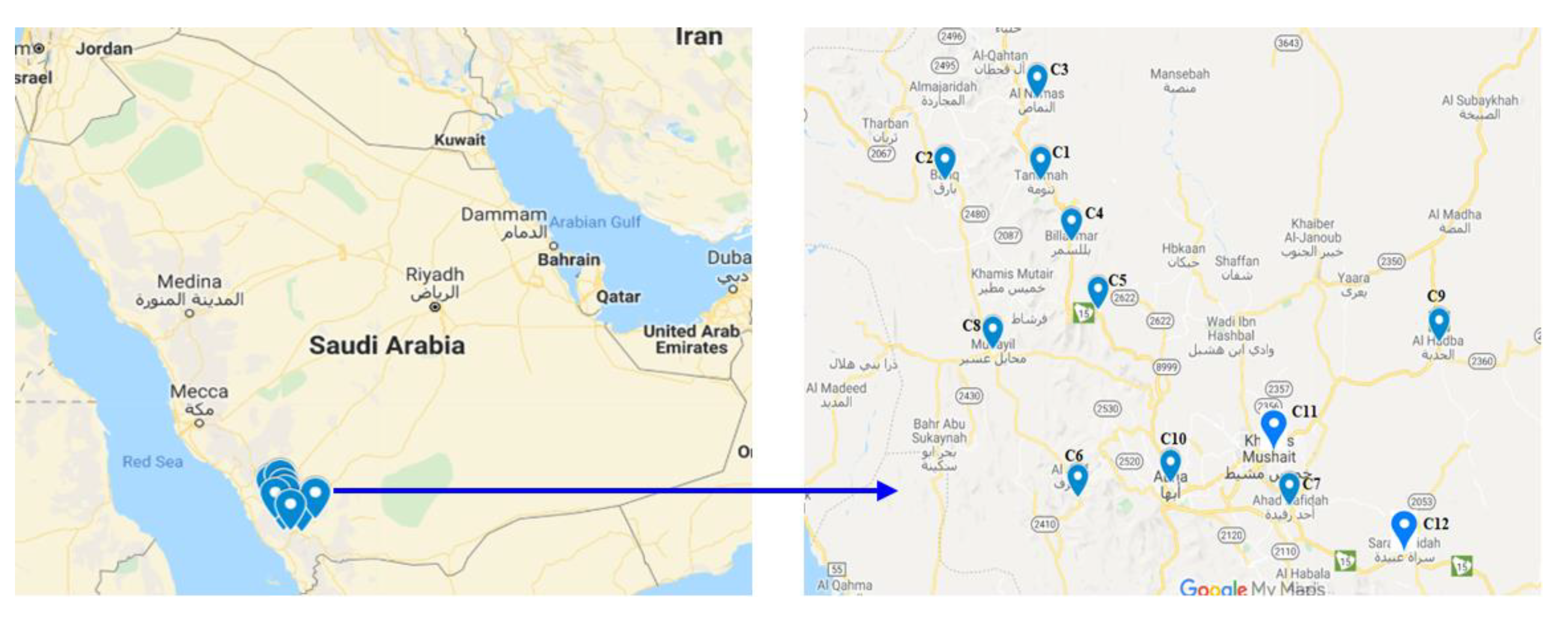
| City/Regions | GPS Location | Code Assigned to Well Water | Code Assigned to Filtered Water |
|---|---|---|---|
| Tanomah | 18.92901, 42.17702 | C1 | F1 |
| Belqarn | 18.93053, 41.92956 | C2 | F2 |
| Al Namas | 19.11342, 42.16714 | C3 | F3 |
| Bellasmar | 18.79251, 42.25596 | C4 | F4 |
| Bellahmar | 18.63841, 42.32379 | C5 | F5 |
| Rigal Alma | 18.21253, 42.27384 | C6 | F6 |
| Ahad Rafidah | 18.1952, 42.82051 | C7 | F7 |
| Muhayil | 18.54739, 42.05343 | C8 | F8 |
| Tareeb | 18.56551, 43.20596 | C9 | F9 |
| Abha | 18.24646, 42.51172 | C10 | F10 |
| KhamisMushayat | 18.30933, 42.76623 | C11 | F11 |
| SaratAbedah | 18.09931, 43.11656 | C12 | F12 |
| Water Source | Code | No. of Samples | Fluoride Content (ppm) | Std. Deviation | ||
|---|---|---|---|---|---|---|
| Min. | Max. | Mean | ||||
| Well Water | C1 | 5 | 1.10 | 3.50 | 2.44 | 0.97 |
| C2 | 5 | 1.30 | 3.80 | 2.24 | 0.99 | |
| C3 | 5 | 1.05 | 3.80 | 2.10 | 1.09 | |
| C4 | 5 | 1.70 | 3.70 | 2.34 | 0.81 | |
| C5 | 5 | 1.50 | 3.20 | 2.12 | 0.66 | |
| C6 | 5 | 1.30 | 2.20 | 2.21 | 0.71 | |
| C7 | 5 | 1.10 | 1.90 | 1.69 | 0.34 | |
| C8 | 5 | 1.75 | 3.10 | 2.33 | 0.63 | |
| C9 | 5 | 1.15 | 2.00 | 1.43 | 0.35 | |
| C10 | 5 | 1.20 | 2.40 | 1.78 | 0.49 | |
| C11 | 5 | 1.10 | 2.60 | 2.08 | 0.63 | |
| C12 | 5 | 0.60 | 1.10 | 0.82 | 0.20 | |
| Average/mean | 1.24 | 2.78 | 1.97 | |||
| Water Source | Code | No. of Samples | Fluoride Content (ppm) | Std. Deviation | ||
|---|---|---|---|---|---|---|
| Min. | Max. | Mean | ||||
| Filtered Water | F1 | 5 | 0.40 | 2.15 | 1.11 | 0.65 |
| F2 | 5 | 0.30 | 2.55 | 1.02 | 0.89 | |
| F3 | 5 | 0.03 | 2.45 | 0.89 | 1.03 | |
| F4 | 5 | 0.05 | 2.45 | 1.12 | 0.86 | |
| F5 | 5 | 0.07 | 2.55 | 0.98 | 0.94 | |
| F6 | 5 | 0.40 | 2.05 | 1.11 | 0.76 | |
| F7 | 5 | 0.08 | 2.25 | 1.19 | 0.80 | |
| F8 | 5 | 0.50 | 1.75 | 1.05 | 0.51 | |
| F9 | 5 | 0.30 | 2.05 | 0.93 | 0.70 | |
| F10 | 5 | 0.30 | 2.05 | 0.91 | 0.68 | |
| F11 | 5 | 0.30 | 2.25 | 1.11 | 0.77 | |
| F12 | 5 | 0.50 | 2.35 | 1.21 | 0.69 | |
| Average/mean | 0.27 | 2.24 | 1.05 | |||
| Water Source | Code | No. of Samples | Fluoride Content (ppm) | Std. Deviation | ||
|---|---|---|---|---|---|---|
| Min. | Max. | Mean | ||||
| Bottled Water | B1 | 3 | 0.8 | 1 | 0.92 | 0.10 |
| B2 | 3 | 1.2 | 1.4 | 1.30 | 0.10 | |
| B3 | 3 | 0.8 | 1.9 | 1.83 | 0.06 | |
| B4 | 3 | 0.9 | 1.1 | 1.00 | 0.10 | |
| B5 | 3 | 0.9 | 1 | 0.93 | 0.06 | |
| B6 | 3 | 1 | 1.1 | 1.03 | 0.06 | |
| B7 | 3 | 0.9 | 1.1 | 0.97 | 0.12 | |
| B8 | 3 | 0.8 | 0.9 | 0.87 | 0.06 | |
| B9 | 3 | 0.9 | 1.1 | 1.00 | 0.10 | |
| Average/mean | 0.91 | 1.18 | 1.09 | |||
| Variables | The Severity of Dental Fluorosis | ||||||
|---|---|---|---|---|---|---|---|
| None | Questionable | Very Mild | Mild | Moderate | Severe | Total | |
| Well water | 163 | 141 | 105 | 71 | 12 | 3 | 495 |
| Filtered water | 414 | 197 | 36 | 5 | 3 | 0 | 655 |
| Total | 577 | 338 | 141 | 76 | 15 | 3 | 1150 |
| p < 0.002 | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Das, G.; Tirth, V.; Arora, S.; Algahtani, A.; Kafeel, M.; Alqarni, A.H.G.; Saluja, P.; Vij, H.; Bavabeedu, S.S.; Tirth, A. Effect of Fluoride Concentration in Drinking Water on Dental Fluorosis in Southwest Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 3914. https://doi.org/10.3390/ijerph17113914
Das G, Tirth V, Arora S, Algahtani A, Kafeel M, Alqarni AHG, Saluja P, Vij H, Bavabeedu SS, Tirth A. Effect of Fluoride Concentration in Drinking Water on Dental Fluorosis in Southwest Saudi Arabia. International Journal of Environmental Research and Public Health. 2020; 17(11):3914. https://doi.org/10.3390/ijerph17113914
Chicago/Turabian StyleDas, Gotam, Vineet Tirth, Suraj Arora, Ali Algahtani, Mohammed Kafeel, Ayed Hassan G Alqarni, Priyanka Saluja, Hitesh Vij, Shashit Shetty Bavabeedu, and Amit Tirth. 2020. "Effect of Fluoride Concentration in Drinking Water on Dental Fluorosis in Southwest Saudi Arabia" International Journal of Environmental Research and Public Health 17, no. 11: 3914. https://doi.org/10.3390/ijerph17113914
APA StyleDas, G., Tirth, V., Arora, S., Algahtani, A., Kafeel, M., Alqarni, A. H. G., Saluja, P., Vij, H., Bavabeedu, S. S., & Tirth, A. (2020). Effect of Fluoride Concentration in Drinking Water on Dental Fluorosis in Southwest Saudi Arabia. International Journal of Environmental Research and Public Health, 17(11), 3914. https://doi.org/10.3390/ijerph17113914