Awareness of Clenching and Underweight are Risk Factors for Onset of Crowding in Young Adults: A Prospective 3-Year Cohort Study

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethical Procedures and Informed Consent
2.3. Self-Questionnaires
2.4. Assessment of Malocclusion
2.5. Assessment of Body Mass Index (BMI)
2.6. Statistical Analyses
3. Results
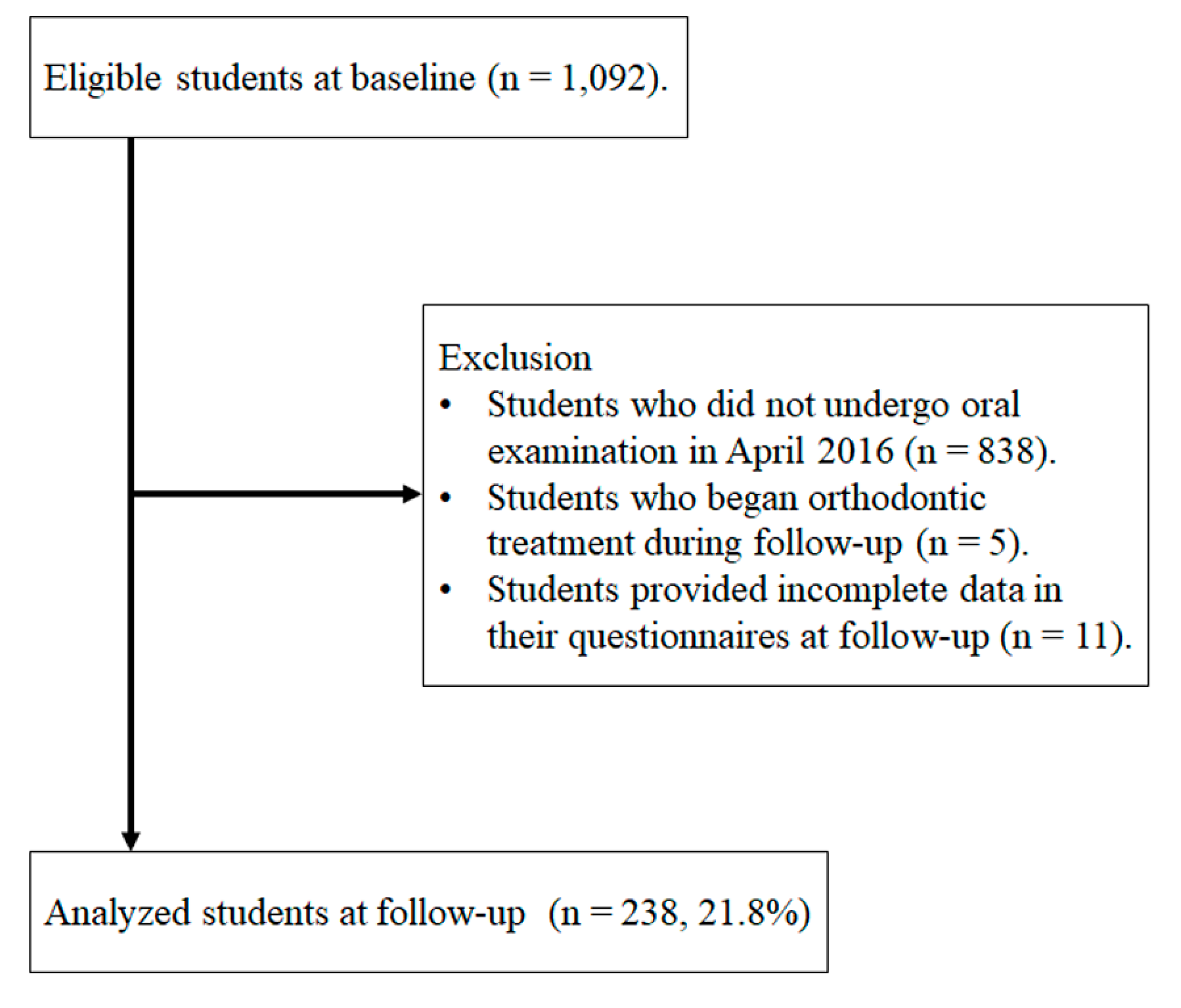
3.1. Study Population
3.2. Changes in Parameters from Baseline to Follow-Up
3.3. Association between Malocclusion/Crowding and Other Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Item No. | Recommendation | Page No. | |
|---|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract | 1 |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | 1 | ||
| Introduction | |||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | 1-2 |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses | 2 |
| Methods | |||
| Study design | 4 | Present key elements of study design early in the paper | 2 |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection | 2 |
| Participants | 6 | (a) Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of follow-up | 2 |
| (b) For matched studies, give matching criteria and number of exposed and unexposed | N/A | ||
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable | 2-3 |
| Data sources/measurement | 8 * | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | 2-3 |
| Bias | 9 | Describe any efforts to address potential sources of bias | 2 |
| Study size | 10 | Explain how the study size was arrived at | 2 |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | 3 |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding | 4 |
| (b) Describe any methods used to examine subgroups and interactions | 4 | ||
| (c) Explain how missing data were addressed | 2 | ||
| (d) If applicable, explain how loss to follow-up was addressed | 2 | ||
| (e) Describe any sensitivity analyses | N/A | ||
| Results | |||
| Participants | 13 * | (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed | 4 |
| (b) Give reasons for non-participation at each stage | 4 | ||
| (c) Consider use of a flow diagram | Figure 1 | ||
| Descriptive data | 14 * | (a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential confounders | 5 |
| (b) Indicate number of participants with missing data for each variable of interest | 4 | ||
| (c) Summarise follow-up time (eg, average and total amount) | 4 | ||
| Outcome data | 15 * | Report numbers of outcome events or summary measures over time | 5 |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence interval). Make clear which confounders were adjusted for and why they were included | 5-6 |
| (b) Report category boundaries when continuous variables were categorized | 5-7 | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | N/A | ||
| Other analyses | 17 | Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses | 6-7 |
| Discussion | |||
| Key results | 18 | Summarise key results with reference to study objectives | 7 |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | 8 |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | 8 |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results | 8 |
| Other information | |||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | 9 |
References
- Lobbezoo, F.; Ahlberg, J.; Glaros, A.G.; Kato, T.; Koyano, K.; Lavigne, G.J.; de Leeuw, R.; Manfredini, D.; Svensson, P.; Winocur, E. Bruxism defined and graded: An international consensus. J. Oral Rehabil. 2013, 40, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.V.; Kumar, M.P.; Sravanthi, D.; Mohsin, A.H.B.; Anuhya, V. Bruxism: A Literature Review. J. Int. Oral Health 2014, 6, 105–109. [Google Scholar] [PubMed]
- de Leeuw, R.; Klasser, G.D. Orofacial Pain: Guidelines for Assessment, Diagnosis, and Management (American Academy of Orofacial Pain), 5th ed.; Quintessence: Chicago, IL, USA, 2013; pp. 1–312. [Google Scholar]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Blair, G.S. Temporomandibular Joint—Function and Dysfunction. J. R. Soc. Med. 1979, 72, 882. [Google Scholar] [CrossRef]
- de la Hoz-Aizpurua, J.-L.; Díaz-Alonso, E.; LaTouche-Arbizu, R.; Mesa-Jiménez, J. Sleep bruxism. Conceptual review and update. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e231–e238. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, G.J.; Khoury, S.; Abe, S.; Yamaguchi, T.; Raphael, K. Bruxism physiology and pathology: An overview for clinicians. J. Oral Rehabil. 2008, 35, 476–494. [Google Scholar] [CrossRef] [PubMed]
- Shetty, S.; Pitti, V.; Satish Babu, C.L.; Surendra Kumar, G.P.; Deepthi, B.C. Bruxism: A literature review. J. Indian Prosthodont. Soc. 2010, 10, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Winocur, E.; Guarda-Nardini, L.; Paesani, D.; Lobbezoo, F. Epidemiology of bruxism in adults: A systematic review of the literature. J. Orofac. Pain 2013, 27, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Glaros, A.G. Incidence of diurnal and nocturnal bruxism. J. Prosthet. Dent. 1981, 45, 545–549. [Google Scholar] [CrossRef]
- Nekora-Azak, A.; Yengin, E.; Evlioglu, G.; Ceyhan, A.; Ocak, O.; Issever, H. Prevalence of bruxism awareness in Istanbul, Turkey. Cranio 2010, 28, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.; Rasmussen, B.K.; Pedersen, B.; Lous, I.; Olesen, J. Prevalence of oromandibular dysfunction in a general population. J. Orofac. Pain 1993, 7, 175–182. [Google Scholar] [PubMed]
- Melis, M.; Abou-Atme, Y.S. Prevalence of bruxism awareness in a Sardinian population. Cranio 2003, 21, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Seligman, D.A.; Pullinger, A.G.; Solberg, W.K. The prevalence of dental attrition and its association with factors of age, gender, occlusion, and TMJ symptomatology. J. Dent. Res. 1988, 67, 1323–1333. [Google Scholar] [CrossRef] [PubMed]
- Dantas-Neta, N.B.; Laurentino, J.B.; Nunes-Dos-Santos, D.L.; Mendes, R.F.; Prado-Júnior, R.R. Prevalence and potential factors associated with probable sleep or awake bruxism and dentin hypersensitivity in undergraduate students. Rev. Odontol. UNESP 2014, 43, 245–251. [Google Scholar] [CrossRef]
- Ilovar, S.; Zolger, D.; Castrillon, E.; Car, J.; Huckvale, K. Biofeedback for treatment of awake and sleep bruxism in adults: Systematic review protocol. Syst. Rev. 2014, 3, 42. [Google Scholar] [CrossRef] [PubMed]
- Paesani, D.A. Bruxism: Theory and Practice; Quintessence: Chicago, IL, USA, 2010. [Google Scholar]
- Murali, R.V.; Rangarajan, P.; Mounissamy, A. Bruxism: Conceptual discussion and review. J. Pharm. Bioallied Sci. 2015, 7, S265–S270. [Google Scholar] [CrossRef] [PubMed]
- Lobbezoo, F.; Brouwers, J.E.I.G.; Cune, M.S.; Naeije, M. Dental implants in patients with bruxing habits. J. Oral Rehabil. 2006, 33, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.; Omar, R.; Carlsson, G.E. Bruxism and prosthetic treatment: A critical review. J. Prosthodont. Res. 2011, 55, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Abboud, M.; Grüner, M.; Koeck, B. Anterior crowding—Just an esthetic problem? J. Orofac. Orthop. Fortschr. Kieferorthopädie 2002, 63, 264–273. [Google Scholar] [CrossRef]
- Kataoka, K.; Ekuni, D.; Mizutani, S.; Tomofuji, T.; Azuma, T.; Yamane, M.; Kawabata, Y.; Iwasaki, Y.; Morita, M. Association Between Self-Reported Bruxism and Malocclusion in University Students: A Cross-Sectional Study. J. Epidemiol. 2015, 25, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Ekuni, D.; Furuta, M.; Irie, K.; Azuma, T.; Tomofuji, T.; Murakami, T.; Yamashiro, T.; Ogura, T.; Morita, M. Relationship between impacts attributed to malocclusion and psychological stress in young Japanese adults. Eur. J. Orthod. 2011, 33, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Ekuni, D.; Mizutani, S.; Kojima, A.; Tomofuji, T.; Irie, K.; Azuma, T.; Yoneda, T.; Furuta, M.; Eshima, N.; Iwasaki, Y.; et al. Relationship between increases in BMI and changes in periodontal status: A prospective cohort study. J. Clin. Periodontol. 2014, 41, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Pintado, M.R.; Anderson, G.C.; DeLong, R.; Douglas, W.H. Variation in tooth wear in young adults over a two-year period. J. Prosthet. Dent. 1997, 77, 313–320. [Google Scholar] [CrossRef]
- Mizutani, S.; Ekuni, D.; Tomofuji, T.; Azuma, T.; Irie, K.; Machida, T.; Yoneda, T.; Iwasaki, Y.; Morita, M. Factors related to the formation of buccal mucosa ridging in university students. Acta Odontol. Scand. 2014, 72, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Palinkas, M.; De Luca Canto, G.; Rodrigues, L.A.; Bataglion, C.; Siéssere, S.; Semprini, M.; Regalo, S.C. Comparative Capabilities of Clinical Assessment, Diagnostic Criteria, and Polysomnography in Detecting Sleep Bruxism. J. Clin. Sleep Med. 2015, 11, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Emodi-Perlman, A.; Eli, I.; Friedman-Rubin, P.; Goldsmith, C.; Reiter, S.; Winocur, E. Bruxism, oral parafunctions, anamnestic and clinical findings of temporomandibular disorders in children. J. Oral Rehabil. 2012, 39, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Panek, H.; Nawrot, P.; Mazan, M.; Bielicka, B.; Sumisławska, M.; Pomianowski, R. Coincidence and awareness of oral parafunctions in college students. Commun. Dent. Health 2012, 29, 74–77. [Google Scholar]
- Gavish, A.; Halachmi, M.; Winocur, E.; Gazit, E. Oral habits and their association with signs and symptoms of temporomandibular disorders in adolescent girls. J. Oral Rehabil. 2000, 27, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Souki, B.Q.; Pimenta, G.B.; Souki, M.Q.; Franco, L.P.; Becker, H.M.G.; Pinto, J.A. Prevalence of malocclusion among mouth breathing children: Do expectations meet reality? Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Grippaudo, C.; Pantanali, F.; Paolantonio, E.G.; Grecolini, M.E.; Saulle, R.; La Torre, G.; Deli, R. Prevalence of malocclusion in Italian schoolchildren and orthodontic treatment need. Eur. J. Paediatr. Dent. 2013, 14, 314–318. [Google Scholar] [PubMed]
- Burden, D.J.; Pine, C.M.; Burnside, G. Modified IOTN: An orthodontic treatment need index for use in oral health surveys. Commun. Dent. Oral Epidemiol. 2001, 29, 220–225. [Google Scholar] [CrossRef]
- WHO Consultation on Obesity. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Hochberg, Y.; Tamhane, A.C. Multiple Comparison Procedures; Wiley Series in Probability and Statistics; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 1987. [Google Scholar]
- Gibbs, C.H.; Anusavice, K.J.; Young, H.M.; Jones, J.S.; Esquivel-Upshaw, J.F. Maximum clenching force of patients with moderate loss of posterior tooth support: A pilot study. J. Prosthet. Dent. 2002, 88, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Ono, Y.; Suganuma, T.; Shinya, A.; Furuya, R.; Baba, K. Effects of sleep bruxism on periodontal sensation and tooth displacement in the molar region. Cranio 2008, 26, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, K. Displacement Analysis of Living Human Teeth by X-ray CT Images and Coordinate Transformation. J. JSEM 2012, 12, s249–s254. [Google Scholar]
- Mack, K.B.; Phillips, C.; Jain, N.; Koroluk, L.D. Relationship between body mass index percentile and skeletal maturation and dental development in orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Armond, M.C.; Generoso, R.; Falci, S.G.M.; Ramos-Jorge, M.L.; Marques, L.S. Skeletal maturation of the cervical vertebrae: Association with various types of malocclusion. Braz. Oral Res. 2012, 26, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Malocclusion of Teeth: MedlinePlus Medical Encyclopedia. Available online: https://medlineplus.gov/ency/article/001058.htm (accessed on 28 November 2018).
- Aloufi, S.A.; Jan, H.E.; Abuhamda, I.S.; Assiri, A.T.; Samanodi, H.S.; Alsulami, A.A.; Alghamdi, M.A.; Algamdi, M.A.; Almobrki, W.A.; Algarni, S.M.; et al. Meta-Analysis of Prevalence of Bad Oral Habits and Relationship with Prevalence of Malocclusion. EC Dent. Sci. 2017, 11, 111–117. [Google Scholar]
- Tooth Clenching or Grinding. Available online: http://www.aaom.com/index.php%3Foption%3Dcom_content%26view%3Darticle%26id%3D129:tooth-clenching-or-grinding%26catid%3D22:patient-condition-information%26Itemid%3D120 (accessed on 28 November 2018).
- Komazaki, Y.; Fujiwara, T.; Ogawa, T.; Sato, M.; Suzuki, K.; Yamagata, Z.; Moriyama, K. Association between malocclusion and headache among 12- to 15-year-old adolescents: A population-based study. Commun. Dent. Oral Epidemiol. 2014, 42, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Puertes-Fernández, N.; Montiel-Company, J.M.; Almerich-Silla, J.M.; Manzanera, D. Orthodontic treatment need in a 12-year-old population in the Western Sahara. Eur. J. Orthod. 2011, 33, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Chestnutt, I.G.; Burden, D.J.; Steele, J.G.; Pitts, N.B.; Nuttall, N.M.; Morris, A.J. The orthodontic condition of children in the United Kingdom, 2003. Br. Dent. J. 2006, 200, 609–612. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare Japan National Health and Nutrition Survey 2013. Available online: http://ghdx.healthdata.org/record/japan-national-health-and-nutrition-survey-2013 (accessed on 28 November 2018).
- Miguel, J.A.; Sales, H.X.; Quintão, C.C.; Oliveira, B.H.; Feu, D. Factors associated with orthodontic treatment seeking by 12–15-year-old children at a state university-funded clinic. J. Orthodont. 2010, 37, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Dias, P.F.; Gleiser, R. Orthodontic treatment need in a group of 9–12-year-old Brazilian schoolchildren. Braz. Oral Res. 2009, 23, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Bernabé, E.; Borges-Yáñez, S.A.; Flores-Mir, C. The impact of orthodontic treatment on normative need. A case-control study in Peru. Aust. Orthodont. J. 2007, 23, 50–54. [Google Scholar]
- Flanagan, D.; Ilies, H.; McManus, A.; Larrow, B. Jaw Bite Force Measurement Device. J. Oral Implantol. 2012, 38, 361–364. [Google Scholar] [CrossRef] [PubMed]
- Cannavale, R.; Matarese, G.; Isola, G.; Grassia, V.; Perillo, L. Early treatment of an ectopic premolar to prevent molar-premolar transposition. Am. J. Orthodont. Dent. Orthop. 2013, 143, 559–569. [Google Scholar] [CrossRef] [PubMed]

| Missing teeth | Hypodontia requiring pre-restorative orthodontics or orthodontic space closure to obviate the need of a prosthesis. |
| Impeded eruption of teeth, presence of supernumerary teeth, and retained deciduous teeth. | |
| Overjet | Increased overjet greater than 6 mm. |
| Reverse overjet greater than 3.5 mm with no masticatory or speech difficulties. | |
| Reverse overjet greater than 1 mm but less than 3.5 mm with recorded masticatory and speech difficulties. | |
| Crossbite | Anterior or posterior crossbites with greater than 2 mm discrepancy between retruded contact position and intercuspal position. |
| Displacement of contact points (crowding) | Contact point displacements greater than 4 mm. |
| Overbite | Lateral or anterior open bites greater than 4 mm. |
| Deep overbite with gingival or palatal trauma. |
| Parameters | Total (n = 238) | 95%CI | P Value | |
|---|---|---|---|---|
| Baseline | Follow-Up Period | |||
| n (%) | n (%) | |||
| Mean ± SD | Mean ± SD | |||
| Malocclusion | 0 (0.0) | 128 (53.8) | ||
| Crowding | 0 (0.0) | 106 (44.5) | ||
| BMI (kg/m2) | ||||
| Normal range (18.5 ≤ BMI < 25) | 180 (75.6) | 187 (78.6) | 0.389 1 | |
| Underweight (<18.5) | 41 (17.2) | 35 (14.7) | ||
| Overweight (≥25) | 17 (7.1) | 16 (6.7) | ||
| Height (cm) | 164.8 ± 8.3 | 165.0 ± 8.5 | 0.15–0.33 | <0.001 2 |
| Weight (kg) | 56.4 ± 10.0 | 57.1 ± 9.7 | 0.13–1.15 | 0.015 2 |
| Parameter | Normal Occlusion n = 110 | Malocclusion n = 128 | P Value 1 |
|---|---|---|---|
| n (%) | n (%) | ||
| Sex | |||
| Male | 56 (50.9) | 70 (54.7) | 0.560 |
| Awareness of bruxism at baseline | |||
| Grinding during daytime | |||
| Yes | 2 (1.8) | 4 (3.1) | 0.689 |
| Clenching during daytime | |||
| Yes | 4 (3.6) | 13 (10.2) | 0.052 |
| Sleep bruxism | |||
| Yes | 10 (9.1) | 7 (5.5) | 0.279 |
| Oral habits at baseline | |||
| Gum chewing | |||
| Yes | 12 (10.9) | 10 (7.8) | 0.411 |
| Biting fingernail/pens/pencils | |||
| Yes | 10 (9.1) | 11 (8.6) | 0.893 |
| Biting mucosa of cheeks/lips | |||
| Yes | 22 (20.0) | 26 (20.3) | 0.952 |
| Early loss of primary teeth | |||
| Yes | 9 (8.2) | 4 (3.1) | 0.087 |
| Presence of malocclusion in parents | |||
| Yes | 5 (4.5) | 14 (10.9) | 0.070 |
| BMI at baseline (kg/m2) | |||
| Normal range (18.5 ≤ BMI < 25) | 91 (82.7) | 89 (69.5) | 0.043 |
| Underweight (<18.5) | 12 (10.9) | 29 (22.7) | |
| Overweight (≥25) | 7 (6.4) | 10 (7.8) |
| Parameter | Normal Occlusion n = 110 | Crowding n = 106 | P Value 1 |
|---|---|---|---|
| n (%) | n (%) | ||
| Sex | |||
| Male | 56 (50.9) | 59 (55.7) | 0.484 |
| Awareness of bruxism at baseline | |||
| Grinding during daytime | |||
| Yes | 2 (1.8) | 4 (3.8) | 0.439 |
| Clenching during daytime | |||
| Yes | 4 (3.6) | 12 (11.3) | 0.031 |
| Sleep bruxism | |||
| Yes | 10 (9.1) | 6 (5.7) | 0.336 |
| Oral habits at baseline | |||
| Gum chewing | |||
| Yes | 12 (10.9) | 7 (6.6) | 0.264 |
| Biting fingernail/pens/pencils | |||
| Yes | 10 (9.1) | 10 (9.4) | 0.931 |
| Biting mucosa of cheeks/lips | |||
| Yes | 22 (20.0) | 21 (19.8) | 0.972 |
| Early loss of primary teeth | |||
| Yes | 9 (8.2) | 4 (3.8) | 0.173 |
| Presence of malocclusion in parents | |||
| Yes | 5 (4.5) | 11 (10.4) | 0.102 |
| BMI at baseline (kg/m2) | |||
| Normal range (18.5 ≤ BMI < 25) | 91 (82.7) | 71 (67.0) | 0.020 |
| Underweight (<18.5) | 12 (10.9) | 26 (24.5) | |
| Overweight (≥25) | 7 (6.4) | 9 (8.5) |
| Variables | Malocclusion | Crowding | ||||
|---|---|---|---|---|---|---|
| OR | 95%CI | P Value 1 | OR | 95%CI | P Value 1 | |
| Sex | ||||||
| Female | 1.00 | Ref | 1.00 | Ref | ||
| Male | 1.34 | 0.79–2.29 | 0.279 | 1.45 | 0.82–2.55 | 0.183 |
| Clenching during daytime | ||||||
| No | 1.00 | Ref | 1.00 | Ref | ||
| Yes | 3.00 | 0.91–9.88 | 0.070 | 3.63 | 1.08–12.17 | 0.037 |
| BMI at baseline (kg/m2) | ||||||
| Normal range (18.5 ≤ BMI < 25) | 1.00 | Ref | 1.00 | Ref | ||
| Underweight (<18.5) | 2.34 | 1.11–4.92 | 0.025 | 2.52 | 1.25–5.76 | 0.011 |
| Overweight (≥25) | 1.41 | 0.51–3.91 | 0.505 | 1.67 | 0.57–4.58 | 0.373 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toyama, N.; Ekuni, D.; Taniguchi-Tabata, A.; Kataoka, K.; Yamane-Takeuchi, M.; Fujimori, K.; Kobayashi, T.; Fukuhara, D.; Irie, K.; Azuma, T.; et al. Awareness of Clenching and Underweight are Risk Factors for Onset of Crowding in Young Adults: A Prospective 3-Year Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 690. https://doi.org/10.3390/ijerph16050690
Toyama N, Ekuni D, Taniguchi-Tabata A, Kataoka K, Yamane-Takeuchi M, Fujimori K, Kobayashi T, Fukuhara D, Irie K, Azuma T, et al. Awareness of Clenching and Underweight are Risk Factors for Onset of Crowding in Young Adults: A Prospective 3-Year Cohort Study. International Journal of Environmental Research and Public Health. 2019; 16(5):690. https://doi.org/10.3390/ijerph16050690
Chicago/Turabian StyleToyama, Naoki, Daisuke Ekuni, Ayano Taniguchi-Tabata, Kota Kataoka, Mayu Yamane-Takeuchi, Kohei Fujimori, Terumasa Kobayashi, Daiki Fukuhara, Koichiro Irie, Tetsuji Azuma, and et al. 2019. "Awareness of Clenching and Underweight are Risk Factors for Onset of Crowding in Young Adults: A Prospective 3-Year Cohort Study" International Journal of Environmental Research and Public Health 16, no. 5: 690. https://doi.org/10.3390/ijerph16050690
APA StyleToyama, N., Ekuni, D., Taniguchi-Tabata, A., Kataoka, K., Yamane-Takeuchi, M., Fujimori, K., Kobayashi, T., Fukuhara, D., Irie, K., Azuma, T., Iwasaki, Y., & Morita, M. (2019). Awareness of Clenching and Underweight are Risk Factors for Onset of Crowding in Young Adults: A Prospective 3-Year Cohort Study. International Journal of Environmental Research and Public Health, 16(5), 690. https://doi.org/10.3390/ijerph16050690