Satisfaction with the Aesthetic Effect and Quality of Life for Women after Breast Conserving Therapy (BCT)—Preliminary Research


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
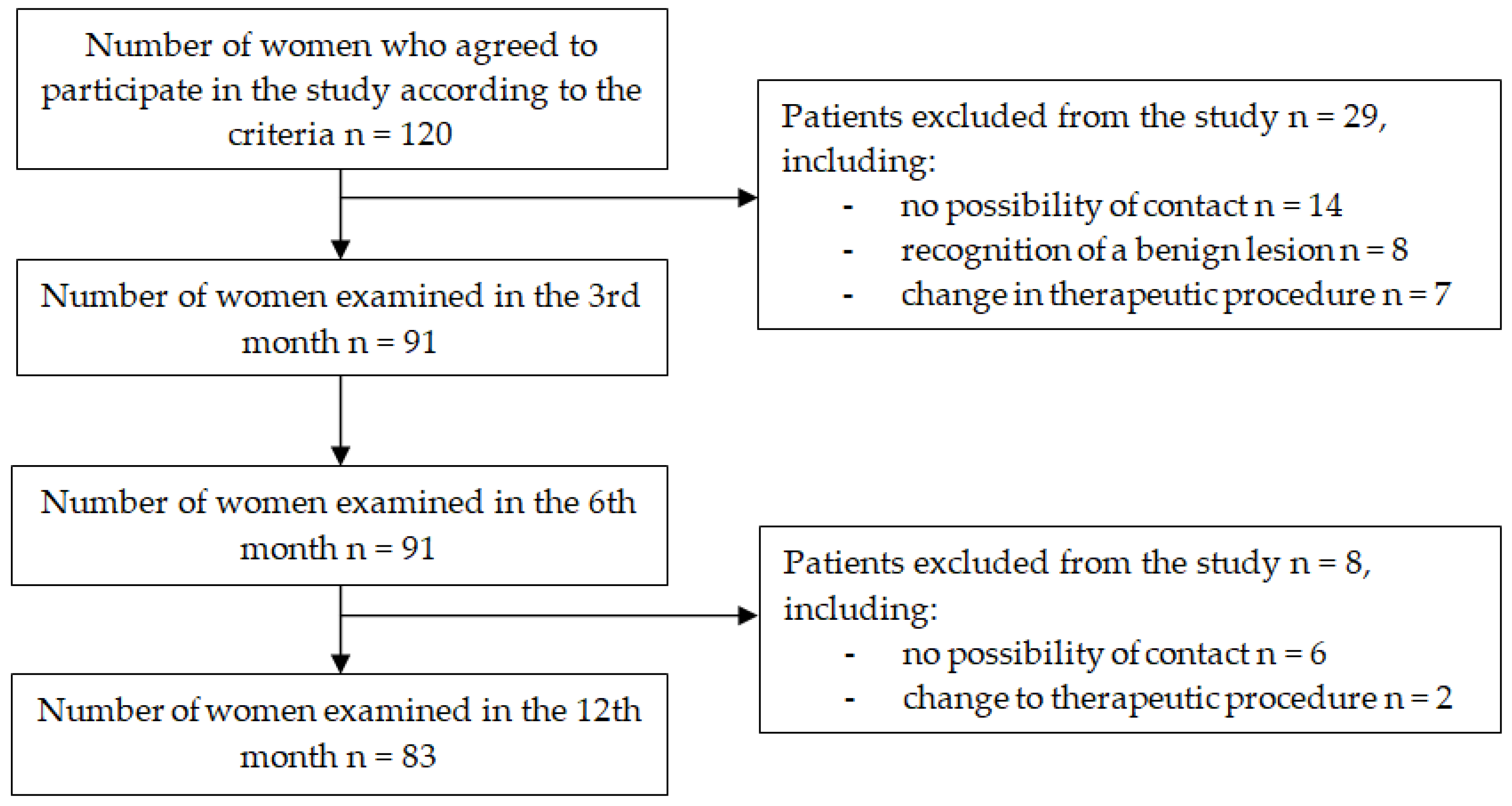
2.2. Participants
2.3. Ethical Approval
2.4. Questionnaire
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Results of Breast-Q Questionnaire
4. Discussion
5. Conclusions
- The level of patient satisfaction with the outcome of the surgery and the QoL related to health (according to the Breast-Q) do not differ significantly at any stage of long-term post-operative follow-up.
- The level of satisfaction with the aesthetic outcome of the surgery at all stages of post-operative assessment is higher than the level of satisfaction of women with their breast appearance before the operation.
- The QoL in terms of psychosocial functioning in patients with breast cancer undergoing BCT is significantly higher 12 months after surgery than in the pre-operative period.
- Patient satisfaction with the aesthetic outcome of the surgery has a strong positive relationship with the evaluation of their QoL in terms of psychosocial functioning at all stages of longitudinal observation.
Author Contributions
Funding
Conflicts of Interest
References
- Wojciechowska, U.; Czaderny, K.; Ciuba, A. Nowotwory złośliwe w Polsce w 2016 roku; Centrum Onkologii-Instytutim. M: Warszawa, Poland, 2018. [Google Scholar]
- WHO. International Agency for Research on Cancer: Breast. Available online: http://gco.iarc.fr/today/fact-sheets-cancers (accessed on 28 June 2019).
- Piekarski, J.; Jeziorski, A. Leczenie oszczędzające pierś jako pierwotne leczenie bez stosowania neoadjuwantowego leczenia systemowego. In Chirurgiczne Leczenie Zmian Nowotworowych Piersi; Konsensus Polskiego Towarzystwa Chirurgii Onkologicznej; Biblioteka Chirurga Onkologa; Jeziorski, A., Ed.; Via Medica: Gdańsk, Poland, 2016; Volume 5, pp. 17–19. [Google Scholar]
- Jassem, J.; Krzakowski, M. Breast cancer. Oncol. Clin. Pract. 2018, 14, 171–215. [Google Scholar] [CrossRef]
- Gentilini, O.; Botteri, E.; Rotmensz, N.; Da Lima, L.; Caliskan, M.; Garcia-Etienne, C.A.; Sosnovskikh, I.; Intra, M.; Mazzarol, G.; Musmeci, S.; et al. Conservative surgery in patients with multifocal/multicentric breast cancer. Breast Cancer Res. Treat. 2009, 113, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, H.P.; Cardoso, J.S.; Magalhães, A.; Cardoso, M.J. Methods for the aesthetic evaluation of breast cancer conservation treatment: A technological review. Curr. Med. Imaging Rev. 2013, 9, 32–46. [Google Scholar] [CrossRef]
- Cardoso, M.J.; Oliviera, H.; Cardoso, J. Assessing cosmetic results after breast conserving surgery. J. Surg. Oncol. 2014, 110, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Głowacka, I.; Nowikiewicz, T.; Nowacka, K.; Hagner, W.; Zegarski, W. Ocena jakości życia kobiet leczonych metodą BCT z procedurą węzła wartowniczego z powodu raka piersi. Polskie Forum Psychologiczne 2015, 20, 261–272. [Google Scholar] [CrossRef]
- Noguchi, M.; Saito, Y.; Mizukami, Y.; Nonomura, A.; Ohta, N.; Koyasaki, N.; Taniya, T.; Miyazaki, I. Breast deformity, its correction, and assessment of breast conserving surgery. Breast Cancer Res. Treat. 1991, 18, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Slavin, S.A.; Halperin, T. Reconstruction of breast the conservation deformity. Semin. Plast. Surg. 2004, 18, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Neto, E.A.; Alves, B.C.; Gehrke, F.D.; Azzalis, L.A.; Junqueira, V.C.; Sousa, L.V.; Adami, F.; Fonseca, F.L. Quality of life of post-mastectomy women living in a semi-arid region of Brazil. Int. J. Environ. Res. Public Health 2017, 14, 601. [Google Scholar] [CrossRef] [PubMed]
- Jabłoński, M.J.; Streb, J.; Mirucka, B.; Słowik, A.J.; Jach, R. The relationship between surgical treatment (mastectomy vs. breast conserving treatment) and body acceptance, manifesting femininity and experiencing an intimate relation with a partner in breast cancer patients. Psychiatr. Pol. 2018, 52, 859–872. [Google Scholar] [CrossRef] [PubMed]
- Montazeri, A. Health-related quality of life in breast cancer patients: A bibliographic review of the literature from 1974 to 2007. J. Exp. Clin. Cancer Res. 2008, 27, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Esplen, M.J.; Wong, J.; Warner, E.; Toner, B. Restoring body image after cancer (ReBIC): Results of a randomized controlled trial. J. Clin. Oncol. 2018, 36, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Pusic, A.L.; Klassen, A.F.; Scott, A.M.; Klok, J.A.; Cordeiro, P.G.; Cano, S.J. Development of a new patient reported outcome measure for breast surgery: The BREAST-Q. Plast. Reconstr. Surg. 2009, 124, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Cano, S.J.; Klassen, A.F.; Scott, A.M.; Pusic, A.L. A closer look at the BREAST-Q(©). Clin. Plast. Surg. 2013, 40, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Vrouwe, S.Q.; Somogyi, R.B.; Snell, L.; McMillan, C.; Vespirini, D.; Lipa, J.E. Patient-reported outcomes following breast conservation therapy and barriers to referral for partial breast reconstruction. Plast. Reconstr. Surg. 2018, 141, 1–9. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, R.L.; DiMicco, R.; Khabra, K.; O’Flynn, E.A.; de Souza, N.; Roche, N.; Barry, P.A.; Kirby, A.M.; Rusby, J.E. Initial experience of the BREAST-Q breast-conserving therapy module. Breast. Cancer. Res. Treat. 2016, 160, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Lagendijk, M.; van Egdom, L.S.E.; van Veen, F.E.E.; Vos, E.L.; Mureau, M.A.M.; van Leeuwen, N.; Hazelzet, J.A.; Lingsma, H.F.; Koppert, L.B. Patient-reported outcome measures may add value in breast cancer surgery. Ann. Surg. Oncol. 2018, 25, 3563–3571. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.D.; Kim, Z.; Kuk, J.C.; Jeong, J.; Choi, K.S.; Hur, S.M.; Jeong, G.A.; Chung, J.C.; Cho, G.S.; Shin, E.J.; et al. Long-term results of oncoplastic breast surgery with latissimus dorsi flap reconstruction: A pilot study of the objective cosmetics results and patient reported outcome. Ann. Surg. Treat. Res. 2016, 90, 117–123. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Flanagan, M.R.; Zabor, E.C.; Romanoff, A.; Fuzesi, S.; Stempel, M.; Mehrara, B.J.; Morrow, M.; Pusic, A.L.; Gemignani, M.L. A comparison of patient-reported outcomes after breast-conserving surgery and mastectomy with implant breast reconstruction. Ann. Surg. Oncol. 2019, 26, 3133–3140. [Google Scholar] [CrossRef] [PubMed]
- Atisha, D.M.; Tessiatore, K.M.; Rushing, C.N.; Dayicioglu, D.; Pusic, A.; Hwang, S. A national snapshot of patient-reported outcomes comparing types of abdominal flaps for breast reconstruction. Plast. Reconstr. Surg. 2019, 143, 667–677. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Socio-Demographic and Clinical Characteristics | % | n | |
|---|---|---|---|
| Place of residence | country | 30.8 | 28 |
| city<100 thousand citizens | 41.8 | 38 | |
| city>100 thousand citizens | 27.4 | 25 | |
| Marital status | married | 78.0 | 71 |
| single | 4.4 | 4 | |
| widowed | 9.9 | 9 | |
| divorced | 5.5 | 5 | |
| informal relationship | 2.2 | 2 | |
| Education | primary | 2.1 | 2 |
| vocational | 20.9 | 19 | |
| secondary | 44.0 | 40 | |
| higher | 33.0 | 30 | |
| Hormonal status | post-menopausal | 73.6 | 67 |
| pre-menopausal | 26.4 | 24 | |
| Brest cancer | right | 57.1 | 52 |
| left | 42.9 | 39 | |
| Histological type of cancer | no special type (NST) | 82.4 | 75 |
| invasive lobular carcinoma (ILC) | 3.3 | 3 | |
| ductal carcinoma in situ (DCIS) | 7.7 | 7 | |
| other (tubular, medullary, mucous) | 6.6 | 6 | |
| Scope of surgical operations within regional lymph nodes | SLNB | 83.5 | 76 |
| ALND | 12.1 | 11 | |
| no | 4.4 | 4 | |
| Breast-Q BCT Domain | Observation Period | M | SD | −95% | +95% | n | Min | Max |
|---|---|---|---|---|---|---|---|---|
| SwB | before operation | 56.0 | 11.9 | 53.5 | 58.5 | 91 | 29 | 100 |
| SwO | 3 months after | 63.0 | 13.2 | 60.2 | 65.7 | 91 | 27 | 100 |
| 6 months after | 61.8 | 11.0 | 59.5 | 64.1 | 91 | 43 | 100 | |
| 12 months after | 62.2 | 12.7 | 59.4 | 64.9 | 83 | 41 | 100 | |
| Psych-soc W-B | before operation | 62.0 | 14.2 | 59.0 | 65.0 | 91 | 34 | 100 |
| 3 months after | 66.2 | 17.2 | 62.6 | 69.8 | 91 | 32 | 100 | |
| 6 months after | 65.9 | 15.4 | 62.7 | 69.1 | 91 | 35 | 100 | |
| 12 months after | 68.4 | 16.5 | 64.8 | 72.0 | 83 | 36 | 100 | |
| Physical W-B | before operation | 69.9 | 8.6 | 68.1 | 71.7 | 91 | 50 | 80 |
| 3 months after | 67.9 | 14.9 | 64.8 | 71.0 | 91 | 34 | 100 | |
| 6 months after | 67.5 | 15.1 | 64.4 | 70.6 | 91 | 25 | 100 | |
| 12 months after | 67.9 | 15.4 | 64.5 | 71.2 | 83 | 0 | 100 |
| Breast-Q BCT Domain | Observation Period | M | SD | −95% | +95% | Min | Max | ANOVA Friedman | |
|---|---|---|---|---|---|---|---|---|---|
| Chi 2 | p | ||||||||
| SwB | before operation | 55.0 | 10.2 | 52.7 | 57.2 | 29 | 100 | 40.592 1 | <0.001 1 |
| SwO | 3 months after | 62.6 | 12.7 | 59.8 | 65.4 | 39 | 100 | ||
| 6 months after | 61.4 | 11.1 | 59.0 | 63.8 | 43 | 100 | |||
| 12 months after | 62.2 | 12.7 | 59.4 | 64.9 | 41 | 100 | 0.591 2 | >0.05 2 | |
| Psych-soc W-B | before operation | 61.6 | 13.8 | 58.6 | 64.6 | 34 | 93 | ||
| 3 months after | 66.4 | 17.3 | 62.7 | 70.2 | 32 | 100 | 17.214 1 | <0.001 1 | |
| 6 months after | 66.4 | 15.1 | 63.1 | 69.7 | 35 | 100 | |||
| 12 months after | 68.4 | 16.5 | 64.8 | 72.0 | 36 | 100 | 2.9472 | >0.05 2 | |
| Physical W-B | before operation | 70.4 | 8.6 | 68.5 | 72.2 | 53 | 80 | ||
| 3 months after | 69.2 | 14.5 | 66.1 | 72.4 | 34 | 100 | 1.630 1 | >0.05 1 | |
| 6 months after | 68.3 | 15.0 | 65.0 | 71.6 | 25 | 100 | |||
| 12 months after | 67.9 | 15.4 | 64.5 | 71.2 | 0 | 100 | 1.047 2 | >0.05 2 | |
| Breast-Q BCT Domain | Observation Period | n | R | T (n−2) | p |
|---|---|---|---|---|---|
| SwB vs. Psych-soc W-B | before operation | 91 | 0.410 | 4.243 | <0.001 |
| SwO vs. Psych-soc W-B | 3 months after | 91 | 0.502 | 5.477 | <0.001 |
| 6 months after | 91 | 0.447 | 4.721 | <0.001 | |
| 12 months after | 83 | 0.516 | 5.421 | <0.001 | |
| SwB vs. Physical W-B | before operation | 91 | 0.048 | 0.454 | >0.05 |
| SwO vs. Physical W-B | 3 months after | 91 | 0.097 | 0.916 | >0.05 |
| 6 months after | 91 | 0.056 | 0.526 | >0.05 | |
| 12 months after | 83 | 0.064 | 0.574 | >0.05 | |
| Psych-soc W-B vs. Physical W-B | before operation | 91 | −0.099 | −0.937 | >0.05 |
| Psych-soc W-B vs. Physical W-B | 3 months after | 91 | 0.215 | 2.077 | <0.05 |
| 6 months after | 91 | 0.236 | 2.294 | <0.05 | |
| 12 months after | 83 | 0.189 | 1.730 | >0.05 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krzos, A.; Stanisławek, A.; Jędrych, M.; Łuczyk, M.; Ślusarska, B. Satisfaction with the Aesthetic Effect and Quality of Life for Women after Breast Conserving Therapy (BCT)—Preliminary Research. Int. J. Environ. Res. Public Health 2019, 16, 4682. https://doi.org/10.3390/ijerph16234682
Krzos A, Stanisławek A, Jędrych M, Łuczyk M, Ślusarska B. Satisfaction with the Aesthetic Effect and Quality of Life for Women after Breast Conserving Therapy (BCT)—Preliminary Research. International Journal of Environmental Research and Public Health. 2019; 16(23):4682. https://doi.org/10.3390/ijerph16234682
Chicago/Turabian StyleKrzos, Agata, Andrzej Stanisławek, Marian Jędrych, Marta Łuczyk, and Barbara Ślusarska. 2019. "Satisfaction with the Aesthetic Effect and Quality of Life for Women after Breast Conserving Therapy (BCT)—Preliminary Research" International Journal of Environmental Research and Public Health 16, no. 23: 4682. https://doi.org/10.3390/ijerph16234682
APA StyleKrzos, A., Stanisławek, A., Jędrych, M., Łuczyk, M., & Ślusarska, B. (2019). Satisfaction with the Aesthetic Effect and Quality of Life for Women after Breast Conserving Therapy (BCT)—Preliminary Research. International Journal of Environmental Research and Public Health, 16(23), 4682. https://doi.org/10.3390/ijerph16234682