Incidence of Cellulitis Following Acupuncture Treatments in Taiwan

 ,
,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Data Source
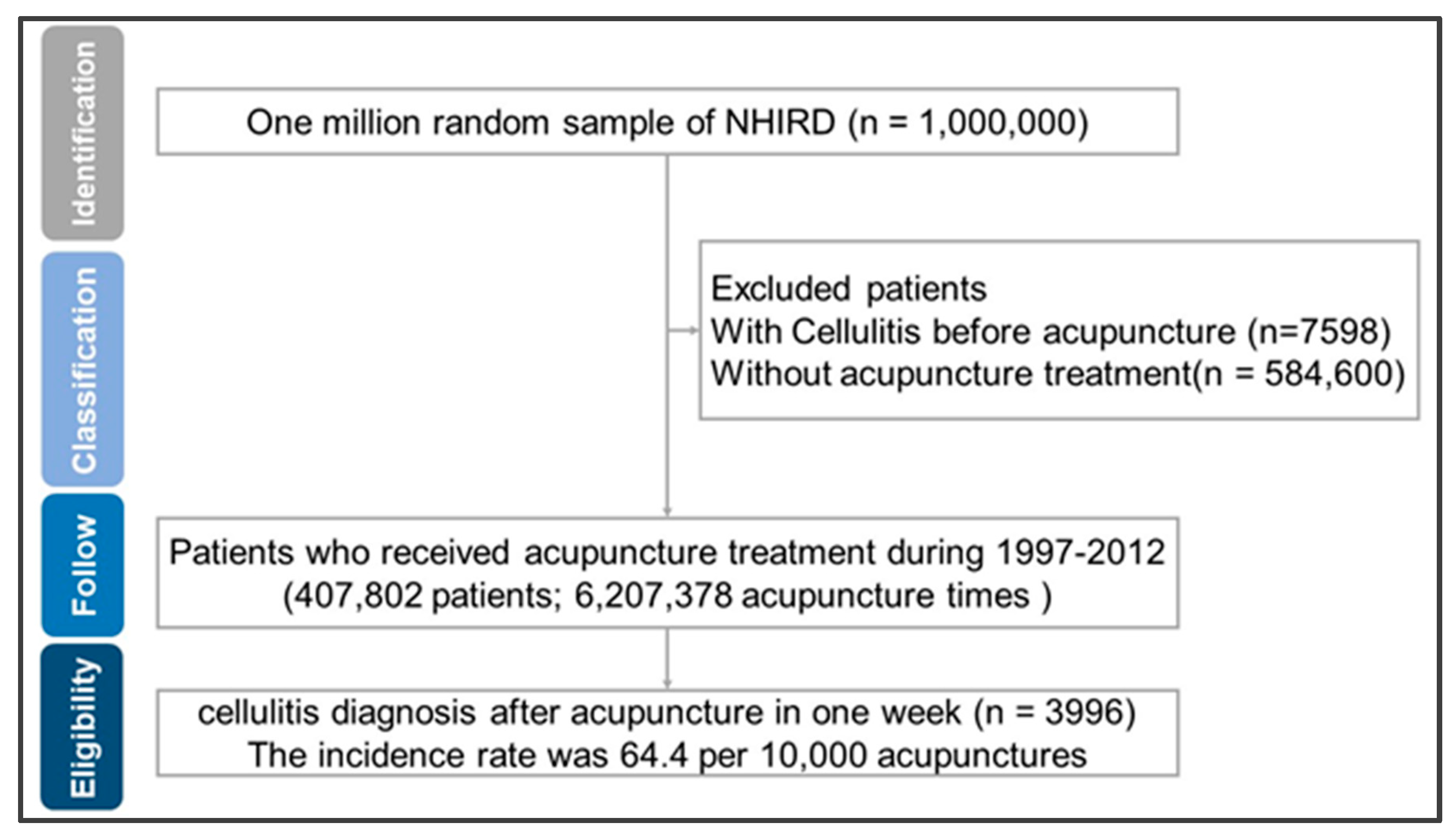
2.2. Study Population
2.3. Cellulitis after Acupuncture
2.4. Possible Confounder
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- White, A.; Hayhoe, S.; Hart, A.; Ernst, E.; Volunteers from BMAS and AACP. British Medical Acupuncture Society and Acupuncture Association of Chartered Physiotherapists. Survey of adverse events following acupuncture (SAFA): A prospective study of 32,000 consultations. Acupunct. Med. 2001, 19, 84–92. [Google Scholar] [CrossRef]
- Kim, Y.J.; Kim, S.H.; Lee, H.J.; Kim, W.Y. Infectious Adverse Events Following Acupuncture: Clinical Progress and Microbiological Etiology. J. Korean Med. Sci. 2018, 33, e164. [Google Scholar] [CrossRef]
- Witt, C.M.; Pach, D.; Brinkhaus, B.; Wruck, K.; Tag, B.; Mank, S.; Willich, S.N. Safety of acupuncture: Results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Complement. Med. Res. 2009, 16, 91–97. [Google Scholar] [CrossRef] [PubMed]
- MacPherson, H.; Thomas, K.; Walters, S.; Fitter, M. A prospective survey of adverse events and treatment reactions following 34,000 consultations with professional acupuncturists. Acupunct. Med. 2001, 19, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Wang, L.; Cooper, E.; Zhang, M.; Manheimer, E.; Berman, B.; Shen, X.; Lao, L. Adverse events of acupuncture: A systematic review of case reports. Evid. Based Complement. Alternat. Med. 2013, 581203. [Google Scholar] [CrossRef] [PubMed]
- Raff, A.B.; Kroshinsky, D. Cellulitis: A Review. JAMA 2016, 316, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.K.; Tsai, Y.T.; Lo, P.C.; Lai, J.N. Traditional Chinese medicine therapy decreases the pneumonia risk in patients with dementia. Medicine 2016, 95, e4917. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.K.; Yan, S.H.; Lai, J.N.; Tsai, T.H. Patterns of Chinese medicine use in prescriptions for treating Alzheimer’s disease in Taiwan. Chin. Med. 2016, 11, 12. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.K.; Lin, P.H.; Hsu, R.J.; Chuang, H.C.; Liu, J.M. Traditional Chinese medicine therapy reduces the catheter indwelling risk in dementia patients with difficult voiding symptoms. J. Ethnopharmacol. 2017, 203, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.J.; Tian, W.H.; Chen, C.C. Urbanization and the utilization of outpatient services under National Health Insurance in Taiwan. Health Policy 2011, 103, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.K.; Liu, J.M.; Chang, Y.H.; Ting, Y.T.; Pang, S.T.; Hsu, R.J.; Lin, P.H. Increased risk of endotracheal intubation and heart failure following acute myocardial infarction in patients with urolithiasis: A nationwide population-based study. Ther. Clin. Risk Manag. 2017, 13, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.C.; Lin, S.K.; Lai, J.N.; Wei, J.C.; Cheng, C.Y. The traditional Chinese medicine prescription patterns of Sjögren’s patients in Taiwan: A population-based study. J. Ethnopharmacol. 2014, 155, 435–442. [Google Scholar] [CrossRef] [PubMed]
- McNamara, D.R.; Tleyjeh, I.M.; Berbari, E.F.; Lahr, B.D.; Martinez, J.; Mirzoyev, S.A.; Baddour, L.M. A predictive model of recurrent lower extremity cellulitis in a population-based cohort. Arch. Intern. Med. 2007, 167, 709. [Google Scholar] [CrossRef] [PubMed]
- Baddour, L.M.; Bisno, A.L. Recurrent cellulitis after saphenous venectomy for coronary bypass surgery. Ann. Intern. Med. 1982, 97, 493. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Chen, Y.; Chen, B.; Wang, Y.; Huang, X.; Fan, X.G. Acupuncture-associated infections: A matter of concern in China. Infect. Control Hosp. Epidemiol. 2019, 40, 383–384. [Google Scholar] [CrossRef] [PubMed]
- Ekpanyapong, S.; Reddy, K.R. Infections in Cirrhosis. Curr. Treat. Opt. Gastroenterol. 2019, 17, 254–270. [Google Scholar] [CrossRef] [PubMed]
- Garcia Garcia de Paredes, A.; Tellez, L.; Rodriguez-Gandia, M.A.; Martinez, J.; Rodriguez de Santiago, E.; Aguilera Castro, L.; Gea, F.; Albillos, A. Incidence, predictive factors and impacts of acute kidney injury in cirrhotic patients hospitalized for cellulitis. Liver Int. 2018, 38, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Escalante, A.; Beardmore, T.D. Risk factors for early wound complications after orthopedic surgery for rheumatoid arthritis. J. Rheumatol. 1995, 22, 1844–1851. [Google Scholar] [CrossRef] [PubMed]
- Cannon, J.; Rajakaruna, G.; Dyer, J.; Carapetis, J.; Manning, L. Severe lower limb cellulitis: Defining the epidemiology and risk factors for primary episodes in a population-based case-control study. Clin. Microbiol. Infect. 2018, 24, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Mawanda, F.; Wallace, R.B.; McCoy, K.; Abrams, T.E. Systemic and localized extra-central nervous system bacterial infections and the risk of dementia among US veterans: A retrospective cohort study. Alzheimers Dement. 2016, 4, 109–117. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Cellulitis Patients No. (%) | All Patients without Cellulitis No. (%) | p-Value of Chi-Square Test | 1:4 Matching Patients without Cellulitis No. (%) | p-Value of Chi-Square Test |
|---|---|---|---|---|---|
| Total | 3996 (100.0%) | 407,802 (100.0%) | - | 15,984 (100.0%) | |
| Age at diagnosis | <0.0001 | 0.67 | |||
| <20 | 116 (2.9%) | 40,768 (10.0%) | - | 451 (2.8%) | |
| 20–40 | 859 (21.5%) | 157,152 (38.5%) | - | 3381 (21.2%) | |
| 40–60 | 1322 (33.1%) | 143,472 (35.2%) | - | 5271 (33.0%) | |
| ≥60 | 1699 (42.5%) | 66,410 (16.3%) | - | 6881 (43.0%) | |
| Gender | <0.0001 | 1.00 | |||
| Female | 1839 (46.0%) | 217,814 (53.4%) | - | 7356 (46.0%) | |
| Male | 2157 (54.0%) | 189,988 (46.6%) | - | 8628 (54.0%) | |
| Urbanization | <0.0001 | 0.75 | |||
| Very high | 1796 (44.9%) | 204,226 (50.1%) | - | 7152 (44.7%) | |
| High | 1015 (25.4%) | 103,250 (25.3%) | - | 3948 (24.7%) | |
| Moderate | 806 (20.2%) | 73,017 (17.9%) | - | 3316 (20.7%) | |
| Low | 379 (9.5%) | 27,309 (6.7%) | - | 1568 (9.8%) | |
| Insured amount (NT$) | <0.0001 | 0.79 | |||
| Dependent | 1035 (25.9%) | 155,239 (38.1%) | - | 4039 (25.3%) | |
| $1–19,999 | 2153 (53.9%) | 161,563 (39.6%) | - | 8382 (52.4%) | |
| $20,000–39,999 | 573 (14.3%) | 61,244 (15.0%) | - | 2231 (14.0%) | |
| ≥$40,000 | 235 (5.9%) | 29,756 (7.3%) | - | 1332 (8.3%) | |
| Comorbidity | - | ||||
| Chronic kidney disease | 607 (15.2%) | 15,947 (3.9%) | <0.0001 | 1343 (8.4%) | <0.05 |
| Autoimmune diseases | 666 (16.7%) | 28,473 (7.0%) | <0.0001 | 1522 (9.5%) | <0.05 |
| Liver Cirrhosis | 277 (6.9%) | 7298 (1.8%) | <0.0001 | 687 (4.3%) | <0.05 |
| Diabetes mellitus | 1755 (43.9%) | 77,716 (19.1%) | <0.0001 | 3596 (22.5%) | <0.05 |
| Dementia | 447 (11.2%) | 12,407 (3.0%) | <0.0001 | 975 (6.1%) | <0.05 |
| Parkinson’s disease | 218 (5.5%) | 6551 (1.6%) | <0.0001 | 1646 (10.3%) | <0.05 |
| Stroke | 750 (18.8%) | 23,311 (5.7%) | <0.0001 | 751 (4.7%) | <0.05 |
| Varicose veins | 247 (6.2%) | 6333 (1.6%) | <0.0001 | 943 (5.9%) | <0.05 |
| Heart failure | 751 (18.8%) | 19,320 (4.7%) | <0.0001 | 2270 (14.2%) | <0.05 |
| Acupuncture treatment courses | <0.0001 | 0.81 | |||
| <6 | 1567 (39.2%) | 247,625 (60.7%) | - | 6251 (39.1%) | |
| 6–30 | 1546 (38.7%) | 121,621 (29.8%) | - | 6172 (38.6%) | |
| ≥30 | 883 (22.1%) | 38,556 (9.5%) | - | 3561 (22.3%) | |
| Variables | Odds Ratio (95% Confidence Interval) | ||
|---|---|---|---|
| Crude Odds Ratio | Adjusted Model 1 | Adjusted Model 2 | |
| Age at diagnosis | |||
| <20 | [Reference] | [Reference] | [Reference] |
| 20–40 | 1.92 (1.58–2.33) * | 1.62 (1.33–1.98) * | 1.62 (1.32–1.97) * |
| 40–60 | 3.24 (2.68–3.92) * | 1.98 (1.61–2.44) * | 1.98 (1.60–2.43) * |
| ≥60 | 8.99 (7.45–10.86) * | 2.90 (2.34–3.58) * | 2.89 (2.34–3.58) * |
| Gender | |||
| Female | [Reference] | [Reference] | [Reference] |
| Male | 1.35 (1.26–1.43) * | 1.57 (1.47–1.68) * | 1.57 (1.47–1.68) * |
| Urbanization | |||
| Very high | [Reference] | [Reference] | [Reference] |
| High | 1.13 (1.04–1.22) * | 1.09 (1.01–1.18) * | 1.08 (1.06–1.17) * |
| Moderate | 1.26 (1.16–1.37) * | 1.19 (1.09–1.30) * | 1.19 (1.09–1.29) * |
| Low | 1.59 (1.42–1.78) * | 1.35 (1.20–1.51) * | 1.35 (1.20–1.51) * |
| Insured amount (NT$) | |||
| Dependent | [Reference] | [Reference] | [Reference] |
| $1–19,999 | 2.00 (1.86–2.15) * | 1.18 (1.09–1.29) * | 1.18 (1.08–1.28) * |
| $20,000–39,999 | 1.40 (1.27–1.56) * | 0.92 (0.82–1.03) | 0.91 (0.81–1.02) |
| $≥40,000 | 1.19 (1.03–1.37) * | 0.73 (0.63–0.85) * | 0.73 (0.62–0.85) * |
| Comorbidity | |||
| Chronic kidney disease | 1.87 (1.70–2.06) * | 1.67 (1.51–1.84) * | 1.66 (1.51–1.84) * |
| Autoimmune diseases | 1.36 (1.10–1.68) * | 1.41 (1.28–1.54) * | 1.39 (1.27–1.53) * |
| Liver Cirrhosis | 2.31 (2.03–2.63) * | 2.05 (1.80–2.34) * | 2.05 (1.80–2.34) * |
| Diabetes mellitus | 1.98 (1.85–2.12) * | 1.72 (1.59–1.85) * | 1.71 (1.59–1.84) * |
| Dementia | 1.50 (1.34–1.69) * | 1.35 (1.21–1.52) * | 1.35 (1.20–1.52) * |
| Parkinson’s disease | 1.11 (0.95–1.29) * | 1.00 (0.86–1.17) | 0.99 (0.85–1.16) |
| Stroke | 1.69 (1.54–1.85) * | 1.45 (1.32–1.59) * | 1.44 (1.31–1.58) * |
| Varicose veins | 2.58 (2.25–2.96) * | 2.48 (2.16–2.85) * | 2.48 (2.16–2.85) * |
| Heart failure | 2.03 (1.86–2.23) * | 1.77 (1.61–1.94) * | 1.76 (1.60–1.93) * |
| Acupuncture treatment courses | |||
| <6 | [Reference] | [Reference] | [Reference] |
| 6–30 | 1.84 (1.72–1.98) * | 1.79 (1.67–1.93) * | 1.79 (1.66–1.92) * |
| ≥30 | 2.80 (2.58–3.05) * | 2.69 (2.47–2.93) * | 2.68 (2.46–2.93) * |
| Comorbidity | Odds Ratio (95% Confidence Interval) | |
|---|---|---|
| Crude Odds Ratio | Adjusted Odds Ratio | |
| Chronic kidney disease | 1.84 (1.67–2.03) * | 1.62 (1.47–1.79) * |
| Autoimmune diseases | 1.44 (1.22–1.70) * | 1.38 (1.17–1.62) * |
| Liver Cirrhosis | 2.26 (1.98–2.57) * | 2.00 (1.75–2.28) * |
| Diabetes mellitus | 2.06 (1.92–2.21) * | 1.71 (1.59–1.84) * |
| Dementia | 1.49 (1.33–1.67) * | 1.32 (1.18–1.48) * |
| Parkinson’s disease | 1.14 (0.98–1.33) | 1.02 (0.87–1.19) |
| Stroke | 1.75 (1.60–1.92) * | 1.47 (1.34–1.62) * |
| Varicose veins | 2.74 (2.39–3.13) * | 2.55 (2.22–2.92) * |
| Heart failure | 2.02 (1.84–2.22) * | 1.71 (1.56–1.88) * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, S.-K.; Liu, J.-M.; Wang, P.-H.; Hung, S.-P.; Hsu, R.-J.; Chuang, H.-C.; Lin, P.-H. Incidence of Cellulitis Following Acupuncture Treatments in Taiwan. Int. J. Environ. Res. Public Health 2019, 16, 3831. https://doi.org/10.3390/ijerph16203831
Lin S-K, Liu J-M, Wang P-H, Hung S-P, Hsu R-J, Chuang H-C, Lin P-H. Incidence of Cellulitis Following Acupuncture Treatments in Taiwan. International Journal of Environmental Research and Public Health. 2019; 16(20):3831. https://doi.org/10.3390/ijerph16203831
Chicago/Turabian StyleLin, Shun-Ku, Jui-Ming Liu, Pin-Hsuan Wang, Sheng-Ping Hung, Ren-Jun Hsu, Heng-Chang Chuang, and Po-Hung Lin. 2019. "Incidence of Cellulitis Following Acupuncture Treatments in Taiwan" International Journal of Environmental Research and Public Health 16, no. 20: 3831. https://doi.org/10.3390/ijerph16203831
APA StyleLin, S.-K., Liu, J.-M., Wang, P.-H., Hung, S.-P., Hsu, R.-J., Chuang, H.-C., & Lin, P.-H. (2019). Incidence of Cellulitis Following Acupuncture Treatments in Taiwan. International Journal of Environmental Research and Public Health, 16(20), 3831. https://doi.org/10.3390/ijerph16203831