The Relationship between Childhood Maltreatment and Risky Sexual Behaviors: A Meta-Analysis

Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Exposure and Outcome Indicators of Interest
2.3. Inclusion Criteria
2.4. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
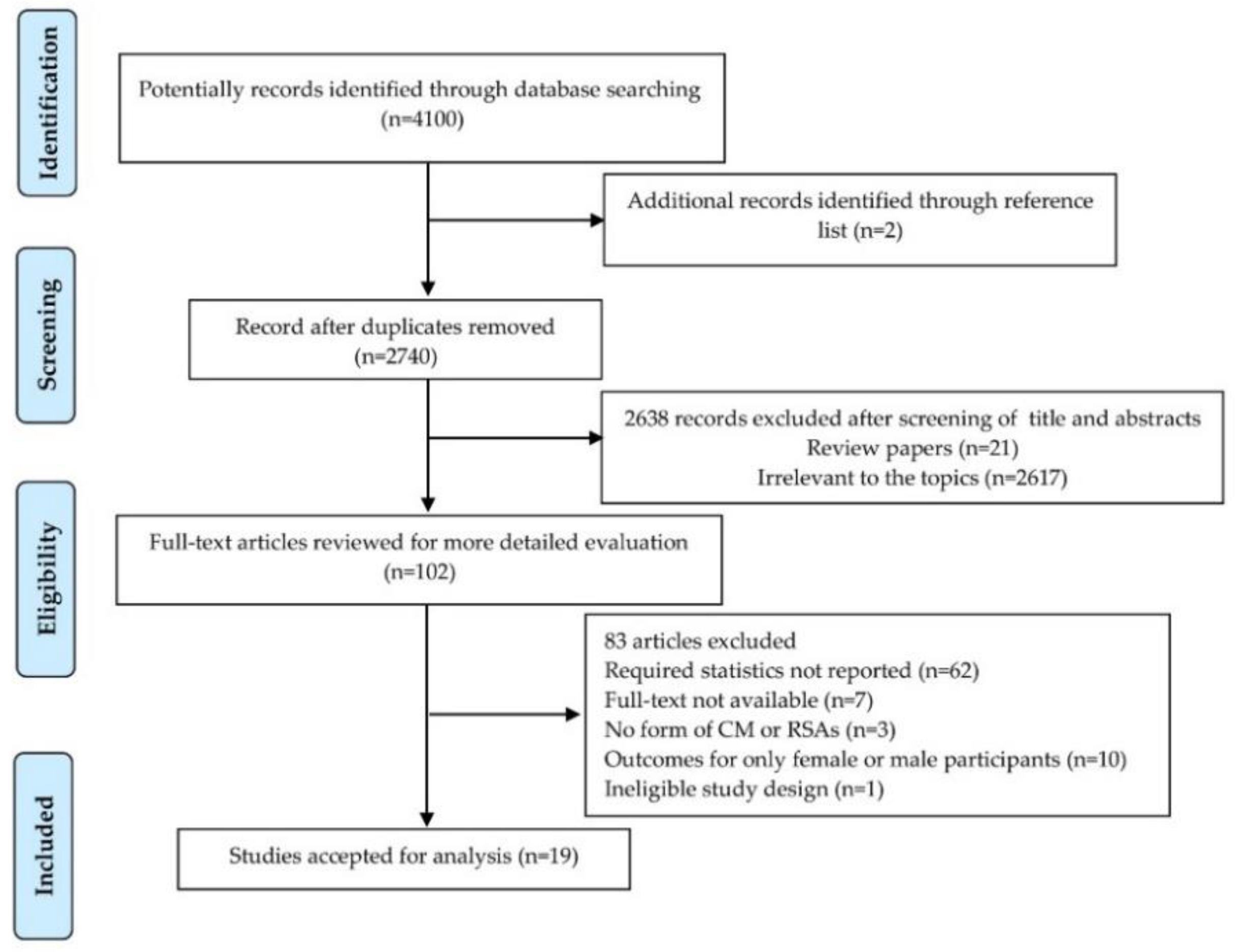
3.1. Search Results and Study Characteristics
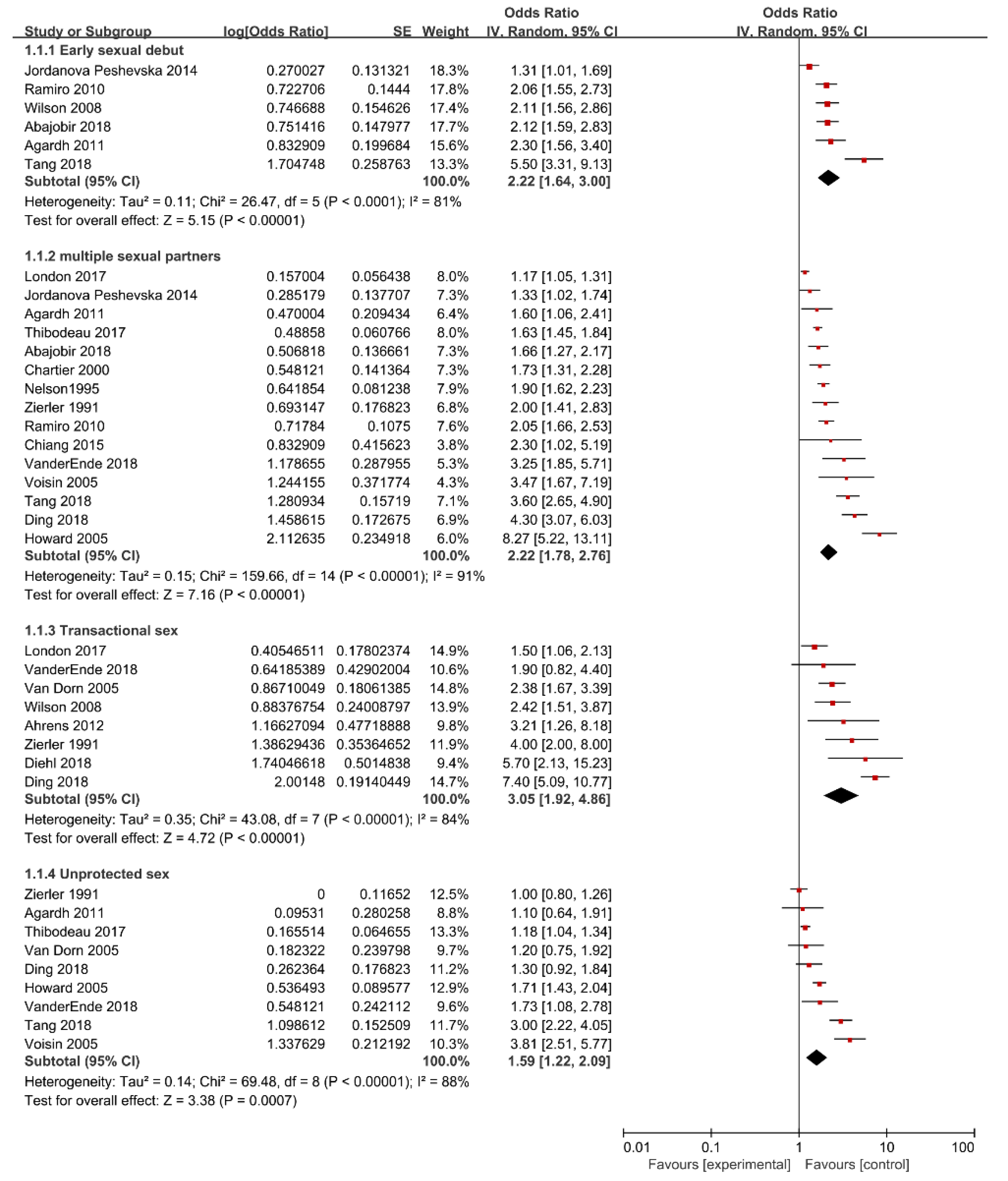
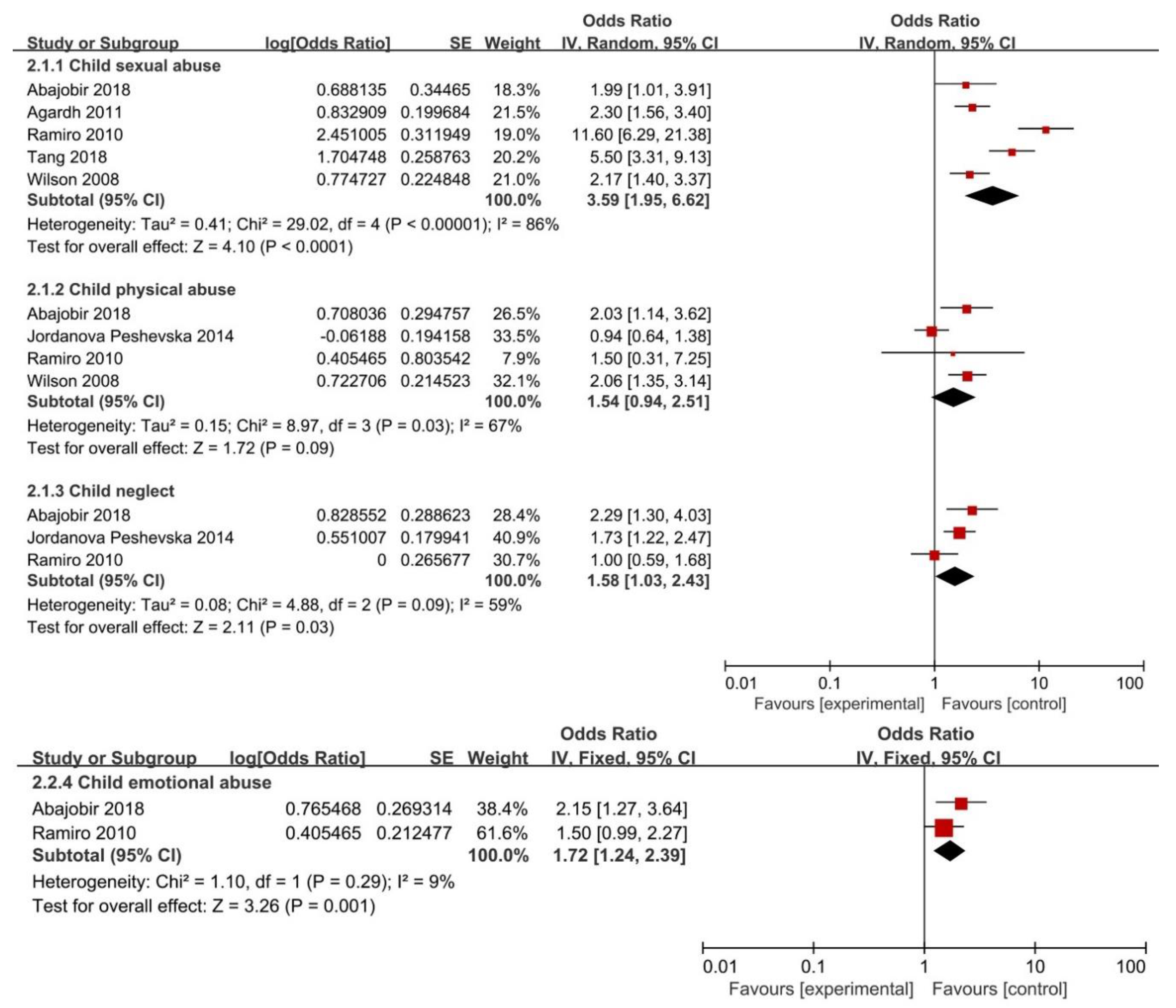
3.2. Childhood Maltreatment and Risk of Having an Early Sexual Debut
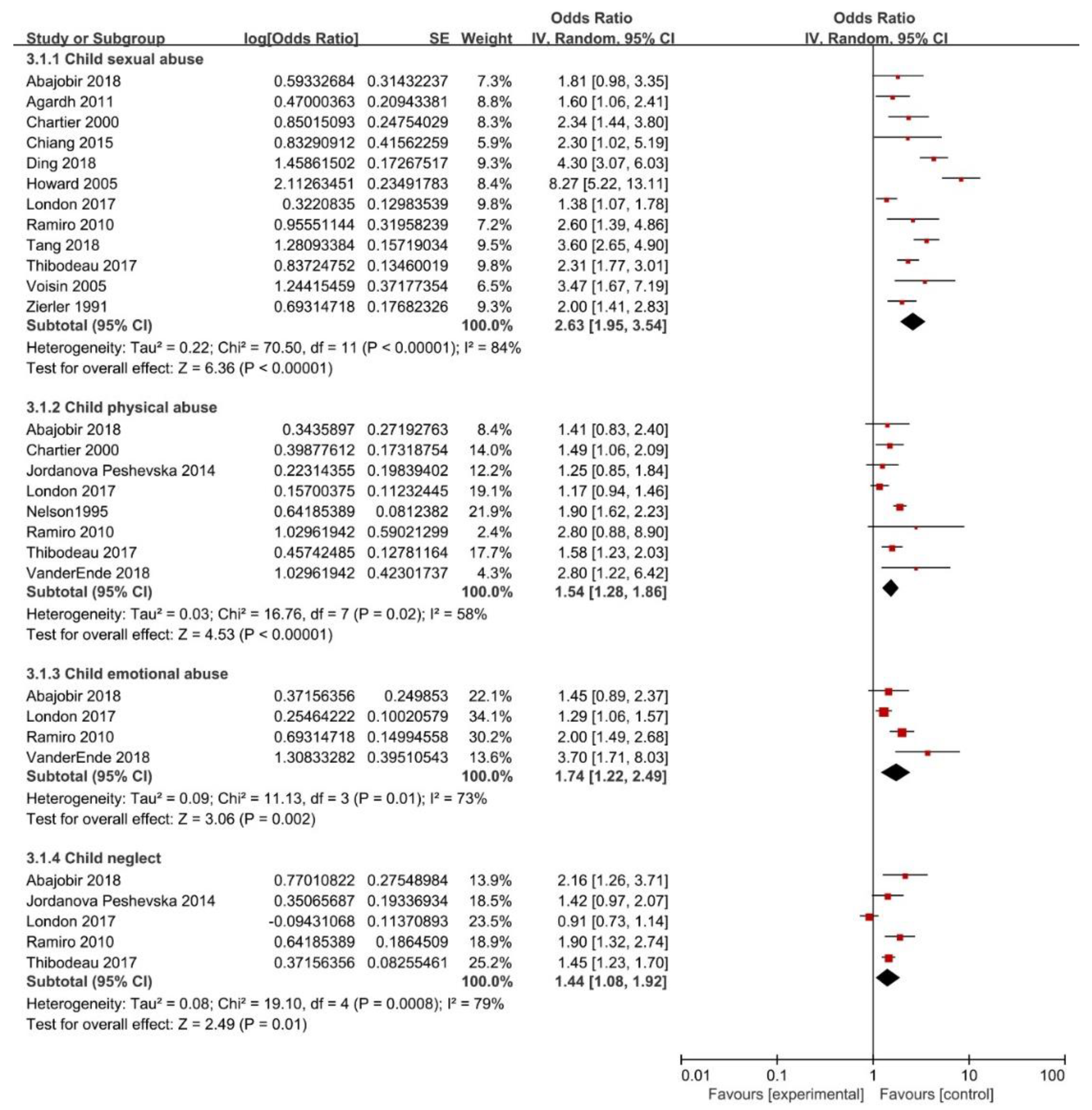
3.3. Childhood Maltreatment and Risk of Having Multiple Sexual Partners
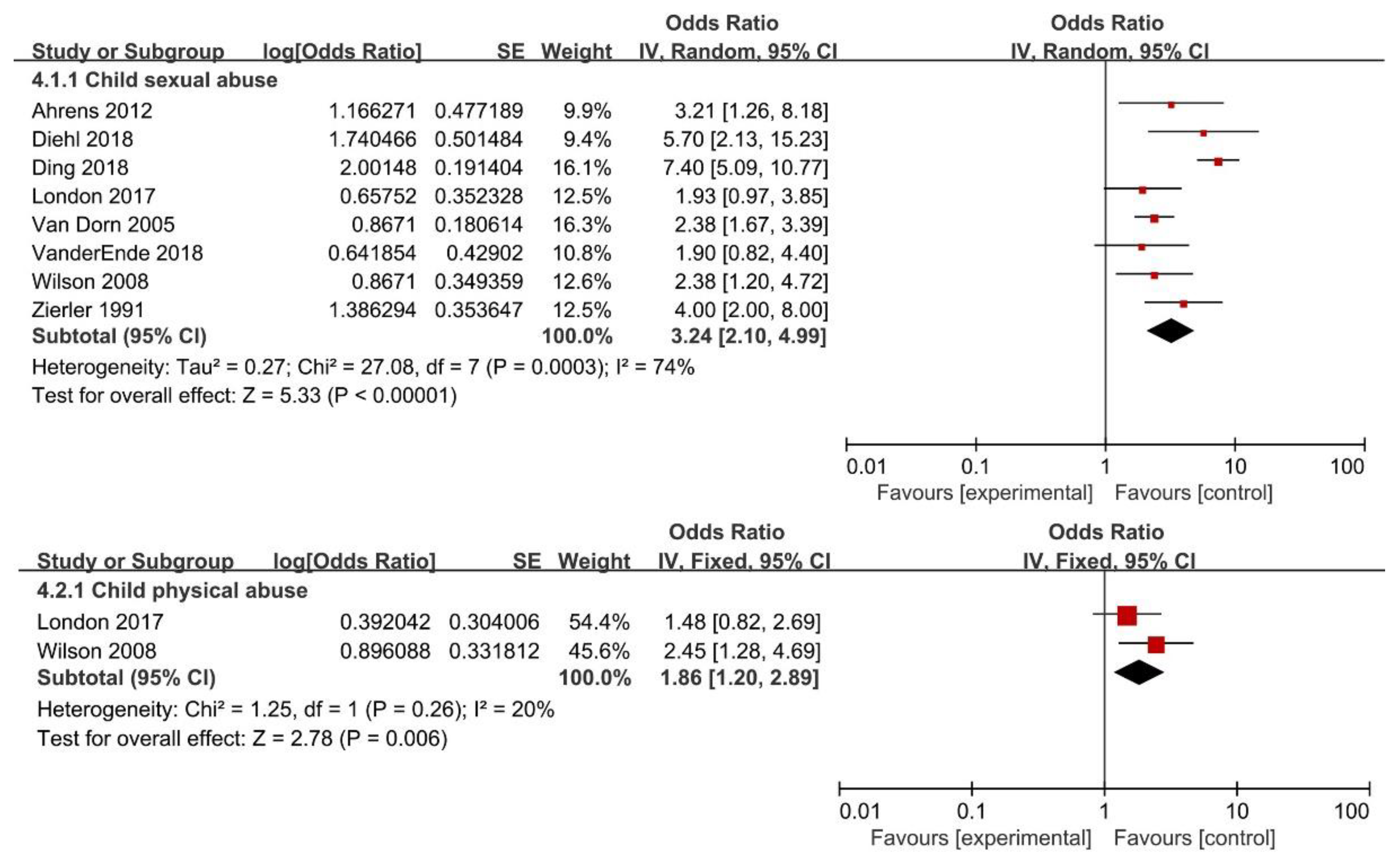
3.4. Childhood Maltreatment and Risk of Having Transactional Sex
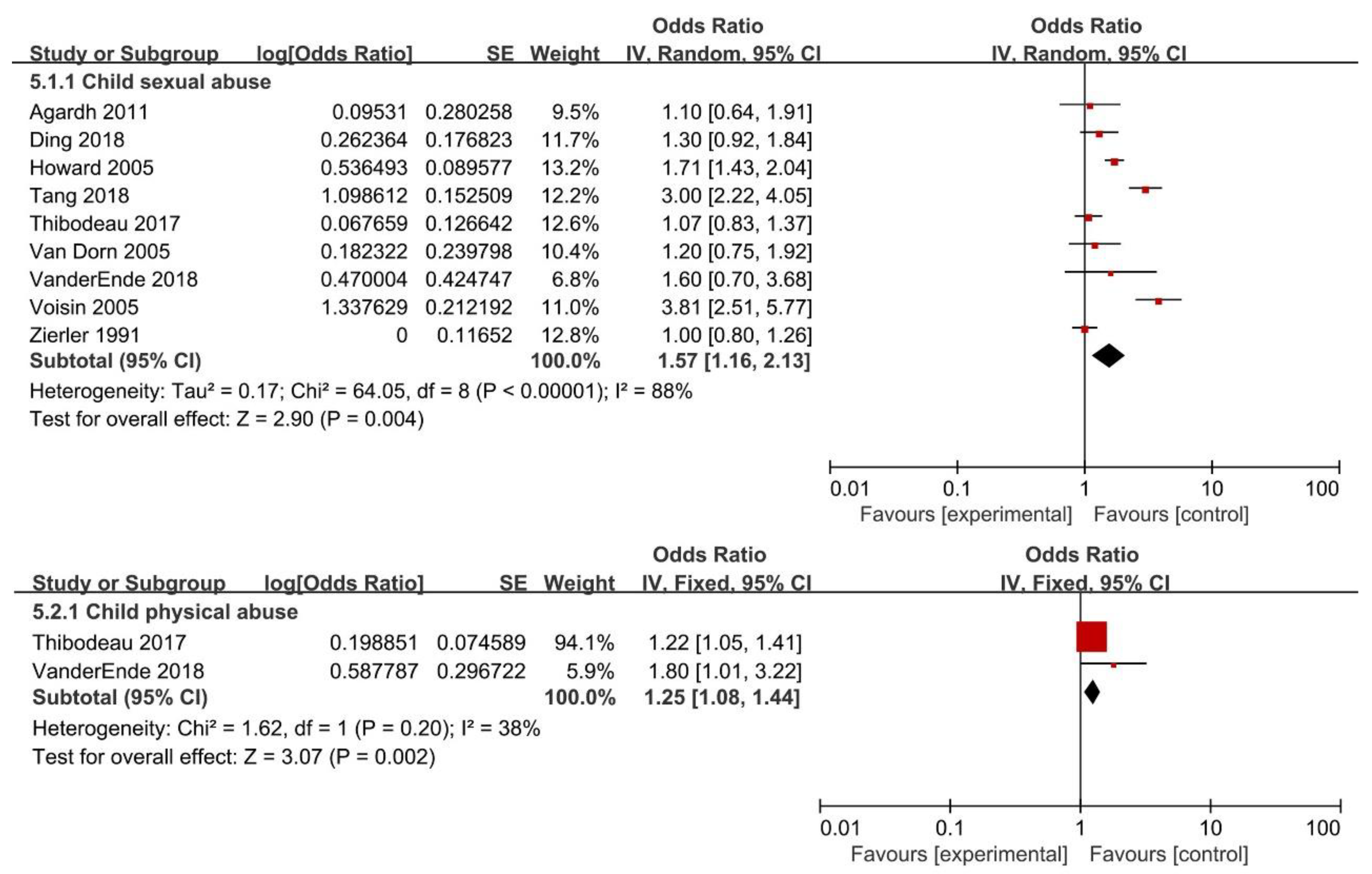
3.5. Childhood Maltreatment and Risk of Having Unprotected Sex
3.6. Subgroup Analysis
3.7. Sensitivity Analysis
3.8. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Norman, R.E.; Byambaa, M.; De, R.; Butchart, A.; Scott, J.; Vos, T. The long-term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta-analysis. PLoS Med. 2012, 9, e1001349. [Google Scholar] [CrossRef] [PubMed]
- Finkelhor, D.; Turner, H.A.; Shattuck, A.; Hamby, S.L. Prevalence of Childhood Exposure to Violence, Crime, and Abuse: Results From the National Survey of Children’s Exposure to Violence. JAMA Pediatr. 2015, 169, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, R.; Widom, C.S.; Browne, K.; Fergusson, D.; Webb, E.; Janson, S. Burden and consequences of child maltreatment in high-income countries. Lancet 2009, 373, 68–81. [Google Scholar] [CrossRef]
- Tran, B.X.; Pham, T.V.; Ha, G.H.; Ngo, A.T.; Nguyen, L.H.; Vu, T.T.M.; Do, H.N.; Nguyen, V.; Nguyen, A.T.L.; Tran, T.T.; et al. A Bibliometric Analysis of the Global Research Trend in Child Maltreatment. Int. J. Environ. Res. Public Health 2018, 15, 1456. [Google Scholar] [CrossRef] [PubMed]
- Jaffee, S.R. Child Maltreatment and Risk for Psychopathology in Childhood and Adulthood. Annu. Rev. Clin. Psychol. 2017, 13, 525–551. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Feng, T.; Qin, J.; Wang, T.; Wu, X.; Cai, Y.; Lan, L.; Yang, T. Reported prevalence of childhood maltreatment among Chinese college students: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0205808. [Google Scholar] [CrossRef]
- Nelson, J.; Klumparendt, A.; Doebler, P.; Ehring, T. Childhood maltreatment and characteristics of adult depression: Meta-analysis. Br. J. Psychiatry J. Ment. Sci. 2017, 210, 96–104. [Google Scholar] [CrossRef]
- Clayton, K.; Lee, J.B.; Cheung, K.; Theule, J.; Henrikson, B. Quantifying the Relationship between Attention-Deficit/Hyperactivity Disorder and Experiences of Child Maltreatment: A Meta-Analysis. Child Abus. Rev. 2018, 27, 361–377. [Google Scholar] [CrossRef]
- Abajobir, A.A.; Kisely, S.; Williams, G.; Strathearn, L.; Najman, J.M. Risky Sexual Behaviors and Pregnancy Outcomes in Young Adulthood Following Substantiated Childhood Maltreatment: Findings From a Prospective Birth Cohort Study. J. Sex Res. 2018, 55, 106–119. [Google Scholar] [CrossRef]
- Abajobir, A.A.; Kisely, S.; Scott, J.G.; Williams, G.; Clavarino, A.; Strathearn, L.; Najman, J.M. Childhood Maltreatment and Young Adulthood Hallucinations, Delusional Experiences, and Psychosis: A Longitudinal Study. Schizophr. Bull. 2017, 43, 1045–1055. [Google Scholar] [CrossRef]
- Yoon, S.; Voith, L.A.; Kobulsky, J.M. Gender differences in pathways from child physical and sexual abuse to adolescent risky sexual behavior among high-risk youth. J. Adolesc. 2018, 64, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Fowler, P.J.; Motley, D.; Zhang, J.; Rolls-Reutz, J.; Landsverk, J. Adolescent maltreatment in the child welfare system and developmental patterns of sexual risk behaviors. Child Maltreatment 2015, 20, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Ramiro, L.S.; Madrid, B.J.; Brown, D.W. Adverse childhood experiences (ACE) and health-risk behaviors among adults in a developing country setting. Child Abus. Negl. 2010, 34, 842–855. [Google Scholar] [CrossRef] [PubMed]
- Hahm, H.C.; Lee, Y.; Ozonoff, A.; Van Wert, M.J. The impact of multiple types of child maltreatment on subsequent risk behaviors among women during the transition from adolescence to young adulthood. J. Youth Adolesc. 2010, 39, 528–540. [Google Scholar] [CrossRef] [PubMed]
- VanderEnde, K.; Chiang, L.; Mercy, J.; Shawa, M.; Hamela, J.; Maksud, N.; Gupta, S.; Wadonda-Kabondo, N.; Saul, J.; Gleckel, J.; et al. Adverse Childhood Experiences and HIV Sexual Risk-Taking Behaviors Among Young Adults in Malawi. J. Interpers. Violence 2018, 33, 1710–1730. [Google Scholar] [CrossRef] [PubMed]
- Thibodeau, M.E.; Lavoie, F.; Hebert, M.; Blais, M. Pathways Linking Childhood Maltreatment and Adolescent Sexual Risk Behaviors: The Role of Attachment Security. J. Sex Res. 2017, 54, 994–1005. [Google Scholar] [CrossRef]
- Abdala, N.; Li, F.; Shaboltas, A.V.; Skochilov, R.V.; Krasnoselskikh, T.V. History of Childhood Abuse, Drinking Motives, Alcohol Use, and Sexual Risk Behavior Among STD Clinic Patients in St. Petersburg, Russia: A Cross-Sectional Study. AIDS Behav. 2016, 20, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.J.; Lewis, T.; Litrownik, A.; Thompson, R.; Proctor, L.J.; Isbell, P.; Dubowitz, H.; English, D.; Jones, B.; Nagin, D.; et al. Linking childhood sexual abuse and early adolescent risk behavior: The intervening role of internalizing and externalizing problems. J. Abnorm. Child Psychol. 2013, 41, 139–150. [Google Scholar] [CrossRef]
- Senn, T.E.; Carey, M.P. Child maltreatment and women’s adult sexual risk behavior: Childhood sexual abuse as a unique risk factor. Child Maltreatment 2010, 15, 324–335. [Google Scholar] [CrossRef]
- Chartier, M.J.; Walker, J.R.; Naimark, B. Health Risk Behaviors and Mental Health Problems as Mediators of the Relationship between Childhood Abuse and Adult Health. Am. J. Public Health 2009, 99, 847–854. [Google Scholar] [CrossRef]
- Tomori, C.; McFall, A.M.; Srikrishnan, A.K.; Mehta, S.H.; Nimmagadda, N.; Anand, S.; Vasudevan, C.K.; Solomon, S.; Solomon, S.S.; Celentano, D.D. The prevalence and impact of childhood sexual abuse on HIV-risk behaviors among men who have sex with men (MSM) in India. BMC Public Health 2016, 16, 784. [Google Scholar] [CrossRef] [PubMed]
- Wekerle, C.; Goldstein, A.L.; Tanaka, M.; Tonmyr, L. Childhood sexual abuse, sexual motives, and adolescent sexual risk-taking among males and females receiving child welfare services. Child Abus. Negl. 2017, 66, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Diehl, A.; Clemente, J.; Pillon, S.C.; Santana, P.R.H.; da Silva, C.J.; Mari, J.J. Early childhood maltreatment experience and later sexual behavior in Brazilian adults undergoing treatment for substance dependence. Rev. Bras. Psiquiatr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.; Qu, X.; Li, C.; Tan, S. Childhood sexual abuse, risky sexual behaviors and adverse reproductive health outcomes among Chinese college students. Child Abus. Negl. 2018, 84, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.K.; Wilton, L.; Magnus, M.; Wang, L.; Wang, J.; Dyer, T.P.; Koblin, B.A.; Hucks-Ortiz, C.; Fields, S.D.; Shoptaw, S.; et al. Relation of Childhood Sexual Abuse, Intimate Partner Violence, and Depression to Risk Factors for HIV among Black Men Who Have Sex with Men in 6 US Cities. Am. J. Public Health 2015, 105, 2473–2481. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.P.; Kingree, J.B.; Lamis, D. Associations of adverse childhood experiences and suicidal behaviors in adulthood in a U.S. nationally representative sample. Child Care Health Dev. 2019, 45, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.E.; Higginson, G.K.; Grant-Worley, J.A. Physical abuse among high school students. Prevalence and correlation with other health behaviors. Arch. Pediatr. Adolesc. Med. 1995, 149, 1254–1258. [Google Scholar] [CrossRef]
- Klein, H.; Elifson, K.W.; Sterk, C.E. Childhood neglect and adulthood involvement in HIV-related risk behaviors. Child Abus. Negl. 2007, 31, 39–53. [Google Scholar] [CrossRef]
- Wilson, H.W.; Widom, C.S. An examination of risky sexual behavior and HIV in victims of child abuse and neglect: A 30-year follow-up. Health Psychol. 2008, 27, 149–158. [Google Scholar] [CrossRef]
- Homma, Y.; Wang, N.; Saewyc, E.; Kishor, N. The relationship between sexual abuse and risky sexual behavior among adolescent boys: A meta-analysis. J. Adolesc. Health 2012, 51, 18–24. [Google Scholar] [CrossRef]
- Abajobir, A.A.; Kisely, S.; Maravilla, J.C.; Williams, G.; Najman, J.M. Gender differences in the association between childhood sexual abuse and risky sexual behaviours: A systematic review and meta-analysis. Child Abus. Negl. 2017, 63, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, E.O.; Genuis, M.L.; Violato, C. A meta-analysis of the published research on the effects of child sexual abuse. J. Psychol. 2001, 135, 17–36. [Google Scholar] [CrossRef] [PubMed]
- Arriola, K.R.; Louden, T.; Doldren, M.A.; Fortenberry, R.M. A meta-analysis of the relationship of child sexual abuse to HIV risk behavior among women. Child Abus. Negl. 2005, 29, 725–746. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, K.R.; Katon, W.; McCarty, C.; Richardson, L.P.; Courtney, M.E. Association between childhood sexual abuse and transactional sex in youth aging out of foster care. Child Abus. Negl. 2012, 36, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Chiang, L.F.; Chen, J.; Gladden, M.R.; Mercy, J.A.; Kwesigabo, G.; Mrisho, F.; Dahlberg, L.L.; Nyunt, M.Z.; Brookmeyer, K.A.; Vagi, K. HTV and childhood sexual violence: Implications for sexual risk behaviors and HIV testing in Tanzania. AIDS Educ. Prev. 2015, 27, 474–487. [Google Scholar] [CrossRef]
- Ding, R.; Wen, X.; He, P.; Guo, C.; Luo, Y.; Song, X.; Zheng, X. Association between Childhood and Adolescent Sexual Abuse Experiences and High-Risk Sexual Behaviors among Chinese Youth. Sex. Med. 2018, 6, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Jordanova Peshevska, D.; Raleva, M.; Filov, I.; Sethi, D.; Jordanova, T.; Hazdi Hamza, K.; Tozija, F.; Damchevska Ilievska, V. Association between physical abuse, physical neglect and health risk behaviors among young adolescents: Results from the national study. Maced. J. Med. Sci. 2014, 7, 380–385. [Google Scholar]
- Thibodeau, M.E.; Lavoie, F.; Hebert, M.; Blais, M. Childhood maltreatment and adolescent sexual risk behaviors: Unique, cumulative and interactive effects. Child Abus. Negl. 2017, 72, 411–420. [Google Scholar] [CrossRef]
- London, S.; Quinn, K.; Scheidell, J.D.; Frueh, B.C.; Khan, M.R. Adverse Experiences in Childhood and Sexually Transmitted Infection Risk from Adolescence into Adulthood. Sex. Transm. Dis. 2017, 44, 524–532. [Google Scholar] [CrossRef]
- Agardh, A.; Odberg-Pettersson, K.; Ostergren, P.O. Experience of sexual coercion and risky sexual behavior among Ugandan university students. BMC Public Health 2011, 11, 527. [Google Scholar] [CrossRef]
- Van Dorn, R.A.; Mustillo, S.; Elbogen, E.B.; Dorsey, S.; Swanson, J.W.; Swartz, M.S. The effects of early sexual abuse on adult risky sexual behaviors among persons with severe mental illness. Child Abus. Negl. 2005, 29, 1265–1279. [Google Scholar] [CrossRef] [PubMed]
- Voisin, D.R. The relationship between violence exposure and HIV sexual risk behavior: Does gender matter? Am. J. Orthopsychiatry 2005, 75, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.E.; Wang, M.Q. Psychosocial correlates of U.S. adolescents who report a history of forced sexual intercourse. J. Adolesc. Health 2005, 36, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Zierler, S.; Feingold, L.; Laufer, D.; Velentgas, P.; Kantrowitz-Gordon, I.; Mayer, K. Adult survivors of childhood sexual abuse and subsequent risk of HIV infection. Am. J. Public Health 1991, 81, 572–575. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.Y.; Choi, E.P.; Chan, C.K.; Fong, D.Y. Controlling Anxiety Mediates the Influence of Childhood Adversities on Risky Sexual Behaviors among Emerging Adults. J. Sex Res. 2017, 54, 1018–1025. [Google Scholar] [CrossRef]
- Suzuki, H.; Tomoda, A. Roles of attachment and self-esteem: Impact of early life stress on depressive symptoms among Japanese institutionalized children. BMC Psychiatry 2015, 15, 8. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K.; Latzman, N.E.; Latzman, R.D. Pathway from child sexual and physical abuse to risky sex among emerging adults: The role of trauma-related intrusions and alcohol problems. J. Adolesc. Health 2014, 54, 442–448. [Google Scholar] [CrossRef]
- Thompson, R.; Lewis, T.; Neilson, E.C.; English, D.J.; Litrownik, A.J.; Margolis, B.; Proctor, L.; Dubowitz, H. Child Maltreatment and Risky Sexual Behavior: Indirect Effects through Trauma Symptoms and Substance Use. Child Maltreatment 2017, 22, 69–78. [Google Scholar] [CrossRef]
- Trickett, P.K.; Noll, J.G.; Putnam, F.W. The impact of sexual abuse on female development: Lessons from a multigenerational, longitudinal research study. Dev. Psychopathol. 2011, 23, 453–476. [Google Scholar] [CrossRef]
- Castro, M.; Alcantara-Lopez, M.; Martinez, A.; Fernandez, V.; Sanchez-Meca, J.; Lopez-Soler, C. Mother’s IPV, Child Maltreatment Type and the Presence of PTSD in Children and Adolescents. Int. J. Environ. Res. Public Health 2017, 14, 1077. [Google Scholar] [CrossRef]
- Masters, N.T.; George, W.H.; Davis, K.C.; Norris, J.; Heiman, J.R.; Jacques-Tiura, A.J.; Gilmore, A.K.; Nguyen, H.V.; Kajumulo, K.F.; Otto, J.M.; et al. Women’s unprotected sex intentions: Roles of sexual victimization, intoxication, and partner perception. J. Sex Res. 2014, 51, 586–598. [Google Scholar] [CrossRef] [PubMed][Green Version]
- English, D.J.; Thompson, R.; White, C.R. Predicting risk of entry into foster care from early childhood experiences: A survival analysis using LONGSCAN data. Child Abus. Negl. 2015, 45, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Payne, J.S.; Galvan, F.H.; Williams, J.K.; Prusinski, M.; Zhang, M.; Wyatt, G.E.; Myers, H.F. Impact of childhood sexual abuse on the emotions and behaviours of adult men from three ethnic groups in the USA. Cult. Health Sex. 2014. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.C.; Thompson, E.A.; Morrison-Beedy, D. Multi-system influences on adolescent risky sexual behavior. Res. Nurs. Health 2010, 33, 512–527. [Google Scholar] [CrossRef] [PubMed]
- Hahn, A.M.; Simons, R.M.; Simons, J.S. Childhood Maltreatment and Sexual Risk Taking: The Mediating Role of Alexithymia. Arch. Sex. Behav. 2016, 45, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Chocyk, A.; Majcher-Maslanka, I.; Dudys, D.; Przyborowska, A.; Wedzony, K. Impact of early-life stress on the medial prefrontal cortex functions—A search for the pathomechanisms of anxiety and mood disorders. Pharmacol. Rep. 2013, 65, 1462–1470. [Google Scholar] [CrossRef]
- Gutnik, L.A.; Hakimzada, A.F.; Yoskowitz, N.A.; Patel, V.L. The role of emotion in decision-making: A cognitive neuroeconomic approach towards understanding sexual risk behavior. J. Biomed. Inform. 2006, 39, 720–736. [Google Scholar] [CrossRef]
- Noll, J.G.; Haralson, K.J.; Butler, E.M.; Shenk, C.E. Childhood maltreatment, psychological dysregulation, and risky sexual behaviors in female adolescents. J. Pediatr. Psychol. 2011, 36, 743–752. [Google Scholar] [CrossRef]
- Dodge, B.; Reece, M.; Cole, S.L.; Sandfort, T.G. Sexual compulsivity among heterosexual college students. J. Sex Res. 2004, 41, 343–350. [Google Scholar] [CrossRef][Green Version]
- Isaksson, J.; Stickley, A.; Koposov, R.; Ruchkin, V. The danger of being inattentive—ADHD symptoms and risky sexual behaviour in Russian adolescents. Eur. Psychiatry 2018, 47, 42–48. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Author(s) (Year) | Geographic Region | Sample Size | Assessment of CM | Study Design | Study Sample | Quality Sore | Form(s) of CM |
|---|---|---|---|---|---|---|---|
| Abajobir (2018) [9] | Oceania | 3081 | Substantiated record | Cohort study | Other | 8 | CSA, CPA, CEA, CN |
| Ahrens (2012) [34] | America | 574 | SR | Cohort study | Other | 6 | CSA |
| Chartier (2009) [20] | America | 8116 | SR | Cross-sectional study | Other | 6 | CSA, CPA |
| Chiang (2015) [35] | Africa | 3739 | SR | Cross-sectional study | Other | 6 | CSA |
| Ding (2018) [36] | Asia | 4974 | SR | Cross-sectional study | Other | 6 | CSA |
| Jordanova Peshevska (2014) [37] | America | 1277 | SR | Cross-sectional study | School sample | 7 | CPA, CN |
| Thibodeau (2017) [38] | America | 1940 | SR | Cross-sectional study | School sample | 7 | CSA, CPA CN |
| Ramiro (2010) [13] | Asia | 1068 | SR | Cross-sectional study | Other | 6 | CSA, CPA CEA, CN |
| Nelson (1995) [27] | America | 1957 | SR | Cross-sectional study | School sample | 5 | CPA |
| VanderEnde (2018) [15] | Africa | 610 | SR | Cross-sectional study | Other | 6 | CSA, CPA CEA |
| London (2017) [39] | America | 12288 | SR | Cohort study | Other | 7 | CSA, CPA CEA, CN |
| Diehl (2018) [23] | America | 134 | SR | Cross-sectional study | Other | 5 | CSA |
| Agardh (2011) [40] | Africa | 980 | SR | Cross-sectional study | School sample | 5 | CSA |
| Tang (2018) [24] | Asia | 17966 | SR | Cross-sectional study | School sample | 7 | CSA |
| Van Dorn (2005) [41] | America | 609 | SR | Cross-sectional study | Other | 5 | CSA |
| Voisin (2005) [42] | America | 409 | SR | Cross-sectional study | School sample | 6 | CSA |
| Howard (2005) [43] | America | 13601 | SR | Cross-sectional study | School sample | 7 | CSA |
| Wilson (2008) [29] | America | 1070 | Substantiated record | Cohort study | Other | 9 | CSA, CPA |
| Zierler (1991) [44] | Europe | 164 | SR | Cohort study | Other | 7 | CSA |
| Subgroup | Early Sexual Debut | Multiple Sexual Partners | Transactional Sex | Unprotected Sex |
|---|---|---|---|---|
| Geographic Region | TSD: I2 = 0% P = 0.38 | TSD: I2 = 2.8% P = 0.38 | TSD: I2 = 85.5% P < 0.01 | TSD: I2 = 59.2% P = 0.06 |
| America | 1.65 (1.04, 2.63) n = 2 | 2.00 (1.49, 2.69) n = 7 | 2.29 (1.55, 3.38) n = 4 | 1.71 (1.14, 2.55) n = 4 |
| I2 = 82% P = 0.02 | I2 = 93% P < 0.01 | I2 = 64% P = 0.04 | I2 = 91% P < 0.01 | |
| Asia | 3.27 (1.26, 8.60) n = 2 | 3.12 (1.94, 5.03) n = 3 | 7.40 (5.09, 10.77) n = 1 | 1.98 (0.87, 4.50) n = 2 |
| I2 = 91% P < 0.01 | I2 = 88% P < 0.01 | Not applicable | I2 = 92% P < 0.01 | |
| Europe | Not applicable | 2.00 (1.41, 2.83) n = 1 | 4.00 (2.00, 8.00) n = 1 | 1.00 (0.80, 1.26) n = 1 |
| Not applicable | Not applicable | Not applicable | ||
| Other | 2.18 (1.73, 2.75) n = 2 | 1.83 (1.49, 2.24) n = 4 | 2.40 (1.29, 4.49) n = 2 | 1.43 (1.00, 2.04) n = 2 |
| I2 = 0% P = 0.74 | I2 = 42% P = 0.16 | I2 = 0% P = 0.41 | I2 = 33% P = 0.22 | |
| Assessment of CM | TSD: I2 = 0% P = 0.72 | TSD: I2 = 67.1% P = 0.08 | TSD: I2 = 0% P = 0.56 | Not applicable |
| Substantiated records | 2.12 (1.72, 2.61) n = 2 | 1.66 (1.27, 2.17) n = 1 | 2.56 (1.68, 3.90) n = 2 | |
| I2 = 0% P = 0.98 | Not applicable | I2 = 0% P = 0.60 | Not applicable | |
| Self-report | 2.33 (1.41, 3.85) n = 4 | 2.28 (1.80, 2.88) n = 14 | 3.18 (1.75, 5.79) n = 6 | 1.59 (1.22, 2.09) n = 9 |
| I2 = 88% P < 0.01 | I2 = 92% P < 0.01 | I2 = 88% P < 0.01 | I2 = 88% P < 0.01 | |
| Study design | TSD: I2 = 54.4% P = 0.14 | TSD: I2 = 90.6% P < 0.01 | TSD: I2 = 1.1% P = 0.31 | TSD: I2 = 87.3% P < 0.01 |
| Cross-sectional study | 2.86 (1.69, 4.86) n = 3 | 2.62 (2.03, 3.38) n = 11 | 3.74 (1.79, 7.83) n = 4 | 1.70 (1.27, 2.29) n = 8 |
| I2 = 82% P < 0.01 | I2 = 89% P < 0.01 | I2 = 86% P < 0.01 | I2 = 88% P < 0.01 | |
| Cohort study | 1.79 (1.29, 2.48) n = 3 | 1.46 (1.15, 1.86) n = 4 | 2.39 (1.51, 3.78) n = 4 | 1.00 (0.80, 1.26) n = 1 |
| I2 = 75% P = 0.02 | I2 = 76% P < 0.01 | I2 = 63% P = 0.05 | Not applicable | |
| Study sample | TSD: I2 = 0% P = 0.67 | TSD: I2 = 0% P = 0.53 | Not applicable | TSD: I2 = 71.7% P = 0.06 |
| School sample | 2.49 (1.14, 5.42) n = 3 | 2.42 (1.72, 3.38) n = 7 | 1.91 (1.26, 2.89) n = 5 | |
| I2 = 92% P < 0.01 | I2 = 92% P < 0.01 | Not applicable | I2 = 93% P < 0.01 | |
| Other | 2.10 (1.77, 2.48) n = 3 | 2.08 (1.51, 2.87) n = 8 | 3.05 (1.92, 4.86) n = 8 | 1.16 (0.98, 1.37) n = 4 |
| I2 = 0% P = 0.99 | I2 = 91% P < 0.01 | I2 = 84% P < 0.01 | I2 = 37% P = 0.19 | |
| Quality score | TSD: I2 = 0% P = 0.80 | TSD: I2 = 0% P = 0.67 | TSD: I2 = 1.1% P = 0.31 | TSD: I2 = 0% P = 0.85 |
| ≥7 | 2.02 (1.43, 2.87) n = 4 | 2.11 (1.51, 2.96) n = 7 | 2.39 (1.51, 3.78) n = 4 | 1.55 (1.06, 2.25) n = 4 |
| I2 = 88% P < 0.01 | I2 = 94% P < 0.01 | I2 = 66% P = 0.02 | I2 = 93% P < 0.01 | |
| <7 | 2.14 (1.70, 2.69) n = 2 | 2.31 (1.83, 2.92) n = 8 | 3.74 (1.79, 7.83) n = 4 | 1.64 (1.04, 2.59) n = 5 |
| I2 = 0% P = 0.65 | I2 = 74% P < 0.01 | I2 = 86% P < 0.01 | I2 = 81% P < 0.01 | |
| Year of publication | TSD: I2 = 0% P = 0.74 | TSD: I2 = 0% P = 0.56 | TSD: I2 = 0% P = 0.59 | TSD: I2 = 0% P = 0.80 |
| <2013 | 2.13 (1.77, 2.56) n = 3 | 2.38(1.76, 3.21) n = 7 | 2.58 (1.98, 3.35) n = 3 | 1.54 (1.01, 2.35) n = 5 |
| I2 = 0% P = 0.90 | I2 = 85% P < 0.01 | I2 = 0% P = 0.40 | I2 = 89% P < 0.01 | |
| ≥2013 | 2.40 (1.21, 4.75) n = 3 | 2.09 (1.53, 2.85) n = 8 | 3.27 (1.43, 7.47) n = 5 | 1.67 (1.05, 2.66) n = 4 |
| I2 = 92% P < 0.01 | I2 = 93% P < 0.01 | I2 = 90% P < 0.01 | I2 = 91% P < 0.01 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Z.-Y.; Hu, M.; Yu, T.-L.; Yang, J. The Relationship between Childhood Maltreatment and Risky Sexual Behaviors: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3666. https://doi.org/10.3390/ijerph16193666
Wang Z-Y, Hu M, Yu T-L, Yang J. The Relationship between Childhood Maltreatment and Risky Sexual Behaviors: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(19):3666. https://doi.org/10.3390/ijerph16193666
Chicago/Turabian StyleWang, Zi-Yu, Ming Hu, Tao-Lin Yu, and Jun Yang. 2019. "The Relationship between Childhood Maltreatment and Risky Sexual Behaviors: A Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 19: 3666. https://doi.org/10.3390/ijerph16193666
APA StyleWang, Z.-Y., Hu, M., Yu, T.-L., & Yang, J. (2019). The Relationship between Childhood Maltreatment and Risky Sexual Behaviors: A Meta-Analysis. International Journal of Environmental Research and Public Health, 16(19), 3666. https://doi.org/10.3390/ijerph16193666