The Measurements and an Elaborated Understanding of Chinese eHealth Literacy (C-eHEALS) in Chronic Patients in China


Abstract
1. Introduction
eHealth Literacy
2. Materials and Methods
2.1. Measures and Development of the C-eHEALS
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Identifying C-eHEALS Items
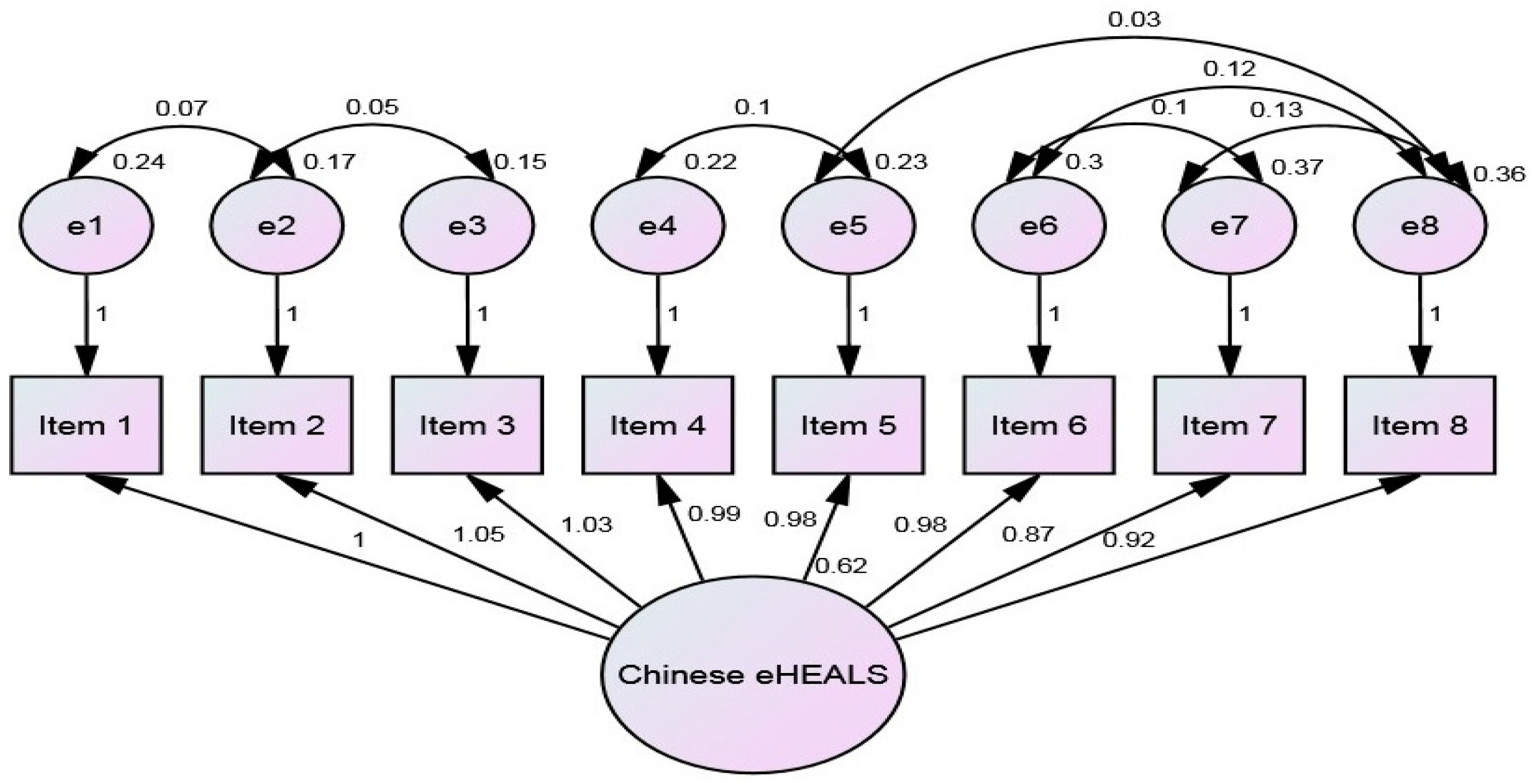
3.2. The C-eHEALS Model
3.3. Sample Characteristics
3.4. Cluster Analysis of eHealth Literacy
4. Discussion
4.1. Low and High eHealth Literacy
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Item | Factor Loading | Communalities | Item-Total Correlation | α, If Item Deleted |
|---|---|---|---|---|
| 1. I know what health resources are available on the Internet | 1 | 0.744 | 0.730 | 0.949 |
| 2. I know where to find helpful health resources on the Internet | 0.839 | 0.819 | 0.831 | 0.945 |
| 3. I know how to find helpful resources on the Internet | 0.780 | 0.812 | 0.798 | 0.946 |
| 4. I know how to use the Internet to answer my questions about health | 0.708 | 0.773 | 0.772 | 0.947 |
| 5. I know how to use the health information I find on the Internet to help me | 0.703 | 0.785 | 0.777 | 0.947 |
| 6. I have the skills I need to evaluate the health resources I find on the Internet | 0.698 | 0.759 | 0.713 | 0.948 |
| 7. I can tell high quality health resources from low quality health resources on the Internet | 0.635 | 0.665 | 0.622 | 0.952 |
| 8. I feel confident in using information from the Internet to make health decisions | 0.638 | 0.707 | 0.681 | 0.950 |
References
- Chari, R.; Warsh, J.; Ketterer, T.; Hossain, J.; Sharif, I. Association between health literacy and child and adolescent obesity. Patient Educ. Couns. 2014, 94, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.C.; Story, M.; Larson, N.I.; Neumark-Sztainer, D.; Lytle, L.A. Emerging adulthood and college-aged youth: An overlooked age for weight-related behavior change. Obesity 2008, 16, 2205–2211. [Google Scholar] [CrossRef] [PubMed]
- Frisch, A.L.; Camerini, L.; Diviani, N.; Schulz, P.J. Defining and measuring health literacy: How can we profit from other literacy domains? Health Promot. Int. 2012, 27, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Takeuchi, T.; Yano, E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care 2008, 31, 874–879. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.B.; Liu, L.; Li, Y.F.; Chen, Y.L. Relationship between health literacy, health-related behaviors and health status: A survey of elderly Chinese. Int. J. Environ. Res. Public Health 2015, 12, 9714–9725. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Davis, T.C.; McCormack, L. Health literacy: What is it? J. Health Commun. 2010, 15, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.H.; Gazmararian, J.; Parker, R.M. The impact of low health literacy on the medical costs of medicare managed care enrollees. Am. J. Med. 2005, 118, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.T.; Wen, D.; Liang, J.; Lei, J.B. How the public uses social media wechat to obtain health information in China: A survey study. BMC Med. Inform. Decis. Mak. 2017, 17, 71–100. [Google Scholar] [CrossRef] [PubMed]
- Tennant, B.; Stellefson, M.; Dodd, V.; Chaney, B.; Chaney, D.; Paige, S.; Alber, J. Ehealth literacy and web 2.0 health information seeking behaviors among baby boomers and older adults. J. Med. Internet Res. 2015, 17, e70. [Google Scholar]
- Tse, M.M.; Choi, K.C.; Leung, R.S. E-health for older people: The use of technology in health promotion. CyberPsychol. Behav. 2008, 11, 475–479. [Google Scholar] [PubMed]
- Bodie, G.D.; Dutta, M.J. Understanding health literacy for strategic health marketing: Ehealth literacy, health disparities, and the digital divide. Health Mark. Q. 2008, 25, 175–203. [Google Scholar] [CrossRef] [PubMed]
- Cline, R.J.; Haynes, K.M. Consumer health information seeking on the internet: The state of the art. Health Educ. Res. 2001, 16, 671–692. [Google Scholar] [CrossRef] [PubMed]
- Lee, M. China’s Nearly 700 Million Internet Users Are Hot for Online Finance. Forbes. Available online: https://www.forbes.com/sites/melanieleest/2016/01/25/chinas-nearly-700-million-internet-users-are-hot-for-online-finance/ (accessed on 26 January 2016).
- Oh, H.; Rizo, C.; Enkin, M.; Jadad, A.; Powell, J.; Pagliari, C. What is ehealth: A systematic review of published definitions. J. Med. Internet Res. 2005, 7, e1. [Google Scholar] [CrossRef] [PubMed]
- Ghaddar, S.F.; Valerio, M.A.; Garcia, C.M.; Hansen, L. Adolescent health literacy: The importance of credible sources for online health information. J. Sch. Health 2012, 82, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Neter, E.; Brainin, E. Ehealth literacy: Extending the digital divide to the realm of health information. J. Med. Internet Res. 2012, 14, e19. [Google Scholar] [CrossRef] [PubMed]
- Norman, C.D.; Skinner, H.A. eHEALS: The ehealth literacy scale. J. Med. Internet Res. 2006, 8, 3–31. [Google Scholar] [CrossRef] [PubMed]
- Norman, C.D.; Skinner, H.A.; Ronson, B.; Simms, M. Ehealth literacy: Essential skills for consumer health in a networked world. J. Med. Internet Res. 2006, 8, e9. [Google Scholar] [CrossRef] [PubMed]
- Mackert, M.; Champlin, S.E.; Holton, A.; Muñoz, I.I.; Damásio, M.J. Ehealth and health literacy: A research methodology review. J. Comput.-Mediat. Commun. 2014, 19, 516–528. [Google Scholar] [CrossRef]
- Norman, C. Ehealth literacy 2.0: Problems and opportunities with an evolving concept. J. Med. Internet Res. 2011, 13, e125. [Google Scholar]
- Manganello, J.A. Health literacy and adolescents: A framework and agenda for future research. Health Educ. Res. 2008, 23, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.C.; Su, C.L.; Chen, C.H. Development of a health literacy scale for Chinese-speaking adults in Taiwan. Int. J. Biol. Sci. 2010, 6, 150–156. [Google Scholar]
- Pleasant, A.; McKinney, J.; Rikard, R.V. Health literacy measurement: A proposed research agenda. J. Health Commun. 2011, 16, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Petrič, G.; Atanasova, S.; Kamin, T. Ill literates or illiterates? Investigating the ehealth literacy of users of online health communities. J. Med. Internet Res. 2017, 19, e331. [Google Scholar] [PubMed]
- Chan, C.V.; Kaufman, D.R. A framework for characterizing ehealth literacy demands and barriers. J. Med. Internet Res. 2011, 3, e94. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.; Leung, A.; Chiang, V.C.; Li, H.C.; Wong, E.M.; Liu, A.N.; Chan, S.S. A pilot project to build e-health literacy among university students in Hong Kong. In Proceedings of the Positioning the Profession: The Tenth International Congress on Medical Librarianship, Brisbane, Australia, 31 August–4 September 2009; pp. 1–15. [Google Scholar]
- Hove, T.; Paek, H.-J.; Isaacson, T. Using adolescent ehealth literacy to weigh trust in commercial web sites. J. Advert. Res. 2011, 51, 524–537. [Google Scholar] [CrossRef]
- Paek, H.J.; Hove, T. Social cognitive factors and perceived social influences that improve adolescent ehealth literacy. Health Commun. 2012, 27, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Percheski, C.; Hargittai, E. Health information-seeking in the digital age. J. Am. Coll. Health 2011, 59, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Skinner, H.; Biscope, S.; Poland, B.; Goldberg, E.; Gray, N.; Richardson, C. How adolescents use technology for health information: Implications for health professionals from focus group studies. J. Med. Internet Res. 2003, 5, e32. [Google Scholar] [CrossRef] [PubMed]
- Paramio Perez, G.; Almagro, B.J.; Hernando Gomez, A.; Aguaded Gomez, J.I. Validation of the ehealth literacy scale (eHEALS) in Spanish university students. Rev. Esp. Salud Publ. 2015, 89, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Koo, M.; Norman, C.D.; Chang, H.M. Psychometric evaluation of a Chinese version of the ehealth literacy scale (eHEALS) in school age children. Int. Electron. J. Health Educ. 2012, 15, 29–36. [Google Scholar]
- Paige, S.R.; Krieger, J.L.; Stellefson, M.; Alber, J.M. Ehealth literacy in chronic disease patients: An item response theory analysis of the ehealth literacy scale (eHEALS). Patient Educ. Couns. 2017, 100, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Soellner, R.; Huber, S.; Reder, M. The concept of ehealth literacy and its measurement: German translation of the eHEALS. J. Media Psychol. Theor. Methods Appl. 2014, 26, 29–38. [Google Scholar] [CrossRef]
- Mitsutake, S.; Shibata, A.; Ishii, K.; Okazaki, K.; Oka, K. Developing Japanese version of the ehealth literacy scale (eHEALS). [Nihon koshu eisei zasshi] Jpn. J. Public Health 2011, 58, 361–371. [Google Scholar]
- Van der Vaart, R.; van Deursen, A.J.; Drossaert, C.H.; Taal, E.; van Dijk, J.A.; van de Laar, M.A. Does the ehealth literacy scale (eHEALS) measure what it intends to measure? Validation of a Dutch version of the eHEALS in two adult populations. J. Med. Internet Res. 2011, 13, e86. [Google Scholar] [PubMed]
- Diviani, N.; Dima, A.L.; Schulz, P.J. A psychometric analysis of the Italian version of the ehealth literacy scale using item response and classical test theory methods. J. Med. Internet Res. 2017, 19, e114. [Google Scholar] [CrossRef] [PubMed]
- Hyde, L.L.; Boyes, A.W.; Evans, T.J.; Mackenzie, L.J.; Sanson-Fisher, R. Three-factor structure of the ehealth literacy scale among magnetic resonance imaging and computed tomography outpatients: A confirmatory factor analysis. JMIR Hum. Factors 2018, 5, e6. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.Y.; Nahm, E.S. Testing reliability and validity of the ehealth literacy scale (eHEALS) for older adults recruited online. CIN Comput. Inform. Nurs. 2015, 33, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Tomás, C.C.; Queirós, P.J.P.; Ferreira, T.D.J.R. Analysis of the psychometric properties of the Portuguese version of an ehealth literacy assessment tool. Rev. Enferm. Ref. 2014, 4, 19–28. [Google Scholar] [CrossRef]
- Karnoe, A.; Kayser, L. How is eHealth literacy measured and what do the measurements tell us? A systematic review. Knowl. Manag. E-Learn. Int. J. 2015, 7, 576–600. [Google Scholar]
- Nguyen, J.; Moorhouse, M.; Curbow, B.; Christie, J.; Walsh-Childers, K.; Islam, S. Construct validity of the ehealth literacy scale (eHEALS) among two adult populations: A rasch analysis. JMIR Public Health Surveill. 2016, 2, e24. [Google Scholar] [CrossRef] [PubMed]
- Hutcheson, G.D.; Sofroniou, N. The Multivariate Social Scientist: Introductory Statistics Using Generalized Linear Models; Sage: Newcastle upon Tyne, UK, 1999. [Google Scholar]
- Tsai, T.I.; Lee, S.Y.D.; Tsai, Y.W.; Kuo, K.N. Methodology and validation of health literacy scale development in Taiwan. J. Health Commun. 2011, 16, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Wang, L.; Cai, Z.; Bao, L.; Ai, P.; Ai, Z. Prevalence and risk factors of low health literacy: A community-based study in Shanghai, China. Int. J. Environ. Res. Public Health 2017, 14, 628–638. [Google Scholar] [CrossRef] [PubMed]

| Reliability | Validity | |||||
|---|---|---|---|---|---|---|
| Cronbach’s | Media & Computer | Computer | Information | Health | Education | |
| alpha | Split-half | literacy | skills | literacy | status | attainment |
| 0.95 *** | 0.92 *** | 0.13 * | 0.44 *** | 0.12 * | 0.08 | 0.11 ** |
| Item | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1. I know what health resources are available on the Internet | 1 | |||||||
| 2. I know where to find helpful health resources on the Internet | 0.839 | 1 | ||||||
| 3. I know how to find helpful resources on the Internet | 0.780 | 0.869 | 1 | |||||
| 4. I know how to use the Internet to answer my questions about health | 0.708 | 0.764 | 0.777 | 1 | ||||
| 5. I know how to use the health information I find on the Internet to help me | 0.703 | 0.760 | 0.754 | 0.852 | 1 | |||
| 6. I have the skills I need to evaluate the health resources I find on the Internet | 0.698 | 0.721 | 0.722 | 0.709 | 0.73 | 1 | ||
| 7. I can tell high quality health resources from low quality health resources on the Internet | 0.635 | 0.660 | 0.668 | 0.635 | 0.656 | 0.725 | 1 | |
| 8. I feel confident in using information from the Internet to make health decisions | 0.638 | 0.671 | 0.688 | 0.669 | 0.706 | 0.769 | 0.73 | 1 |
| Variables | n (%) | 8-Item Score | |
|---|---|---|---|
| 352 (100) | Mean ± SD | ||
| Sex | Male | 187 (53.1) | 29.19 ± 6.63 |
| Female | 165 (46.9) | 28.75 ± 6.27 | |
| Age | 18–25 | 124 (35.2) | 29.84 ± 6.79 |
| 26–35 | 137 (38.9) | 28.64 ± 6.26 | |
| 36–45 | 56 (15.9) | 28.39 ± 6.16 | |
| 46–55 | 30 (8.5) | 27.80 ± 6.27 | |
| Over 55 | 5 (1.4) | 30.80 ± 7.04 | |
| Education | Primary & secondary school | 2 (0.6) | 20.00 ± 5.66 |
| Junior high | 9 (2.6) | 28.67 ± 3.64 | |
| High school | 22 (6.3) | 25.73 ± 7.67 | |
| College or bachelor | 238 (67.6) | 29.22 ± 6.55 | |
| Master degree or above | 81 (23.0) | 29.43 ± 5.77 | |
| Resident *** | Guangdong | 129 (36.6) | 28.63 ± 6.60 |
| Others | 223 (63.2) | 29.46 ± 6.48 | |
| Occupation | Business | 180 (51.5) | 28.74 ± 6.54 |
| Student | 63 (17.9) | 30.60 ± 5.50 | |
| Self-employed | 34 (9.7) | 29.60 ± 6.45 | |
| Public servant | 29 (8.2) | 29.96 ± 4.82 | |
| Clinicians | 27 (7.7) | 26.25 ± 5.33 | |
| Others | 19 (5.4) | 24.95 ± 9.36 | |
| Income (RMB) | less than 1000 | 55 (15.6) | 29.35 ± 5.55 |
| 1000–3000 | 50 (14.2) | 29.32 ± 6.69 | |
| 3001–5000 | 85 (24.1) | 28.61 ± 6.94 | |
| 5001–7000 | 75 (21.3) | 28.59 ± 6.49 | |
| 7001 & above | 87 (24.7) | 29.26 ± 6.44 | |
| Item | Low eHealth n | % | High eHealth n | % |
|---|---|---|---|---|
| 1. Able to attach files in email | 235 | 66.8 | 71 | 20.2 |
| 2. I worry about computer virus | 62 | 17.6 | 215 | 61.1 |
| 3. My computer skills are better than my peers | 43 | 12.2 | 73 | 20.7 |
| 4. Have knowledge about intellectual property | 33 | 9.4 | 98 | 27.8 |
| 5. Can use a computer to do my work | 25 | 7.1 | 159 | 45.2 |
| 6. Know how to use a word processor | 24 | 6.8 | 160 | 45.5 |
| 7. Can send and receive email | 20 | 5.7 | 218 | 61.9 |
| 8. Can use the Web to search for information | 19 | 5.4 | 197 | 56.0 |
| 9. Can find the file on my computer after downloading | 19 | 5.4 | 174 | 49.4 |
| 10. Can find information on the Web | 12 | 3.4 | 185 | 52.6 |
| Item | Low eHealth n | % | High eHealth n | % |
|---|---|---|---|---|
| 1. Face-to-face inquiry | 179 | 50.9 | 73 | 20.7 |
| 2. Mobile phone apps | 72 | 48.9 | 19 | 5.4 |
| 3. Specific health websites | 167 | 47.4 | 28 | 8.0 |
| 4. Hospital website | 160 | 45.5 | 27 | 7.7 |
| 5. Online forum | 125 | 35.5 | 37 | 10.5 |
| 6. Websites with instant feedback | 77 | 21.9 | 205 | 58.2 |
| 7. Social media (e.g., QQ) | 65 | 18.5 | 234 | 66.5 |
| 8. Online Encyclopedia | 45 | 12.8 | 237 | 67.3 |
| 9. Search engine (e.g., Baidu) | 19 | 5.4 | 155 | 44.0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, A.; Schulz, P.J. The Measurements and an Elaborated Understanding of Chinese eHealth Literacy (C-eHEALS) in Chronic Patients in China. Int. J. Environ. Res. Public Health 2018, 15, 1553. https://doi.org/10.3390/ijerph15071553
Chang A, Schulz PJ. The Measurements and an Elaborated Understanding of Chinese eHealth Literacy (C-eHEALS) in Chronic Patients in China. International Journal of Environmental Research and Public Health. 2018; 15(7):1553. https://doi.org/10.3390/ijerph15071553
Chicago/Turabian StyleChang, Angela, and Peter J. Schulz. 2018. "The Measurements and an Elaborated Understanding of Chinese eHealth Literacy (C-eHEALS) in Chronic Patients in China" International Journal of Environmental Research and Public Health 15, no. 7: 1553. https://doi.org/10.3390/ijerph15071553
APA StyleChang, A., & Schulz, P. J. (2018). The Measurements and an Elaborated Understanding of Chinese eHealth Literacy (C-eHEALS) in Chronic Patients in China. International Journal of Environmental Research and Public Health, 15(7), 1553. https://doi.org/10.3390/ijerph15071553