
Attitude, Acceptability and Knowledge of HPV Vaccination among Local University Students in Hong Kong

 ,
,
Abstract
:1. Introduction
1.1. Attitude on Vaccination
1.2. The Acceptability of Vaccination
1.3. Knowledge of Vaccination
1.4. Research Gaps and Aim/Purpose of the Study
2. Materials and Methods
2.1. Study Design
2.2. Sampling Method
2.3. Inclusion and Exclusion Criteria
2.4. Instrument
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Response Rate
3.2. Socio-Demographic Characteristics
3.3. Health-Related Characteristics
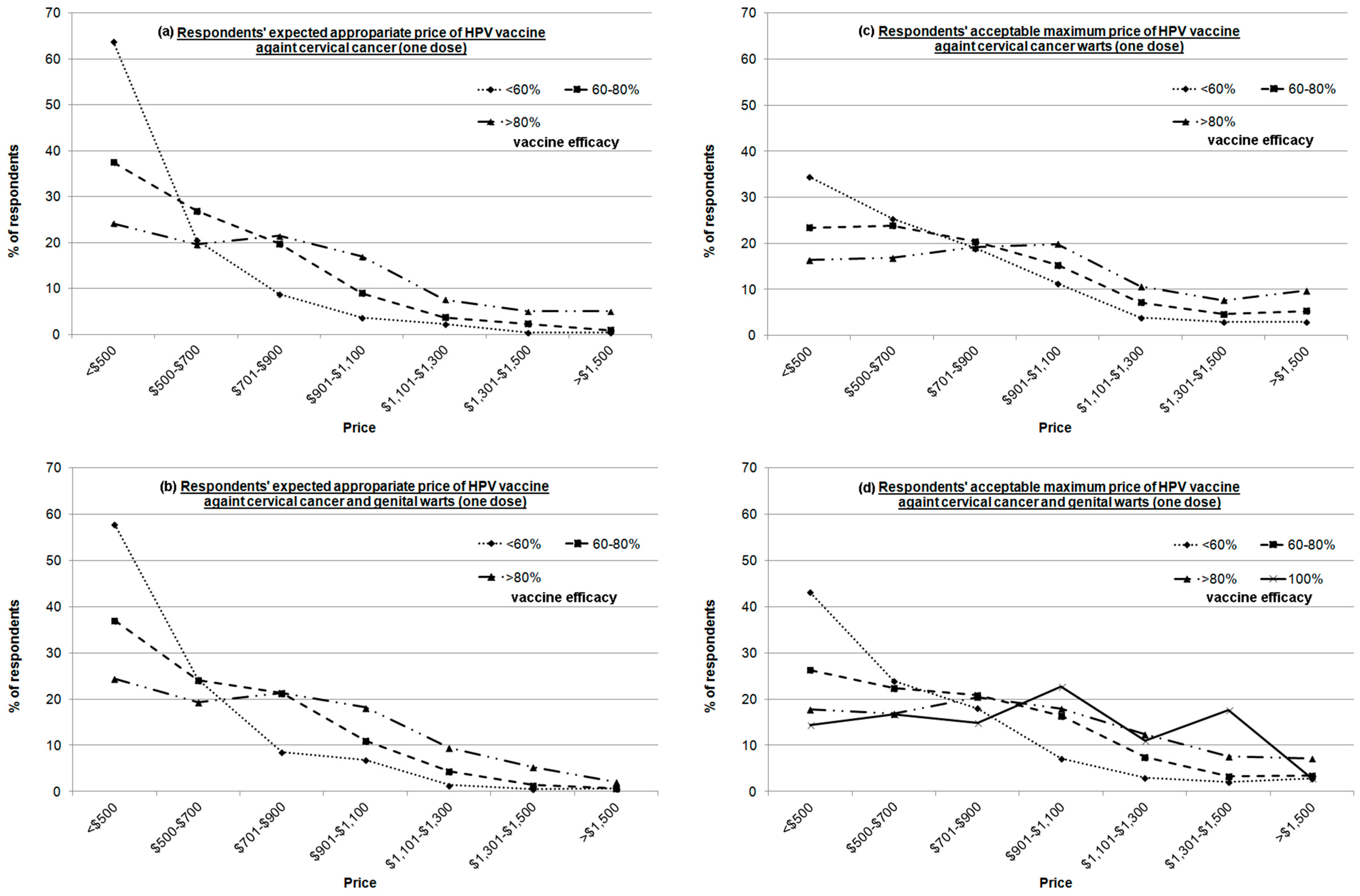
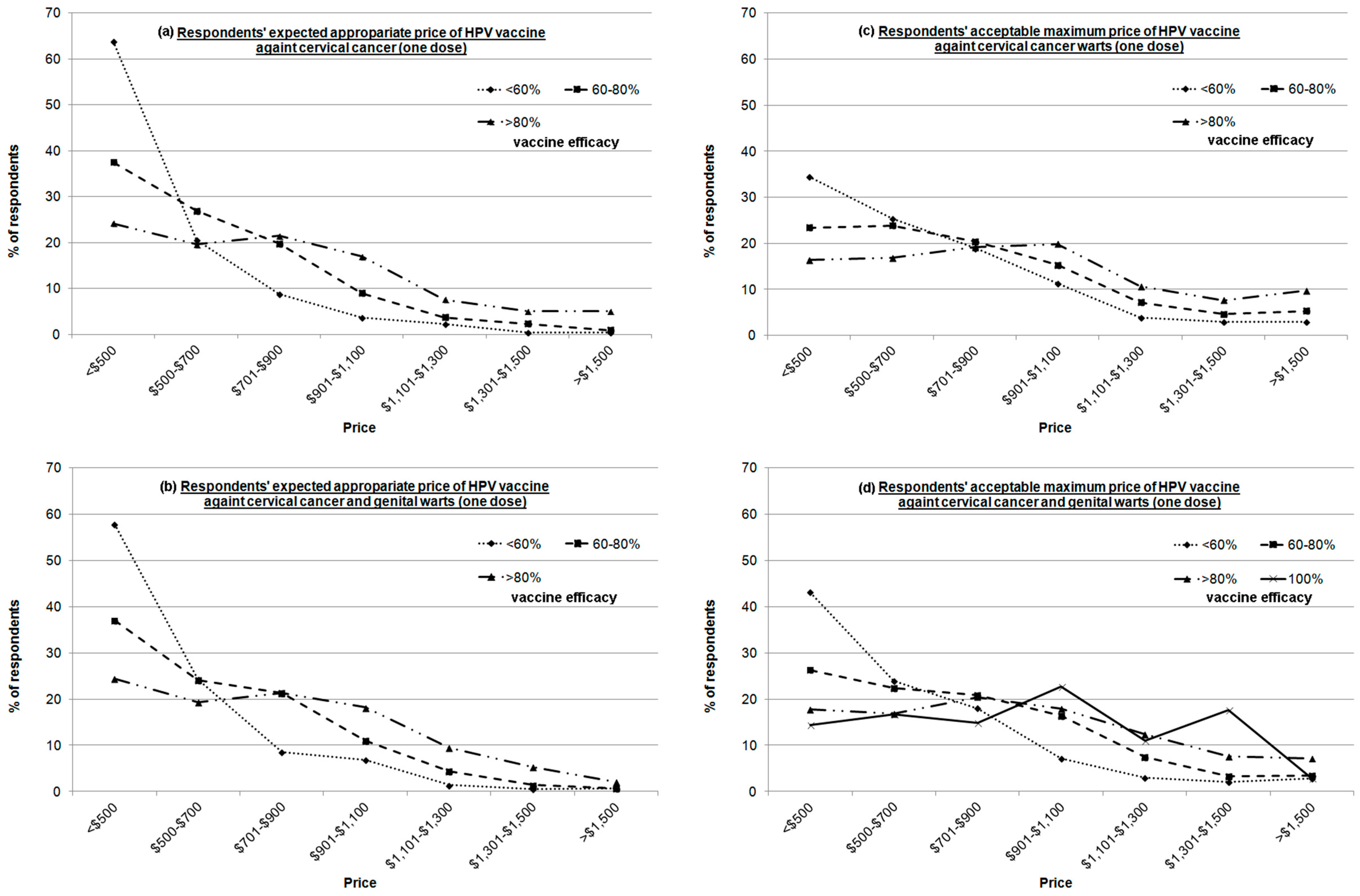
3.4. Acceptability of HPV Vaccination
3.5. Attitude towards HPV Vaccination
3.6. Knowledge of HPV Vaccination
3.7. Predictors of the Respondents’ Attitude towards HPV Vaccination
4. Discussion
4.1. Low HPV Vaccination Uptake Compared to Similar Studies
4.2. Intention of Vaccination
4.3. Knowledge of HPV and HPV Vaccination
4.4. Predictors of Students’ Attitude towards HPV Vaccination
4.5. Limitations
4.6. Recommendations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| HPV | Human Papillomavirus |
| MSM | Men who have sex with other men |
References
- What Is HPV? Available online: http://www.cdc.gov/hpv/parents/whatishpv.html (accessed on 15 February 2016).
- Leading Cancer Sites in Hong Kong in 2012. Available online: http://www3.ha.org.hk/cancereg/Summary%20of%20CanStat%202012.pdf (accessed on 15 February 2016).
- Genital HPV Infection—Fact Sheet. Available online: http://www.cdc.gov/std/hpv/STDFact-HPV.htm (accessed on 15 February 2016).
- Recommendation on the Use of Human Papillovirus (HPV) Vaccine. Available online: http://www.chp.gov.hk/files/pdf/recommendation_on_the_use_of_human_papillomavirus_hpv_vaccine_r.pdf (accessed on 15 February 2016).
- HPV Vaccine Information For Young Women-Fact Sheet. Available online: http://www.cdc.gov/std/hpv/STDFact-HPV-vaccine-young-women.htm (accessed on 15 February 2016).
- The FUTURE I/II Study Group. Four year efficacy of prophylactic human papillomavirus quadrivalent vaccine against low grade cervical, vulvar, and vaginal intraepithelial neoplasia and anogenital warts: Randomised controlled trial. BMJ 2010, 341. [Google Scholar] [CrossRef]
- HPV Vaccines—Questions and Answers. Available online: http://www.cdc.gov/hpv/parents/questions-answers.html (accessed on 15 February 2016).
- Youth HPV Prevention Program. Available online: http://www.famplan.org.hk/fpahk/common/banner/hpvv2015/hpvv2015_eng.html (accessed on 15 February 2016).
- Li, S.L.; Lau, Y.L.; Lam, T.H.; Yip, P.S.; Fan, S.Y.; Ip, P. HPV vaccination in Hong Kong: Uptake and reasons for non-vaccination amongst Chinese adolescent girls. Vaccine 2013, 31, 5785–5788. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.C.; Leung, G.M.; Woo, P.P.; Jit, M.; Wu, J.T. Acceptability and uptake of female adolescent HPV vaccination in Hong Kong: A survey of mothers and adolescents. Vaccine 2013, 32, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Kwan, T.T.C.; Chan, K.K.L.; Yip, A.M.W.; Tam, K.F.; Cheung, A.N.Y.; Young, P.M.C.; Lee, P.W.H.; Ngan, H.Y.S. Barriers and facilitators to human papillomavirus vaccination among Chinese adolescent girls in Hong Kong: A qualitative-quantitative study. Sex. Transm. Infect. 2008, 84, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.M.; Zhang, S.K.; Pan, X.F.; Ren, Z.F.; Yang, C.X.; Wang, Z.Z.; Gao, X.H.; Li, M.; Zheng, Q.Q.; Ma, W.; et al. Human papillomavirus vaccine awareness, acceptability, and decision-making factors among Chinese college students. Asian Pac. J. Cancer Prev. 2014, 15, 3239–3245. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Ho, M.; Cheung, C.K.M.; Keung, V.M.W. Factors influencing adolescent girls’ decision in initiation for human papillomavirus vaccination: A cross-sectional study in Hong Kong. BMC Public Health 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Songthap, A.; Pitisuttithum, P.; Kaewkungwal, J.; Fungladda, W.; Bussaratid, V. Knowledge, attitudes, and acceptability of a human papilloma virus vaccine among students, parents and teachers in Thailand. Southeast Asian J. Trop. Med. 2012, 43, 340–353. [Google Scholar]
- Lee, A.; Chan, P.; Lau, L.; Chan, T. How would family physicians facilitate the uptake of HPV vaccination: Focus group study on parents and single women in Hong Kong. Hong Kong Pract. 2011, 33, 7–114. [Google Scholar]
- Chan, K.K.L.; Kwan, T.T.C.; Yao, T.J.; Tam, K.F.; Cheung, A.N.Y.; Ngan, H.Y.S. Human papillomavirus vaccine: What are women most concerned about? J. Obstet. Gynaecol. Res. 2012, 38, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Cover, J.K.; Nghi, N.Q.; LaMontagne, D.S.; Dang, T.T.H.; Hien, N.T.; Nga, L.T. Acceptance patterns and decision-making for human papillomavirus vaccination among parents in Vietnam: An in-depth qualitative study post-vaccination. BMC Public Health 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- Watson-Jones, D.; Tomlin, K.; Remes, P.; Baisley, K.; Ponsiano, R.; Soteli, S.; de Sanjose, S.; Changalucha, J.; Kapiga, S.; Hayes, R.J. Reasons for receiving or not receiving HPV vaccination in primary schoolgirls in Tanzania: A case control study. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- Perkins, R.B.; Clark, J.A. What affects human papillomavirus vaccination rates? A qualitative analysis of providers’ perceptions. Womens Health Issues 2012, 22, E379–E386. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.W.H.; Kwan, T.T.C.; Tam, K.F.; Chan, K.K.L.; Young, P.M.C.; Lo, S.S.T.; Cheung, A.N.Y.; Ngan, H.Y.S. Beliefs about cervical cancer and human papillomavirus (HPV) and acceptability of HPV vaccination among Chinese women in Hong Kong. Prev. Med. 2007, 45, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Constantine, N.A.; Jerman, P. Acceptance of human papillomavirus vaccination among Californian parents of daughters: A representative statewide analysis. J. Adolesc. Health 2007, 40, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Olshen, E.; Woods, E.R.; Austin, S.B.; Luskin, M.; Bauchner, H. Parental acceptance of the human papillomavirus vaccine. J. Adolesc. Health 2005, 37, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Waller, J.; Marlow, L.A.V.; Wardle, J. Mothers‘ attitudes towards preventing cervical cancer through human papillornavirus vaccination: A qualitative study. Cancer Epidemiol Biomarker. 2006, 15, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.P.; Porch, E.; McWeeney, M.; Ohman-Strickland, P.; Levine, J.P. Knowledge and concerns related to the human papillomavirus vaccine among underserved Latina women. J. Low. Genit. Tract Dis. 2010, 14, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Marshall, H.; Ryan, P.; Roberton, D.; Baghurst, P. A cross-sectional survey to assess community attitudes to introduction of human papillomavirus vaccine. Aust. N. Z. J. Public Health 2007, 31, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Haesebaert, J.; Lutringer-Magnin, D.; Kalecinski, J.; Barone, G.; Jacquard, A.C.; Leocmach, Y.; Regnier, V.; Vanhems, P.; Chauvin, F.; Lasset, C. Disparities of perceptions and practices related to cervical cancer prevention and the acceptability of HPV vaccination according to educational level in a French cross-sectional survey of 18–65 years old women. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Bowyer, H.L.; Marlow, L.A.V.; Hibbitts, S.; Pollock, K.G.; Waller, J. Knowledge and awareness of HPV and the HPV vaccine among young women in the first routinely vaccinated cohort in England. Vaccine 2013, 31, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.Y.; Kim, J.S. Knowledge, attitudes of human papillomavirus vaccine, and intention to obtain vaccine among Korean female undergraduate students. Women Health 2011, 51, 759–776. [Google Scholar] [CrossRef] [PubMed]
- Makwe, C.C.; Anorlu, R.I.; Odeyemi, K.A. Human papillomavirus (HPV) infection and vaccines: Knowledge, attitude and perception among female students at the University of Lagos, Lagos, Nigeria. J. Epidemiol. Glob. Health 2012, 2, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Reimer, R.A.; Schommer, J.A.; Houlihan, A.E.; Gerrard, M. Ethnic and gender differences in HPV knowledge, awareness, and vaccine acceptability among White and Hispanic men and women. J. Commun. Health 2014, 39, 274–284. [Google Scholar] [CrossRef] [PubMed]
- The Family Planning Association of Hong Kong. Report of Youth Sexuality Study 2011; The Family Planning Association of Hong Kong: Hong Kong, China, 2013. [Google Scholar]
- Sample Size Calculator. Available online: http://www.surveymonkey.com/mp/sample-size-calculator/ (accessed on 15 February 2016).
- Commonly Used Statistical Tables: Student (Headcount). Available online: http://cdcf.ugc.edu.hk/cdcf/searchStatSiteReport.do (accessed on 1 April 2016).
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hair, J.F. Multivariate Data Analysis, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Levy-Bruhl, D.; Bousquet, V.; King, L.; O’Flanagan, D.; Bacci, S.; Lopalco, P.; Salmaso, S. The current state of introduction of HPV vaccination into national immunisation schedules in Europe: Results of the VENICE 2008 survey. Eur. J. Cancer 2009, 45, 2709–2713. [Google Scholar] [CrossRef] [PubMed]
- Bang, K.-S.; Sung, S.; Koo, B.; Kim, M.; Kim, Y.; Kim, J.; Ryu, S. Female university students‘ HPV-related knowledge and influencing factors on HPV vaccination. J. Korean Oncol. Nurs. 2011, 11, 186–192. [Google Scholar] [CrossRef]
- Wong, L.P. Young multiethnic women’s attitudes toward the HPV vaccine and HPV vaccination. Int. J. Gynecol. Obstet. 2008, 103, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, G.; Abbate, R.; Liguori, G.; Albano, L.; Angelillo, I. Human papillomavirus and vaccination: Knowledge, attitudes, and behavioural intention in adolescents and young women in Italy. Br. J. Cancer 2008, 99, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Dillard, J.P.; Spear, M.E. Knowledge of human papillomavirus and perceived barriers to vaccination in a sample of US female college students. J. Am. Coll. Health 2010, 59, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Behav. 1984, 11, 1–47. [Google Scholar] [CrossRef]
- Wu, C.S.T.; Kwong, E.W.Y.; Wong, H.T.; Lo, S.H.; Wong, A.S.W. Beliefs and knowledge about vaccination against AH1N1pdm09 infection and uptake factors among Chinese parents. Int. J. Environ. Res. Public Health 2014, 11, 1989–2002. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.S.C.; Ng, B.H.Y.; Lo, W.K.; Cheung, T.H.; Chung, T.K.H. Adolescent girls’ attitudes on human papillomavirus vaccination. J. Pediatr. Adolesc. Gynecol. 2009, 22, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Aronson, E.; Wilson, T.D.; Akert, R.M. Social Psychology, 8th ed.; Pearson: Boston, MA, USA, 2013. [Google Scholar]
- Gutierrez, B.; Leung, A.; Jones, K.T.; Smith, P.; Silverman, R.; Frank, I.; Leader, A.E. Acceptability of the human papillomavirus vaccine among urban adolescent males. Am. J. Mens Health 2013, 7, 27–36. [Google Scholar] [CrossRef]

{kind=link}
| Variable | n (%) | |
|---|---|---|
| Gender | Male | 203 (46.5) |
| Female | 234 (53.5) | |
| Program | Related to healthcare | 232 (53.1) |
| Not related to healthcare | 205 (46.9) | |
| Age | 18–21 | 291 (66.6) |
| 22–25 | 146 (33.4) | |
| Monthly Income | <HK$3000 | 294 (67.3) |
| HK$3001–$6000 | 107 (24.5) | |
| HK$6001–$9000 | 16 (3.7) | |
| >HK$9000 | 20 (4.6) | |
| Residence Status | Live with family | 395 (90.4) |
| Shared Dormitory | 31 (7.1) | |
| Living Alone | 7 (1.6) | |
| Others | 4 (0.9) | |
| Religion | Buddhism | 18 (4.1) |
| Catholicism | 9 (2.1) | |
| Christianity | 93 (21.4) | |
| Others | 1 (0.2) | |
| None | 314 (72.2) | |
| Relationship Status | Single | 276 (63.2) |
| In a relationship with 1 person | 159 (36.4) | |
| In a relationship with >1 person | 2 (0.5) | |
| Had Sexual Experience | 73 (17.0) | |
| Variable | n (%) | |
|---|---|---|
| History of genital warts | 2 (0.5) | |
| History of anal cancer | 1 (0.2) | |
| History of cervical cancer | 0 (0) | |
| Heard about cervical cancer | 384 (87.9) | |
| Source of information about cervical cancer | Television | 322 (73.7) |
| Newspapers/Magazines | 187 (42.8) | |
| Internet | 184 (42.1) | |
| Healthcare Provider | 176 (40.3) | |
| Friend/Relative | 110 (25.2) | |
| Radio | 110 (25.2) | |
| Others | 45 (10.3) | |
| Heard about the HPV vaccine | 403 (92.2) | |
| Source of information about the HPV vaccine | Television | 330 (75.5) |
| Internet | 191 (43.7) | |
| Newspapers/Magazines | 177 (40.5) | |
| Healthcare Provider | 176 (40.3) | |
| Friend/Relative | 133 (30.4) | |
| Radio | 111 (25.4) | |
| Others | 52 (11.9) | |
| History of vaccination | Female | 57 (24.4) |
| Male | 1 (0.5) | |
| Total | 58 (13.3) | |
| Willingness to receive the HPV vaccine if it can protect against cervical/anal cancer and genital warts | Would like to be vaccinated | 300 (69.6) |
| Would not like to be vaccinated | 84 (19.5) | |
| Cannot make a decision | 47 (10.9) | |
| Variables | n (%) | |
|---|---|---|
| If the HPV vaccine is available and deliverable in the places listed below, which option would make it more likely that you would go to get vaccinated against HPV? | Health clinics in universities | 189 (43.2) |
| Public hospitals | 149 (34.1) | |
| General practitioners | 97 (22.2) | |
| Private hospitals | 63 (14.4) | |
| If the HPV vaccine can protect against both cervical cancer and genital warts, who should get the vaccination? | Both males and females should get vaccinated equally | 339 (77.6) |
| Females should get it rather than males + | 68 (15.6) | |
| Females only | 28 (6.4) | |
| Males only | 2 (0.5) | |
| Males should get it rather than females ++ | 0 (0) | |
| If the HPV vaccine is beneficial for adolescents who are not sexually active, which of the following would be the ideal age for vaccination? | 15–16 years old | 117 (26.8) |
| 17–18 years old | 97 (22.2) | |
| 13–14 years old | 95 (21.7) | |
| 11–12 years old | 79 (18.1) | |
| ≤10 years old | 45 (10.3) | |
| >18 years old | 4 (0.9) | |
| Questions on Attitude towards HPV Vaccination | Males | Females | Total | t-Statistics |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| 2.15 (1.02) | 2.32 (0.89) | 2.24 (0.96) | −1.84 |
| 4.03 (0.87) | 4.04 (0.73) | 4.04 (0.80) | −0.05 |
| 4.25 (0.78) | 4.36 (0.71) | 4.31 (0.74) | −1.64 |
| 2.55 (1.02) | 2.71 (0.99) | 2.64 (1.01) | −1.65 |
| 3.93 (0.96) | 4.06 (0.92) | 4.00 (0.94) | −1.44 |
| 3.72 (0.85) | 3.72 (0.86) | 3.72 (0.85) | −0.04 |
| 4.12 (0.81) | 4.26 (0.80) | 4.19 (0.80) | −1.86 |
| 4.11 (0.99) | 4.34 (0.88) | 4.23 (0.93) | −2.52 * |
| 4.03 (0.86) | 4.18 (0.81) | 4.11 (0.84) | −1.87 |
| 3.88 (0.83) | 3.91 (0.83) | 3.89 (0.83) | −0.31 |
| 2.79 (0.96) | 3.02 (1.03) | 2.91 (1.00) | −2.34 * |
| 3.56 (0.95) | 3.81 (0.91) | 3.70 (0.93) | −2.76 ** |
| 3.85 (0.87) | 4.04 (0.85) | 3.95 (0.86) | −2.31 * |
| 3.96 (0.82) | 4.04 (0.77) | 4.00 (0.79) | −1.03 |
| 3.33 (0.95) | 3.43 (0.90) | 3.38 (0.92) | −1.08 |
| 3.08 (0.98) | 3.18 (0.86) | 3.13 (0.92) | −1.15 |
| 3.80 (0.82) | 3.84 (0.84) | 3.82 (0.83) | −0.44 |
| 3.40 (0.77) | 3.43 (0.75) | 3.42 (0.76) | −0.32 |
| 3.40 (0.82) | 3.40 (0.80) | 3.40 (0.81) | 0.08 |
| 2.15 (0.88) | 2.13 (0.73) | 2.14 (0.80) | 0.31 |
| 3.24 (0.89) | 3.38 (0.87) | 3.32 (0.88) | −1.76 |
| Question Type | Questions on HPV and HPV Vaccination | Correctly Answered | χ2 | ||
|---|---|---|---|---|---|
| Males | Females | Total | |||
| n (%) | n (%) | n (%) | |||
| Questions on HPV |
| 34 (16.7) | 27 (11.5) | 61 (14.0) | 2.46 |
| 21 (10.3) | 18 (7.7) | 39 (8.9) | 0.94 | |
| 140 (69.0) | 166 (70.9) | 306 (70.0) | 0.20 | |
| 151 (74.4) | 183 (78.2) | 334 (76.4) | 0.88 | |
| 153 (75.4) | 175 (74.8) | 328 (75.1) | 0.02 | |
| 80 (39.4) | 95 (40.6) | 175 (40.0) | 0.06 | |
| 51 (25.1) | 58 (24.8) | 109 (24.9) | 0.01 | |
| 117 (57.6) | 119 (50.9) | 236 (54.0) | 2.01 | |
| 149 (73.4) | 181 (77.4) | 330 (75.5) | 0.92 | |
| 101 (49.8) | 123 (52.6) | 224 (51.3) | 0.34 | |
| 96 (47.3) | 125 (53.4) | 221 (50.6) | 1.63 | |
| 64 (31.5) | 67 (28.6) | 131 (30.0) | 0.43 | |
| 142 (70.0) | 153 (65.4) | 295 (67.5) | 1.03 | |
| 113 (55.7) | 126 (53.8) | 239 (54.7) | 0.15 | |
| 49 (24.1) | 67 (28.6) | 116 (26.5) | 1.13 | |
| Questions on HPV vaccination |
| 117 (57.6) | 141 (60.3) | 258 (59.0) | 0.31 |
| 124 (61.1) | 142 (60.7) | 266 (60.9) | 0.01 | |
| 122 (60.1) | 164 (70.1) | 286 (65.4) | 4.79 * | |
| 71 (35.0) | 89 (38.0) | 160 (36.6) | 0.44 | |
| 97 (47.8) | 144 (61.5) | 241 (55.1) | 8.32 ** | |
| 163 (80.3) | 206 (88.0) | 369 (84.4) | 4.95 * | |
| 153 (75.4) | 196 (83.8) | 349 (79.9) | 4.76 * | |
| Predictors | B | 95% CI | t-Value | VIF | adj-R2 | |
|---|---|---|---|---|---|---|
| −1.40 | (−2.48, −0.33) | −2.57 * | 1.05 | 0.33 | |
| 0.35 | (0.04, 0.66) | 2.22 * | 1.07 | ||
| −1.90 | (−2.57, −1.24) | −5.60 *** | 1.04 | ||
| Knowledge of vaccination |
| 2.18 | (0.78, 3.58) | 3.06 ** | 1.31 | |
| 1.90 | (0.74, 3.07) | 3.22 ** | 1.23 | ||
| 2.30 | (1.01, 3.60) | 3.49 ** | 1.09 | ||
| 1.94 | (0.72, 3.17) | 3.12 ** | 1.31 | ||
| 1.76 | (0.65, 2.87) | 3.12 ** | 1.12 | ||
| 2.09 | (0.56, 3.61) | 2.69 ** | 1.05 | ||
| 1.36 | (0.19, 2.53) | 2.29 * | 1.20 | ||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, V.C.L.; Wong, H.T.; Yeung, P.C.A.; Choi, Y.K.; Fok, M.S.Y.; Mak, O.I.; Wong, H.Y.; Wong, K.H.; Wong, S.Y.; Wong, Y.S.; et al. Attitude, Acceptability and Knowledge of HPV Vaccination among Local University Students in Hong Kong. Int. J. Environ. Res. Public Health 2016, 13, 486. https://doi.org/10.3390/ijerph13050486
Chiang VCL, Wong HT, Yeung PCA, Choi YK, Fok MSY, Mak OI, Wong HY, Wong KH, Wong SY, Wong YS, et al. Attitude, Acceptability and Knowledge of HPV Vaccination among Local University Students in Hong Kong. International Journal of Environmental Research and Public Health. 2016; 13(5):486. https://doi.org/10.3390/ijerph13050486
Chicago/Turabian StyleChiang, Vico Chung Lim, Ho Ting Wong, Pui Chun Au Yeung, Yuk Ki Choi, Michelle Sum Yue Fok, Oi In Mak, Hing Yu Wong, Kim Ho Wong, Shui Yan Wong, Yee Shan Wong, and et al. 2016. "Attitude, Acceptability and Knowledge of HPV Vaccination among Local University Students in Hong Kong" International Journal of Environmental Research and Public Health 13, no. 5: 486. https://doi.org/10.3390/ijerph13050486
APA StyleChiang, V. C. L., Wong, H. T., Yeung, P. C. A., Choi, Y. K., Fok, M. S. Y., Mak, O. I., Wong, H. Y., Wong, K. H., Wong, S. Y., Wong, Y. S., & Wong, E. Y. Y. (2016). Attitude, Acceptability and Knowledge of HPV Vaccination among Local University Students in Hong Kong. International Journal of Environmental Research and Public Health, 13(5), 486. https://doi.org/10.3390/ijerph13050486