Clinical Significance of Peripheral Arterial Disease Evaluation in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
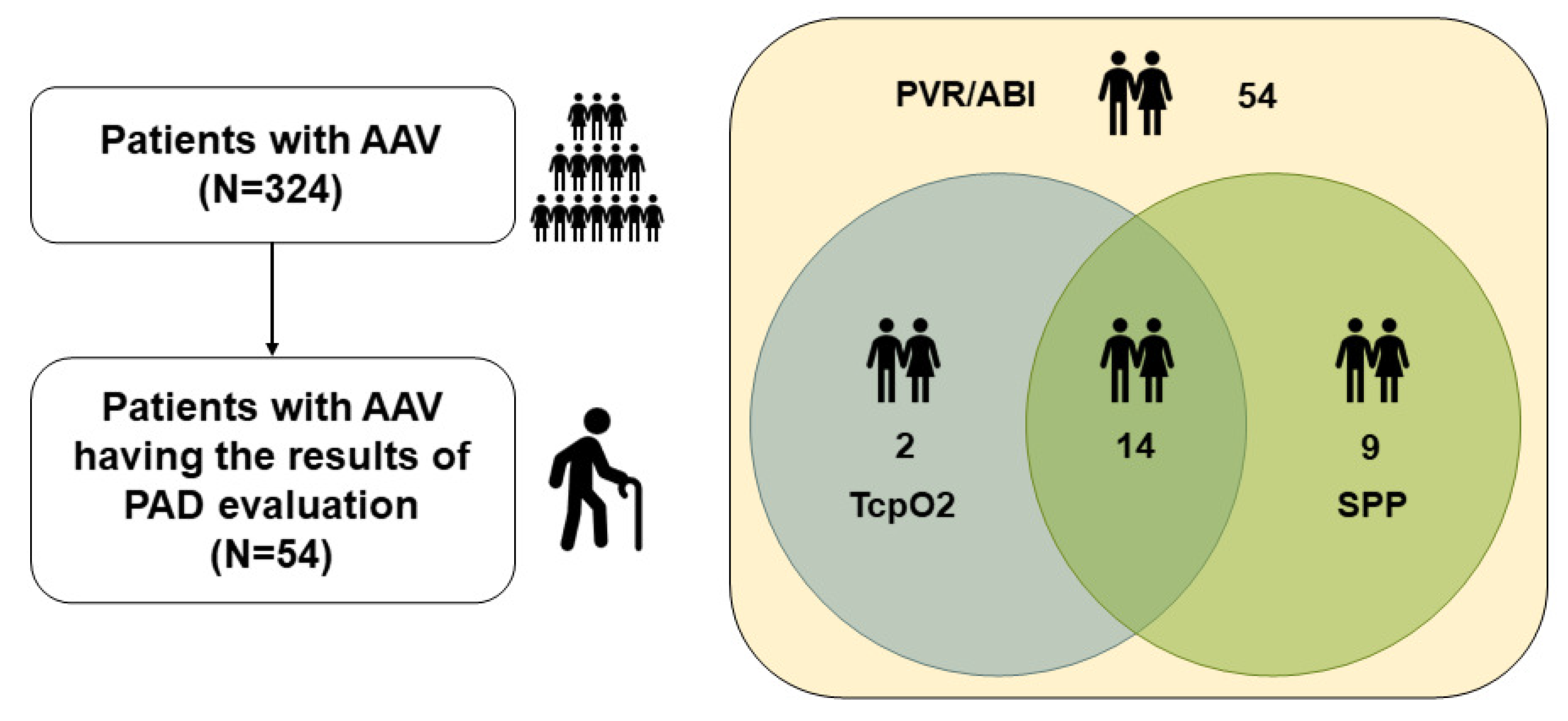
2.1. Patients
2.2. Clinical Data at PAD Evaluation
2.3. PAD Evaluation
2.4. Poor Outcomes During Follow-Up
2.5. Statistical Analyses
3. Results
3.1. Characteristics of Patients with AAV at PAD Evaluation
3.2. Results of PAD Evaluation
3.3. Concordance Rate of Abnormal PAD-Related Values Between PVR/ABI and TcpO2 or SPP
3.4. Systemic Manifestations and Poor Outcomes
3.5. Comparison of Systemic Manifestations and Poor Outcomes According to Abnormal PAD Evaluation
3.6. Comparison of Cumulative ESKD-Free Survival Rates According to Abnormal SPP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Watts, R.; Lane, S.; Hanslik, T.; Hauser, T.; Hellmich, B.; Koldingsnes, W.; Mahr, A.; Segelmark, M.; Cohen-Tervaert, J.W.; Scott, D. Development and validation of a consensus methodology for the classification of the ANCA-associated vasculitides and polyarteritis nodosa for epidemiological studies. Ann. Rheum. Dis. 2007, 66, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Millet, A.; Pederzoli-Ribeil, M.; Guillevin, L.; Witko-Sarsat, V.; Mouthon, L. Antineutrophil cytoplasmic antibody-associated vasculitides: Is it time to split up the group? Ann. Rheum. Dis. 2013, 72, 1273–1279. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.A.; Langford, C.A.; Maz, M.; Abril, A.; Gorelik, M.; Guyatt, G.; Archer, A.M.; Conn, D.L.; Full, K.A.; Grayson, P.C.; et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Arthritis Rheumatol. 2021, 73, 1366–1383. [Google Scholar] [CrossRef]
- Houben, E.; Penne, E.L.; Voskuyl, A.E.; Van Der Heijden, J.W.; Otten, R.H.J.; Boers, M.; Hoekstra, T. Cardiovascular events in anti-neutrophil cytoplasmic antibody-associated vasculitis: A meta-analysis of observational studies. Rheumatology 2018, 57, 555–562. [Google Scholar] [CrossRef]
- Xie, W.; Xiao, S.; Li, X.; Huang, J.; Zhang, Z. Cardiovascular and cerebrovascular outcomes in anti-neutrophil cytoplasmic antibody-associated vasculitis: A systematic review with meta-analysis. Autoimmun. Rev. 2024, 23, 103587. [Google Scholar] [CrossRef]
- Berti, A.; Matteson, E.L.; Crowson, C.S.; Specks, U.; Cornec, D. Risk of Cardiovascular Disease and Venous Thromboembolism Among Patients with Incident ANCA-Associated Vasculitis: A 20-Year Population-Based Cohort Study. Mayo Clin. Proc. 2018, 93, 597–606. [Google Scholar] [CrossRef]
- Galanakis, N.; Maris, T.G.; Kontopodis, N.; Tsetis, K.; Kehagias, E.; Tsetis, D. Perfusion imaging techniques in lower extremity peripheral arterial disease. Br. J. Radiol. 2022, 95, 20211203. [Google Scholar] [CrossRef]
- Shwaiki, O.; Rashwan, B.; Fink, M.A.; Kirksey, L.; Gadani, S.; Karuppasamy, K.; Melzig, C.; Thompson, D.; D’Amico, G.; Rengier, F.; et al. Lower extremity CT angiography in peripheral arterial disease: From the established approach to evolving technical developments. Int. J. Cardiovasc. Imaging 2021, 37, 3101–3114. [Google Scholar] [CrossRef]
- Danieluk, A.; Chlabicz, S. Automated Measurements of Ankle-Brachial Index: A Narrative Review. J. Clin. Med. 2021, 10, 5161. [Google Scholar] [CrossRef]
- Hashimoto, T.; Ichihashi, S.; Iwakoshi, S.; Kichikawa, K. Combination of pulse volume recording (PVR) parameters and ankle-brachial index (ABI) improves diagnostic accuracy for peripheral arterial disease compared with ABI alone. Hypertens. Res. 2016, 39, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Kmiec, M.M.; Hou, H.; Lakshmi Kuppusamy, M.; Drews, T.M.; Prabhat, A.M.; Petryakov, S.V.; Demidenko, E.; Schaner, P.E.; Buckey, J.C.; Blank, A.; et al. Transcutaneous oxygen measurement in humans using a paramagnetic skin adhesive film. Magn. Reson. Med. 2019, 81, 781–794. [Google Scholar] [CrossRef] [PubMed]
- Catella, J.; Long, A.; Mazzolai, L. What Is Currently the Role of TcPO2 in the Choice of the Amputation Level of Lower Limbs? A Comprehensive Review. J. Clin. Med. 2021, 10, 1413. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Chen, G.; Wu, P.; Han, C.; Ho, J.K. Skin perfusion pressure as a predictor of ischemic wound healing potential. Biomed. Rep. 2018, 8, 330–334. [Google Scholar] [CrossRef]
- Lee, Y.J.; Ahn, C.M.; Ko, Y.G.; Park, K.H.; Lee, J.W.; Lee, S.J.; Hong, S.J.; Kim, J.S.; Kim, B.K.; Choi, D. Skin Perfusion Pressure Predicts Early Wound Healing After Endovascular Therapy in Chronic Limb Threatening Ischaemia. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 909–917. [Google Scholar] [CrossRef]
- Suppiah, R.; Robson, J.C.; Grayson, P.C.; Ponte, C.; Craven, A.; Khalid, S.; Judge, A.; Hutchings, A.; Merkel, P.A.; Luqmani, R.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for microscopic polyangiitis. Ann. Rheum. Dis. 2022, 81, 321–326. [Google Scholar] [CrossRef]
- Robson, J.C.; Grayson, P.C.; Ponte, C.; Suppiah, R.; Craven, A.; Judge, A.; Khalid, S.; Hutchings, A.; Watts, R.A.; Merkel, P.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for granulomatosis with polyangiitis. Ann. Rheum. Dis. 2022, 81, 315–320. [Google Scholar] [CrossRef]
- Grayson, P.C.; Ponte, C.; Suppiah, R.; Robson, J.C.; Craven, A.; Judge, A.; Khalid, S.; Hutchings, A.; Luqmani, R.A.; Watts, R.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis. Ann. Rheum. Dis. 2022, 81, 309–314. [Google Scholar] [CrossRef]
- Pyo, J.Y.; Lee, L.E.; Park, Y.B.; Lee, S.W. Comparison of the 2022 ACR/EULAR Classification Criteria for Antineutrophil Cytoplasmic Antibody-Associated Vasculitis with Previous Criteria. Yonsei Med. J. 2023, 64, 11–17. [Google Scholar] [CrossRef]
- Pyo, J.Y.; Ahn, S.S.; Song, J.J.; Park, Y.B.; Lee, S.W. Application of the 2022 ACR/EULAR criteria for microscopic polyangiitis to patients with previously diagnosed microscopic polyangiitis. Clin. Exp. Rheumatol. 2023, 41, 792–799. [Google Scholar] [CrossRef]
- Pyo, J.Y.; Ahn, S.S.; Song, J.J.; Park, Y.B.; Lee, S.W. Reclassification of previously diagnosed GPA patients using the 2022 ACR/EULAR classification criteria. Rheumatology 2023, 62, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Pyo, J.Y.; Ahn, S.S.; Song, J.J.; Park, Y.B.; Lee, S.W. The Reclassification of Patients with Previously Diagnosed Eosinophilic Granulomatosis with Polyangiitis Based on the 2022 ACR/EULAR Criteria for Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. J. Rheumatol. 2023, 50, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Mukhtyar, C.; Lee, R.; Brown, D.; Carruthers, D.; Dasgupta, B.; Dubey, S.; Flossmann, O.; Hall, C.; Hollywood, J.; Jayne, D.; et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann. Rheum. Dis. 2009, 68, 1827–1832. [Google Scholar] [CrossRef] [PubMed]
- Guillevin, L.; Pagnoux, C.; Seror, R.; Mahr, A.; Mouthon, L.; Le Toumelin, P.; French Vasculitis Study Group. The Five-Factor Score revisited: Assessment of prognoses of systemic necrotizing vasculitides based on the French Vasculitis Study Group (FVSG) cohort. Medicine 2011, 90, 19–27. [Google Scholar] [CrossRef]
- Bossuyt, X.; Cohen Tervaert, J.W.; Arimura, Y.; Blockmans, D.; Flores-Suárez, L.F.; Guillevin, L.; Hellmich, B.; Jayne, D.; Jennette, J.C.; Kallenberg, C.G.; et al. Position paper: Revised 2017 international consensus on testing of ANCAs in granulomatosis with polyangiitis and microscopic polyangiitis. Nat. Rev. Rheumatol. 2017, 13, 683–692. [Google Scholar] [CrossRef]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Hankey, G.J. Stroke. Lancet 2017, 389, 641–654. [Google Scholar] [CrossRef]
- Kotecha, T.; Rakhit, R.D. Acute coronary syndromes. Clin. Med. 2016, 16, s43–s48. [Google Scholar] [CrossRef]
- Del Conde, I.; Benenati, J.F. Noninvasive Testing in Peripheral Arterial Disease. Interv. Cardiol. Clin. 2014, 3, 469–478. [Google Scholar] [CrossRef]
- Kitching, A.R.; Anders, H.J.; Basu, N.; Brouwer, E.; Gordon, J.; Jayne, D.R.; Kullman, J.; Lyons, P.A.; Merkel, P.A.; Savage, C.O.; et al. ANCA-associated vasculitis. Nat. Rev. Dis. Primers 2020, 6, 71. [Google Scholar] [CrossRef]
- Flossmann, O.; Bacon, P.; De Groot, K.; Jayne, D.; Rasmussen, N.; Seo, P.; Westman, K.; Luqmani, R. Development of comprehensive disease assessment in systemic vasculitis. Ann. Rheum. Dis. 2007, 66, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, S.; Kotani, T.; Wakura, R.; Suzuka, T.; Kuwabara, H.; Kiboshi, T.; Wada, Y.; Shiba, H.; Hata, K.; Shoda, T.; et al. Examination of nailfold videocapillaroscopy findings in ANCA-associated vasculitis. Rheumatology 2023, 62, 747–757. [Google Scholar] [CrossRef] [PubMed]
- Kronbichler, A.; Shin, J.I.; Lee, K.H.; Nakagomi, D.; Quintana, L.F.; Busch, M.; Craven, A.; Luqmani, R.A.; Merkel, P.A.; Mayer, G.; et al. Clinical associations of renal involvement in ANCA-associated vasculitis. Autoimmun. Rev. 2020, 19, 102495. [Google Scholar] [CrossRef]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5, 56. [Google Scholar] [CrossRef]
- Hendrickson, M.J.; Wallace, Z.S. Mechanisms and Screening for Atherosclerosis in Adults with Vasculitis. Arterioscler. Thromb. Vasc. Biol. 2025, 45, 3–10. [Google Scholar] [CrossRef]
- Libby, P. The changing landscape of atherosclerosis. Nature 2021, 592, 524–533. [Google Scholar] [CrossRef]
- Petermann Smits, D.R.; Wilde, B.; Kianersi Adegani, M.; de Jongh, H.; van Paassen, P.; Cohen Tervaert, J.W. Metabolic syndrome in ANCA-associated vasculitis. Rheumatology 2013, 52, 197–203. [Google Scholar] [CrossRef]
- Lee, S.B.; Kwon, H.C.; Kang, M.I.; Park, Y.B.; Park, J.Y.; Lee, S.W. Increased prevalence rate of metabolic syndrome is an independent predictor of cardiovascular disease in patients with antineutrophil cytoplasmic antibody-associated vasculitis. Rheumatol. Int. 2022, 42, 291–302. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables Regarding Clinical Data | Value |
|---|---|
| Demographic data | |
| Age (years) | 67.0 (56.0–71.0) |
| Male sex (n, (%)) | 26 (48.1) |
| Female sex (n, (%)) | 28 (51.9) |
| BMI (kg/m2) | 22.9 (21.4–24.9) |
| Ex-smoker (n, (%)) | 3 (5.6) |
| AAV subtype (n, (%)) | |
| MPA | 12 (22.2) |
| GPA | 10 (18.5) |
| EGPA | 32 (59.3) |
| ANCA type and positivity (n, (%)) | |
| MPO-ANCA (or P-ANCA) positivity | 41 (75.9) |
| PR3-ANCA (or C-ANCA) positivity | 5 (9.3) |
| Both ANCA positivity | 1 (1.9) |
| ANCA negativity | 9 (16.7) |
| AAV-specific indices | |
| BVAS | 12.0 (5.8–19.0) |
| FFS | 1.0 (0–3.0) |
| Laboratory results | |
| White blood cell count (/mm3) | 9750.0 (6877.5–13,140.0) |
| Haemoglobin (g/dL) | 11.5 (10.0–12.7) |
| Platelet count (×1000/mm3) | 329.0 (240.5–396.3) |
| Fasting glucose (mg/dL) | 101.0 (88.0–114.5) |
| Blood urea nitrogen (mg/dL) | 16.7 (12.3–23.2) |
| Serum creatinine (mg/dL) | 0.8 (0.7–1.1) |
| Total cholesterol (mg/dL) | 164.0 (130.8–194.0) |
| Serum total protein (g/dL) | 6.8 (6.1–7.2) |
| Serum albumin (g/dL) | 3.6 (3.1–4.1) |
| Complement 3 (mg/dL) | 122.4 (103.0–134.3)) |
| Complement 4 (mg/dL) | 25.3 (20.2–31.2) |
| Acute-phase reactants | |
| ESR (mm/hr) | 86.5 (23.8–120.0) |
| CRP (mg/L) | 19.0 (1.8–105.1) |
| Comorbidities (n, (%)) | |
| Hypertension | 16 (29.6) |
| Type 2 diabetes mellitus | 17 (31.5) |
| Dyslipidaemia | 9 (16.7) |
| Results of PAD evaluation | |
| Continuous variables | |
| PVR/ABI right (n = 54) | 1.19 (1.10–1.25) |
| PVR/ABI left (n = 54) | 1.19 (1.11–1.26) |
| TcpO2 right (mmHg) (n = 16) | 49.0 (38.3–58.3) |
| TcpO2 left (mmHg) (n = 16) | 48.0 (33.8–51.0) |
| SPP right (mmHg) (n = 23) | 56.0 (50.0–68.0) |
| SPP left (mmHg) (n = 23) | 57.0 (50.0–66.0) |
| Abnormal results ((n, (%)) | |
| Abnormal any PVR/ABI (n = 54) | 3 (5.6) |
| Abnormal any TcpO2 (n = 16) | 6 (37.5) |
| Abnormal any SPP (n = 23) | 6 (26.1) |
| Time gap between AAV diagnosis and PAD evaluation (months) | 9.99 (0–65.9) |
| Patients with AAV with both PVR/ABI and TcpO2 results (n = 16) | ||
| Normal PVR/ABI | Abnormal PVR/ABI | |
| Normal TcpO2 | 9 (56.3) | 1 (6.3) |
| Abnormal TcpO2 | 6 (37.5) | 0 (0) |
| Patients with AAV with both PVR and SPP results (n = 23) | ||
| Normal PVR/ABI | Abnormal PVR/ABI | |
| Normal SPP | 15 (65.2) | 2 (8.7) |
| Abnormal SPP | 5 (21.7) | 1 (4.4) |
| Variable | Value |
|---|---|
| At PAD evaluation | |
| Systemic manifestations (n, (%)) | |
| General manifestation | 21 (38.9) |
| Cutaneous manifestation | 11 (20.4) |
| Mucous/Ocular manifestation | 2 (3.7) |
| Otorhinolaryngological manifestation | 24 (44.4) |
| Pulmonary manifestation | 36 (66.7) |
| Cardiovascular manifestation | 2 (3.7) |
| Gastrointestinal manifestation | 1 (1.9) |
| Renal manifestation | 33 (61.1) |
| Nervous systemic manifestation | 28 (51.9) |
| During follow-up | |
| Poor outcomes | |
| ACM | 5 (9.3) |
| ESKD | 2 (3.7) |
| CVA | 10 (18.5) |
| ACS | 4 (7.4) |
| PVR/ABI (n = 54) | TcpO2 (n = 16) | SPP (n = 23) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Normal PVR/ABI (n = 51) | Abnormal PVR/ABI (n = 3) | p Value | Normal TcpO2 (n = 10) | Abnormal TcpO2 (n = 6) | p Value | Normal SPP (n = 17) | Abnormal SPP (n = 6) | p Value | |
| Systemic manifestations based on BVAS | |||||||||
| General | 20 (39.2) | 1 (33.3) | 1.000 | 2 (20.0) | 4 (66.7) | 0.118 | 4 (23.5) | 2 (33.3) | 0.632 |
| Cutaneous | 10 (19.6) | 1 (33.3) | 0.502 | 0 (0) | 2 (33.3) | 0.125 | 1 (5.9) | 5 (83.3) | 0.001 |
| Mucous/ocular | 2 (3.9) | 0 (0) | 1.000 | 0 (0) | 0 (0) | N/A | 1 (5.9) | 0 (0) | 1.000 |
| Otorhinolaryngological | 23 (45.1) | 1 (33.3) | 1.000 | 5 (50.0) | 1 (16.7) | 0.307 | 6 (35.3) | 1 (16.7) | 0.621 |
| Pulmonary | 35 (68.6) | 1 (33.3) | 0.255 | 9 (90.0) | 5 (83.3) | 1.000 | 14 (82.4) | 3 (50.0) | 0.279 |
| Cardiovascular | 2 (3.9) | 0 (0) | 1.000 | 1 (10.0) | 0 (0) | 1.000 | 1 (5.9) | 0 (0) | 1.000 |
| Gastrointestinal | 1 (2.0) | 0 (0) | 1.000 | 0 (0) | 0 (0) | N/A | 0 (0) | 0 (0) | N/A |
| Renal | 32 (62.7) | 1 (33.3) | 0.553 | 3 (30.0) | 4 (66.7) | 0.302 | 7 (41.2) | 6 (100) | 0.012 |
| Nervous systemic | 27 (52.9) | 1 (33.3) | 0.604 | 6 (60.0) | 3 (50.0) | 1.000 | 11 (64.7) | 2 (33.3) | 0.341 |
| Poor outcomes | |||||||||
| ACM | 4 (7.8) | 1 (33.3) | 0.257 | 1 (10.0) | 0 (0) | 1.000 | 1 (5.9) | 1 (16.7) | 0.462 |
| ESKD | 1 (2.0) | 1 (33.3) | 0.109 | 0 (0) | 0 (0) | N/A | 0 (0) | 1 (16.7) | 0.261 |
| CVA | 10 (19.6) | 0 (0) | 1.000 | 0 (0) | 0 (0) | N/A | 2 (11.8) | 0 (0) | 1.000 |
| ACS | 4 (7.8) | 0 (0) | 1.000 | 0 (0) | 0 (0) | N/A | 0 (0) | 0 (0) | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Whang, J.Y.; Lee, L.E.; Ha, J.W.; Kwon, O.C.; Park, Y.-B.; Lee, S.-W. Clinical Significance of Peripheral Arterial Disease Evaluation in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Medicina 2025, 61, 1074. https://doi.org/10.3390/medicina61061074
Whang JY, Lee LE, Ha JW, Kwon OC, Park Y-B, Lee S-W. Clinical Significance of Peripheral Arterial Disease Evaluation in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Medicina. 2025; 61(6):1074. https://doi.org/10.3390/medicina61061074
Chicago/Turabian StyleWhang, Jeong Yeop, Lucy Eunju Lee, Jang Woo Ha, Oh Chan Kwon, Yong-Beom Park, and Sang-Won Lee. 2025. "Clinical Significance of Peripheral Arterial Disease Evaluation in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis" Medicina 61, no. 6: 1074. https://doi.org/10.3390/medicina61061074
APA StyleWhang, J. Y., Lee, L. E., Ha, J. W., Kwon, O. C., Park, Y.-B., & Lee, S.-W. (2025). Clinical Significance of Peripheral Arterial Disease Evaluation in Patients with Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Medicina, 61(6), 1074. https://doi.org/10.3390/medicina61061074