
Comparison of the Effects of Spinal Anaesthesia on Frontal QRS-T Angle in Term and Post-Term Pregnancies Planned for Elective Caesarean Section: A Prospective Study

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Patient Selection
2.3. Study Design
2.4. Measurements
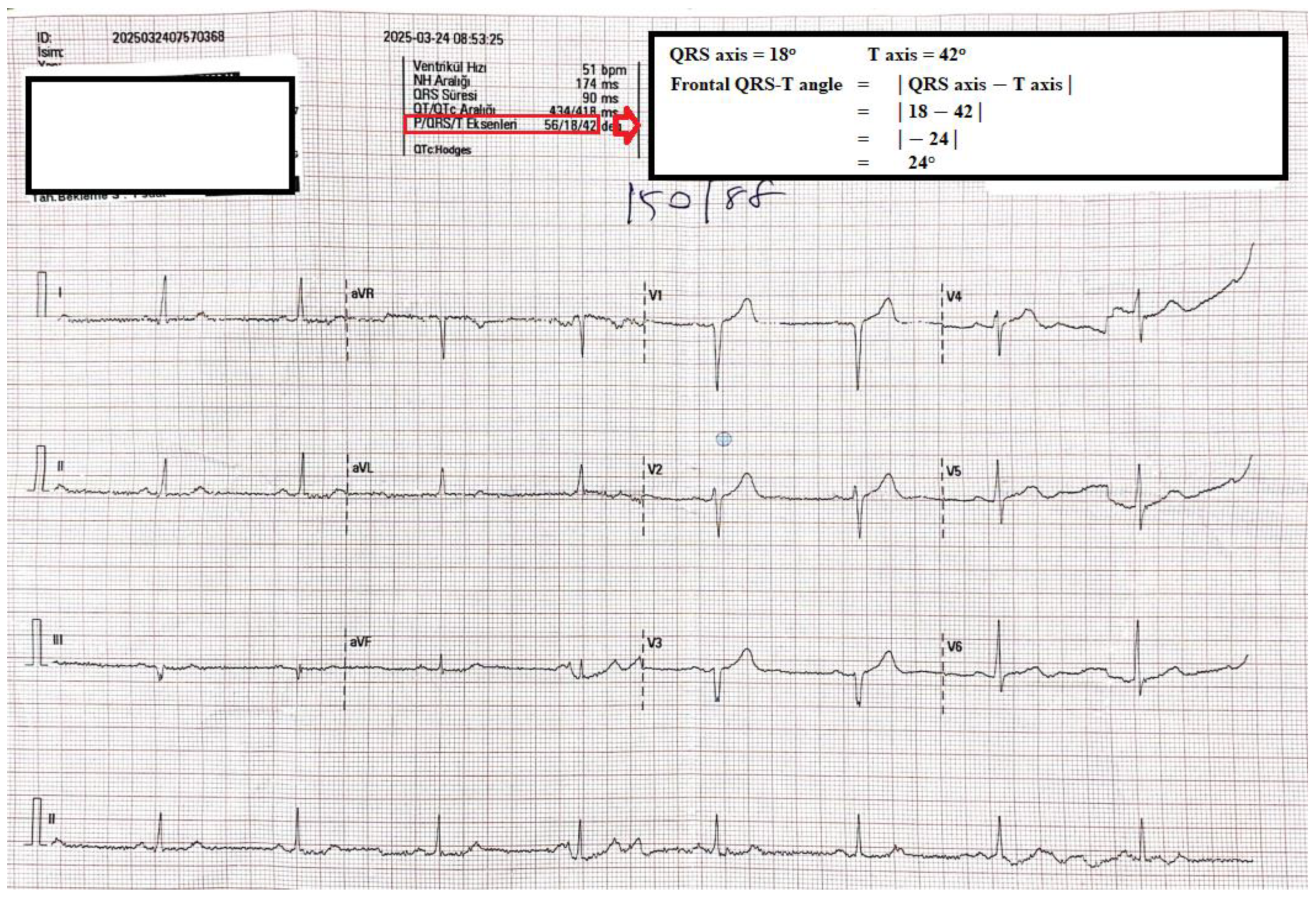
2.5. Measurement of Electrocardiographic Parameters
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ECG | electrocardiography |
| f(QRS-T) | frontal QRS-T angle |
| ASA | American Society of Anesthesiology |
| RL | Ringer Lactate |
| SpO2 | oxygen saturation |
| NIBP | non-invasive blood pressure |
| SAP | systolic arterial pressure |
| DAP | diastolic arterial pressure |
| MAP | mean arterial pressure |
| HR | heart rate |
| QTc | corrected QT |
| QTd | QT dispersion |
| BMI | body mass index |
References
- Meng, M.L.; Arendt, K.W. Obstetric Anesthesia and Heart Disease: Practical Clinical Considerations. Anesthesiology 2021, 135, 164–183. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nikoo, M.H.; Khosropanah, S.; Alborzi, S.; Aslani, A. QT Dispersion in Young, Ideal, and Old Aged Pregnancies. Int. Cardiovasc. Res. J. 2014, 8, 24–26. [Google Scholar] [PubMed] [PubMed Central]
- Deniz, Y.; Okyay, D.; Hancı, V.; Yurtlu, S.; Ayoğlu, H.; Ozkocak Turan, I. The effect of levobupivacaine and bupivacaine on QT, corrected QT (Qtc), and P wave dispersions in cesarean section. Braz. J. Anesthesiol. 2013, 63, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Karahan, M.A.; Incebiyik, A.; Buyukfirat, E.; Altay, N.; Binici, O.; Besli, F. Effect of spinal anesthesia on the QT interval in term and post-term pregnancies scheduled for elective cesarean section: A prospective study. J. Matern. Fetal Neonatal Med. 2020, 33, 3147–3151. [Google Scholar] [CrossRef] [PubMed]
- Tanrıverdi, Z.; Beşli, F.; Güngören, F.; Altıparmak, İ.H.; Biçer Yeşilay, A.; Erkuş, M.E.; Demirbağ, R. Esansiyel Hipertansiyonlu Hastalarda Sol Ventrikül Hipertrofisinin Bir Göstergesi Olarak Frontal QRS-T Açısı. DEU TıpDerg 2018, 32, 77–78. [Google Scholar]
- Bazett, H.C. An analysis of the time relations of electrocardiograms. Heart 1920, 7, 353–370. [Google Scholar] [CrossRef]
- Castro Hevia, J.; Antzelevitch, C.; Tornés Bárzaga, F.; Dorantes Sánchez, M.; Dorticós Balea, F.; Zayas Molina, R.; Quiñones Pérez, M.A.; Fayad Rodríguez, Y. Tpeak-Tend and Tpeak-Tend dispersion as risk factors for ventricular tachycardia/ventricular fibrillation in patients with the Brugada syndrome. J. Am. Coll. Cardiol. 2006, 47, 1828–1834. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Oehler, A.; Feldman, T.; Henrikson, C.A.; Tereshchenko, L.G. QRS-T angle: A review. Ann. Noninvasive Electrocardiol. 2014, 19, 534–542. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Akcay, M.; Albayrak, D.; Akcay, K.F.; Baydar, M.; Pehlivan, V.; Gögüs, N. Comparison of The Effects of VIMA with Sevoflurane and Spinal Anesthesia with Bupivacaine on QT Dispertion. Turk. J. Anest. Reanim. 2004, 2, 137–143. [Google Scholar]
- Erdogan, G.; Yontar, O.C.; Yenercag, M.; Gul, S.; Arslan, U. Frontal QRS-T angle predicts syntax score in patients with non-ST elevation myocardial infarction. J. Electrocardiol. 2020, 61, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Dogan, Z.; Yildiz, H.; Akcay, A.; Coskuner, I.; Arikan, D.C.; Silay, E.; Akbudak, I.H.; Kaya, H.; Oksuz, H. The effect of intraspinal bupivacaine versus levobupivacaine on the QTc intervals during caesarean section: A randomized, double-blind, prospective study. Basic. Clin. Pharmacol. Toxicol. 2014, 114, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Sen, S.; Ozmert, G.; Turan, H.; Caliskan, E.; Onbasili, A.; Kaya, D. The effects of spinal anesthesia on QT interval in preeclamptic patients. Anesth. Analg. 2006, 103, 1250–1255. [Google Scholar] [CrossRef] [PubMed]
- Adedapo, A.M.; Bolaji, B.O.; Adegboye, M.B.; Kolo, P.M.; Ogunmodede, J.A.; Suleiman, Z.A.; Adedapo, O.O.; Jimoh, O.S. Effect of spinal anesthesia on QT interval: Comparative study of severe pre-eclamptic and normotensive parturients undergoing cesarean section. Niger. J. Clin. Pract. 2022, 25, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Demir, F.A.; Bingöl, G.; Ersoy, I.; Arslan, A.; Ersoy, P.; Demir, M.; Ünlü, S. The Relationship between Frontal QRS-T Angle and Vitamin D Deficiency. Medicina 2024, 60, 776. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jogu, H.R.; O’Neal, W.T.; Broughton, S.T.; Shah, A.J.; Zhang, Z.M.; Soliman, E.Z. Frontal QRS-T Angle and the Risk of Atrial Fibrillation in the Elderly. Ann. Noninvasive Electrocardiol. 2017, 22, e12388. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Işık, F.; Aslan, B.; Çap, M.; Akyüz, A.; İnci, Ü.; Baysal, E. The relationship between coronary slow-flow and frontal QRS-T angle. J. Electrocardiol. 2021, 66, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Kuyumcu, M.S.; Özbay, M.B.; Özen, Y.; Yayla, Ç. Evaluation of frontal plane QRS-T angle in patients with slow coronary flow. Scand. Cardiovasc. J. 2020, 54, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Kardys, I.; Kors, J.A.; van der Meer, I.M.; Hofman, A.; van der Kuip, D.A.; Witteman, J.C. Spatial QRS-T angle predicts cardiac death in a general population. Eur. Heart J. 2003, 24, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Statters, D.J.; Malik, M.; Ward, D.E.; Camm, A.J. QT dispersion: Problems of methodology and clinical significance. J. Cardiovasc. Electrophysiol. 1994, 5, 672–685. [Google Scholar] [CrossRef] [PubMed]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E., Jr.; Ganiats, T.G.; Holmes, D.R., Jr.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 64, e139–e228. [Google Scholar] [CrossRef] [PubMed]
- Voulgari, C.; Pagoni, S.; Tesfaye, S.; Tentolouris, N. The spatial QRS-T angle: Implications in clinical practice. Curr. Cardiol. Rev. 2013, 9, 197–210. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tercan, M.; Bingol Tanriverdi, T.; Komurcu, N.; Esercan, A.; Kaya, A.; Ozyurt, E.; Tanriverdi, Z. The Relationship between Body Mass Index and Frontal QRS-T Angle in Pregnant Women Undergoing Cesarean Section with Spinal Anesthesia. Medicina 2024, 60, 1277. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, C.; Zhang, P.; Dai, C.; Zhang, J.; Wu, H.; Liu, Q.; Zhang, Z.; Yin, F.; Ni, H.; Cheng, L. Up-and-down determination of prophylactic norepinephrine boluses combined with crystalloid co-load for preventing post-spinal anesthesia hypotension during cesarean section. BMC Anesthesiol. 2025, 25, 38. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhao, Y.P.; Zhang, X.F.; Qian, J.; Xiao, F.; Chen, X.Z. Randomized Double-Blind Study of the Effect of Injectate Temperature on Intrathecal Bupivacaine Dose Requirement in Spinal Anesthesia for Cesarean Delivery. Anesth. Analg. 2025, 140, 437–443. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| Variables | Post-Term Group (n = 60) | Term Group (n = 60) | p |
|---|---|---|---|
| Age, years | 26.6 ± 4.5 | 27.3 ± 3.7 | 0.362 a |
| Weight, kg | 75.9 ± 10.2 | 73.0 ± 6.0 | 0.060 a |
| Height, cm | 161.1 ± 5.8 | 159.5 ± 3.4 | 0.076 a |
| Gravida | 4 (3–5) | 4 (3–6) | 0.300 b |
| Haemoglobin, g/dL | 11.2 ± 0.9 | 11.4 ± 1.3 | 0.421 a |
| Post-Term Group (n = 60) | Term Group (n = 60) | p | |
|---|---|---|---|
| MAP, mmHG | |||
| Pre-operative | 86.3 ± 13.5 | 87.8 ± 12.8 | 0.542 a |
| 1st minute | 79.9 ± 14.1 | 81.9 ± 11.2 | 0.392 a |
| 5th minute | 71.6 ± 12.2 | 75.9 ± 15.5 | 0.092 a |
| 10th minute | 72.3 ± 11.2 | 75.8 ± 13.7 | 0.134 a |
| Post-operative | 74.5 ± 11.5 | 76.8 ± 22.1 | 0.473 a |
| p < 0.001 c | p < 0.001 c | ||
| HR, /min | |||
| Pre-operative | 93.6 ± 8.8 | 94.7 ± 5.8 | 0.415 a |
| 1st minute | 105.6 ± 15.1 | 105.9 ± 12.1 | 0.899 a |
| 5th minute | 104.4 ± 17.9 | 105.6 ± 12.8 | 0.665 a |
| 10th minute | 102.4 ± 16.8 | 103.9 ± 11.6 | 0.583 a |
| Post-operative | 88.2 ± 17.9 | 86.2 ± 24.1 | 0.600 a |
| p < 0.001 c | p < 0.001 c | ||
| SpO2, % | |||
| Pre-operative | 98.1 ± 1.0 | 98.0 ± 1.3 | 0.575 a |
| 1st minute | 98.1 ± 1.1 | 98.0 ± 1.2 | 0.387 a |
| 5th minute | 98.0 ± 1.2 | 97.9 ± 1.3 | 0.614 a |
| 10th minute | 97.9 ± 1.1 | 98.0 ± 1.2 | 0.937 a |
| Post-operative | 98.3 ± 1.0 | 97.9 ± 1.3 | 0.111 a |
| p = 0.113 c | p = 0.181 c | ||
| Post-Term Group (n = 60) | Term Group (n = 60) | p | |
|---|---|---|---|
| QT, ms | |||
| Pre-operative | 345.1 ± 22.4 | 349.0 ± 20.9 | 0.326 a |
| Post-operative | 368.1 ± 25.4 | 364.9 ± 28.2 | 0.512 a |
| p < 0.001 d | p < 0.001 d | ||
| QTc, ms | |||
| Pre-operative | 415.7 ± 22.7 | 411.9 ± 14.2 | 0.281 a |
| Post-operative | 417.3 ± 20.5 | 410.2 ± 14.5 | 0.032 a |
| p = 0.751 d | p = 0.394 d | ||
| Frontal QRS-T angle (°) | |||
| Pre-operative | 21 (11–37) | 19 (12–23) | 0.349 b |
| Post-operative | 28 (16–55) | 22 (14–34) | 0.042 b |
| p = 0.002 e | p = 0.117 e |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaya, A.; Karahan, M.A.; Bingol Tanriverdi, T.; Esercan, A.; Bostanci Erkmen, M.; Tanriverdi, Z. Comparison of the Effects of Spinal Anaesthesia on Frontal QRS-T Angle in Term and Post-Term Pregnancies Planned for Elective Caesarean Section: A Prospective Study. Medicina 2025, 61, 919. https://doi.org/10.3390/medicina61050919
Kaya A, Karahan MA, Bingol Tanriverdi T, Esercan A, Bostanci Erkmen M, Tanriverdi Z. Comparison of the Effects of Spinal Anaesthesia on Frontal QRS-T Angle in Term and Post-Term Pregnancies Planned for Elective Caesarean Section: A Prospective Study. Medicina. 2025; 61(5):919. https://doi.org/10.3390/medicina61050919
Chicago/Turabian StyleKaya, Ahmet, Mahmut Alp Karahan, Tugba Bingol Tanriverdi, Alev Esercan, Melike Bostanci Erkmen, and Zulkif Tanriverdi. 2025. "Comparison of the Effects of Spinal Anaesthesia on Frontal QRS-T Angle in Term and Post-Term Pregnancies Planned for Elective Caesarean Section: A Prospective Study" Medicina 61, no. 5: 919. https://doi.org/10.3390/medicina61050919
APA StyleKaya, A., Karahan, M. A., Bingol Tanriverdi, T., Esercan, A., Bostanci Erkmen, M., & Tanriverdi, Z. (2025). Comparison of the Effects of Spinal Anaesthesia on Frontal QRS-T Angle in Term and Post-Term Pregnancies Planned for Elective Caesarean Section: A Prospective Study. Medicina, 61(5), 919. https://doi.org/10.3390/medicina61050919