
Optimal Localization of the Foramen Ovale for Transseptal Puncture Using the Vertebral Body Units

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
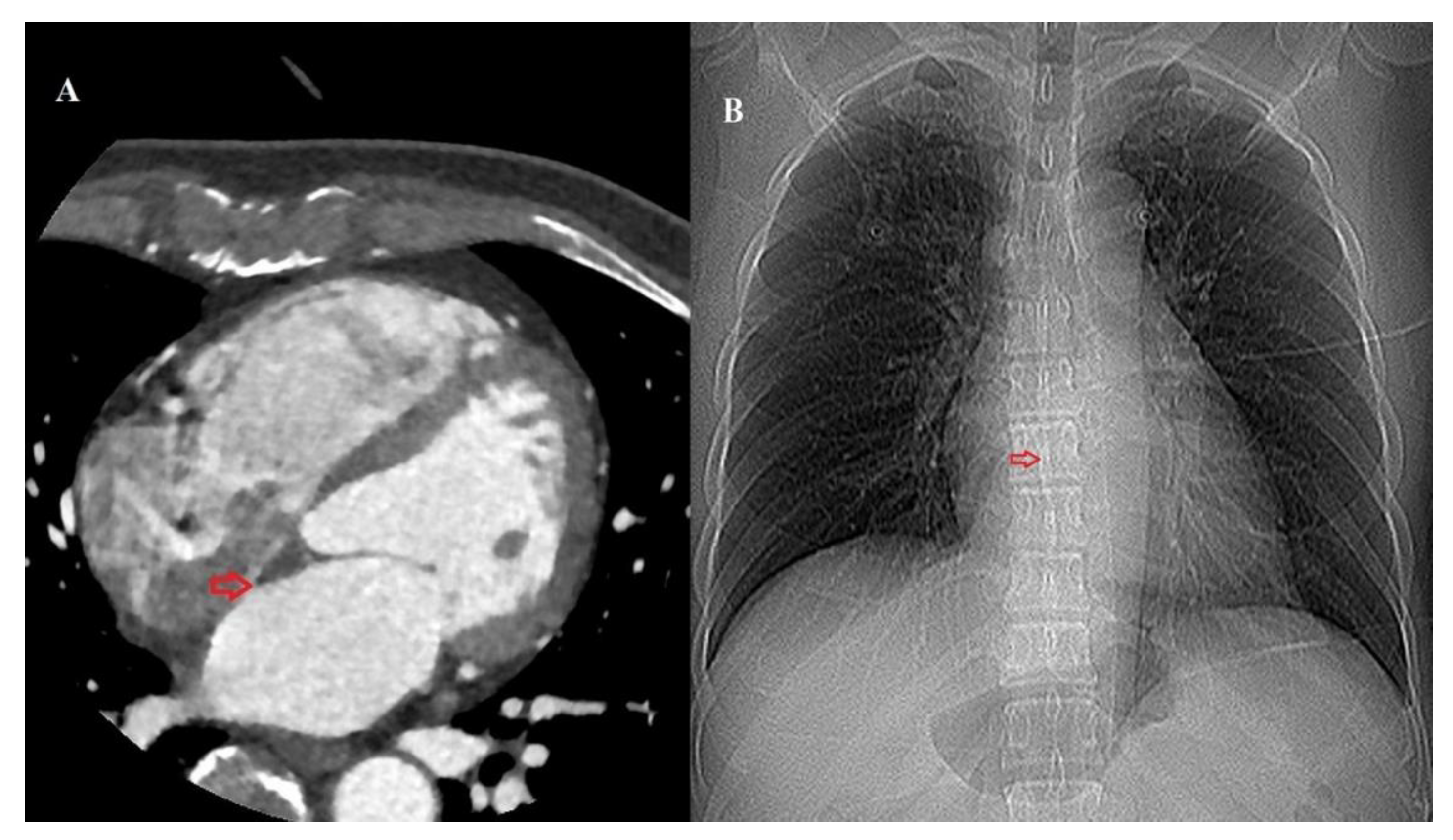
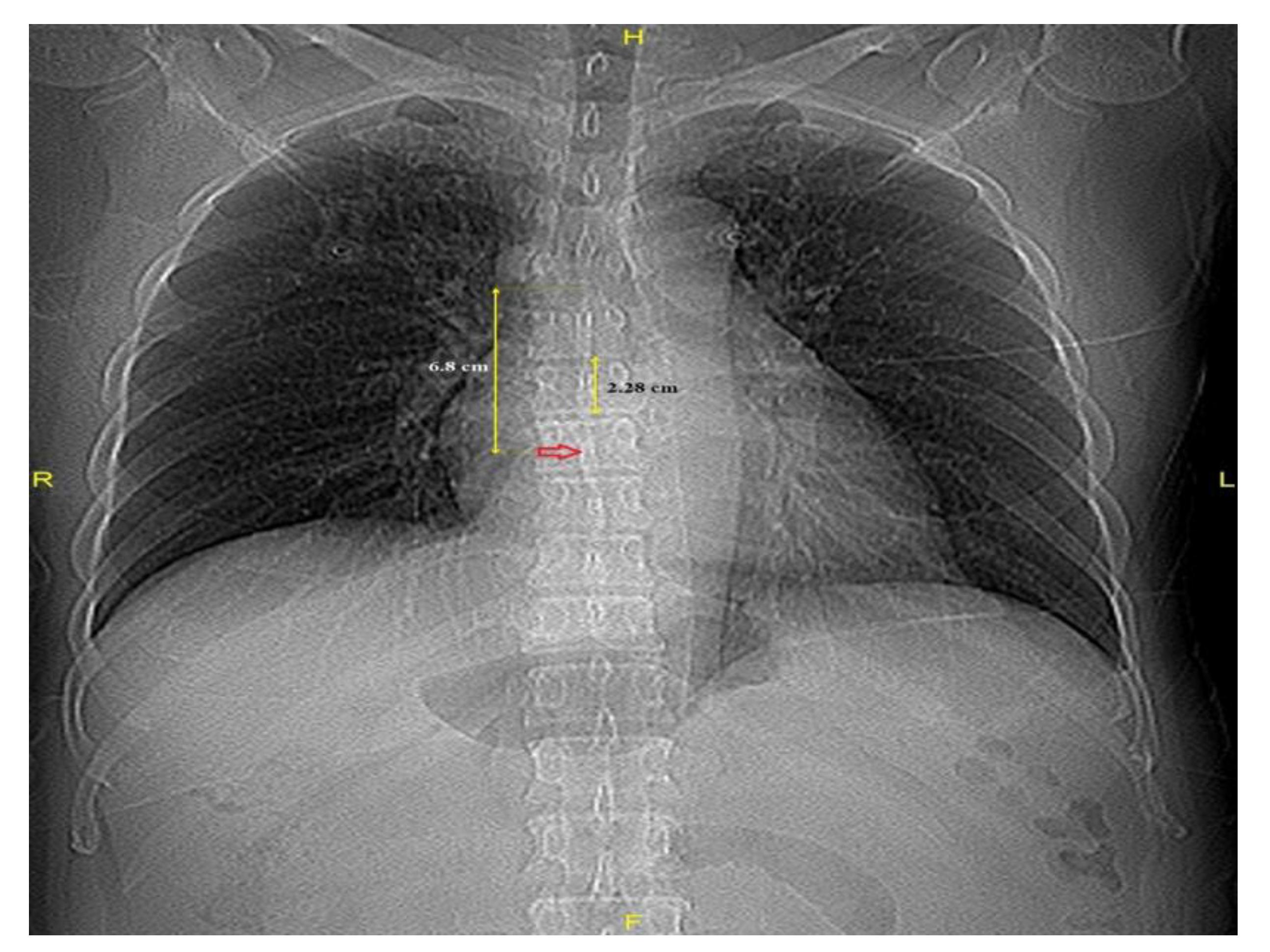
2.3. Image Acquisition and Measurement
2.4. Statistical Analysis
3. Results
3.1. Participants
3.2. Outcome Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TP | transseptal puncture |
| TEE | transesophageal |
| ICE | intracardiac echocardiography |
| ECMO | extracorporeal membrane oxygenation |
| FO | foramen ovale |
| CT | computed tomography |
| VBU | vertebral body unit |
| AF | atrial fibrillation |
| MDCT | multidetector-row computed tomography |
| BMI | body mass index |
| Carina–FO | distance from the carina to the FO |
| AP | anteroposterior |
References
- Ross, J., Jr.; Braunwald, E.; Morrow, A.G. Transseptal left atrial puncture: New technique for the measurement of left atrial pressure in man. Am. J. Cardiol. 1959, 3, 653–655. [Google Scholar] [CrossRef] [PubMed]
- Graham, L.M.; Melton, I.C.; MacDonald, S.; Crozier, I.G. Value of CT localization of the fossa ovalis prior to transseptal left heart catheterization for left atrial ablation. Europace 2007, 9, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Daoud, E.G.; Kalbfleisch, S.J.; Hummel, J.D. Intracardiac echocardiography to guide transseptal left heart catheterization for radiofrequency catheter ablation. J. Cardiovasc. Electrophysiol. 1999, 10, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.R.; Park, H.; Lee, S.E.; Ahn, J.M.; Park, D.W.; Lee, S.W.; Kim, J.J.; Park, S.J.; Hong, J.A.; Kang, P.J.; et al. Outcomes of left ventricular unloading with a transseptal cannula during extracorporeal membrane oxygenation in adults. Artif. Organs 2021, 45, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Aiyagari, R.M.; Rocchini, A.P.; Remenapp, R.T.; Graziano, J.N. Decompression of the left atrium during extracorporeal membrane oxygenation using a transseptal cannula incorporated into the circuit. Crit. Care Med. 2006, 34, 2603–2606. [Google Scholar] [CrossRef] [PubMed]
- Blomstrom-Lundqvist, C.; Olsson, S.B.; Varnauskas, E. Transseptal left heart catheterization: A review of 278 studies. Clin. Cardiol. 1986, 9, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Parwani, P.; Sharma, K. The Feasibility of Using Patent Foramen Ovale During Mitral Balloon Valvuloplasty. J. Am. Coll. Cardiol. 2012, 59 (Suppl. S13), E249. [Google Scholar] [CrossRef]
- Russo, G.; Taramasso, M.; Maisano, F. Transseptal puncture: A step-by-step procedural guide. Card. Interv. Today 2019, 13, 22–26. [Google Scholar]
- Salghetti, F.; Sieira, J.; Chierchia, G.B.; Curnis, A.; de Asmundis, C. Recognizing and reacting to complications of trans-septal puncture. Expert Rev. Cardiovasc. Ther. 2017, 15, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Adler, S.; Berman, A.; Duran, A.; Loar, D. Localization of fossa ovalis and Brockenbrough needle prior to left atrial ablation using three-dimensional mapping with EnSite Fusion. J. Interv. Card. Electrophysiol. 2011, 30, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.G.; Byun, J.H.; Hwang, S.Y.; Kim, C.W.; Shim, S.G. Use of vertebral body units to locate the cavoatrial junction for optimum central venous catheter tip positioning. Br. J. Anaesth. 2015, 115, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Baskin, K.M.; Jimenez, R.M.; Cahill, A.M.; Jawad, A.F.; Towbin, R.B. Cavoatrial junction and central venous anatomy: Implication for central venous access tip position. J. Vasc. Interv. Radiol. 2008, 19, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Pugh, K.G.; Wei, J.Y. Clinical implications of physiological changes in the aging heart. Drugs Aging 2001, 18, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Mahler, D.A.; Rosiello, R.A.; Loke, J. The aging lung. Clin. Geriatr. Med. 1986, 2, 215–225. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | N |
|---|---|
| No cardiac problems (%) | 197 (75.8) |
| 31 (11.9) |
| 32 (12.3) |
| Male (%) | 150 (57.7) |
| Age (years) | 63.8 ± 13.5 |
| Weight (kg) | 66.2 ± 13.3 |
| Height (cm) | 162.9 ± 9.4 |
| BSA (m2) | 1.7 ± 0.2 |
| BMI (kg/m2) | 24.8 ± 3.9 |
| DM (%) | 63 (24.2) |
| Hypertension (%) | 105 (40.5) |
| No Cardiac Problems (N = 197) | Application of ECMO (N = 31) | AF (N = 32) | p-Value | |
|---|---|---|---|---|
| VBU (cm) | 2.3 ± 0.2 | 2.4 ± 0.2 | 2.3 ± 0.2 | 0.002 |
| Carina–FO (cm) | 6.8 ± 0.8 | 7.3 ± 1.2 | 7.5 ± 0.7 | <0.001 |
| Carina–FO VBU−1 | 3.0 ± 0.3 | 3.1 ± 0.4 | 3.2 ± 0.4 | 0.001 |
| Parameters | Univariate Model | Multivariate Model | ||
|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | p-Value | |
| Male | 0.090 (0.010, 0.160) | 0.027 | 0.080 (0.010, 0.160) | 0.028 |
| BMI | −0.020 (−0.030, −0.010) | <0.001 | −0.020 (−0.030, −0.010) | <0.001 |
| DM | −0.030 (−0.120, 0.060) | 0.463 | ||
| Hypertension | −0.020 (−0.100, 0.060) | 0.647 | ||
| Age | 0.010 (0, 0.010) | <0.001 | 0 (0, 0.010) | 0.013 |
| Application of ECMO or AF | 0.120 (0.030, 0.210) | 0.007 | 0.130 (0.040, 0.210) | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, D.H.; Park, S.E.; Kim, J.W.; Moon, S.H.; Cha, H.J.; Ahn, J.H.; Byun, J.H. Optimal Localization of the Foramen Ovale for Transseptal Puncture Using the Vertebral Body Units. Medicina 2025, 61, 896. https://doi.org/10.3390/medicina61050896
Kang DH, Park SE, Kim JW, Moon SH, Cha HJ, Ahn JH, Byun JH. Optimal Localization of the Foramen Ovale for Transseptal Puncture Using the Vertebral Body Units. Medicina. 2025; 61(5):896. https://doi.org/10.3390/medicina61050896
Chicago/Turabian StyleKang, Dong Hoon, Sung Eun Park, Jong Woo Kim, Seong Ho Moon, Ho Jeong Cha, Jong Hwa Ahn, and Joung Hun Byun. 2025. "Optimal Localization of the Foramen Ovale for Transseptal Puncture Using the Vertebral Body Units" Medicina 61, no. 5: 896. https://doi.org/10.3390/medicina61050896
APA StyleKang, D. H., Park, S. E., Kim, J. W., Moon, S. H., Cha, H. J., Ahn, J. H., & Byun, J. H. (2025). Optimal Localization of the Foramen Ovale for Transseptal Puncture Using the Vertebral Body Units. Medicina, 61(5), 896. https://doi.org/10.3390/medicina61050896