1. Introduction
Distal radius fractures (DRFs) are among the most common fractures in humans, with a lifetime incidence of approximately 9% [
1]. Two age peaks can be identified, each differing in its trauma mechanism. In patients under 40 years of age, distal radius fractures are often caused by high-impact trauma. In contrast, in individuals over 40 years of age, low-energy trauma is the predominant cause of DRFs. Women in this group are significantly more affected, with a 6.2-fold higher risk [
2,
3]. Intra-articular DRFs are classified as 23-B1 to C3 fractures according to the
Arbeitsgemeinschaft für Osteosynthesefragen (AO) classification [
2,
4]. The classification of the fracture, along with possible dislocation and associated injuries, determines the indication for surgical treatment. In recent years, there has been a clear trend toward operative management [
5]. The gold standard for surgical treatment is open reduction and internal fixation (ORIF) with volar plate osteosynthesis, which achieves excellent outcomes [
2,
6,
7]. In complex fractures with multiple or difficult-to-reduce fragments, additional procedures may need to be applied if necessary to achieve optimal postoperative outcomes. Also, ligamentous or chondral concomitant injuries can be addressed in a single-stage treatment [
5,
8,
9,
10]. In intra-articular fractures, especially in cases with radiologically detectable joint step-offs of >2 mm and suspected ligament injuries, ORIF combined with wrist arthroscopy is indicated [
11,
12,
13].
The economic impact of distal radius fractures extends beyond direct medical costs [
14,
15]. These fractures can lead to significant indirect costs, including lost work hours and reduced independence, particularly in the elderly population. Additionally, they can result in long-term disability and a decreased quality of life [
14,
15,
16]. Key cost drivers for surgical treatment of distal radius fractures include both surgical and patient factors, such as postoperative hospital admissions, simultaneous treatment of associated injuries, as well as increased operative time [
17].
The reimbursement for hand surgery services for the treatment of distal radius fractures is difficult to compare due to differences in reimbursement within national healthcare systems. For example, the average cost for surgical treatment of DRFs in the USA in 2018 ranged between USD 6577 and USD 8181 when treated surgically [
18]. In Germany, reimbursement depends on whether patients are treated inpatient or outpatient. Currently, slightly more than half of all DRFs are treated inpatient in Germany [
19]. There is an increasing pressure to shift the treatment of distal radius fractures to an outpatient setting. The current Outpatient Surgery Contract of the National Association of Statutory Health Insurance Physicians of Germany does not include ORIF of distal radius fractures. Therefore, this procedure can generally only be performed under inpatient conditions [
20]. However, based on personal experience, for otherwise healthy patients, cost coverage requests are usually submitted to and reviewed by the Medical Service of the Health Insurance Funds. In the context of this development, the necessary treatment must be evaluated from both medical and economic perspectives to justify additional treatment costs, such as those associated with concomitant wrist arthroscopy.
In Germany, the treatment of DRFs is traditionally carried out by orthopedic surgeons as well as plastic surgeons. Surgeons from both specialties can supplement their expertise with an additional qualification in hand surgery [
21,
22]. In the study setting, treatment of DRFs was provided by both the Department of Hand Surgery, Plastic Surgery, and Aesthetic Surgery, as well as the Department of Orthopaedics and Trauma Surgery. Both departments treated intra-articular DRFs, whereas only the plastic surgery department managed complex fractures involving joint surface involvement and ligamentous injuries with arthroscopic assistance.
This study compares the cost structure and cost-effectiveness of fluoroscopy-assisted ORIF and arthroscopy-assisted ORIF, taking into account DRF severity (AO classification) and treatment indications from the literature, to assist surgeons and healthcare providers in making more informed decisions regarding DRF treatment options.
2. Materials and Methods
This monocentric retrospective study was conducted between October 2021 and March 2022 at Ludwig-Maximilians-University (LMU) Hospital, Munich, Germany. Inclusion criteria were a medical indication for surgical treatment of a DRF using volar plate osteosynthesis and the performance of this procedure, as well as a patient age of over 18 years. General exclusion criteria were a DRF without an indication for surgical treatment, a patient’s refusal of surgical treatment, treatment of the DRF using any method other than volar plate osteosynthesis, and a patient’s age under 18 years. Ethical approval for this study was granted by the ethics committee of the LMU (No. 22-0674, Date: 26 August 2022, with Addendum, Date: 15 August 2023).
2.1. Conditions of the Study Implementation
This study was conducted at a subsidiary site of the university clinic, which is certified as a supraregional hand trauma center. When indicated for surgery, distal radius fractures were treated by the Department of Hand Surgery, Plastic Surgery, and Aesthetic Surgery, as well as the Department of Orthopaedics and Trauma Surgery. According to lost internal clinic agreements, complex intra-articular fractures with signs of accompanying ligamentous injuries are mainly treated by plastic surgeons using arthroscopically assisted methods. Extra-articular or minimally displaced fractures are treated by orthopedic surgeons. For polytraumatized patients also presenting with a DRF, treatment is usually provided by the orthopedic/trauma department. Both the Department of Hand Surgery, Plastic Surgery, and Aesthetic Surgery, as well as the Department of Orthopaedics and Trauma Surgery, treated intra-articular fractures, whereas in our hospital, only the Plastic Surgery Department performed arthroscopically assisted fracture management. Patients included in this study were referred either by outpatient physicians or presented via the in-house emergency departments and trauma bay, respectively.
2.2. Indication and Treatment
The fractures were classified according to the AO classification based on preoperative X-rays and CT scans, as assessed by trained hand surgeons [
23]. The decision to perform simultaneous wrist arthroscopy was based on fracture classification, displacement, and intraoperative reduction results or preoperatively suspected concomitant ligament or cartilage injury [
13,
24,
25]. All osteosynthetic treatments of the DRF were performed via ORIF using volar plate osteosynthesis (Medartis AG, Basel, Switzerland) [
3,
6,
7,
26]. The procedures performed during osteosynthesis and arthroscopy were documented from the surgical reports.
2.3. Study Design
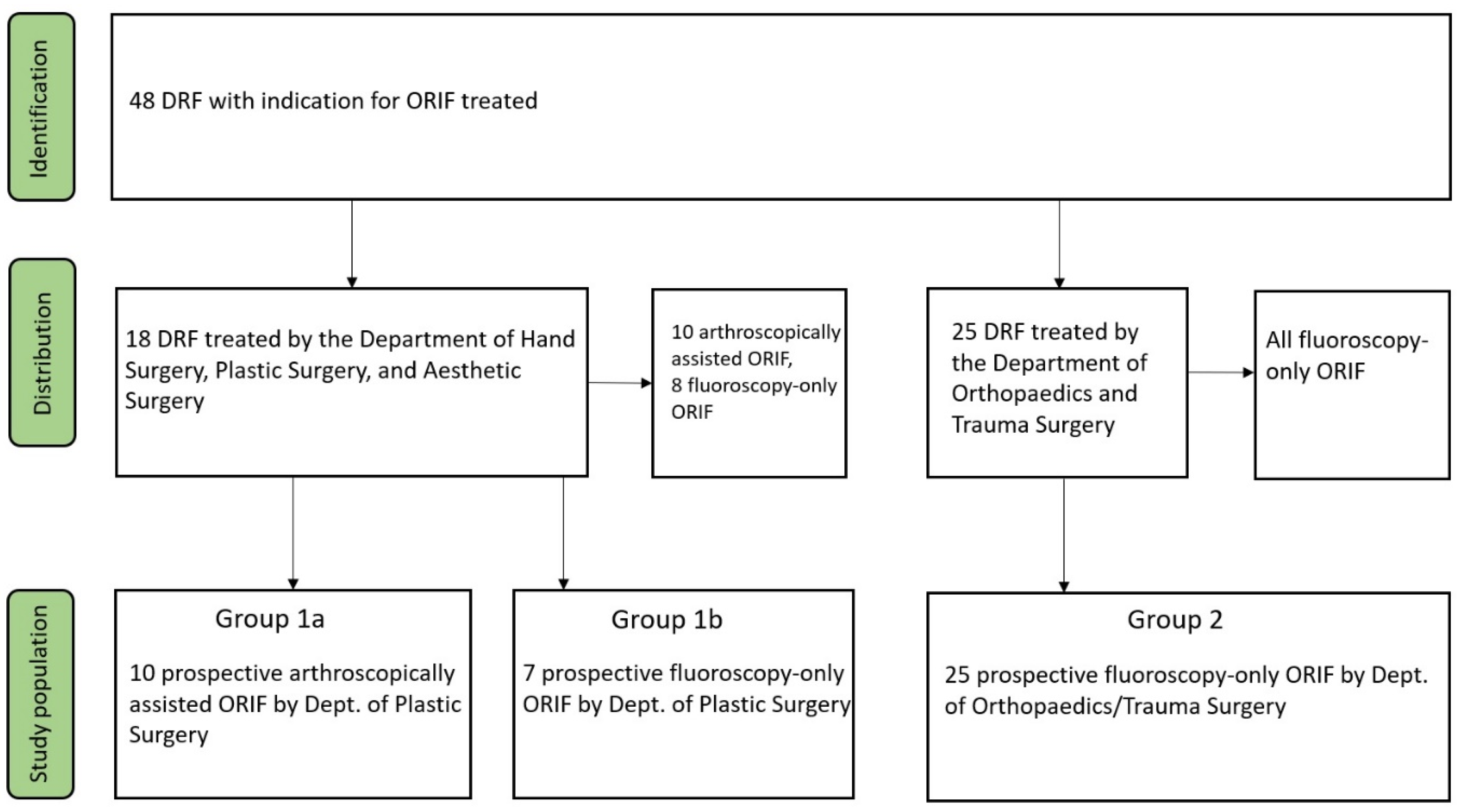
The study population was divided according to the treating department (Group 1 and Group 2, respectively). Additionally, Group 1 was further subdivided into Group 1a and Group 1b based on the type of treatment, with arthroscopic assistance and purely fluoroscopic ORIF, respectively (
Figure 1).
2.4. Analysis
The economic analysis was conducted based on two main aspects: first, the cost breakdown of standard surgical trays, single-use items, and other necessary materials used for the procedures [
18,
27]. Second, the cost of the average surgical minute was calculated, distinguished by the type of treatment and the department performing the procedure. Only the running costs of the surgical interventions were considered in this study; investment costs for equipment and infrastructure were not taken into account. The data were provided and approved by the in-house Department of Controlling.
In Germany, reimbursement for inpatient (surgical) treatment of patients is based on DRGs. These are determined using the diagnosis (according to ICD-10), the treatment performed (e.g., OPS code), and, if applicable, additional factors. The reimbursement for distal radius fractures was exemplarily determined using the Webgrouper tool by the DRG Research Group (
www.drg-research-group.de (accessed on 15 April 2025), DRG Research Group, Senden, Germany) (See
Table 1).
The data are presented as means with standard deviation or as absolute and relative values unless otherwise specified. Normal distribution was assessed using the Shapiro–Wilk test. All calculations were performed using SPSS Statistics 28 (IBM, Armonk, NY, USA). Results were considered statistically significant at a probability level of ≤0.05. Graphs were created using Microsoft Excel MSO 2019, Version 1808 (Microsoft, Redmond, WA, USA).
3. Results
Between October 2021 and March 2022, a total of 43 DRFs were treated. Of these, 17 procedures were performed by the Department of Hand Surgery, Plastic and Aesthetic Surgery (Group 1), of which 10 were arthroscopically assisted (Group 1a) and 7 were performed via fluoroscopy only (Group 1b). Additionally, 25 fracture treatments were performed by the Department of Orthopaedics and Trauma Surgery (Group 2).
The average age in Group 1 was 49.6 years (SD = 19.4), with a 64% majority of female patients. In Group 1a, the average age was 53.9 (SD = 16.3) with 60% female patients and 40% male patients, and in Group 1b, the average age was 43.6 (SD = 23.1) with 71.4% female patients. The average age in Group 2 was 54.2 years (SD = 21.0), with 36% male patients and 64% female patients. There was no significant difference in age and gender distribution within the groups and subgroups (p > 0.05).
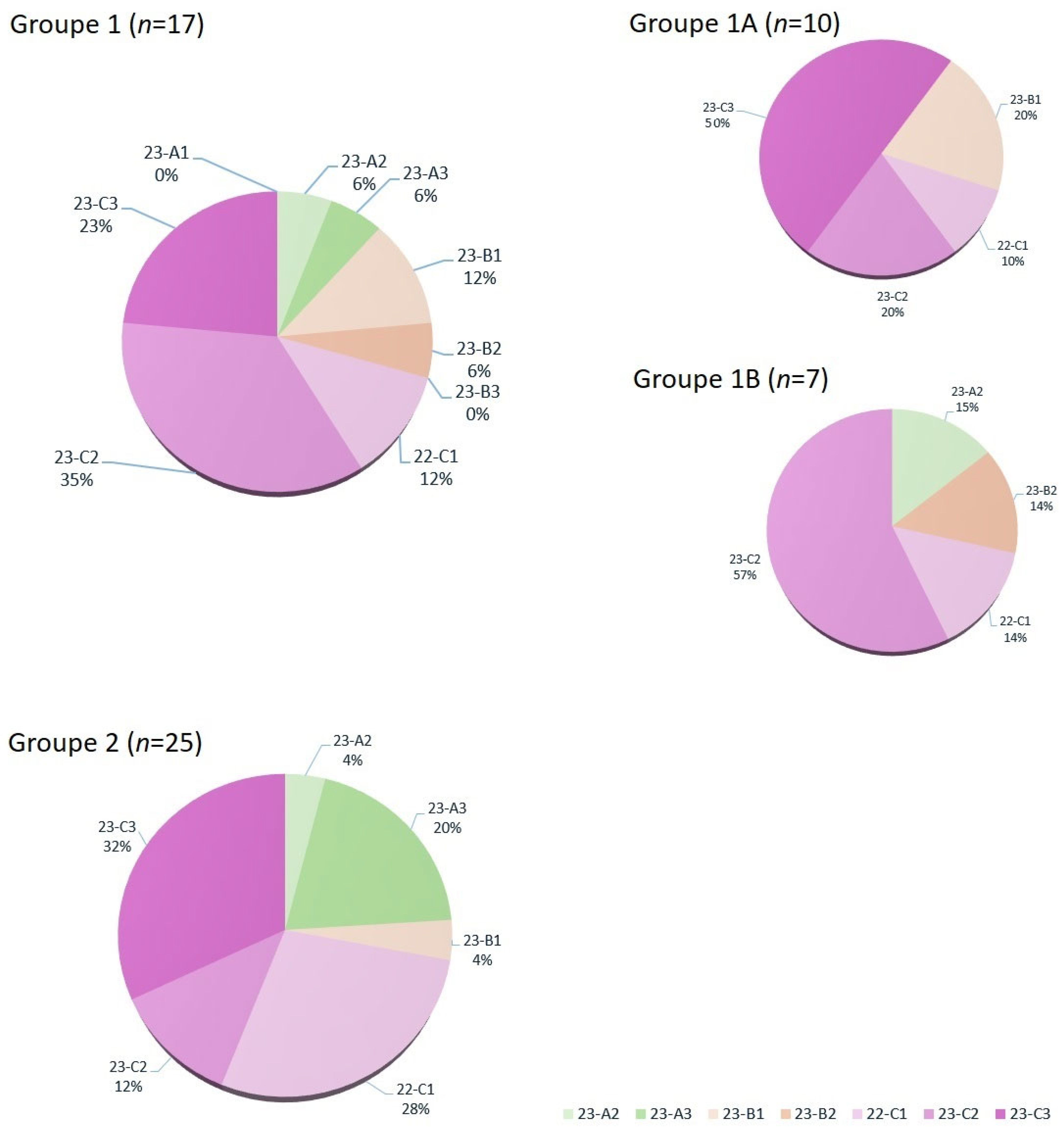
The Department of Plastic Surgery treated a total of seven DRFs via volar plate osteosynthesis using fluoroscopic reduction only (Group 1b). In 10 cases, the intra-articular involvement or fragment displacement was so severe that arthroscopically assisted treatment was necessary (Group 1a). In this Group, diagnostic arthroscopy is used to verify the step-free restoration of the distal radial joint surface. Additionally, debridement using a shaver was performed in seven cases (38.8%), the wrist was flushed, and loose joint bodies were removed. In two cases (11.1%), improved joint surface alignment was achieved through arthroscopic fragment fixation. In one case, a TFCC lesion (Palmer 1B/Atzei 1) was diagnosed, and in another case, the diagnosis of a fresh SL ligament injury led to an open SL ligament repair. Of the 25 DRFs treated in Group 2, 19 were intra-articular (76%) and 6 were extra-articular fractures. All fractures were treated with open reduction and internal fixation using a volar plate. No arthroscopically assisted procedures were performed by orthopedic hand surgeons. The fracture severity according to the AO classification across the different groups is shown in
Figure 2.
4. Procedure Costs
Table 1 and Group 2: In Group 1, the cost for standard surgical draping, such as the treatment of a distal radius fracture, is EUR 216.61, whereas in Group 2, it is only EUR 176.52. The reason is mainly the additional use of a handset for EUR 27.67, an extra small adhesive drape for EUR 0.59, and an adhesive cover drape for EUR 1.19. For the fluids used, there is also a price difference of EUR 1.59 in favor of Group 2. The costs arising from the use of reusable sterile items are higher in Group 1, with the surgical trays being as follows: the “Hand-tray” (EUR 38.50), the “Medartis-Radius-tray” (EUR 32.50), and the Drill-Tray “Colibri” (EUR 38.50). Most of the time, Group 1 requires the standby of wrist arthroscopy. If indicated in the surgical preoperative plan, an additional “Wrist Arthroscopy Set” with a Shaver and a 2.4× optic is prepared, which incurs additional costs of EUR 17.50 and EUR 3.15, respectively, regardless of its actual intraoperative use. Group 1 uses the Orthoscan (Ziehm Imaging GmbH, Nuremberg, Germany) for intraoperative fluoroscopy, whose sterile coverage is EUR 3.22 more expensive than the coverage of the Vista C-Arm (Ziehm Imaging GmbH, Nuremberg, Germany) used by Group 2. Additionally, Group 1 routinely uses more expensive suture material, costing EUR 11.36, compared to Group 2’s suture material costing EUR 9.20. Dressing materials contribute EUR 6.80 to the total cost in Group 1 and EUR 3.26 in Group 2. Both groups use Medartis volar plates and cortical and angular-stable screws of this brand. The total cost for draping materials and other single-use items amounts to EUR 216.61 and EUR 176.52 for the Department of Plastic Surgery and the Department of Orthopaedics and Trauma Surgery, respectively (see
Table 2).
Both departments use osteosynthesis material from Medartis (Basel, Switzerland) by default. For material costs, the prices of the plates (Classic styloid-oriented volar plate and FPL plates) [
26] and the screws used were summed up. In total, the cost of the material used for osteosynthesis amounts to EUR 450.00 (SD: 43.46) for Group 1A and EUR 446.82 (SD: 24.59) for Group 1B, compared to EUR 453.16 (SD: 34.04) in Group 2. The cost difference for the osteosynthesis material used was not significant.
Overall, the material costs in the Department of Plastic Surgery amounted to EUR 665.30, while in the Department of Orthopaedics and Trauma Surgery, they amount to EUR 629.68. With a difference of EUR 35.06, the difference between the two departments was not significant (p = 0.7268). Even when comparing Group 1B, including the cost of arthroscopy equipment, the pure material costs of arthroscopy-supported ORIF performed by plastic surgeons (EUR 663.43, SD: 24.58) are not significantly higher than the costs for fluoroscopically guided ORIF performed by orthopedic surgeons (p = 0.0209).
Costs per surgical minute were determined by adding the overhead costs, operating costs of the OR, and personnel costs of all 14 operating areas at the University Hospital Munich. For the year 2021, this resulted in an average cost of EUR 41.76 per surgical minute (in-house Department of Controlling). Surgical procedures in Group 1 lasted on average 98.5 (SD = 37.3) minutes (incision-to-closure time). In the subgroup analysis of 1a and 1b, the average operation duration was 80.1 (SD = 27.5) minutes for fluoroscopy-only fracture treatment (Groupe 1b) and 111.5 (SD = 39.0) minutes for arthroscopically assisted treatment of the distal radius fracture (Groupe 1a). Among the procedures performed by plastic surgeons, there was a significantly longer duration when arthroscopic assistance for the osteosynthesis was necessary (p = 0.0420). In Group 2, the procedures took an average of 65.0 (SD = 34.5) minutes. Therefore, the duration for fluoroscopy-only ORIF of the distal radius fracture performed by orthopedic surgeons is significantly shorter than the average procedure time in Group 1 overall (p = 0.0048). Comparing the procedure times of subgroups 1a and 1b with Group 2, there is a significantly shorter procedure time of 50.5 min for orthopedic treatment (Group 2) compared to arthroscopically assisted treatment (Group 1a) (p = 0.0015). However, there is no significant difference when comparing the classic fluoroscopy-only treatment between the specialties (Group 2 vs. Group 1b) (p = 0.2994).
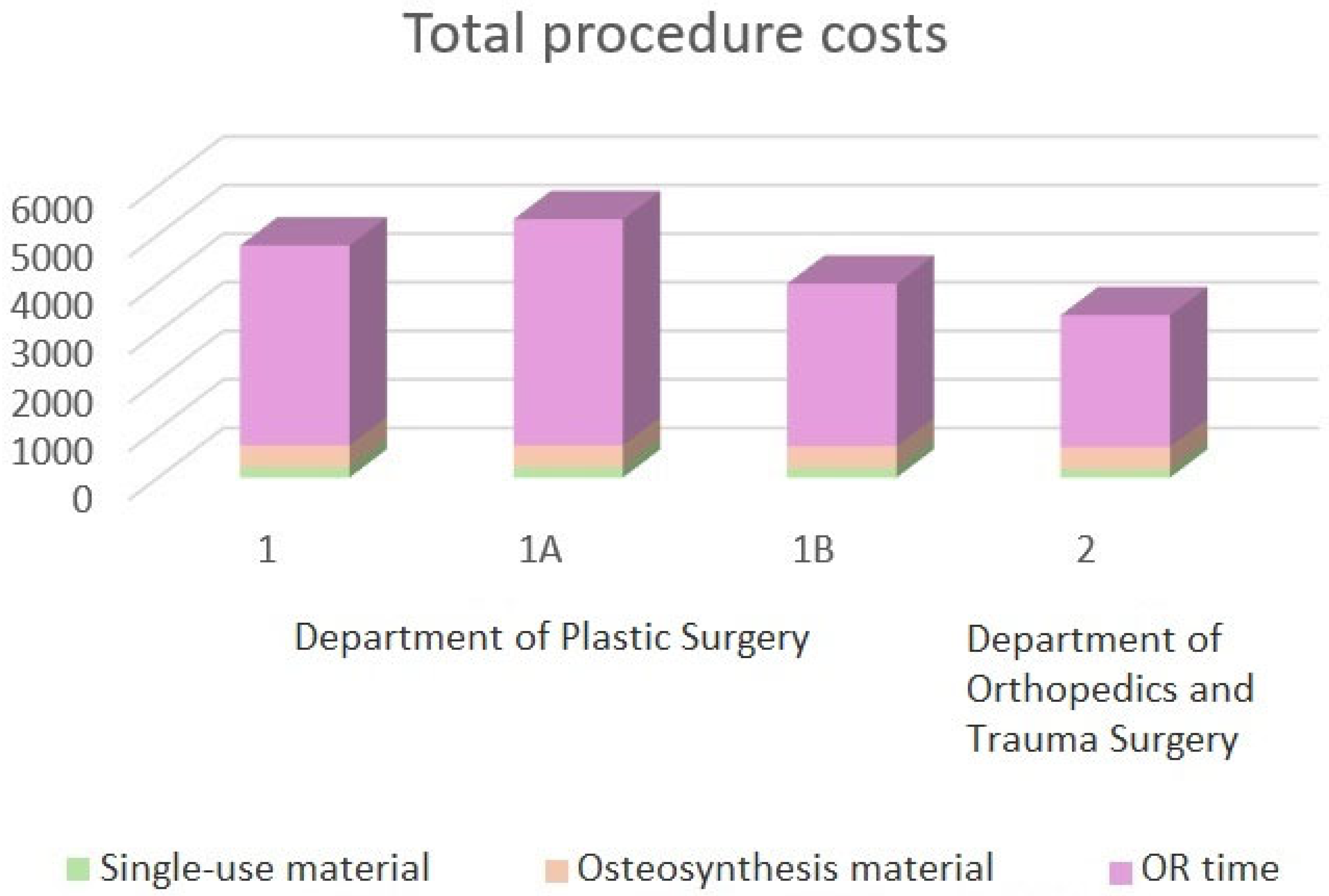
With regards to the costs, the total costs in Group 1, consisting of standard costs, operating minute costs, and material costs, amount to an average of EUR 4906.58. In the subgroup analysis, the average costs for arthroscopically assisted treatment the costs amounted to EUR 5448.24 (Group 1a), and the conventional open reduction and internal fixation (Group 1b) were EUR 4132.80. The costs in Group 2 amount to an average of EUR 3344.08 (
Figure 3).
5. Reimbursement
In Germany, reimbursement for inpatient services is based on DRG (Diagnosis-Related Groups). The base case value in 2022 was EUR 4400.00. The possible diagnoses for distal radius fractures (ICD-10) and surgical treatment options (OP codes) are listed in
Table 1. To determine the minimum reimbursement for the treatment of a DRF according to DRG, the reimbursement was exemplarily calculated using the Webgrouper tool by the DRG Research Group. All ICD-10 codes (S52.50, S52.51, S52.52, and S52.59) used for the cases included in this study were applied and combined with the corresponding OPS codes (5-793.36 and 5-794.26), including the code for arthroscopically assisted fracture treatment (5-810.68). Possible additional procedures, independent of the distal radius fracture, were not taken into account.
The result for each combination was a reimbursement under I21Z. The DRG showed an effective DRG weighting of 0.866, which in 2022 corresponded to EUR 3810.40. Neither the indication-determining severity of the fracture according to the AO classification, nor a possible malalignment of fracture fragments, nor the additional effort of arthroscopy-assisted osteosynthesis, was reflected in the reimbursement.
When the costs of treating a DRF with volar plate osteosynthesis are compared to the reimbursement, it becomes evident that the reimbursement for complex fractures treated by the Department of Plastic Surgery is not cost-covering. In particular, arthroscopically assisted treatment is significantly more expensive than the granted reimbursement. Only the conventionally fluoroscopy-guided osteosyntheses performed by the Department of Orthopaedics and Trauma Surgery are barely cost-covering due to the shorter operative time (
Figure 4). For full reimbursement by the health insurance providers, patients must remain in inpatient treatment for at least two calendar days. However, the accommodation and meal costs already covered by the DRG (§ 17d KHG) have not yet been considered in this calculation.
6. Discussion
This study aimed to compare the cost structure and cost-effectiveness of fluoroscopy-assisted and arthroscopy-assisted open reduction and internal fixation (ORIF) for treating distal radius fractures (DRFs). Previously conducted studies primarily compare postoperative outcomes and often describe the use of arthroscopy as costly, without specifying the actual amount or the reason for these costs [
28,
29,
30]. To our knowledge, a direct comparison of the additional costs of arthroscopically assisted versus purely fluoroscopy-guided ORIF for distal radius fractures (DRFs) has not yet been conducted.
The cost analysis of DRF treatment using volar plate osteosynthesis revealed only slight variations in material costs between the Department of Hand Surgery, Plastic Surgery, and Aesthetic Surgery, and the Department of Orthopaedics and Trauma Surgery, respectively. The differences were primarily due to variations in surgical draping standards and the use of single-use materials. Even though the differences were minimal, the Department of Orthopaedics and Trauma Surgery utilizes slightly more cost-effective materials. Importantly, additional costs associated with arthroscopy were not significant when compared to fluoroscopy-only treatments.
The largest proportion of total costs was attributed to OR usage. Operational costs were calculated per surgical minute and multiplied by the average operation duration for each group. The analysis showed a significantly shorter operation time in the Department of Orthopaedics and Trauma Surgery compared to the Department of Plastic Surgery. In particular, arthroscopically assisted DRF treatments had a significantly longer operation time, resulting in higher costs.
Due to the varying reimbursement models in different national healthcare systems, no universally valid conclusion can be drawn regarding the cost-effectiveness of arthroscopically assisted treatment of intra-articular DRFs [
31,
32]. The cost-effectiveness assessment, therefore, refers specifically to the conditions within the German healthcare system. Since treatment of DRFs via ORIF is not part of the German Mandatory Outpatient Surgeries Catalogue (Katalog ambulant durchführbarer Operationen), thus is usually performed as an inpatient service [
20]. The inpatient treatment of DRFs is reimbursed according to the DRG system. The analysis revealed that reimbursement is both independent of fracture severity (AO classification or displacement) as well as the potential need for arthroscopically assisted fracture treatment. In all cases, reimbursement was classified under DRG I21Z with an effective DRG factor of 0.866, which corresponded to EUR 3810.40 in 2022 (this study’s endpoint). This reimbursement stands in contrast to the costs of an average of EUR 5448.24 for arthroscopically assisted treatment, and EUR 4132.80 or EUR 3344.08 for fluoroscopy-only ORIF. The reimbursement is therefore barely or not cost-covering for the running costs of the actual treatment. Further costs, such as inpatient catering and accommodation, were not considered.
The gold standard for surgical treatment of intra-articular DRFs is ORIF with volar plate osteosynthesis, which achieves excellent outcomes [
2,
3,
6,
7]. In particular, for intra-articular fractures with displaced or difficult-to-reduce fragments, as well as suspected ligamentous or chondral concomitant injuries, accompanying wrist arthroscopy is indicated and can lead to improved postoperative outcomes and allow simultaneous treatment of potential concomitant injuries [
5,
9,
10].
The indication for arthroscopic assistance was based on the preoperative clinical appearance and imaging. For this study, preoperative X-ray and CT images were classified according to the AO classification by experienced hand surgeons. Since the AO classification does not necessarily reflect an increasing severity of the fracture, evaluating the average fracture severity within the analyzed groups proved challenging. It was therefore decided to present the number of fractures graphically and compare them in the discussion.
Both the Department of Hand Surgery, Plastic Surgery, and Aesthetic Surgery, as well as the Department of Orthopaedics and Trauma Surgery, treated intra-articular and non-intra-articular fractures. The relatively high proportion of intra-articular fractures can most likely be attributed to the fact that simpler fractures are often initially reduced and then treated conservatively. Intra-articular fractures more frequently require surgical reduction to achieve a good postoperative outcome. In a subgroup analysis of Group 1 (Department of Plastic Surgery), a significant difference in fracture severity was observed. In Group 1a (arthroscopically assisted), only intra-articular fractures (B1-C3) were found, whereas in Group 1b (treated with fluoroscopy only), both intra-articular fractures and fractures of type A2 and A3 were present. Group 1b closely resembled the Orthopedic/Trauma-Surgical Group 2 in terms of fracture type distribution. A higher frequency of more severe (higher-grade fractures according to the AO classification) was also observed in group 1a. In addition to the more frequent indication for arthroscopy resulting from this, the higher complexity of the fractures likely also contributed to the prolonged operation time and, thus, the significantly higher costs in this group.
Limitations of the study include the limited study population with a small number of cases in each group. Additionally, the monocentric approach may present a one-sided view of the cost structures. Furthermore, there is difficulty in objectively grading the severity and, thus, the potential surgical time required for the individual fractures, making them challenging to compare. Larger trials should be conducted.
Due to the complexity of the fractures and possible concomitant injuries, the treatment of intra-articular radius fractures should, from a medical perspective, be centralized at specialized hand trauma centers. From an economic perspective, this also seems sensible, as the high caseload and increased routine can help reduce operation times, particularly in arthroscopically assisted treatment. Although the results of this study question the cost-effectiveness of arthroscopically assisted treatment for intra-articular DRFs, the authors, from a hand surgery perspective, are convinced of the better outcomes with this technique and continue to use it for the benefit of the patients.
7. Conclusions
Intra-articular DRFs with severely displaced fragments or concomitant injuries benefit from arthroscopically assisted fracture treatment. Arthroscopically assisted and fluoroscopy-only treatments do not differ significantly in material costs; however, the procedures performed with arthroscopic assistance take significantly longer. This results in the largest portion of the costs for performing DRF treatment. Unfortunately, this increased time expenditure is not reflected in the reimbursement through the DRG system. Overall, all variants of fracture treatment are either not or only barely cost-covering. When additional factors for the compulsory inpatient stay are included, like catering and accommodation, the reimbursement is insufficient to perform DRF treatment in a cost-effective manner. As outpatient treatment continues to increase, a significantly adjusted reimbursement is necessary to perform these procedures economically.
Author Contributions
Conceptualization, W.D., A.J., N.W. and R.G.; data curation, A.J., B.F., S.M. and V.A.; formal analysis, A.J., B.F., S.M. and V.A.; investigation, W.D., A.J. and F.G.; methodology, W.D., A.J., F.G. and R.G.; project administration, W.D.; resources, F.G., N.W. and R.G.; software, B.F., S.M. and V.A.; supervision, W.D., F.G. and R.G.; validation, B.F., S.M., N.W. and V.A.; visualization, W.D.; writing—original draft, W.D., A.J. and V.A.; writing—review and editing, W.D., N.W. and V.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Ludwig Maximilian Universität Munich (No. 22-0674, Date: 26 August 2022 with Addendum, Date: 15 June 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The original data presented in this study are openly available in PubMed at DOI.
Conflicts of Interest
The authors have no conflicts of interest.
References
- Vaghela, K.R.; Velazquez-Pimentel, D.; Ahluwalia, A.K.; Choraria, A.; Hunter, A. Distal Radius Fractures: An Evidence-Based Approach to Assessment and Management. Br. J. Hosp. Med. 2020, 81, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Gesellschaft für Unfallchirurgie. S2e Leitlinie Distale Radiusfraktur Des Erwachsenen. AWMF-Nr. 012-015. 2021. Available online: https://register.awmf.org/de/leitlinien/detail/012-015 (accessed on 15 April 2025).
- Azad, A.; Kang, H.P.; Alluri, R.K.; Vakhshori, V.; Kay, H.F.; Ghiassi, A. Epidemiological and Treatment Trends of Distal Radius Fractures across Multiple Age Groups. J. Wrist Surg. 2019, 8, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Schubert, M.; Dávid, A. Diagnostik Und Klassifikation Der Distalen Radiusfraktur—Die Grundlage Der Behandlungsstrategie. Op-J. 2013, 28, 228–233. [Google Scholar] [CrossRef]
- Shihab, Z.; Sivakumar, B.; Graham, D.; del Piñal, F. Outcomes of Arthroscopic-Assisted Distal Radius Fracture Volar Plating: A Meta-Analysis. J. Hand Surg. Am. 2022, 47, 330–340.e1. [Google Scholar] [CrossRef]
- Protopsaltis, T.S.; Ruch, D.S. Volar Approach to Distal Radius Fractures. J. Hand Surg. 2008, 33, 958–965. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, Y.; Fan, J.; Yuan, F.; Tang, Q.; Xian, C.J. Analyses of Fracture Line Distribution in Intra-Articular Distal Radius Fractures. La Radiol. Medica 2019, 124, 613–619. [Google Scholar] [CrossRef]
- Jung, H.-S.; Cho, H.-C.; Lee, J.S. Combined Approach for Intra-Articular Distal Radius Fracture: A Case Series and Literature Review. Clin. Orthop. Surg. 2021, 13, 529–538. [Google Scholar] [CrossRef]
- Abe, Y.; Yoshida, K.; Tominaga, Y. Less Invasive Surgery with Wrist Arthroscopy for Distal Radius Fracture. J. Orthop. Sci. 2013, 18, 398–404. [Google Scholar] [CrossRef]
- Saab, M.; Wunenburger, P.-E.; Guerre, E.; Chantelot, C.; Morel, V.; Ehlinger, M.; Bauer, T. Does Arthroscopic Assistance Improve Reduction in Distal Articular Radius Fracture? A Retrospective Comparative Study Using a Blind Ct Assessment. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 405–411. [Google Scholar] [CrossRef]
- Ardouin, L.; Durand, A.; Gay, A.; Leroy, M. Why Do We Use Arthroscopy for Distal Radius Fractures? Eur. J. Orthop. Surg. Traumatol. 2018, 28, 1505–1514. [Google Scholar] [CrossRef]
- Kamal, R.N.M.; Bronenberg, P.; Shapiro, L.M. The Volar Intra-Articular Extended Window Approach for Intra-Articular Distal Radius Fractures. J. Hand Surg. Am. 2023, 48, 516.e1–516.e5. [Google Scholar] [CrossRef]
- Kastenberger, T.; Kaiser, P.; Schmidle, G.; Schwendinger, P.; Gabl, M.; Arora, R. Arthroscopic Assisted Treatment of Distal Radius Fractures and Concomitant Injuries. Arch. Orthop. Trauma Surg. 2020, 140, 623–638. [Google Scholar] [CrossRef] [PubMed]
- Sabesan, V.J.; Valikodath, T.; Childs, A.; Sharma, V.K. Economic and Social Impact of Upper Extremity Fragility Fractures in Elderly Patients. Aging Clin. Exp. Res. 2015, 27, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Scaf-Klomp, W.; van Sonderen, E.; Sanderman, R.; Ormel, J.; Kempen, G.I.J.M. Recovery of Physical Function after Limb Injuries in Independent Older People Living at Home. Age Ageing 2001, 30, 213–219. [Google Scholar] [CrossRef]
- Nellans, K.W.; Kowalski, E.; Chung, K.C. The Epidemiology of Distal Radius Fractures. Hand Clin. 2012, 28, 113–125. [Google Scholar] [CrossRef]
- Liverneaux, P. Comment: Theca Primary Cost Drivers of Outpatient Distal Radius Fracture Fixation: A Cost-Minimalization Analysis of 15,379 Cases. J. Wrist Surg. 2024, 13, 96. [Google Scholar] [CrossRef] [PubMed]
- Huetteman, H.E.; Zhong, L.; Chung, K.C. Cost of Surgical Treatment for Distal Radius Fractures and the Implications of Episode-Based Bundled Payments. J. Hand Surg. Am. 2018, 43, 720–730. [Google Scholar] [CrossRef]
- Reiland, K.; Haastert, B.; Arend, W.; Klüppelholz, B.; Windolf, J.; Icks, A.; Thelen, S.; Andrich, S. Epidemiology of Distal Radius Fractures in Germany—Incidence Rates and Trends Based on Inpatient and Outpatient Data. Osteoporos. Int. 2024, 35, 317–326. [Google Scholar] [CrossRef]
- KBV. Katalog Ambulant Durchführbarer Operationen, Sonstiger Stationsersetzender Eingriffe Und Stationsersetzender Behandlungen Gemäß § 115b Sgb V Im Krankenhaus; Kassenärztliche Bundesvereinigung (KBV): Berlin, Germany, 2025. [Google Scholar]
- BLAEK. Handchirurgie. Available online: https://www.blaek.de/weiterbildung/qualifikationen-nach-der-weiterbildungsordnung/handchirurgie (accessed on 4 April 2025).
- DGH. Die DGH. Available online: https://dg-h.de/die-dgh/ (accessed on 4 April 2025).
- Kleinlugtenbelt, Y.V.; Groen, S.R.; Ham, S.J.; Kloen, P.; Haverlag, R.; Simons, M.P.; Scholtes, V.A.B.; Bhandari, M.; Goslings, J.C.; Poolman, R.W. Classification Systems for Distal Radius Fractures. Acta Orthop. 2017, 88, 681–687. [Google Scholar] [CrossRef]
- Mehta, J.A.; Bain, G.I.; Heptinstall, R.J. Anatomical Reduction of Intra-Articular Fractures of the Distal Radius. An Arthroscopically-Assisted Approach. J. Bone Jt. Surg. Br. Vol. 2000, 82, 79–86. [Google Scholar] [CrossRef]
- Ruch, D.S.; Vallee, J.; Poehling, G.G.; Smith, B.P.; Kuzma, G.R. Arthroscopic Reduction Versus Fluoroscopic Reduction in the Management of Intra-Articular Distal Radius Fractures. Arthrosc. J. Arthrosc. Relat. Surg. 2004, 20, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Medartis. Product Information—Distal Radius System 2.5. 2019. Available online: https://medartis.com/fileadmin/MDD_Archiv/EN/WRIST-01020001_distal_radius_system_2.5_surgical_technique.pdf (accessed on 15 April 2025).
- Yoon, A.P.; Shauver, M.J.; Hutton, D.W.; Chung, K.C.M.; WRIST Group. Cost-Effectiveness of Treatments after Closed Extraarticular Distal Radius Fractures in Older Adults from the Wrist Clinical Trial. Plast. Reconstr. Surg. 2021, 147, 240e–252e. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, V.L.; Harris, I.A.; Räisänen, M.; Karjalainen, T. Minimal Invasions: Is Wrist Arthroscopy Supported by Evidence? A Systematic Review and Meta-Analysis. Acta Orthop. 2023, 94, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Shkolnikova, J.; Harvey, J. Wrist Arthroscopy in the Management of Distal Radius Fractures. Ann. Jt. 2018, 3, 77. [Google Scholar] [CrossRef]
- von Matthey, F.; Schmid, K.; Zyskowski, M.; Deiler, S.; Biberthaler, P.; Vester, H. The Outcome of Distal Radius Fractures with Concomitant Injuries Is Similar to Those of Isolated Distal Radius Fractures Provided That an Arthroscopically Supported Treatment Is Performed. J. Clin. Med. 2020, 9, 974. [Google Scholar] [CrossRef]
- Quentin, W.; Stephani, V.; Berenson, R.A.; Bilde, L.; Grasic, K.; Sikkut, R.; Touré, M.; Geissler, A. How Denmark, England, Estonia, France, Germany, and the USA Pay for Variable, Specialized and Low Volume Care: A Cross-Country Comparison of in-Patient Payment Systems. Int. J. Health Policy Manag. 2022, 11, 2940–2950. [Google Scholar] [CrossRef]
- Bahnsen, L. Kostenbeteiligungen, Wartezeiten, Leistungsumfang—Ein Europäischer Vergleich Der Gesundheitssysteme. In WIP-Analyse; WIP—Wissenschaftliches Institut der PKV: Köln, Germany, 2022. [Google Scholar]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}