
Remotely Supervised Transcranial Direct Current Stimulation in Post-Stroke Recovery: A Scoping Review

 , , , , and
, , , , and
Abstract
1. Introduction
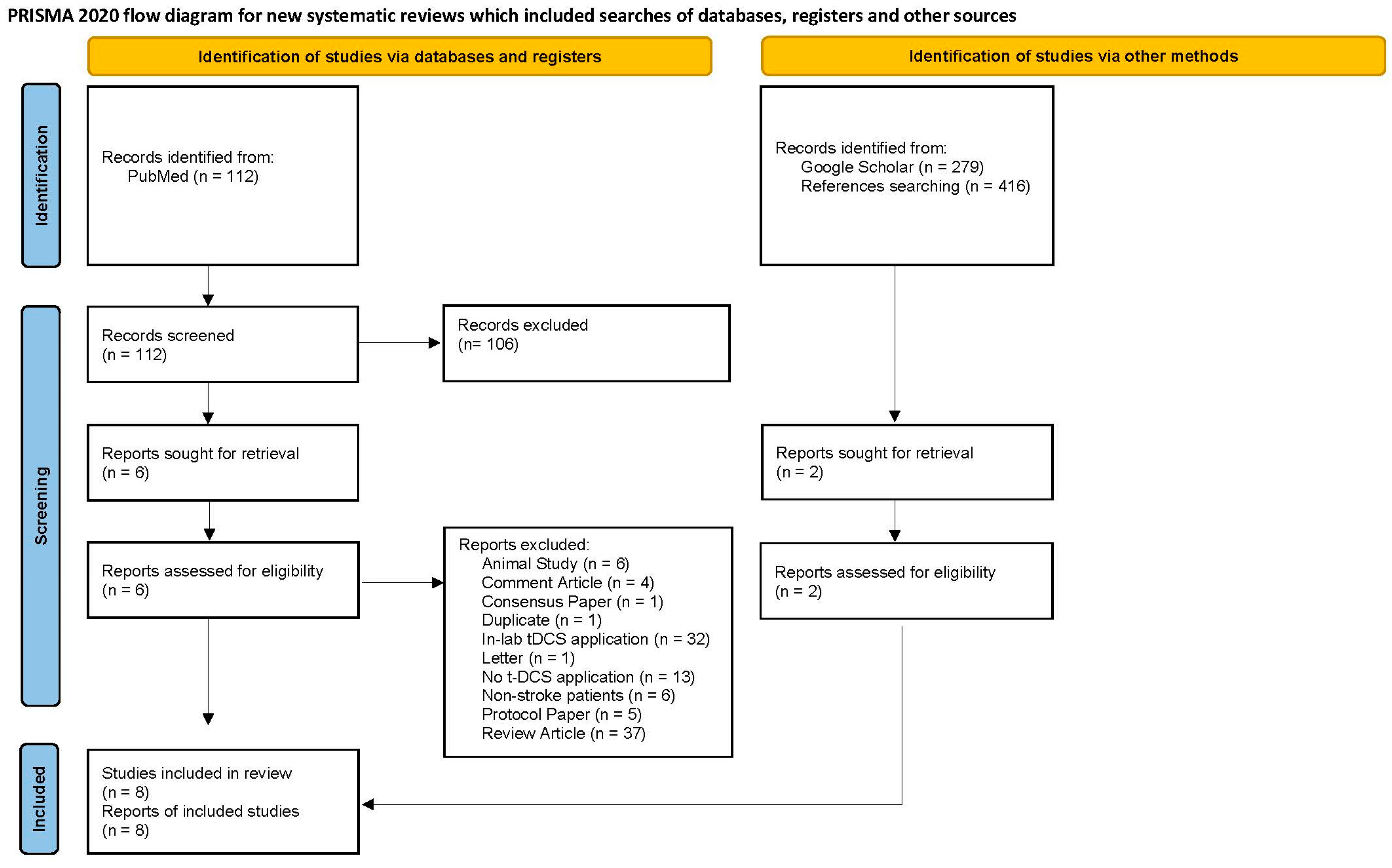
2. Materials and Methods
3. Results
3.1. Motor Recovery
3.2. Language Recovery
3.3. Cognitive Recovery
4. Discussion
5. Limitations
6. Conclusions
7. Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [PubMed]
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [PubMed]
- Dhamoon, M.S.; Moon, Y.P.; Paik, M.C.; Boden-Albala, B.; Rundek, T.; Sacco, R.L.; Elkind, M.S. Quality of life declines after first ischemic stroke. The Northern Manhattan Study. Neurology 2010, 75, 328–334. [Google Scholar]
- Carod-Artal, F.J. Determining quality of life in stroke survivors. Expert. Rev. Pharmacoecon Outcomes Res. 2012, 12, 199–211. [Google Scholar]
- Wang, Y.L.; Pan, Y.S.; Zhao, X.Q.; Wang, D.; Johnston, S.C.; Liu, L.P.; Meng, X.; Wang, A.X.; Wang, C.X.; Wang, Y.J.; et al. Recurrent stroke was associated with poor quality of life in patients with transient ischemic attack or minor stroke: Finding from the CHANCE trial. CNS Neurosci. Ther. 2014, 20, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.W. Update on Stroke Rehabilitation in Motor Impairment. Brain Neurorehabilit. 2022, 15, e12. [Google Scholar]
- Wissel, J.; Manack, A.; Brainin, M. Toward an epidemiology of poststroke spasticity. Neurology 2013, 80, S13–S19. [Google Scholar]
- Ghika-Schmid, F.; Ghika, J.; Regli, F.; Bogousslavsky, J. Hyperkinetic movement disorders during and after acute stroke: The Lausanne Stroke Registry. J. Neurol. Sci. 1997, 146, 109–116. [Google Scholar]
- Alarcon, F.; Zijlmans, J.C.; Duenas, G.; Cevallos, N. Post-stroke movement disorders: Report of 56 patients. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1568–1574. [Google Scholar]
- Handley, A.; Medcalf, P.; Hellier, K.; Dutta, D. Movement disorders after stroke. Age Ageing 2009, 38, 260–266. [Google Scholar]
- Berthier, M.L. Poststroke aphasia: Epidemiology, pathophysiology and treatment. Drugs Aging 2005, 22, 163–182. [Google Scholar] [CrossRef]
- Frederick, A.; Jacobs, M.; Adams-Mitchell, C.J.; Ellis, C. Global Rate of Post-Stroke Aphasia (Frederick et al., 2022). ASHA Journals. Available online: https://asha.figshare.com/articles/online_resource/Global_rate_of_post-stroke_aphasia_Frederick_et_al_2022_/21183478 (accessed on 30 December 2024).
- Blackburn, D.J.; Bafadhel, L.; Randall, M.; Harkness, K.A. Cognitive screening in the acute stroke setting. Age Ageing 2013, 42, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Yang, Y.; Wang, X.; Huang, Y.; Nan, J.; Feng, J.; Yan, F.; Han, L. Prevalence and Risk Factors of Poststroke Cognitive Impairment: A Systematic Review and Meta-Analysis. Public. Health Nurs. 2025, 42, 1047–1059. [Google Scholar] [CrossRef]
- Huang, Y.; Wang, Q.; Zou, P.; He, G.; Zeng, Y.; Yang, J. Prevalence and factors influencing cognitive impairment among the older adult stroke survivors: A cross-sectional study. Front. Public. Health 2023, 11, 1254126. [Google Scholar] [CrossRef] [PubMed]
- El Husseini, N.; Katzan, I.L.; Rost, N.S.; Blake, M.L.; Byun, E.; Pendlebury, S.T.; Aparicio, H.J.; Marquine, M.J.; Gottesman, R.F.; Smith, E.E.; et al. Cognitive Impairment After Ischemic and Hemorrhagic Stroke: A Scientific Statement From the American Heart Association/American Stroke Association. Stroke 2023, 54, e272–e291. [Google Scholar] [CrossRef] [PubMed]
- Damush, T.M.; Plue, L.; Bakas, T.; Schmid, A.; Williams, L.S. Barriers and facilitators to exercise among stroke survivors. Rehabil. Nurs. 2007, 32, 253–260, 262. [Google Scholar] [CrossRef]
- Lynch, E.A.; Cadilhac, D.A.; Luker, J.A.; Hillier, S.L. Inequities in access to inpatient rehabilitation after stroke: An international scoping review. Top. Stroke Rehabil. 2017, 24, 619–626. [Google Scholar] [CrossRef]
- Pantoja-Ruiz, C.; Akinyemi, R.; Lucumi-Cuesta, D.I.; Youkee, D.; Emmett, E.; Soley-Bori, M.; Kalansooriya, W.; Wolfe, C.; Marshall, I.J. Socioeconomic Status and Stroke: A Review of the Latest Evidence on Inequalities and Their Drivers. Stroke 2025, 56, 794–805. [Google Scholar] [CrossRef]
- Ratnakumar, R.; Javed, J.; Senthil, K.; Vasanthan, R. A Cross Sectional Study to Identify Perceived Barriers and Facilitators to Physical Activity and Exercise Participation of People with Post Stroke Depression. Indian. J. Physiother. Occup. Ther. An. Int. J. 2022, 16, 88–93. [Google Scholar] [CrossRef]
- Hodics, T.; Cohen, L.G.; Pezzullo, J.C.; Kowalske, K.; Dromerick, A.W. Barriers to Enrollment in Post-Stroke Brain Stimulation in a Racially and Ethnically Diverse Population. Neurorehabil Neural Repair. 2022, 36, 596–602. [Google Scholar] [CrossRef]
- Kathir, N.; Rowe, V.; Bosch, P.; Toliver, A.; Jondoc, J.; Honeycutt, C. Preliminary Evidence to Support the use of Startle Adjuvant Rehabilitation Therapy (START) via tele-health sessions to promote accessibility and reduce socioeconomic disparities in post-stroke care. Arch. Phys. Med. Rehabil. 2024, 105, e37. [Google Scholar]
- Thair, H.; Holloway, A.L.; Newport, R.; Smith, A.D. Transcranial Direct Current Stimulation (tDCS): A Beginner’s Guide for Design and Implementation. Front. Neurosci. 2017, 11, 641. [Google Scholar]
- Feng, W.W.; Bowden, M.G.; Kautz, S. Review of transcranial direct current stimulation in poststroke recovery. Top. Stroke Rehabil. 2013, 20, 68–77. [Google Scholar]
- Brunoni, A.R.; Nitsche, M.A.; Bolognini, N.; Bikson, M.; Wagner, T.; Merabet, L.; Edwards, D.J.; Valero-Cabre, A.; Rotenberg, A.; Pascual-Leone, A.; et al. Clinical research with transcranial direct current stimulation (tDCS): Challenges and future directions. Brain Stimul. 2012, 5, 175–195. [Google Scholar]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul 2016, 9, 641–661. [Google Scholar] [CrossRef]
- Fregni, F.; Nitsche, M.A.; Loo, C.K.; Brunoni, A.R.; Marangolo, P.; Leite, J.; Carvalho, S.; Bolognini, N.; Caumo, W.; Paik, N.J.; et al. Regulatory Considerations for the Clinical and Research Use of Transcranial Direct Current Stimulation (tDCS): Review and recommendations from an expert panel. Clin. Res. Regul. Aff. 2015, 32, 22–35. [Google Scholar] [PubMed]
- Pilloni, G.; Woods, A.J.; Charvet, L. No risk of skin lesion or burn with transcranial direct current stimulation (tDCS) using standardized protocols. Brain Stimul. 2021, 14, 511–512. [Google Scholar] [PubMed]
- Pilloni, G.; Vogel-Eyny, A.; Lustberg, M.; Best, P.; Malik, M.; Walton-Masters, L.; George, A.; Mirza, I.; Zhovtis, L.; Datta, A.; et al. Tolerability and feasibility of at-home remotely supervised transcranial direct current stimulation (RS-tDCS): Single-center evidence from 6,779 sessions. Brain Stimul. 2022, 15, 707–716. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]
- Mortensen, J.; Figlewski, K.; Andersen, H. Combined transcranial direct current stimulation and home-based occupational therapy for upper limb motor impairment following intracerebral hemorrhage: A double-blind randomized controlled trial. Disabil. Rehabil. 2016, 38, 637–643. [Google Scholar]
- Riggs, A.; Patel, V.; Paneri, B.; Portenoy, R.K.; Bikson, M.; Knotkova, H. At-Home Transcranial Direct Current Stimulation (tDCS) with Telehealth Support for Symptom Control in Chronically-Ill Patients with Multiple Symptoms. Front. Behav. Neurosci. 2018, 12, 93. [Google Scholar]
- Van de Winckel, A.; Carey, J.R.; Bisson, T.A.; Hauschildt, E.C.; Streib, C.D.; Durfee, W.K. Home-based transcranial direct current stimulation plus tracking training therapy in people with stroke: An open-label feasibility study. J. Neuroeng. Rehabil. 2018, 15, 83. [Google Scholar] [PubMed]
- Prathum, T.; Piriyaprasarth, P.; Aneksan, B.; Hiengkaew, V.; Pankhaew, T.; Vachalathiti, R.; Klomjai, W. Effects of home-based dual-hemispheric transcranial direct current stimulation combined with exercise on upper and lower limb motor performance in patients with chronic stroke. Disabil. Rehabil. 2022, 44, 3868–3879. [Google Scholar]
- Ko, M.H.; Yoon, J.Y.; Jo, Y.J.; Son, M.N.; Kim, D.S.; Kim, G.W.; Won, Y.H.; Park, S.H.; Seo, J.H.; Kim, Y.H. Home-Based Transcranial Direct Current Stimulation to Enhance Cognition in Stroke: Randomized Controlled Trial. Stroke 2022, 53, 2992–3001. [Google Scholar]
- Richardson, J.D.; Galletta, E.E.; Charvet, L.; Shaw, M. Feasibility of Remotely Supervised Transcranial Direct Current Stimulation (RS-tDCS) for People with Stroke-Induced and Progressive Aphasia. Aphasiology 2023, 37, 1039–1063. [Google Scholar]
- Kertesz, A. Western Aphasia Battery—Revised; APA PsycNet: Washington, DC, USA, 2007. [Google Scholar]
- Walker, G.M.; Schwartz, M.F. Short-form Philadelphia naming test: Rationale and empirical evaluation. Am. J. Speech Lang. Pathol. 2012, 21, S140–S153. [Google Scholar]
- Duncan, E.S.; Donovan, N.J.; Gentimis, T. Are People With Poststroke Aphasia Receptive to Transcranial Direct Current Stimulation? A Survey. Am. J. Speech Lang. Pathol. 2022, 31, 1383–1393. [Google Scholar] [PubMed]
- Gunduz, M.E.; Bucak, B.; Keser, Z. Advances in Stroke Neurorehabilitation. J. Clin. Med. 2023, 12, 6734. [Google Scholar] [CrossRef]
- Keser, Z.; Ikramuddin, S.; Shekhar, S.; Feng, W. Neuromodulation for Post-Stroke Motor Recovery: A Narrative Review of Invasive and Non-Invasive Tools. Curr. Neurol. Neurosci. Rep. 2023, 23, 893–906. [Google Scholar]
- Sebastian, R.; Kim, J.H.; Brenowitz, R.; Tippett, D.C.; Desmond, J.E.; Celnik, P.A.; Hillis, A.E. Cerebellar neuromodulation improves naming in post-stroke aphasia. Brain Commun. 2020, 2, fcaa179. [Google Scholar]
- Stockbridge, M.D.; Faria, A.V.; Fridriksson, J.; Rorden, C.; Bonilha, L.; Hillis, A.E. Subacute aphasia recovery is associated with resting-state connectivity within and beyond the language network. Ann. Clin. Transl. Neurol. 2023, 10, 1525–1532. [Google Scholar] [PubMed]
- Fridriksson, J.; Rorden, C.; Elm, J.; Sen, S.; George, M.S.; Bonilha, L. Transcranial Direct Current Stimulation vs Sham Stimulation to Treat Aphasia After Stroke: A Randomized Clinical Trial. JAMA Neurol. 2018, 75, 1470–1476. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xu, N.; Wang, R.; Zai, W. Systematic review and network meta-analysis of effects of noninvasive brain stimulation on post-stroke cognitive impairment. Front. Neurosci. 2022, 16, 1082383. [Google Scholar]
- Bahr-Hosseini, M.; Nael, K.; Unal, G.; Iacoboni, M.; Liebeskind, D.S.; Bikson, M.; Saver, J.L.; Group, T.T. High-definition Cathodal Direct Current Stimulation for Treatment of Acute Ischemic Stroke: A Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e2319231. [Google Scholar] [PubMed]
- Gunduz, M.E.; Kocahasan, M.; Keser, Z. Transcranial Direct Current Stimulation to Provide Neuroprotection and Enhance Cerebral Blood Flow in Stroke: A Comprehensive Review. Medicina 2024, 60, 2061. [Google Scholar] [CrossRef]
- Curtis, M.E.; Clingan, S.E.; Guo, H.; Zhu, Y.; Mooney, L.J.; Hser, Y.I. Disparities in digital access among American rural and urban households and implications for telemedicine-based services. J. Rural. Health 2022, 38, 512–518. [Google Scholar]


{kind=link}
{kind=link}
| Authors and Year of the Article | Number of Subjects (Active/Sham) | Time Since Stroke | Post-Stroke Impairment Type | Coupling Treatment | Treatment Period | Place | Intensity and Duration | Polarity | Area of Stimulation (According to the 10–20 System of EEG Electrode Placement) | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| MORTENSEN, 2016 [31] | 15 (8/7) | >6 months and <5 years | Upper-limb motor impairment | 30 min of occupational therapy (simultaneous with RS-tDCS) | Once a day for 5 consecutive days | At home | 1.5 mA, 20 min | Active or Sham | Anode = Ipsilesional M1 (C3 or C4) Cathode = Contralesional supraorbital area (Fp1 or Fp2) |
|
| RIGGS, 2018 [32] | 1 | Unknown | Left upper- and lower-limb motor impairment, chronic pain, feeling sad and nervous | None | Once a day ×10 consecutive days + 10 daily sessions in the following 20 days | At home | 1.5 mA, 20 min | Active | Anode = Left DLPFC (F3) Cathode = Right DLPFC (F4) |
|
| VAN DE WINCKEL, 2018 [33] | 6 | >6 months (Mean = 5.5 years) | Hemiplegia | 20 min of finger-tracking training (simultaneous with RS-tDCS) | Once a day × 5 consecutive days | At a university (3 participants) and at home (3 participants) | 1.5 mA, 20 min | Active | Anode = Ipsilesional upper-limb motor area (C3 or C4) Cathode = Contralesional upper-limb motor area (C3 or C4) |
|
| PRATHUM, 2022 [34] | 24 (12/12) | >6 months and <2 years | Upper- and lower-limb motor impairment | 1 h of home-based exercise (after RS-tDCS) | 3 times a week × 4 weeks | At home | 2 mA, 20 min | Active or Sham | Anode = ipsilesional upper-limb motor area (C3 or C4) Cathode = Contralesional upper-limb motor area (C3 or C4) |
|
| PILLONI, 2022 [29] | 3 | Unknown | Post-stroke aphasia | Cognitive training and physical exercise | Up to 60 sessions | At home or remote | 2.0–2.5 mA, 20 min | Active | Anode = Left DLPFC (F3) Cathode = Right DLPFC (F4) |
|
| KO, 2022 [35] | 26 (12/14) | >6 months | Cognitive impairment | 30 min of computerized cognitive training (simultaneous with RS-tDCS) | 5 times a week × 4 weeks | At home | 2 mA, 30 min | Active or Sham | Anode = Left DLPFC (F3) Cathode = Right supraorbital area (Fp2) |
|
| RICHARDSON, 2023 [36] | Phase 1: 11 Phase 2: 2 | Unknown | Post-stroke aphasia | Phase 1: RS-tDCS aptitude test and virtual stimulation of home tDCS Phase 2: 30 min of computerized language treatment (simultaneous with RS-tDCS) | Phase 1: One time Phase 2: Once a day × 10 consecutive weekdays | At home | Phase 1: 0 mA, 1 h Phase 2: 2 mA, 20 min | Phase 1: Sham Phase 2: Active | Anode = Left DLPFC (F3) Cathode = Right DLPFC (F4 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kocahasan, M.; Stockbridge, M.D.; Stilling, J.; Utianski, R.L.; Sebastian, R.; Keser, Z. Remotely Supervised Transcranial Direct Current Stimulation in Post-Stroke Recovery: A Scoping Review. Medicina 2025, 61, 627. https://doi.org/10.3390/medicina61040627
Kocahasan M, Stockbridge MD, Stilling J, Utianski RL, Sebastian R, Keser Z. Remotely Supervised Transcranial Direct Current Stimulation in Post-Stroke Recovery: A Scoping Review. Medicina. 2025; 61(4):627. https://doi.org/10.3390/medicina61040627
Chicago/Turabian StyleKocahasan, Melike, Melissa D. Stockbridge, Joan Stilling, Rene L. Utianski, Rajani Sebastian, and Zafer Keser. 2025. "Remotely Supervised Transcranial Direct Current Stimulation in Post-Stroke Recovery: A Scoping Review" Medicina 61, no. 4: 627. https://doi.org/10.3390/medicina61040627
APA StyleKocahasan, M., Stockbridge, M. D., Stilling, J., Utianski, R. L., Sebastian, R., & Keser, Z. (2025). Remotely Supervised Transcranial Direct Current Stimulation in Post-Stroke Recovery: A Scoping Review. Medicina, 61(4), 627. https://doi.org/10.3390/medicina61040627