1. Introduction
Cases of SARS-CoV-2 virus-induced atypical pneumonia were reported in Wuhan, China, in 2019. In February 2020, the World Health Organization declared it a global pandemic caused by the coronavirus disease [
1]. COVID-19 is an infectious disease caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). COVID-19 is most commonly transmitted by airborne droplets when an infected person coughs, sneezes or exhales, but it can also be transmitted by contact when a person touches his or her own eyes, nose or mouth after touching infected surfaces. The speed and severity of the spread of infection, rising morbidity and mortality rates and the impact of the demand for services on health systems require adequate infection management strategies and measures. The governments of several countries took aggressive measures to stop the virus from spreading all over the world. This procedure involved quarantine, isolation, mask wearing and social distancing. These measures have effectively slowed the spread of the epidemic, but severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is still increasing worldwide [
2].
In 2020, several COVID-19 vaccines were created and tested, and after regulatory authorization or approval for use and WHO recommendations [
3,
4], it was expected that efficacious vaccines would put an end to the COVID-19 pandemic [
5]. Many countries began mass immunization programs for their citizens [
6]. However, despite vaccines being available for society, individuals need to be encouraged to take the shot that prevents COVID-19 complications [
7]. Even though these vaccinations are said to be safe and only occasionally result in minor side effects, allergy and thrombotic events have been linked to mortality [
8]. Because of these unwelcome side effects and the lack of knowledge regarding the length of efficacy, many people were and are still skeptical of COVID-19 vaccinations [
6]. However, taking into account the pandemic scenario and the benefit–risk ratio, the WHO authorized the use of vaccines for the wider population, especially for the most vulnerable part of society. Several countries have also begun mass immunization programs for their citizens [
8].
In January 2021, Lithuania also started a mass inoculation program for the local population. However, most of the public was skeptical about immunization because of a lack of health literacy, political mistrust and the activity of the “anti-vaxxer” movement. The anti-vaccination movement’s initiators proved to be better persuaders because they used close sources of information—family members and people in the public eye—to communicate with people in a language they understood [
9]. Nevertheless, vaccination coverage has increased significantly since the Ministry of Economy and Innovation announced the introduction of the vaccination certificate on 24 May 2021. Within 4 months, vaccination rates rose by 39%. This pandemic management measure caused a lot of controversy, as some people had to limit their social lives. However, citizens who wanted to lead a socially active life chose between the COVID-19 vaccine and the option of regular testing. This pandemic management strategy has attracted criticism and dissatisfaction in Lithuania, but statistics show that it has been an effective approach to pandemic management [
10]. This led to the intention to investigate the reasons why the Lithuanian population chose the COVID-19 vaccination. This research reveals the real reasons why people in the country chose to vaccinate—whether it was a desire to protect themselves/others or whether it was a consequence of adapting to a political pandemic management tool. It is normal that vaccination, as a medical intervention, is not acceptable among the population. Even in a previous study, it was found that the COVID-19 vaccine acceptance rate in different countries varies. The acceptability percentage for vaccines is comparable in European nations, including Italy (53.7%), France (58.1%) and Poland (56.3%) [
11]. Research has shown that 71.6% of the general population in Lithuania has been vaccinated for COVD-19. However, according to studies, a plethora of factors, including adverse health effects after vaccination, a lack of credible information and proper communication about safety and efficacy, long-term difficulties and a lack of trust in the current healthcare system, affect the attitudes of the general public toward COVID-19 vaccination [
12]. The analysis showed that socio-demographic factors have an impact on how well-accepted the COVID-19 vaccine is. Therefore, this study was designed to identify public attitudes toward COVID-19 vaccination in terms of knowledge, attitude and perception. Accordingly, it is essential to start educating the public more intensively on vaccination issues by involving professionals from different fields, including doctors, scientists, journalists and politicians, in a more intensive discussion with the public on the most relevant science, health and technology topics, with the right messages to the public.
The impact of misinformation on public attitudes toward vaccination, particularly in the context of recent global health crises, is a critical area of concern. The spread of false information through various channels, notably social media, has emerged as a significant barrier to vaccine acceptance in many regions, including Europe and North America. This phenomenon underscores the urgent need for effective communication strategies to counteract misinformation and enhance public trust in health authorities and vaccines.
Misinformation, defined as false or misleading information presented as fact, has been particularly pervasive in the digital age, where social media platforms facilitate rapid information dissemination [
13]. The ease with which misinformation spreads on these platforms can quickly lead to widespread public misconceptions about vaccination. For instance, false narratives around the safety and efficacy of vaccines have been shown to contribute to vaccine hesitancy, a reluctance or refusal to vaccinate despite the availability of vaccination services [
14].
The consequences of misinformation are not merely theoretical but have tangible impacts on public health. In Europe and North America, where vaccine hesitancy fueled by misinformation has been notably prevalent, there has been a marked decline in vaccination rates, leading to the resurgence of diseases previously under control [
15]. This decline underscores the critical need for effective communication strategies that can address and rectify misconceptions caused by misinformation.
Health communication strategies need to be multifaceted to be effective. They should not only provide accurate and transparent information about vaccines but also engage with the public to understand their concerns and build trust. The World Health Organization (WHO) emphasizes the importance of building trust in health authorities and the healthcare system as a cornerstone of increasing vaccine acceptance [
16]. This involves proactive communication, transparency about vaccine development and safety and engagement with community leaders and influencers to disseminate accurate information.
Furthermore, studies have highlighted the role of tailored messaging and the use of behavioral insights in crafting communication strategies. For instance, some researchers suggest that messages that directly address specific misconceptions about vaccines can be more effective than generic pro-vaccine messages [
17]. Additionally, leveraging social norms, such as highlighting the high percentage of people who vaccinate, can positively influence vaccination intentions [
18].
This study represents a novel approach in examining the determinants of COVID-19 vaccine uptake, transcending traditional demographic factors such as education, age, income and urban residency. It uniquely investigates the sources from which individuals receive information regarding vaccine efficacy and composition. This aspect is crucial for health policymakers and AI specialists in devising targeted interventions across diverse media platforms, including social networks, television and radio. By evaluating the credibility of information disseminated on these platforms, this study aims to enhance strategies for promoting vaccination during pandemic crises, thereby contributing significantly to public health efforts [
19].
2. Materials and Methods
2.1. Study Settings and Population
A cross-sectional study was conducted to identify the attitudes of the Lithuanian population toward COVID-19 vaccination. The target group was the general population in Lithuania. A convenient sampling technique was applied, and the study sample consisted of 3166 respondents.
2.2. Data Collection
When a respondent decided to participate in the study, informed consent was immediately obtained. After that, the questionnaire followed. In the informed consent process, participants received information regarding the study’s aims and objectives. Additionally, the participants were made aware that their data would be kept confidential. The questionnaire was addressed to the general public. It was created using the “Google” forms platform, and the sources were shared on the following social media sites: “Linkedin”, “Twitter” and “Facebook”. The Lithuanian population’s attitudes toward the COVID-19 vaccine were evaluated using questions about knowledge, attitudes and perceptions. The questionnaire consisted of five parts: respondents’ socio-demographic information, information on COVID-19 vaccination status, attitudes toward the effectiveness of vaccination for pandemic management, reasons for (not) taking the vaccine and where people obtain information about vaccination and its effectiveness.
2.3. Study Design
In this study, a cross-sectional study methodology was used. This survey received 3166 respondents, and there were no incorrectly filled-out questionnaires because it was online and respondents could not leave empty answers. Therefore, all responses were included in the study.
2.4. Inclusion and Exclusion Criteria
The study comprised members of the public who resided in Lithuania and had internet access. Participants were not approached personally or given anything in exchange for taking part in the study. In this study, there were no exclusions due to incorrectly filled-out surveys.
2.5. Statistical Analysis
Descriptive and analytical statistical methods were used to analyze the survey data. Prevalence estimates and 95% confidence intervals (CI) were calculated. Odds ratios (ORs) were estimated, and logistic regression models were constructed. Pearson’s χ2 test was used to detect differences in distributions across sociodemographic groups, and Fisher’s exact test was used to detect differences in the expected frequencies when the value per cell was less than 5. Mann–Whitney and Kruskal–Wallis tests were used to analyze the distributions of other dependent and independent variables. The differences were considered statistically significant when p ≤ 0.05. Data analysis was carried out using SPSS version 26.0 (IBM Corp, Armonk, NY, USA) and Rstudio version 4.2.2 (PBC Corp, Boston, MA, USA).
4. Discussion
The present study provides comprehensive insight into the attitudes, beliefs and factors influencing the uptake of the COVID-19 vaccine among the Lithuanian population. The findings of this study are consistent with global trends, in which vaccine hesitancy is influenced by a myriad of factors ranging from socio-demographic characteristics to personal beliefs and external influences [
14].
A significant observation from this study is the disparity in vaccination rates based on socio-demographic factors. The higher uptake of the vaccine among individuals with a university degree, those residing in urban areas and those with a higher income is consistent with findings from other studies [
20]. This could be attributed to better access to information, higher health literacy and greater trust in the healthcare system among these groups [
21]. The role of education in influencing vaccine uptake cannot be understated. As observed, individuals with higher education levels were more likely to perceive the vaccine as an effective tool against the pandemic. This underscores the importance of targeted educational interventions to address vaccine hesitancy among those with lower educational attainment [
22].
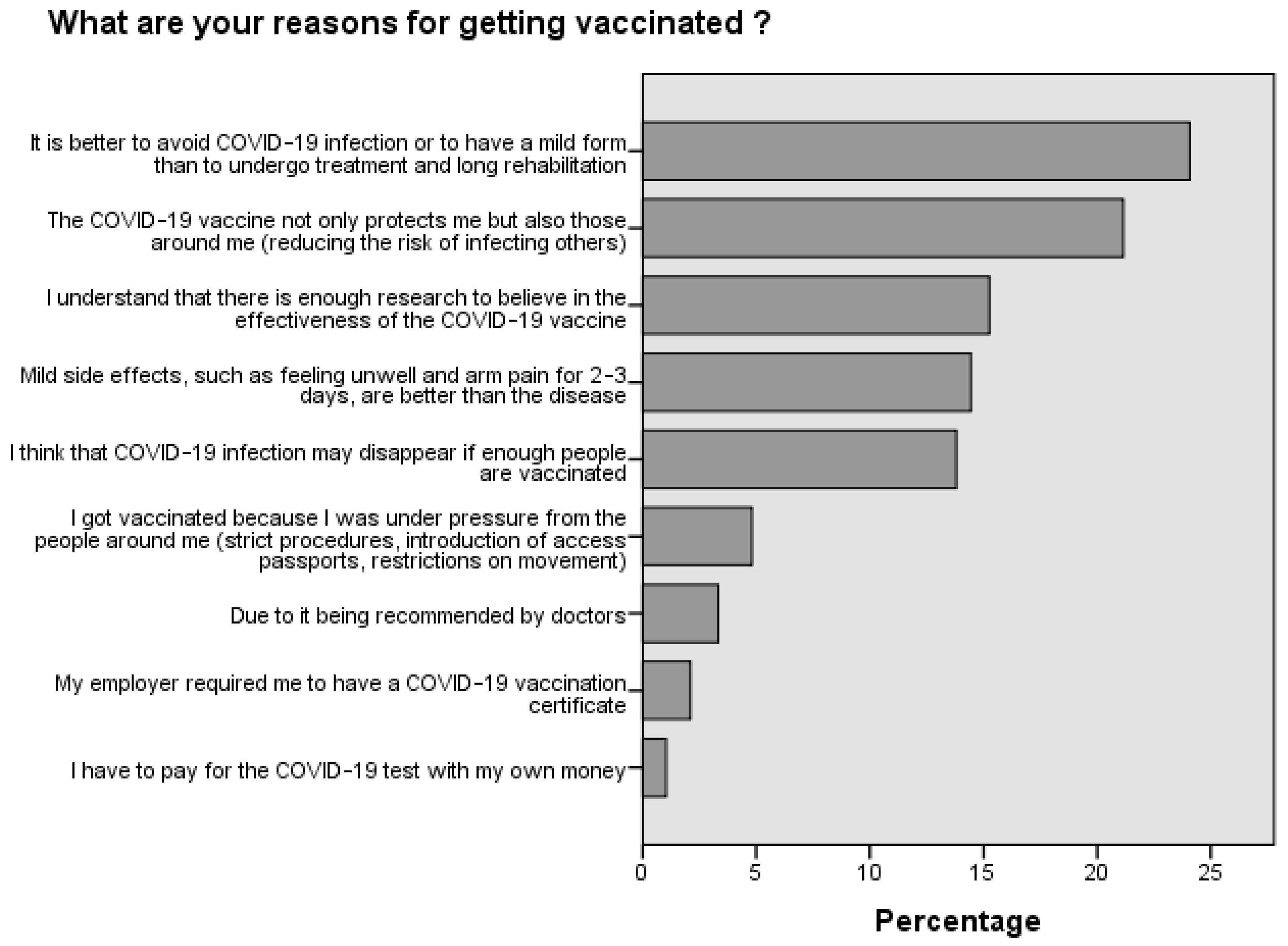
The influence of personal beliefs and attitudes on vaccine uptake was evident in this study. The perception of the vaccine’s effectiveness played a pivotal role in determining whether an individual chose to get vaccinated. This is in line with the Health Belief Model, which posits that individuals are more likely to take preventive health actions if they perceive a threat and believe that the action will mitigate the threat [
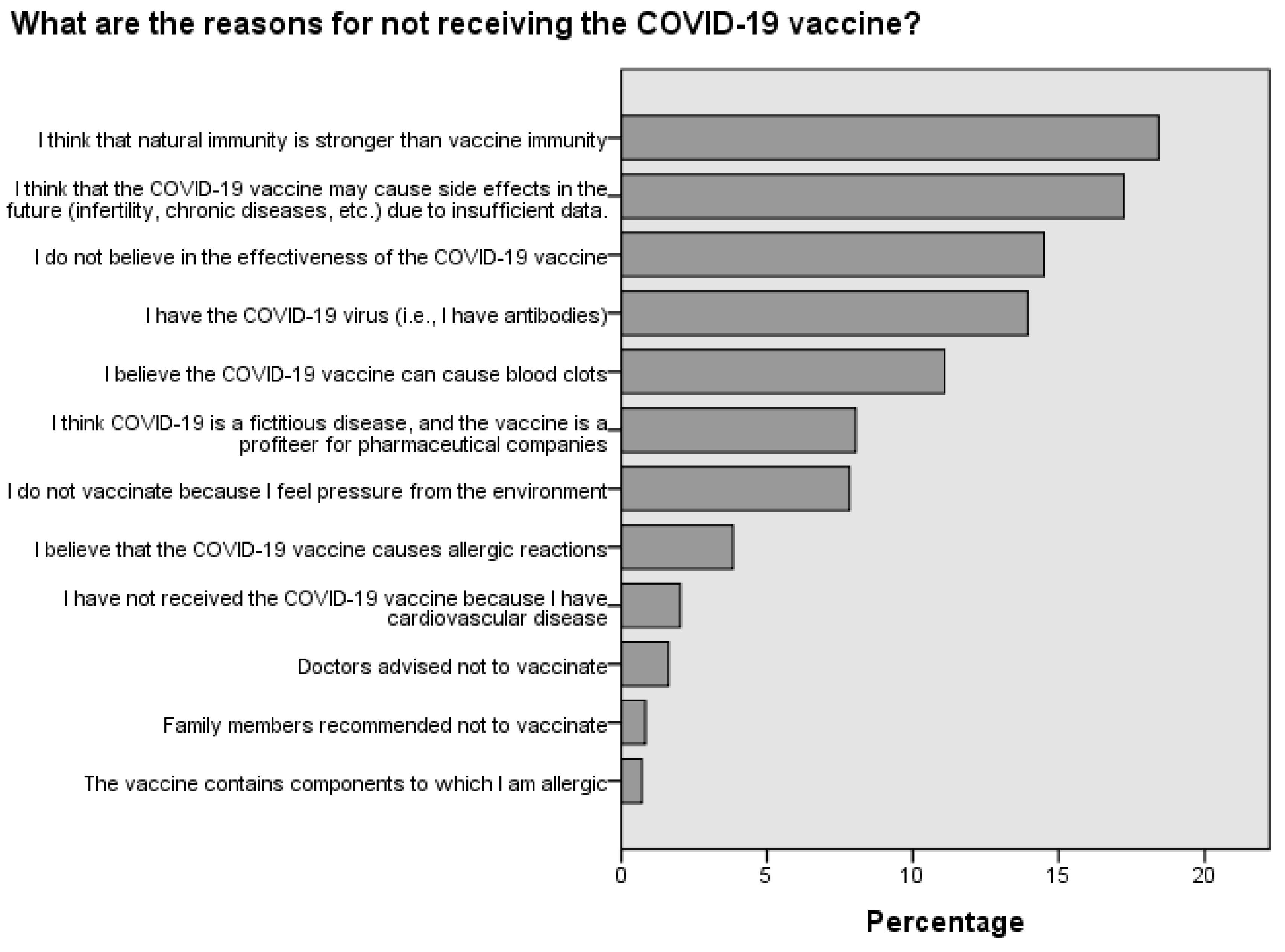
23]. The fact that a significant proportion of the population believed in the efficacy of natural immunity over vaccine-induced immunity highlights the need for public health campaigns to address misconceptions and provide evidence-based information on the benefits of vaccination [
24].
The role of external influences, particularly the “anti-vaxxer” movement, was evident in this study. The ability of the anti-vaccination movement to leverage close sources of information and communicate in a language that resonates with the public underscores the challenges faced by public health authorities in promoting vaccination [
25]. The introduction of the vaccination certificate and its subsequent impact on vaccination rates is a testament to the power of policy interventions in influencing public behavior. However, it also raises ethical questions about the balance between individual rights and public health imperatives [
26].
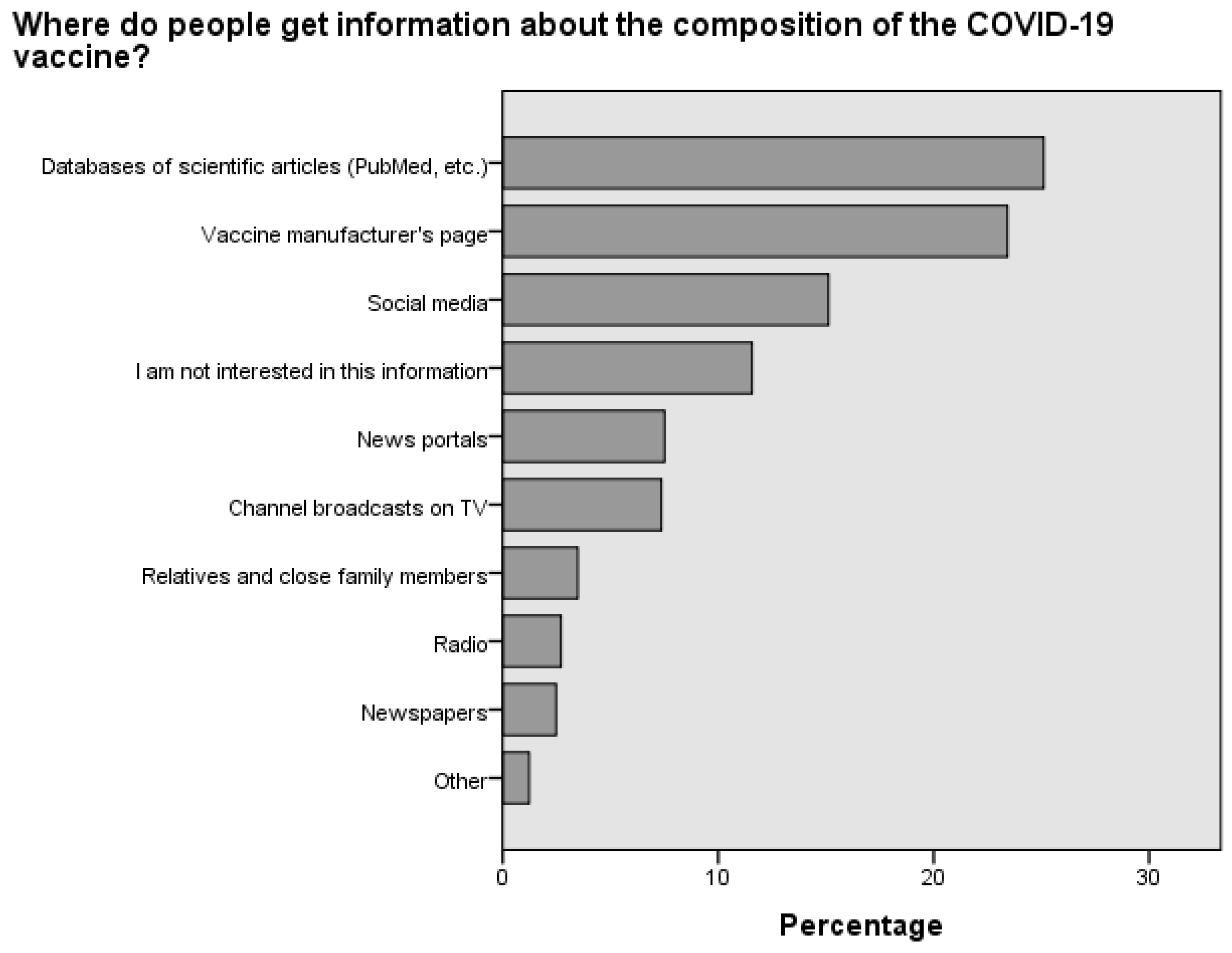
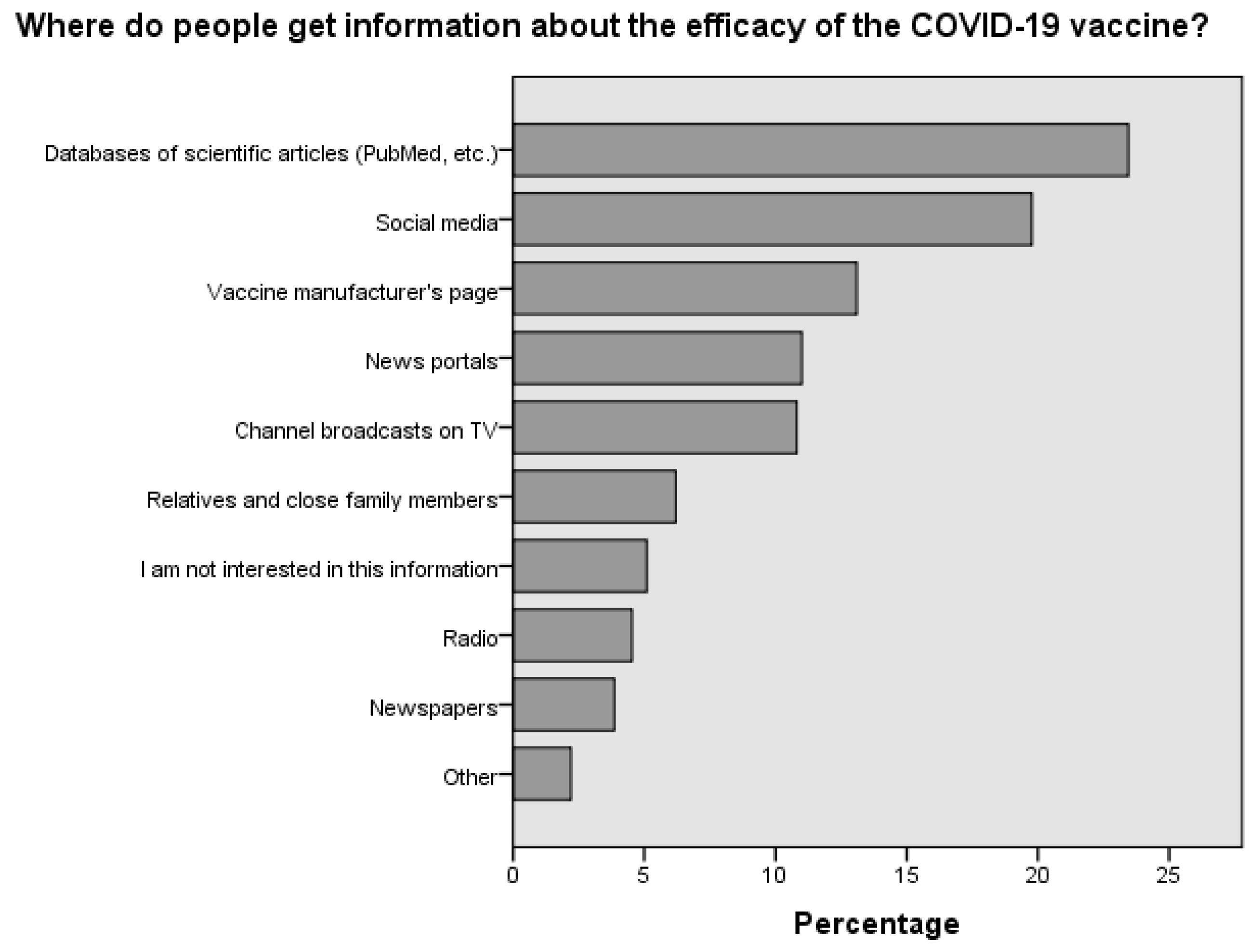
The sources of information that individuals relied upon for vaccine-related information were diverse. The reliance on scientific articles and manufacturer websites is encouraging, as it indicates a preference for evidence-based information. However, the significant proportion of individuals who sought information from social networks is cause for concern given the potential for misinformation on these platforms [
27].
Comparing vaccination attitudes and behaviors in Poland with those of its neighboring country, Lithuania, reveals notable differences. In Lithuania, a majority of the younger population appears more inclined toward vaccination compared to its counterpart in Poland. For both countries, individuals over the age of 50 exhibit high vaccination rates, representing the most active demographic in this regard [
28].
In Poland, there is a discernible gender disparity in the perception of vaccination effectiveness, with men generally perceiving vaccines as more reliable than how women perceive them. Conversely, in Lithuania, the assessment of vaccine effectiveness is relatively uniform across different genders. A particularly interesting observation in Poland is the positive correlation between age and confidence in vaccine effectiveness; this trend is reversed in Lithuania, where older individuals, despite being more likely to get vaccinated, exhibit the highest levels of vaccine non-confidence [
28].
The urban–rural divide also presents contrasting patterns in these countries. In Poland, the perception of vaccine effectiveness is fairly consistent between urban and rural areas. However, in Lithuania, a significant disparity exists, with urban residents demonstrating greater confidence in vaccine effectiveness compared to their rural counterparts [
28].
This study, conducted in Lithuania, is notably more robust, involving a larger sample size of 3166 respondents. Beyond mere frequency calculations, it employs logistic regression models to predict vaccination status. For instance, individuals with university education are 2.12 times (odds ratio [OR] of 2.12,
Table 5) more likely to be vaccinated compared to those without higher education. Similarly, urban residents are 1.22 times (OR of 1.22,
Table 5) more likely to be vaccinated than rural inhabitants. This study also indicates that individuals over 50 years old are 0.72 times (OR 0.72,
Table 5) more likely to be vaccinated than those aged 18–29.
Income levels also correlate with vaccination likelihood; individuals earning between EUR 500 and 1000 per month are 1.3 times (OR 1.3,
Table 5) more likely to be vaccinated than those earning below EUR 500. This trend persists for individuals earning between EUR 1000 and 2000 per month. Furthermore, belief in vaccine effectiveness dramatically increases the likelihood of vaccination, with a 28.45 times (OR of 28.45,
Table 6) higher probability among believers. Similarly, those advocating for mandatory vaccination are 16.68 times (OR of 16.68,
Table 6) more likely to be vaccinated. The predictive model extends these findings, estimating group-specific attitudes toward vaccine effectiveness (
Table 7).
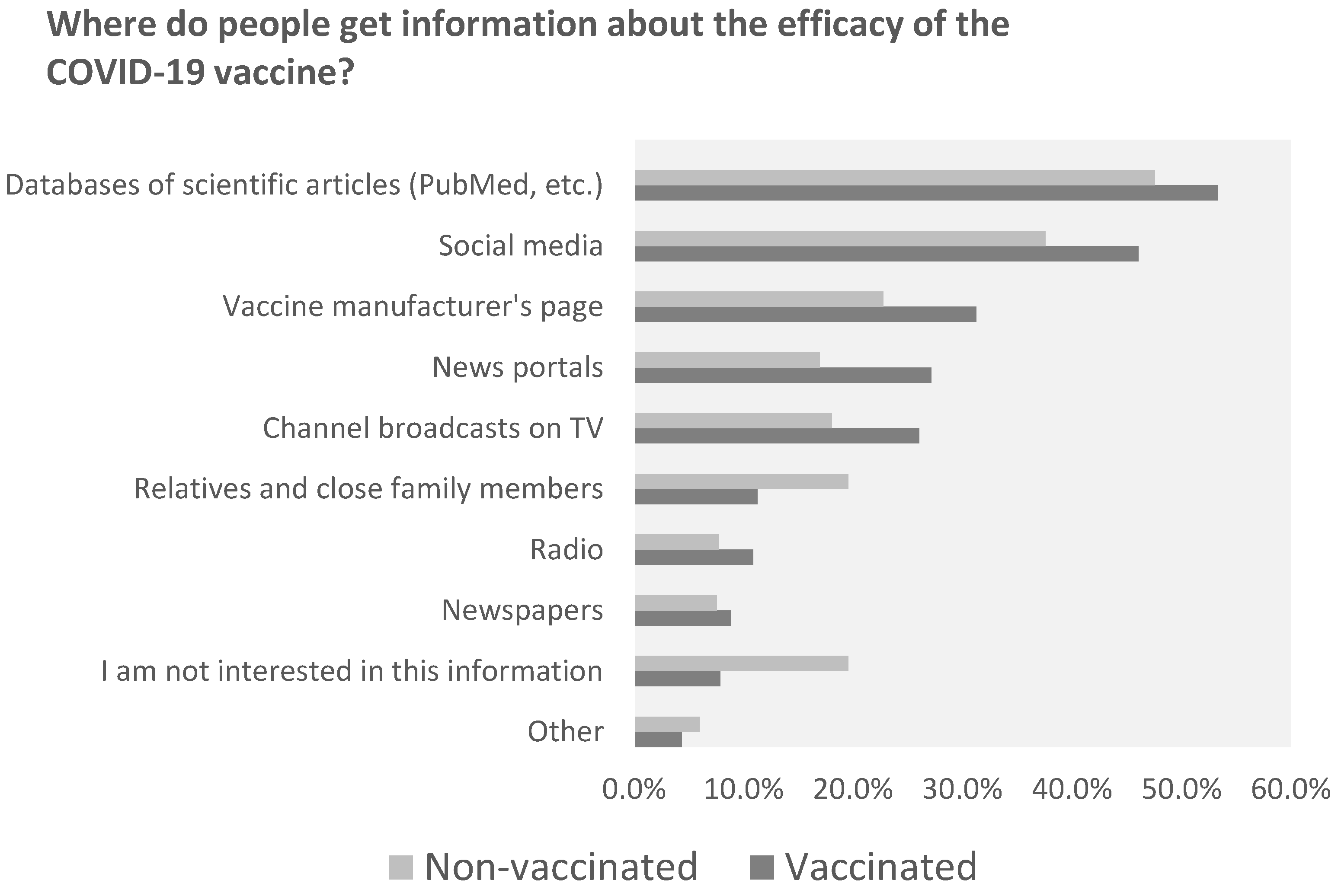
Considering the varying vaccination rates across different countries, age groups and cities, this study distinguishes itself by examining the sources from which individuals gather information about vaccine composition (
Figure 3) and effectiveness (
Figure 4) [
28,
29,
30,
31]. A notable finding is the significant influence of not only social media but also scientific journals that discuss common complications. These complications include cerebrovascular disorders, such as cerebral venous sinus thrombosis, transient ischemic attack, intracerebral hemorrhage, ischemic stroke and demyelinating disorders like transverse myelitis, first manifestations of multiple sclerosis (MS) and neuromyelitis optica [
32,
33]. This study’s results indicate that approximately 47.6% of individuals who chose not to vaccinate (
Figure 5) regularly read scientific journals. This study is of paramount importance, as it highlights the necessity for concerted efforts by medical professionals, public health authorities and policymakers to communicate that, although such complications can occur, they are rare. By doing so, we can alleviate fears and enhance vaccination rates, not only in Lithuania, which is centrally located in Europe, but also globally.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}