
New Robotic Platforms in General Surgery: What’s the Current Clinical Scenario?
 , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
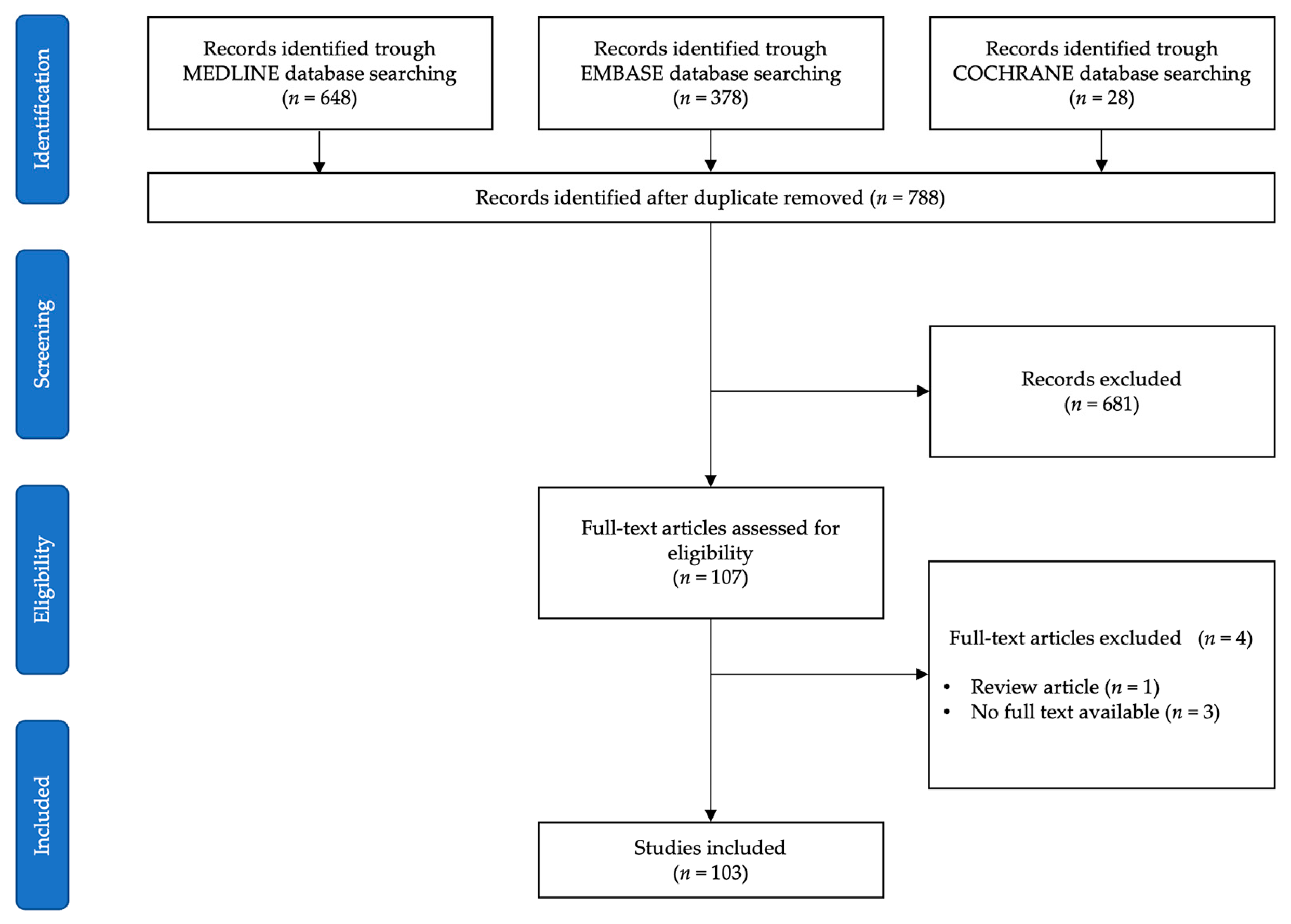
2.1. Search Strategy and Data Sources
- P, population: patients > 18 years undergoing a robotic intervention with a platform different from Intuitive Surgical multiport Da Vinci S®/Si®/Xi®/X®.
- I, intervention: any general surgery intervention with the following exclusions: gynecology, urology, thoracic surgery, othorinolaringoiatry, plastic surgery, pediatric surgery.
- C, comparison: any comparison or no comparison.
- O, outcomes: all reported outcomes, such as intraoperative, postoperative, short-term, long-term, functional, learning-curve, or cost analysis.
- S, study design: due to the expected paucity of studies on the topic, all types of study design were considered, including case reports. Systematic and narrative reviews were excluded. Redundant studies were included and highlighted in the results. Abstract or congress communications were excluded. Only studies in English language were included.
2.2. Data Extraction and Synthesis
2.3. Quality Assessment
3. Results
3.1. Surgery Setting
3.2. Robotic Platforms
3.2.1. Patient Chart Architecture
3.2.2. Surgeon Console Architecture
3.2.3. Trocars, Instruments, and Reusability
3.2.4. Advanced Energy and Staplers
3.3. Training
3.4. Registries
3.5. Costs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sheetz, K.H.; Claflin, J.; Dimick, J.B. Trends in the Adoption of Robotic Surgery for Common Surgical Procedures. JAMA Netw. Open 2020, 3, e1918911. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; Cheng Ng, J.; Andrew Awuah, W.; Huang, H.; Kalmanovich, J.; Agrawal, A.; Abdul-Rahman, T.; Hasan, M.M.; Sikora, V.; Isik, A. Embracing robotic surgery in low- and middle-income countries: Potential benefits, challenges, and scope in the future. Ann. Med. Surg. 2022, 84, 104803. [Google Scholar] [CrossRef] [PubMed]
- Pugin, F.; Bucher, P.; Morel, P. History of robotic surgery: From AESOP® and ZEUS® to da Vinci®. J. Visc. Surg. 2011, 148, e3–e8. [Google Scholar] [CrossRef] [PubMed]
- World Intellectual Property Organization (WIPO). Global Forum for Intellectual Property Policy, Services, Information and Cooperation. Available online: https://patentscope.wipo.int (accessed on 23 May 2023).
- Brodie, A.; Vasdev, N. The future of robotic surgery. Ann. R. Coll. Surg. Engl. 2018, 100, 4–13. [Google Scholar] [CrossRef]
- Hughes, T.; Rai, B.; Madaan, S.; Chedgy, E.; Somani, B. The Availability, Cost, Limitations, Learning Curve and Future of Robotic Systems in Urology and Prostate Cancer Surgery. J. Clin. Med. 2023, 12, 2268. [Google Scholar] [CrossRef]
- Intuitive Surgical. J.P. Morgan Healthcare Conference 2023. Available online: https://isrg.intuitive.com/static-files/6683d2bb-75e2-4fa0-b0cd-463ead7c30a4 (accessed on 23 May 2023).
- Zhang, W.; Li, H.; Cui, L.; Li, H.; Zhang, X.; Fang, S.; Zhang, Q. Research progress and development trend of surgical robot and surgical instrument arm. Int. J. Med. Robot. 2021, 17, e2309. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Cochrane: London, UK, 2022. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Kim, C.H.; Al-Sawat, A.; Lee, C.S. Single-port robot-assisted extended totally extraperitoneal repair for ventral hernia using the da Vinci single-port platform: A video vignette. Asian J. Surg. 2022, 45, 1751–1752. [Google Scholar] [CrossRef]
- Kim, D.; Lee, C.S. Single-port robotic totally extraperitoneal(TEP) inguinal hernia repair using the da Vinci SP platform: A video vignette. Asian J. Surg. 2022, 45, 2062–2063. [Google Scholar] [CrossRef]
- Cruz, C.J.; Yang, H.Y.; Kang, I.; Kang, C.M.; Lee, W.J. Technical feasibility of da Vinci SP single-port robotic cholecystectomy: A case report. Ann. Surg. Treat. Res. 2019, 97, 217–221. [Google Scholar] [CrossRef]
- Alshalawi, W.; Lee, C.S.; Lee, Y.S. Single-port robotic intersphincteric resection for very low rectal cancer with the da Vinci SP platform. Asian J. Surg. 2022, 46, 1056–1057. [Google Scholar] [CrossRef] [PubMed]
- Bak, M.R.; Lee, I.K.; Lee, Y.S.; Lee, C.S. Single-port robotic ventral mesh rectopexy for recurrent rectal prolapse with the da Vinci SP platform: A video vignette. Asian J. Surg. 2022, 46, 1317–1318. [Google Scholar] [CrossRef] [PubMed]
- Minagawa, Y.; Hirano, Y.; Kataoka, A.; Shimamura, S.; Kataoka, M.; Asari, M.; Fujii, T.; Ishikawa, S.; Ishii, T.; Sato, H.; et al. The first single-incision plus one-port transverse colon resection using Senhance Digital Laparoscopy System: A case report. Surg. Case Rep. 2021, 7, 89. [Google Scholar] [CrossRef] [PubMed]
- Samalavicius, N.E.; Klimasauskiene, V.; Janusonis, V.; Samalavicius, A.; Dulskas, A. Robotic total mesorectal excision for mid-rectal cancer using the Senhance® robotic platform—A video vignette. Color. Dis. 2020, 22, 592–593. [Google Scholar] [CrossRef]
- Hirano, Y.; Kondo, H.; Miyawaki, Y.; Sugita, H.; Sakuramoto, S.; Yamaguchi, S. Single-incision plus two-port robotic surgery for sigmoid colon cancer using the Senhance robotic system. Asian J. Endosc. Surg. 2021, 14, 94–96. [Google Scholar] [CrossRef] [PubMed]
- Samalavicius, N.E.; Smolskas, E.; Deduchovas, O.; Janusonis, V.; Dulskas, A. Robotic abdominoperineal resection for pT2N0M0 low rectal cancer using the Senhance TransEnterix robotic platform—A video vignette. Color. Dis. 2019, 21, 847–848. [Google Scholar] [CrossRef]
- Samalavicius, N.E.; Smolskas, E.; Deduchovas, O.; Janusonis, V.; Dulskas, A. Robotic right colectomy using the new Senhance® robotic platform: A three-trocar technique—A video vignette. Color. Dis. 2019, 21, 1092–1093. [Google Scholar] [CrossRef]
- Samalavicius, N.E.; Smolskas, E.; Janusonis, V.; Deduchovas, O.; Dulskas, A. Robotic sigmoid resection for locally advanced cancer using the Senhance Transenterix robotic platform—A video vignette. Color. Dis. 2019, 21, 1216. [Google Scholar] [CrossRef]
- Samalavicius, N.E.; Janusonis, V.; Smolskas, E.; Dulskas, A. Transanal and robotic total mesorectal excision (robotic-assisted TaTME) using the Senhance® robotic system—A video vignette. Color. Dis. 2020, 22, 114–115. [Google Scholar] [CrossRef]
- Samalavicius, N.E.; Klimasauskiene, V.; Janusonis, V.; Samalavicius, R.S.; Janusonis, T.; Dulskas, A. Abdominoperineal resection for low rectal neuroendocrine carcinoma after neoadjuvant chemotherapy using the Senhance robotic system with articulating Radia instrument—A Video Vignette. Color. Dis. 2022, 24, 798–799. [Google Scholar] [CrossRef]
- Samalavicius, N.E.; Klimasauskiene, V.; Nausediene, V.; Janusonyte-Mongirdiene, H.; Liekis, A.; Dulskas, A. Sigmoid colon resection for sigmoid cancer using a Senhance robotic system and indocyanine green fluorescent angiography-a video correspondence. Color. Dis. 2023, 25, 1062–1063. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, A.; Hirano, Y.; Kondo, H.; Shimamura, S.; Kataoka, M.; Asari, M.; Fujii, T.; Ishikawa, S.; Ishii, T.; Yamaguchi, S. Right hemicolectomy with D3 lymph node dissection for right-sided transverse colon cancer using the Senhance robotic system: A case report. Surg. Case Rep. 2020, 6, 263. [Google Scholar] [CrossRef] [PubMed]
- Kondo, H.; Yamaguchi, S.; Hirano, Y.; Ishii, T.; Obara, N.; Wang, L.; Asari, M.; Kato, T.; Takayama, T.; Sugita, H.; et al. A first case of ileocecal resection using a Senhance Surgical System in Japan. Surg. Case Rep. 2020, 6, 95. [Google Scholar] [CrossRef] [PubMed]
- Campagna, G.; Panico, G.; Vacca, L.; Caramazza, D.; Mastrovito, S.; Lombisani, A.; Ercoli, A.; Scambia, G. Robotic sacrocolpopexy plus ventral rectopexy as combined treatment for multicompartment pelvic organ prolapse using the new Hugo RAS system. Tech. Coloproctol. 2023, 27, 499–500. [Google Scholar] [CrossRef] [PubMed]
- Piozzi, G.N.; Lee, D.Y.; Kim, J.S.; Kim, S.H. Da Vinci Single-Port (SP) robotic transverse colectomy for mid-transverse colon cancer. Tech. Coloproctol. 2022, 26, 681–682. [Google Scholar] [CrossRef] [PubMed]
- Choo, J.M.; Kim, J.S.; Cheong, J.Y.; Rusli, S.M.; Park, H.; Kim, S.H. Application of a Single-Port Robotic System for Right Colectomy: A Novel Suprapubic Approach. Dis. Colon. Rectum 2022, 65, e1029. [Google Scholar] [CrossRef]
- Cheong, J.Y.; Choo, J.M.; Kim, J.S.; Rusli, S.M.; Kim, J.; Kim, S.H. Da Vinci SP System Optimized for Intersphincteric Resection of Very Low Rectal Cancer. Dis. Colon. Rectum 2022, 65, e174. [Google Scholar] [CrossRef]
- Marks, J.H.; Salem, J.F.; Anderson, B.K.; Josse, J.M.; Schoonyoung, H.P. Single-port robotic left colectomy: First clinical experience using the SP robot (rSILS). Tech. Coloproctol. 2020, 24, 57–63. [Google Scholar] [CrossRef]
- Arezzo, A.; Forcignanò, E.; Morino, M. Robotic endoscopic submucosal dissection and full-thickness excision for laterally spreading tumors of the rectum. Minim. Invasive Ther. Allied Technol. 2022, 31, 377–379. [Google Scholar] [CrossRef]
- Marks, J.H.; Kunkel, E.; Salem, J.; Martin, C.; Schoonyoung, H.P.; Agarwal, S. rSILS: Initial clinical experience with single-port robotic (SPr) right colectomy. Tech. Coloproctol. 2020, 24, 817–822. [Google Scholar] [CrossRef]
- Marks, J.H.; Kunkel, E.; Salem, J.F.; Martin, C.; Anderson, B.; Agarwal, S. First clinical experience with single-port robotic transanal minimally invasive surgery (SP rTAMIS) for benign rectal neoplasms. Tech. Coloproctol. 2021, 25, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Marks, J.H.; Agarwal, S.; Kunkel, E.; Schoonyoung, H.; Salem, J.F. Video Demonstration of an Initial Single-Port Robotic Transanal Total Mesorectal Excision. Dis. Colon. Rectum 2021, 64, e472–e473. [Google Scholar] [CrossRef] [PubMed]
- Marks, J.H.; Salem, J.F.; Adams, P.; Sun, T.; Kunkel, E.; Schoonyoung, H.; Agarwal, S. SP rTaTME: Initial clinical experience with single-port robotic transanal total mesorectal excision (SP rTaTME). Tech. Coloproctol. 2021, 25, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.J.; Park, P.J.; Choi, S.B.; Kim, W.B. Case report of pure single-port robotic left lateral sectionectomy using the da Vinci SP system. Medicine 2021, 100, e28248. [Google Scholar] [CrossRef]
- Kang, I.; Hwang, H.K.; Lee, W.J.; Kang, C.M. First experience of pancreaticoduodenectomy using Revo-i in a patient with insulinoma. Ann. Hepatobiliary Pancreat. Surg. 2020, 24, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Ku, G.; Kang, I.; Lee, W.J.; Kang, C.M. Revo-i assisted robotic central pancreatectomy. Ann. Hepatobiliary Pancreat. Surg. 2020, 24, 547–550. [Google Scholar] [CrossRef]
- Park, H.S.; Lee, J.; Lee, H.; Lee, K.; Song, S.Y.; Toesca, A. Development of Robotic Mastectomy Using a Single-Port Surgical Robot System. J. Breast Cancer 2020, 23, 107–112. [Google Scholar] [CrossRef]
- Joo, O.Y.; Song, S.Y.; Park, H.S.; Roh, T.S. Single-port robot-assisted prosthetic breast reconstruction with the da Vinci SP Surgical System: First clinical report. Arch. Plast. Surg. 2021, 48, 194–198. [Google Scholar] [CrossRef]
- Dreifuss, N.H.; Schlottmann, F.; Cubisino, A.; Bianco, F.M. Novel surgical approach for gastric gastrointestinal stromal tumor (GIST): Robotic single port partial gastrectomy. Surg. Oncol. 2022, 40, 101704. [Google Scholar] [CrossRef]
- Sugita, H.; Sakuramoto, S.; Aoyama, J.; Ito, S.; Oya, S.; Watanabe, K.; Fujiwara, N.; Kondo, H.; Miyawaki, Y.; Hirano, Y.; et al. First experience using the Senhance surgical system in laparoscopic local gastrectomy for gastrointestinal stromal tumor. Asian J. Endosc. Surg. 2021, 14, 790–793. [Google Scholar] [CrossRef]
- Cui, H.; Cui, J.X.; Zhang, K.C.; Liang, W.Q.; Li, S.Y.; Huang, J.; Chen, L.; Wei, B. Can a single-port robot be safely used for robotic total gastrectomy for advanced gastric cancer? First experience using the da Vinci SP platform. Gastroenterol. Rep. 2022, 10, goac023. [Google Scholar] [CrossRef] [PubMed]
- Cubisino, A.; Dreifuss, N.H.; Schlottmann, F.; Baz, C.; Mangano, A.; Masrur, M.A.; Bianco, F.M. Robotic single port anti-reflux surgery: Initial worldwide experience of two cases with a novel surgical approach to treat gastroesophageal reflux disease. Int. J. Med. Robot. 2022, 18, e2437. [Google Scholar] [CrossRef] [PubMed]
- Halabi, M.; Abid, G.; Zenilman, M.E.; Moussa, H. Treatment of an unusual case of Meckel’s diverticulum with a new robotic platform. Int. J. Surg. Case Rep. 2022, 99, 107613. [Google Scholar] [CrossRef]
- Dixon, F.; Qureshi, A.; Vitish-Sharma, P.; Khanna, A.; Keeler, B.D. Implementation of robotic hernia surgery using the Versius® system. J. Robot. Surg. 2022, 17, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Samalavicius, N.E.; Dulskas, A.; Sirvys, A.; Klimasauskiene, V.; Janusonis, V.; Janusonis, T.; Eismontas, V.; Deduchovas, O.; Stephan, D.; Darwich, I.; et al. Inguinal hernia TAPP repair using Senhance® robotic platform: First multicenter report from the TRUST registry. Hernia 2022, 26, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, R.; Willeke, F.; Barr, J.; Scheidt, M.; Saelzer, H.; Darwich, I.; Zani, S.; Stephan, D. Robotic Inguinal Hernia Repair (TAPP) First Experience with the New Senhance Robotic System. Surg. Technol. Int. 2019, 34, 243–249. [Google Scholar]
- Aggarwal, R.; Winter Beatty, J.; Kinross, J.; von Roon, A.; Darzi, A.; Purkayastha, S. Initial Experience With a New Robotic Surgical System for Cholecystectomy. Surg. Innov. 2020, 27, 136–142. [Google Scholar] [CrossRef]
- Kelkar, D.S.; Kurlekar, U.; Stevens, L.; Wagholikar, G.D.; Slack, M. An Early Prospective Clinical Study to Evaluate the Safety and Performance of the Versius Surgical System in Robot-Assisted Cholecystectomy. Ann. Surg. 2022, 277, 9–17. [Google Scholar] [CrossRef]
- Khanna, S.; Barua, A. Robotic assisted cholecystectomy—A retrospective cohort study of experience of 106 first robotic cholecystectomies in versius robotic platform. Int. J. Surg. Open 2022, 47, 100554. [Google Scholar] [CrossRef]
- Lim, J.H.; Lee, W.J.; Choi, S.H.; Kang, C.M. Cholecystectomy using the Revo-i robotic surgical system from Korea: The first clinical study. Updates Surg. 2021, 73, 1029–1035. [Google Scholar] [CrossRef]
- Melling, N.; Barr, J.; Schmitz, R.; Polonski, A.; Miro, J.; Ghadban, T.; Wodack, K.; Izbicki, J.; Zani, S.; Perez, D. Robotic cholecystectomy: First experience with the new Senhance robotic system. J. Robot. Surg. 2019, 13, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, T.; Tomohisa, F.; Nishimura, M.; Arifuku, H.; Ono, T.; Noda, A.; Otsubo, T. Initial 30 cholecystectomy procedures performed with the Senhance digital laparoscopy system. Asian J. Endosc. Surg. 2022, 16, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Collins, D.; Paterson, H.M.; Skipworth, R.J.E.; Speake, D. Implementation of the Versius robotic surgical system for colorectal cancer surgery: First clinical experience. Color. Dis. 2021, 23, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Dixon, F.; O’Hara, R.; Ghuman, N.; Strachan, J.; Khanna, A.; Keeler, B.D. Major colorectal resection is feasible using a new robotic surgical platform: The first report of a case series. Tech. Coloproctol. 2021, 25, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Fok, K.Y.; Arabaci, F.; Barto, W. Flexible robotic transanal resection of rectal polyps—A case series. Int. J. Med. Robot. 2022, 18, e2413. [Google Scholar] [CrossRef]
- Lin, C.C.; Huang, S.C.; Lin, H.H.; Chang, S.C.; Chen, W.S.; Jiang, J.K. An early experience with the Senhance surgical robotic system in colorectal surgery: A single-institute study. Int. J. Med. Robot. Comput. Assist. Surg. 2021, 17, e2206. [Google Scholar] [CrossRef]
- Morino, M.; Forcignanò, E.; Arezzo, A. Initial clinical experience with a novel flexible endoscopic robot for transanal surgery. Tech. Coloproctol. 2022, 26, 301–308. [Google Scholar] [CrossRef]
- Noh, G.T.; Oh, B.Y.; Han, M.; Chung, S.S.; Lee, R.A.; Kim, K.H. Initial clinical experience of single-incision robotic colorectal surgery with da Vinci SP platform. Int. J. Med. Robot. 2020, 16, e2091. [Google Scholar] [CrossRef]
- Salem, J.F.; Agarwal, S.; Schoonyoung, H.; Martin, C.; Marks, J.H. Initial clinical experience with Single-Port robotic (SP r) left colectomy using the SP surgical system: Description of the technique. Surg. Endosc. 2021, 35, 4022–4027. [Google Scholar] [CrossRef]
- Sasaki, M.; Hirano, Y.; Yonezawa, H.; Shimamura, S.; Kataoka, A.; Fujii, T.; Okazaki, N.; Ishikawa, S.; Ishii, T.; Deguchi, K.; et al. Short-term results of robot-assisted colorectal cancer surgery using Senhance Digital Laparoscopy System. Asian J. Endosc. Surg. 2022, 15, 613–618. [Google Scholar] [CrossRef]
- Spinelli, A.; David, G.; Gidaro, S.; Carvello, M.; Sacchi, M.; Montorsi, M.; Montroni, I. First experience in colorectal surgery with a new robotic platform with haptic feedback. Color. Dis. 2017, 20, 228–235. [Google Scholar] [CrossRef]
- Darwich, I.; Stephan, D.; Klöckner-Lang, M.; Scheidt, M.; Friedberg, R.; Willeke, F. A roadmap for robotic-assisted sigmoid resection in diverticular disease using a Senhance™ Surgical Robotic System: Results and technical aspects. J. Robot. Surg. 2020, 14, 297–304. [Google Scholar] [CrossRef]
- Hirano, Y.; Kondo, H.; Yamaguchi, S. Robot-assisted surgery with Senhance robotic system for colon cancer: Our original single-incision plus 2-port procedure and a review of the literature. Tech. Coloproctol. 2021, 25, 467–471. [Google Scholar] [CrossRef]
- Huscher, C.; Marchegiani, F.; Cobellis, F.; Tejedor, P.; Pastor, C.; Lazzarin, G.; Wheeler, J.; Di Saverio, S. Robotic oncologic colorectal surgery with a new robotic platform (CMR Versius): Hope or hype? A preliminary experience from a full-robotic case-series. Tech. Coloproctol. 2022, 26, 745–753. [Google Scholar] [CrossRef]
- Kim, H.J.; Choi, G.S.; Song, S.H.; Park, J.S.; Park, S.Y.; Lee, S.M.; Choi, J.A. An initial experience with a novel technique of single-port robotic resection for rectal cancer. Tech. Coloproctol. 2021, 25, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhu, S.; Juan, J.; Yi, B. Preliminary exploration of robotic complete mesocolic excision for colon cancer with the domestically produced Chinese minimally invasive Micro Hand S surgical robot system. Int. J. Med. Robot. 2020, 16, e2148. [Google Scholar] [CrossRef] [PubMed]
- Piozzi, G.N.; Kim, J.S.; Choo, J.M.; Shin, S.H.; Kim, J.S.; Lee, T.H.; Baek, S.J.; Kwak, J.M.; Kim, J.; Kim, S.H. Da Vinci SP robotic approach to colorectal surgery: Two specific indications and short-term results. Tech. Coloproctol. 2022, 26, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Puntambekar, S.P.; Rajesh, K.N.; Goel, A.; Hivre, M.; Bharambe, S.; Chitale, M.; Panse, M. Colorectal cancer surgery: By Cambridge Medical Robotics Versius Surgical Robot System-a single-institution study. Our experience. J. Robot. Surg. 2022, 16, 587–596. [Google Scholar] [CrossRef]
- Samalavicius, N.E.; Dulskas, A.; Janusonis, V.; Klimasauskiene, V.; Eismontas, V.; Deduchovas, O.; Janusonis, T.; Markelis, R.; Smolskas, E. Robotic colorectal surgery using the Senhance® robotic system: A single center experience. Tech. Coloproctol. 2022, 26, 437–442. [Google Scholar] [CrossRef]
- Song, S.H.; Kim, H.J.; Choi, G.S.; Park, J.S.; Park, S.Y.; Lee, S.M.; Choi, J.A. Initial experience with a suprapubic single-port robotic right hemicolectomy in patients with colon cancer. Tech. Coloproctol. 2021, 25, 1065–1071. [Google Scholar] [CrossRef]
- Liu, S.; Kelley, S.R.; Behm, K.T. Single-port robotic transanal minimally invasive surgery (SPR-TAMIS) approach to local excision of rectal tumors. Tech. Coloproctol. 2021, 25, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Marks, J.H.; Kunkel, E.; Salem, J.F.; Martin, C.T.; Anderson, B.; Agarwal, S. First Clinical Experience With Single-Port Robotic Transanal Minimally Invasive Surgery: Phase II Trial of the Initial 26 Cases. Dis. Colon. Rectum 2021, 64, 1003–1013. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, N.; Penezic, L.; Kulis, T.; Zekulic, T.; Saic, H.; Hudolin, T.; Kastelan, Z. Senhance robot-assisted adrenalectomy: A case series. Croat. Med. J. 2022, 63, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Raffaelli, M.; Gallucci, P.; Voloudakis, N.; Pennestrì, F.; De Cicco, R.; Arcuri, G.; De Crea, C.; Bellantone, R. The new robotic platform Hugo™ RAS for lateral transabdominal adrenalectomy: A first world report of a series of five cases. Updates Surg. 2023, 75, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Jo, H.S.; Kim, D.S.; Yu, Y.D. Single-port robot plus one port (SP + 1) distal pancreatectomy using the new da Vinci SP system. Langenbecks Arch. Surg. 2022, 407, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Liu, Q.; Zhao, G.; Zhao, Z.; Li, M.; Gao, Y. Single-port (SP) robotic pancreatic surgery using the da Vinci SP system: A retrospective study on prospectively collected data in a consecutive patient cohort. Int. J. Surg. 2022, 104, 106782. [Google Scholar] [CrossRef]
- Go, J.; Ahn, J.H.; Park, J.M.; Choi, S.B.; Lee, J.; Kim, J.Y.; Park, H.S. Analysis of robot-assisted nipple-sparing mastectomy using the da Vinci SP system. J. Surg. Oncol. 2022, 126, 417–424. [Google Scholar] [CrossRef]
- Ho, J.; Kim, D.; Lee, J.E.; Kim, J.K.; Lee, C.R.; Kang, S.W.; Jeong, J.J.; Nam, K.H.; Chung, W.Y. Single-Port Transaxillary Robotic Modified Radical Neck Dissection (STAR-RND): Initial Experiences. Laryngoscope 2022, 133, 709–714. [Google Scholar] [CrossRef]
- Kim, K.; Kang, S.W.; Kim, J.K.; Lee, C.R.; Lee, J.; Jeong, J.J.; Nam, K.H.; Chung, W.Y. Robotic Transaxillary Hemithyroidectomy Using the da Vinci SP Robotic System: Initial Experience With 10 Consecutive Cases. Surg. Innov. 2020, 27, 256–264. [Google Scholar] [CrossRef]
- Park, J.; Kang, L.K.; Kim, K.; Bae, J.S.; Kim, J.S. The learning curve for single-port transaxillary robotic thyroidectomy (SP-TART): Experience through initial 50 cases of lobectomy. Updates Surg. 2022, 75, 691–700. [Google Scholar] [CrossRef]
- Li, W.; Kong, K.; Li, P.; Wang, G.; Cui, B.; Zhu, L.; Zhu, S. Robot-assisted sleeve gastrectomy in patients with obesity with a novel Chinese domestic MicroHand SII surgical system. BMC Surg. 2021, 21, 260. [Google Scholar] [CrossRef]
- Puntambekar, S.; Bharambe, S.; Pawar, S.; Chitale, M.; Panse, M. Feasibility of transthoracic esophagectomy with a next-generation surgical robot. Sci. Rep. 2022, 12, 17925. [Google Scholar] [CrossRef]
- Schmitz, R.; Willeke, F.; Darwich, I.; Kloeckner-Lang, S.M.; Saelzer, H.; Labenz, J.; Borkenstein, D.P.; Zani, S. Robotic-Assisted Nissen Fundoplication with the Senhance® Surgical System: Technical Aspects and Early Results. Surg. Technol. Int. 2019, 35, 113–119. [Google Scholar]
- Bianco, F.M.; Dreifuss, N.H.; Chang, B.; Schlottmann, F.; Cubisino, A.; Mangano, A.; Pavelko, Y.; Masrur, M.A.; Giulianotti, P.C. Robotic single-port surgery: Preliminary experience in general surgery. Int. J. Med. Robot. 2022, 18, e2453. [Google Scholar] [CrossRef]
- deBeche-Adams, T.; Eubanks, W.S.; de la Fuente, S.G. Early experience with the Senhance®-laparoscopic/robotic platform in the US. J. Robot. Surg. 2019, 13, 357–359. [Google Scholar] [CrossRef]
- Dixon, F.; Khanna, A.; Vitish-Sharma, P.; Singh, N.S.; Nakade, K.; Singh, A.; Qureshi, A.; O’Hara, R.; Keeler, B.D. Initiation and feasibility of a multi-specialty minimally invasive surgical programme using a novel robotic system: A case series. Int. J. Surg. 2021, 96, 106182. [Google Scholar] [CrossRef] [PubMed]
- El Dahdah, J.; Halabi, M.; Kamal, J.; Zenilman, M.E.; Moussa, H. Initial experience with a novel robotic surgical system in abdominal surgery. J. Robot. Surg. 2022, 17, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Kelkar, D.; Borse, M.A.; Godbole, G.P.; Kurlekar, U.; Slack, M. Interim safety analysis of the first-in-human clinical trial of the Versius surgical system, a new robot-assisted device for use in minimal access surgery. Surg. Endosc. 2021, 35, 5193–5202. [Google Scholar] [CrossRef] [PubMed]
- Montlouis-Calixte, J.; Ripamonti, B.; Barabino, G.; Corsini, T.; Chauleur, C. Senhance 3-mm robot-assisted surgery: Experience on first 14 patients in France. J. Robot. Surg. 2019, 13, 643–647. [Google Scholar] [CrossRef]
- Samalavicius, N.E.; Janusonis, V.; Siaulys, R.; Jasėnas, M.; Deduchovas, O.; Venckus, R.; Ezerskiene, V.; Paskeviciute, R.; Klimaviciute, G. Robotic surgery using Senhance® robotic platform: Single center experience with first 100 cases. J. Robot. Surg. 2020, 14, 371–376. [Google Scholar] [CrossRef]
- Stephan, D.; Darwich, I.; Willeke, F. The TransEnterix European Patient Registry for Robotic-Assisted Laparoscopic Procedures in Urology, Abdominal, Thoracic, and Gynecologic Surgery (“TRUST”). Surg. Technol. Int. 2021, 38, 103–107. [Google Scholar] [PubMed]
- Wehrmann, S.; Tischendorf, K.; Mehlhorn, T.; Lorenz, A.; Gündel, M.; Rudolph, H.; Mirow, L. Clinical implementation of the Versius robotic surgical system in visceral surgery-A single centre experience and review of the first 175 patients. Surg. Endosc. 2023, 37, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Liu, Y.; Li, Z.; Yi, B.; Wang, G.; Zhu, S. Chinese surgical robot micro hand S: A consecutive case series in general surgery. Int. J. Surg. 2020, 75, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Yi, B.; Wang, G.; Li, J.; Jiang, J.; Son, Z.; Su, H.; Zhu, S.; Wang, S. Domestically produced Chinese minimally invasive surgical robot system “Micro Hand S” is applied to clinical surgery preliminarily in China. Surg. Endosc. 2017, 31, 487–493. [Google Scholar] [CrossRef]
- Yi, B.; Wang, G.; Li, J.; Jiang, J.; Son, Z.; Su, H.; Zhu, S. The first clinical use of domestically produced Chinese minimally invasive surgical robot system “Micro Hand S”. Surg. Endosc. 2016, 30, 2649–2655. [Google Scholar] [CrossRef]
- Dreifuss, N.H.; Chang, B.; Schlottmann, F.; Cubisino, A.; Mangano, A.; Masrur, M.A.; Bianco, F.M. Robotic inguinal hernia repair: Is the new Da Vinci single port platform providing any benefit? Surg. Endosc. 2022, 37, 2003–2013. [Google Scholar] [CrossRef]
- Kang, Y.H.; Kang, J.S.; Cho, Y.S.; Kim, H.S.; Lee, M.; Han, Y.; Sohn, H.J.; Kim, H.; Kwon, W.; Jang, J.Y.; et al. A retrospective multicentre study on the evaluation of perioperative outcomes of single-port robotic cholecystectomy comparing the Xi and SP versions of the da Vinci robotic surgical system. Int. J. Med. Robot. 2022, 18, e2345. [Google Scholar] [CrossRef]
- Kim, W.J.; Choi, S.B.; Kim, W.B. Feasibility and Efficacy of Single-Port Robotic Cholecystectomy Using the da Vinci SP® Platform. JSLS J. Soc. Laparosc. Robot. Surg. 2022, 26, e2021.00091. [Google Scholar] [CrossRef]
- Samalavicius, N.E.; Kaminskas, T.; Zidonis, Z.; Janusonis, V.; Deduchovas, O.; Eismontas, V.; Nausediene, V.; Dulskas, A. Robotic cholecystectomy using Senhance robotic platform versus laparoscopic conventional cholecystectomy: A propensity score analysis. Acta Chir. Belg. 2022, 122, 160–163. [Google Scholar] [CrossRef]
- Wang, G.; Yi, B.; Li, Z.; Zhu, L.; Hao, L.; Zeng, Y.; Zhu, S. Micro-Hand Robot-Assisted Versus da Vinci Robot-Assisted Cholecystectomy: A Multi-centre, Randomized Controlled Trial. World J. Surg. 2022, 46, 2632–2641. [Google Scholar] [CrossRef]
- Jiang, J.; Zhu, S.; Yi, B.; Li, J. Comparison of the short-term operative, Oncological, and Functional Outcomes between two types of robot-assisted total mesorectal excision for rectal cancer: Da Vinci versus Micro Hand S surgical robot. Int. J. Med. Robot. 2021, 17, e2260. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.; Jiang, J.; Zhu, S.; Yi, B.; Li, J. Comparison of the short-term efficacy of two types of robotic total mesorectal excision for rectal cancer. Tech. Coloproctol. 2022, 26, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, M.; Lei, Y.; Zhang, H.; Xie, J.; Zhu, S.; Jiang, J.; Li, J.; Yi, B. Evaluation of effect of robotic versus laparoscopic surgical technology on genitourinary function after total mesorectal excision for rectal cancer. Int. J. Surg. 2022, 104, 106800. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Liu, Y.; Zhu, H.; Li, X.; Gao, W.; Li, X.; Zhu, S.; Yu, X. The MicroHand S robotic-assisted versus Da Vinci robotic-assisted radical resection for patients with sigmoid colon cancer: A single-center retrospective study. Surg. Endosc. 2020, 34, 3368–3374. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, Z.; Yi, B.; Zhu, S. Initial experience of Chinese surgical robot “Micro Hand S’’-assisted versus open and laparoscopic total mesorectal excision for rectal cancer: Short-term outcomes in a single center. Asian J. Surg. 2022, 45, 299–306. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, G.; Li, Z.; Ling, H.; Yi, B.; Zhu, S. Comparison of the operative outcomes and learning curves between laparoscopic and “Micro Hand S” robot-assisted total mesorectal excision for rectal cancer: A retrospective study. BMC Gastroenterol. 2021, 21, 251. [Google Scholar] [CrossRef]
- Zeng, Y.; Wang, G.; Li, Z.; Lin, H.; Zhu, S.; Yi, B. The Micro Hand S vs. da Vinci Surgical Robot-Assisted Surgery on Total Mesorectal Excision: Short-Term Outcomes Using Propensity Score Matching Analysis. Front. Surg. 2021, 8, 656270. [Google Scholar] [CrossRef]
- Zeng, Y.; Wang, G.; Liu, Y.; Li, Z.; Yi, B.; Zhu, S. The “Micro Hand S” Robot-Assisted Versus Conventional Laparoscopic Right Colectomy: Short-Term Outcomes at a Single Center. J. Laparoendosc. Adv. Surg. Tech. A 2020, 30, 363–368. [Google Scholar] [CrossRef]
- Lee, I.A.; Kim, J.K.; Kim, K.; Kang, S.W.; Lee, J.; Jeong, J.J.; Nam, K.H.; Chung, W.Y. Robotic Adrenalectomy Using the da Vinci SP Robotic System: Technical Feasibility Comparison with Single-Port Access Using the da Vinci Multi-arm Robotic System. Ann. Surg. Oncol. 2022, 29, 3085–3092. [Google Scholar] [CrossRef]
- Kim, J.K.; Choi, S.H.; Choi, S.M.; Choi, H.R.; Lee, C.R.; Kang, S.W.; Jeong, J.J.; Nam, K.H.; Chung, W.Y. Single-port transaxillary robotic thyroidectomy (START): 200-cases with two-step retraction method. Surg. Endosc. 2022, 36, 2688–2696. [Google Scholar] [CrossRef]
- Cambridge Medical Robotics. 10,000 Cases—Making Every Procedure Count. Available online: https://cmrsurgical.com/features/making-every-procedure-count (accessed on 23 May 2023).
- Cambridge Medical Robotics. CMR Surgical Announces More Than 100 Versius Systems Installed Globally. Available online: https://cmrsurgical.com/news/cmr-announces-more-than-100-systems-installed (accessed on 23 May 2023).
- Intuitive Surgical. Annual Report Pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934—Form 10-K. Available online: https://isrg.intuitive.com/static-files/f9d16f73-dcea-419e-ac73-7ae13b86c207 (accessed on 23 May 2023).
- Asensus. Asensus Surgical Provides Corporate Update. Available online: https://ir.asensus.com/news-releases/news-release-details/asensus-surgical-provides-corporate-update (accessed on 23 May 2023).
- Japan 2 Earth. Japan’s First Surgical Robot: Technological Innovation in the World of Medicine. Available online: https://featured.japan-forward.com/japan2earth/2023/01/2034/ (accessed on 23 May 2023).
- Avateramedical. Avateramedical Robot-Assisted Surgery System Progresses to Clinical Use. Available online: https://www.avatera.eu/en/company/news/detail?tx_news_pi1%5Bnews%5D=42&cHash=84ba505a890ba27dcf6bec17706087cf (accessed on 23 May 2023).
- Distalmotion. Available online: https://www.distalmotion.com/news (accessed on 23 May 2023).
- SAGES. Moon Surgical Maestro Surgical Robotics System. Available online: https://www.sages.org/publications/tavac/moon-surgical-maestro-surgical-robotics-system/ (accessed on 23 May 2023).
- Madanapalle, A. ‘Made in India’ Surgical Robot SSI Mantra Completes 100 Successful Surgeries. Available online: https://www.news9live.com/health/medicine/made-in-india-surgical-robot-ssi-mantra-completes-100-successful-surgeries-au941-2068412 (accessed on 23 May 2023).
- RobSurgical. Rob Surgical Receives Authorisation to Conduct Fih Clinical Trials. Available online: https://www.robsurgical.com/rob-surgical-receives-fih-authorisation/ (accessed on 23 May 2023).
- Soumpasis, I.; Nashef, S.; Dunning, J.; Moran, P.; Slack, M. Safe Implementation of a Next-Generation Surgical Robot: First Analysis of 2,083 Cases in the Versius Surgical Registry. Ann. Surg. 2023. [Google Scholar] [CrossRef]
- Race, A.; Horgan, S. Overview of Current Robotic Technology. In Innovative Endoscopic and Surgical Technology in the GI Tract; Horgan, S., Fuchs, K.-H., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 1–17. [Google Scholar] [CrossRef]
- Grimsley, E.A.; Barry, T.M.; Janjua, H.; Eguia, E.; DuCoin, C.; Kuo, P.C. Exploring the paradigm of robotic surgery and its contribution to the growth of surgical volume. Surg. Open Sci. 2022, 10, 36–42. [Google Scholar] [CrossRef]
- Bianchi, P.P.; Salaj, A.; Rocco, B.; Formisano, G. First worldwide report on Hugo RAS surgical platform in right and left colectomy. Updates Surg. 2023, 75, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Quijano, Y.; Vicente, E.; Ferri, V.; Naldini, C.; Pizzuti, G.; Caruso, R. Robot-assisted Nissen fundoplication with the new HUGO Robotic assisted system: First worldwide report with system description, docking settings and video. Int. J. Surg. Case Rep. 2023, 106, 108178. [Google Scholar] [CrossRef]
- de’Angelis, N.; Khan, J.; Marchegiani, F.; Bianchi, G.; Aisoni, F.; Alberti, D.; Ansaloni, L.; Biffl, W.; Chiara, O.; Ceccarelli, G.; et al. Robotic surgery in emergency setting: 2021 WSES position paper. World J. Emerg. Surg. 2022, 17, 4. [Google Scholar] [CrossRef]
- O’Meara, S. Medical robotics in China: The rise of technology in three charts. Nature 2020, 582, S51–S52. [Google Scholar] [CrossRef]
- Guo, Y.; Chen, W.; Zhao, J.; Yang, G.-Z. Medical Robotics: Opportunities in China. Annu. Rev. Control Robot. Auton. Syst. 2022, 5, 361–383. [Google Scholar] [CrossRef]
- Harbin Sagebot Intelligent Medical Equipment Co., Ltd. KangDuo Robot Has Passed the Registration Review of the NMPA. Available online: http://www.hrbszr.com (accessed on 23 May 2023).
- Medbot. FAHZU Completed the First DomesticChinese-Developed 4-Arm Laparoscopic Robot-Assisted Total Intracavitary Radical Cystectomy & Orthotopic Neobladder in China. Available online: https://www.medbotsurgical.com/ (accessed on 23 May 2023).
- Ronovo Surgical. Ronovo Wins Resounding KOL Accolades in Latest Carina™ RAS Platform Animal Labs. Available online: https://www.ronovosurgical.com (accessed on 23 May 2023).
- Kikuchi, K.; Suda, K.; Shibasaki, S.; Tanaka, T.; Uyama, I. Challenges in improving the minimal invasiveness of the surgical treatment for gastric cancer using robotic technology. Ann. Gastroenterol. Surg. 2021, 5, 604–613. [Google Scholar] [CrossRef]
- Orsi Academy. Orsi Academy Welcomes Medicaroid’s Hinotori™ Surgical Robot System*, a World’s First! Available online: https://www.orsi-online.com/news/worlds-first-orsi-welcomes-hinotoritm-surgical-robot-medicaroid (accessed on 23 May 2023).
- Tuliao, P.H.; Kim, S.W.; Rha, K.H. New technologies in robotic surgery: The Korean experience. Curr. Opin. Urol. 2014, 24, 111–117. [Google Scholar] [CrossRef]
- Bora, G.S.; Narain, T.A.; Sharma, A.P.; Mavuduru, R.S.; Devana, S.K.; Singh, S.K.; Mandal, A.K. Robot-assisted surgery in India: A SWOT analysis. Indian. J. Urol. 2020, 36, 1–3. [Google Scholar] [CrossRef]
- Cisu, T.; Crocerossa, F.; Carbonara, U.; Porpiglia, F.; Autorino, R. New robotic surgical systems in urology: An update. Curr. Opin. Urol. 2021, 31, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Zhang, J.; Li, X.; Li, Y.; Su, S. Comparative outcomes of single-incision laparoscopic, mini-laparoscopic, four-port laparoscopic, three-port laparoscopic, and single-incision robotic cholecystectomy: A systematic review and network meta-analysis. Updates Surg. 2023, 75, 41–51. [Google Scholar] [CrossRef] [PubMed]
- de’Angelis, N.; Marchegiani, F.; Schena, C.A.; Khan, J.; Agnoletti, V.; Ansaloni, L.; Barria Rodriguez, A.G.; Bianchi, P.P.; Biffl, W.; Bravi, F.; et al. Training curriculum in minimally invasive emergency digestive surgery: 2022 WSES position paper. World J. Emerg. Surg. 2023, 18, 11. [Google Scholar] [CrossRef] [PubMed]
- Stefanidis, D.; Huffman, E.M.; Collins, J.W.; Martino, M.A.; Satava, R.M.; Levy, J.S. Expert Consensus Recommendations for Robotic Surgery Credentialing. Ann. Surg. 2022, 276, 88–93. [Google Scholar] [CrossRef]
- Burke, J.R.; Fleming, C.A.; King, M.; El-Sayed, C.; Bolton, W.S.; Munsch, C.; Harji, D.; Bach, S.P.; Collins, J.W. Utilising an accelerated Delphi process to develop consensus on the requirement and components of a pre-procedural core robotic surgery curriculum. J. Robot. Surg. 2023. online ahead of print. [Google Scholar] [CrossRef]
- Sighinolfi, M.C.; Terzoni, S.; Scanferla, E.; Bianchi, P.P.; Formisano, G.; Gaia, G.; Marconi, A.M.; Chiumello, D.; Patel, V.; Moschovas, M.C.; et al. Impact of hands-on practice with HugoRAS and Versius System simulators on the attractiveness of robotic surgery among medical and nurse undergraduate students. J. Robot. Surg. 2023. online ahead of print. [Google Scholar] [CrossRef]
- Myklebust, M.V.; Storheim, H.; Hartvik, M.; Dysvik, E. Anesthesia Professionals’ Perspectives of Teamwork During Robotic-Assisted Surgery. AORN J. 2020, 111, 87–96. [Google Scholar] [CrossRef]
- Larkins, K.M.; Mohan, H.M.; Gray, M.; Costello, D.M.; Costello, A.J.; Heriot, A.G.; Warrier, S.K. Transferability of robotic console skills by early robotic surgeons: A multi-platform crossover trial of simulation training. J. Robot. Surg. 2022, 17, 859–867. [Google Scholar] [CrossRef]
- Ghazi, A.; Schuler, N.; Saba, P.; Holler, T.; Steinmetz, A.; Yuen, K.; Doersch, K.; Ellis, E.; Tabayoyong, W.; Bloom, J.; et al. Do Skills Naturally Transfer Between Multiport and Single-Port Robotic Platforms? A Comparative Study in a Simulated Environment. J. Endourol. 2023, 37, 233–239. [Google Scholar] [CrossRef]
- Hussein, A.A.; Mohsin, R.; Qureshi, H.; Leghari, R.; Jing, Z.; Ramahi, Y.O.; Rizvi, I.; Guru, K.A.; Rizvi, A. Transition from da Vinci to Versius robotic surgical system: Initial experience and outcomes of over 100 consecutive procedures. J. Robot. Surg. 2023, 17, 419–426. [Google Scholar] [CrossRef]
- Nakauchi, M.; Suda, K.; Nakamura, K.; Tanaka, T.; Shibasaki, S.; Inaba, K.; Harada, T.; Ohashi, M.; Ohigashi, M.; Kitatsuji, H.; et al. Establishment of a new practical telesurgical platform using the hinotori Surgical Robot System: A preclinical study. Langenbecks Arch. Surg. 2022, 407, 3783–3791. [Google Scholar] [CrossRef]
- Asensus. Asensus Surgical Receives CE Mark for Expanded Machine Vision Capabilities. Available online: https://ir.asensus.com/news-releases/news-release-details/asensus-surgical-receives-ce-mark-expanded-machine-vision (accessed on 23 May 2023).


{kind=link}
| Robotic Platform | Intuitive Surgical Da Vinci SP® | CMR Versius® | Asensus Senhance® | Wego MicroHand S/SII | Medrobotics Flex® | Meerecompany Revo-i™ | Medtronic Hugo™ RAS | Total Cases Per Specialty | |
|---|---|---|---|---|---|---|---|---|---|
| Surgical Specialty | |||||||||
| Hepatobiliary | 386 | 422 | 114 | 96 | 0 | 17 | 0 | 1035 | |
| Colorectal | 78 | 169 | 251 | 209 | 33 | 0 | 1 | 741 | |
| Abdominal wall | 89 | 97 | 345 | 0 | 0 | 0 | 0 | 531 | |
| Endocrine | 298 | 5 | 12 | 0 | 0 | 0 | 0 | 315 | |
| Upper GI | 4 | 69 | 19 | 32 | 0 | 0 | 0 | 124 | |
| Breast | 73 | 0 | 0 | 0 | 0 | 0 | 0 | 73 | |
| Total cases per platform | 928 | 762 | 741 | 337 | 33 | 17 | 1 | 2819 | |
| Clinically Adopted Platforms | ||||
|---|---|---|---|---|
| Company | Product Name | Country | Regulatory Approvals | Marketing Information (n. Procedures/Platform) |
| Medtronic | Hugo™ RAS | US | FDA: ongoing CE-mark: general surgery; urology; gynecology Australian TGA: urology; gynecology Health Canada: general surgery MHLW PMDA Japan: urology; gynecology | NR |
| Cambridge Medical Robotics | Versius® | England | CE-mark: general surgery; urology; gynecology; thoracic surgery Australian TGA: general surgery; urology; gynecology Anvisa Brazil: general surgery; urology; gynecology Other countries: India; Pakistan; Egypt | 10,000 procedures performed (March 2023) [114] >100 installed platforms (November 2022) [115] |
| Intuitive Surgical | Da Vinci SP® | US | FDA: urology; transoral procedures MHLW PMDA Japan: urology; gynecology; general surgery; thoracic surgery; transoral MFDS Korea: urology; general surgery; gynecology; thoracic surgery; transoral NMPA China: yes, not specified | 121 installed platform (December 2022) [116] A’design award winner 2019 |
| Medrobotics Corp. | Flex® Robotic System | US | FDA: transoral; colorectal; general surgery; gynecology; thoracic surgery CE-mark: colorectal Australian TGA: colorectal | Bankrupt of the producing company |
| Asensus (formerly TransEnterix) | Senhance® ALF-X | US | FDA: general surgery; gynecology. Pediatric surgery expected in 2023 CE-mark: general surgery; gynecology; pediatric surgery MHLW PMDA Japan: urology; gynecology; general surgery; thoracic surgery Roszdravnadzor—Russia: yes, not specified Taiwan: yes, not specified | >10,000 procedures performed (February 2023) >49 installed platforms between 2016 and 2022 [117] |
| Meerecompany Inc. | Revo-i™ | South Korea | MFDS Korea: urology; gynecology; general surgery | NR |
| Wego | Micro Hand S | China | NMPA China: general surgery | Reddot award winner 2022 |
| Platforms under Clinical Investigation | ||||
| Company | Product Name | Country | Regulatory Approvals | Marketing Information |
| Medicaroid | Hinotori™ | Japan | MHLW PMDA Japan: urology; gastrointestinal; gynecology | 840 procedures (December 2022) 28 installed platforms (September 2022) [118] |
| Avatera Medical | Avatera | Germany | CE-mark: urology; gynecology | Fist clinical procedure in May 2022 [119] |
| Distalmotion | Dexter | Switzerland | CE-mark: general surgery; gynecology | 4 installed platforms [120] iF design award 2020 |
| Moon Surgical | Maestro | US | FDA: laparoscopic procedures CE-mark: laparoscopic procedures | 30 procedures performed [121] |
| Virtual Incision | MIRA | US | FDA: completed IDE for bowel resections. De novo classification pathway ongoing | NR |
| Titan Medical Inc. | ENOS™ (formerly SPORT) | Canada | FDA: planned in 2023 CE-mark: planned in 2023/24 | NR |
| SS Innovation | Mantra | India | FDA: planned in 2023 CE-mark: planned in 2023 Other countries: India | 5 installed platforms 100 procedures performed [122] |
| Rob Surgical Systems S | Bitrack System | Spain | NR | First clinical trial ongoing [123] |
| Robotic Platform | Patient Chart Architecture | Console Architecture | Operative Arms No. | Trocars | Instruments | Instruments’ Reusability | Advanced Energy |
|---|---|---|---|---|---|---|---|
| Medtronic Hugo™ RAS | Modular | Open | 3 | Commercial | Wristed | Reusables (some disposables) | NA |
| Cambridge Medical Robotics Versius® | Modular | Open | 3 | Commercial | Wristed | Reusables | NA |
| Intuitive Surgical Da Vinci SP® | Single port | Closed | 3 | Dedicated + commercial | Wristed | Reusables | NA |
| Medrobotics Corp. Flex® Robotic System | Flexible system | / | 2 | / | Wristed | Disposables | NA |
| Asensus Senhance® ALF-X | Modular | Open | 3 | Commercial | Rigid with a kit of wristed | Reusables | Ultrasonic (rigid) |
| Meerecompany Inc. Revo-i™ | Multiarm | Closed | 3 | Commercial | Wristed | Reusables | Ultrasonic (rigid) |
| Wego Micro Hand S | Multiarm | Open | 2 | Dedicated | Wristed | Reusables | Ultrasonic (rigid) |
| Medicaroid Hinotori™ | Multiarm | Semi-open | 3 | Dedicated | Wristed | Reusables | NA |
| Avatera Medical Avatera | Multiarm | Semi-open | 3 | NR | Wristed | Disposables | NA |
| Distalmotion Dexter | Modular | Open (with laparoscopic screen) | 2 | Commercial | Wristed | Disposables | NA |
| Moon Surgical Maestro | Multiport instrument holder | / | 1 | Commercial | / | / | NA |
| Virtual Incision MIRA | Single port | Open | 2 | NR | Wristed | Reusables | NA |
| Titan Medical Inc. ENOS™ (formerly SPORT) | Single port | Open | 2 | NR | Wristed | Reusables | NA |
| SS Innovation Mantra | Modular | Open | 3 | Dedicated | Wristed | Reusables | NA |
| Rob Surgical Systems S Bitrack System | Multiarm | Open | 3 | Commercial | Wristed | Disposables | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchegiani, F.; Siragusa, L.; Zadoroznyj, A.; Laterza, V.; Mangana, O.; Schena, C.A.; Ammendola, M.; Memeo, R.; Bianchi, P.P.; Spinoglio, G.; et al. New Robotic Platforms in General Surgery: What’s the Current Clinical Scenario? Medicina 2023, 59, 1264. https://doi.org/10.3390/medicina59071264
Marchegiani F, Siragusa L, Zadoroznyj A, Laterza V, Mangana O, Schena CA, Ammendola M, Memeo R, Bianchi PP, Spinoglio G, et al. New Robotic Platforms in General Surgery: What’s the Current Clinical Scenario? Medicina. 2023; 59(7):1264. https://doi.org/10.3390/medicina59071264
Chicago/Turabian StyleMarchegiani, Francesco, Leandro Siragusa, Alizée Zadoroznyj, Vito Laterza, Orsalia Mangana, Carlo Alberto Schena, Michele Ammendola, Riccardo Memeo, Paolo Pietro Bianchi, Giuseppe Spinoglio, and et al. 2023. "New Robotic Platforms in General Surgery: What’s the Current Clinical Scenario?" Medicina 59, no. 7: 1264. https://doi.org/10.3390/medicina59071264
APA StyleMarchegiani, F., Siragusa, L., Zadoroznyj, A., Laterza, V., Mangana, O., Schena, C. A., Ammendola, M., Memeo, R., Bianchi, P. P., Spinoglio, G., Gavriilidis, P., & de’Angelis, N. (2023). New Robotic Platforms in General Surgery: What’s the Current Clinical Scenario? Medicina, 59(7), 1264. https://doi.org/10.3390/medicina59071264