
Point-of-Care Ultrasound—History, Current and Evolving Clinical Concepts in Emergency Medicine


Abstract
:1. Introduction
1.1. “You Have to Know the Past to Understand the Present”—Carl Sagan
1.2. Current EMUS Concepts
- −
- Incomplete to complete coverage of the problem by the sonographic question/s (simple or complex, a single question or multiple yes–no questions, directly or indirectly translatable into the clinical question);
- −
- Degree of difficulty in technical execution;
- −
- Whether rare or common;
- −
- Whether of clinical importance or less relevant;
- −
- Availability of probe and special software (for example, echocardiography).
- Resuscitative;
- Diagnostic;
- Procedural guidance;
- Symptom- or sign-based;
- Therapeutic.
2. Evolving EMUS Concepts
3. Examples of New EMUS Application Possibilities and Concepts
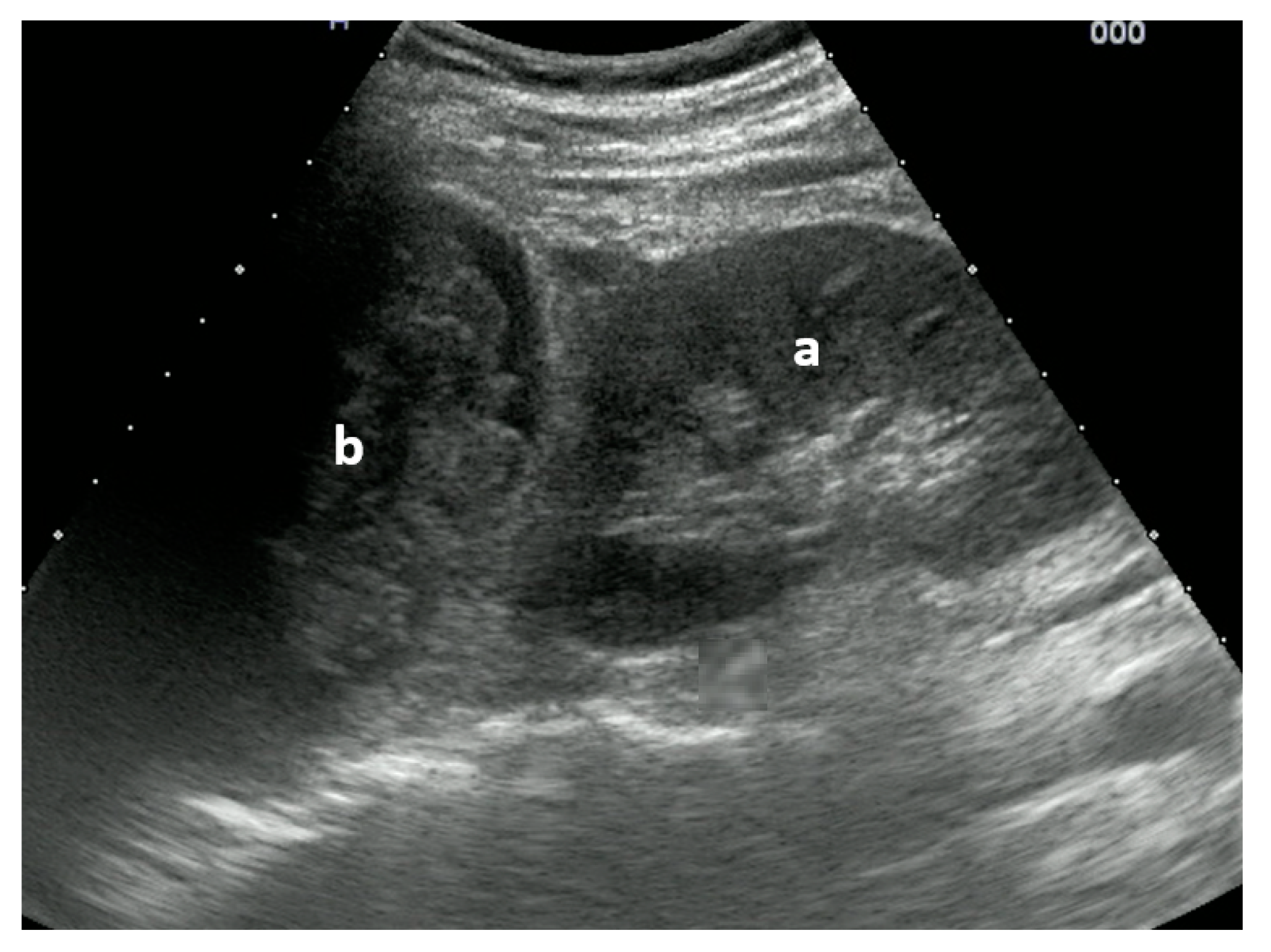
3.1. To New Shores in Trauma
- Expanding E-FAST in stable patients to include additional views for abdominal FAST including the retroperitoneum, evidence of solid organ injury, and free air;
- PoCUS other than traditional E-FAST such as ABCDE during the primary trauma survey;
- The monitoring of hemodynamics including cerebral perfusion in TBI to guide fluid and vasopressor treatment;
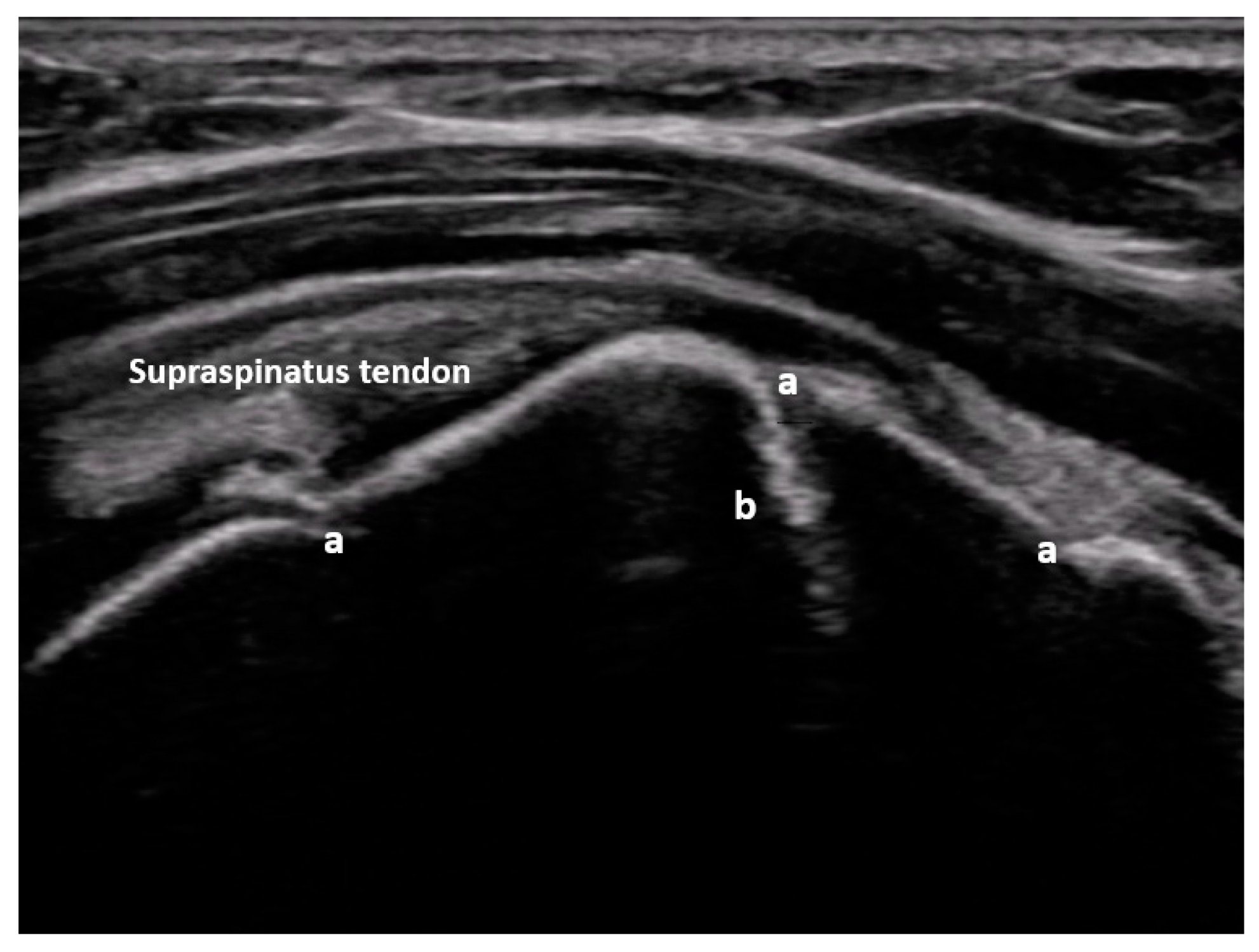
- Search for musculoskeletal and soft-tissue or vascular injuries;
- Guidance with invasive procedures.
Pulmonary Embolism
3.2. From the Stethoscope to PoCUS
3.3. PoCUS-Ultrasound Visualization of Pathophysiological Processes and Correlation of Lung Ultrasound Artifacts with Pathological Lung Changes
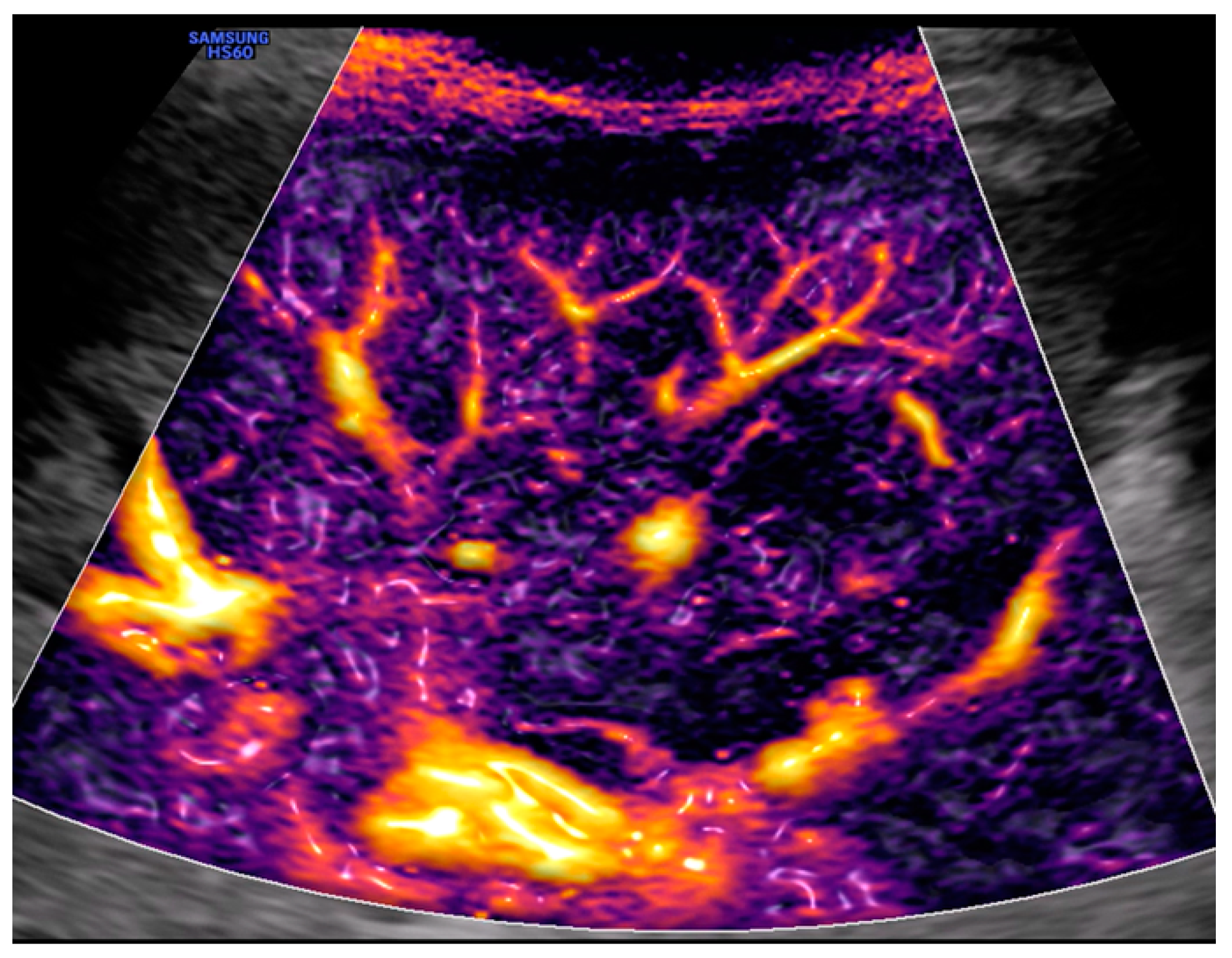
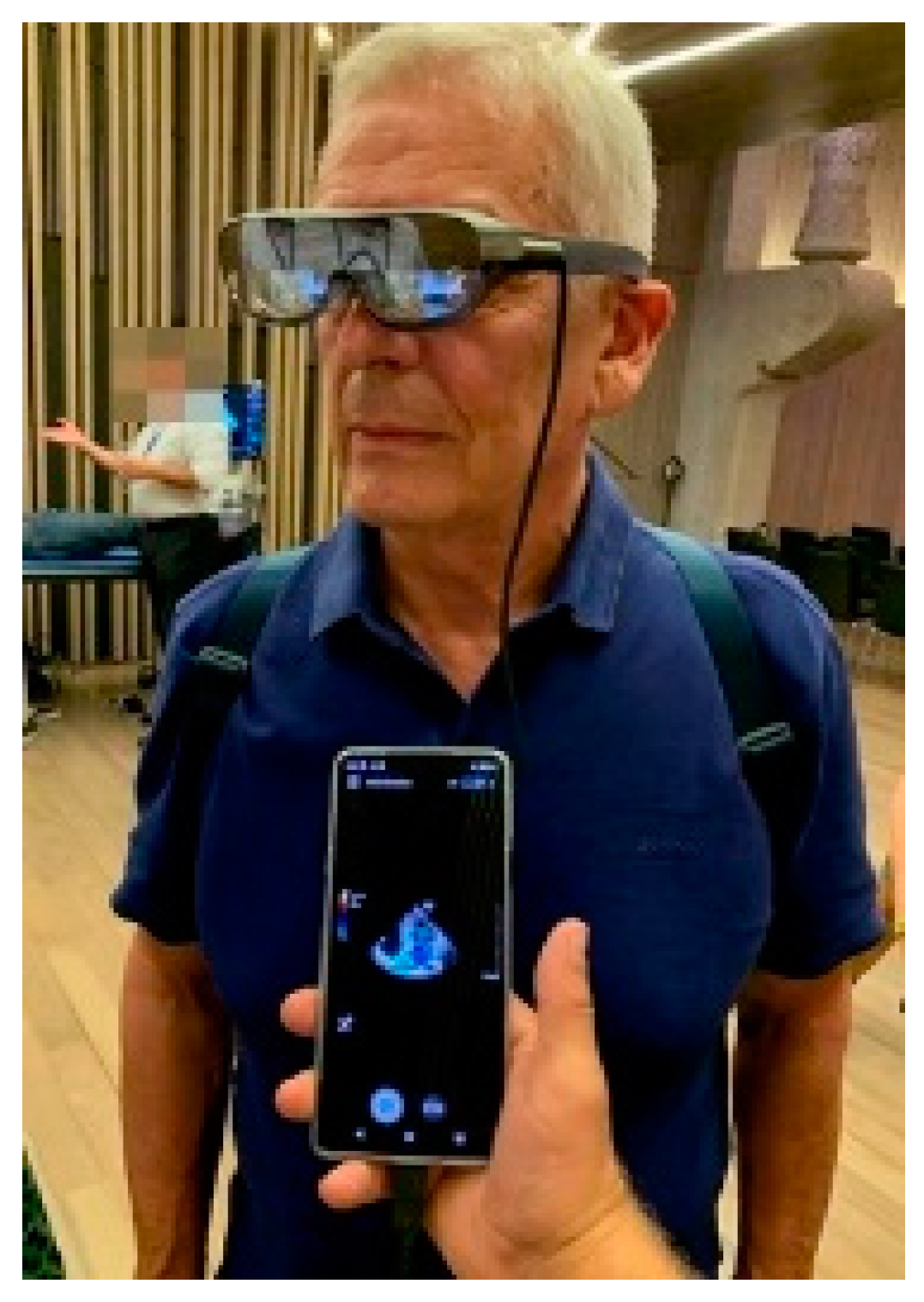
3.4. Technical Innovations
4. Conclusions
- There are new indications that concern all organs and systems of the human body. Only a small part has found its way into routine use. The following are two important examples: ultrasound in trauma patients, which should have gone beyond E-FAST long ago, and pulmonary embolism, which is already a standard among experts.
- As soon as the financial barriers fall, the change from stethoscope, percussion, and mostly palpation, to sonoscope should be implemented as much as possible. That is, the training of clinical examination of medical students must be revolutionized and, wherever possible and appropriate, the already trained physicians must be retrained—a Herculean task.
- A profound insight into the pathophysiological processes and an understanding of the physical phenomena of ultrasound should be combined. This knowledge must be translated into concepts to better handle hemodynamics, especially volume management, and artifact sonography of the lung (b-lines and elastography to determine lung density).
- Technical innovations, such as elastography, advanced color Doppler, CEUS and other flow technology, artificial intelligence, cloud-based PoCUS and smart glasses, await their use in emergencies.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dietrich, C.F.; Bolondi, L.; Duck, F.; Evans, D.H.; Ewertsen, C.; Fraser, A.G.; Gilja, O.H.; Jenssen, C.; Merz, E.; Nolsoe, C.; et al. History of Ultrasound in Medicine from its birth to date (2022), on occasion of the 50 Years Anniversary of EFSUMB. A publication of the European Federation of Societies for Ultrasound In Medicine and Biology (EFSUMB), designed to record the historical development of medical ultrasound. Med. Ultrason. 2022, 24, 434–450. [Google Scholar] [PubMed]
- Hoffmann, B. The future is not the sonoscope. J. Ultrasound Med. 2003, 22, 997–998, author reply 998–1000. [Google Scholar] [PubMed]
- Available online: https://www.ultraschallmuseum.de/index.php?link=120 (accessed on 3 October 2023).
- Rettenmaier, G. Sonografischer Oberbauchstatus. Aussagefähigkeit und Indikationen der Ultraschall-Schnittbilduntersuchung des Oberbauchs [Sonographic status of upper abdomen. Diagnostic significance and indications of the ultrasonic sectional examination of the upper abdomen]. Internist 1976, 17, 549–564. [Google Scholar] [PubMed]
- Kristensen, J.K.; Buemann, B.; Kühl, E. Ultrasonic scanning in the diagnosis of splenic haematomas. Acta Chir. Scand. 1971, 137, 653–657. [Google Scholar] [PubMed]
- Edler, I.; Lindström, K. The history of echocardiography. Ultrasound Med. Biol. 2004, 30, 1565–1644. [Google Scholar] [CrossRef]
- Li, L.; Yong, R.J.; Kaye, A.D.; Urman, R.D. Perioperative Point of Care Ultrasound (POCUS) for Anesthesiologists: An Overview. Curr. Pain. Headache Rep. 2020, 24, 20. [Google Scholar] [CrossRef]
- Sorensen, B.; Hunskaar, S. Point-of-care ultrasound in primary care: A systematic review of generalist performed point-of-care ultrasound in unselected populations. Ultrasound J. 2019, 11, 31. [Google Scholar] [CrossRef] [PubMed]
- Simard, R. Ultrasound Imaging of Orthopedic Injuries. Emerg. Med. Clin. N. Am. 2020, 38, 243–265. [Google Scholar] [CrossRef]
- Breakey, N.; Osterwalder, J.; Mathis, G.; Lehmann, B.; Sauter, T.C. Point of care ultrasound for rapid assessment and treatment of palliative care patients in acute medical settings. Eur. J. Intern. Med. 2020, 81, 7–14. [Google Scholar] [CrossRef]
- Krug, B.; Stützer, H.; Wolters, U.; Mauch, C.; Staib, P.; Töx, U.; Steffen, H.M.; Warm, M.; Ghafur, S.; Araba, F.; et al. Entwicklung der sonographischen Diagnostik in einer Radiologischen Universitätsklinik von 1994 bis 2001 [Development of ultrasonography in a radiological university department from 1994 to 2001]. Rofo 2002, 174, 767–775. [Google Scholar] [CrossRef]
- Liebeskind, M.E.; Arger, P.H.; Liebeskind, A.; Maston, K.; Langlotz, C. Using. sonography to examine adult patients at an academic medical center: Have usage patterns changed with the expansion of managed care? AJR Am. J. Roentgenol. 2002, 179, 1395–1399. [Google Scholar] [CrossRef]
- Strittmatter, B.; Lausen, M.; Salm, R.; Kohlberger, E. Die Wertigkeit der Ultraschalldiagnostik beim stumpfen Bauch- und Thoraxtrauma. Langenbecks Arch. Chiv. 1988, 373, 202–205. [Google Scholar] [CrossRef]
- Jehle, D.; Guarino, J.; Karamanoukian, H. Emergency department ultrasound in the evaluation of blunt abdominal trauma. Am. J. Emerg. Med. 1993, 11, 342–346. [Google Scholar] [CrossRef]
- Rozycki, G.S.; Shackford, S.R. Ultrasound, what every trauma surgeon should know. J. Trauma 1996, 40, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.ob-ultrasound.net/history2.html (accessed on 3 October 2023).
- Schwarz, K.Q.; Meltzer, R.S. Experience rounding with a hand-held two-dimensional cardiac ultrasound device. Am. J. Cardiol. 1988, 62, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Kendall, J.L.; Hoffenberg, S.R.; Smith, R.S. History of emergency and critical care ultrasound: The evolution of a new imaging paradigm. Crit. Care Med. 2007, 35 (Suppl. 5), S126–S130. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.reliasmedia.com/articles/68664-society-for-academic-medicine-ultrasound-position-statement (accessed on 3 October 2023).
- American College of Emergency Physicians. ACEP emergency ultrasound guidelines—2001. Ann Emerg Med. 2001, 38, 470–481. [Google Scholar] [CrossRef]
- Seitz, K.; Braun, B. Sonografie kompetent Von der Indikation zur Interpretation; Georg Thieme Verlag: New York, NY, USA, 2016. [Google Scholar]
- Maio, G. Medicine and the holistic understanding of the human being: Ultrasound examination as dialog. Ultraschall Med. 2014, 35, 98–107. [Google Scholar] [CrossRef]
- Pivetta, E.; Goffi, A.; Nazerian, P.; Castagno, D.; Tozzetti, C.; Tizzani, P.; Tizzani, M.; Porrino, G.; Ferreri, E.; Busso, V.; et al. Lung ultrasound integrated with clinical assessment for the diagnosis of acute decompensated heart failure in the emergency department: A randomized controlled trial. Eur. J. Heart Fail. 2019, 21, 754–766. [Google Scholar] [CrossRef]
- Maw, A.M.; Hassanin, A.; Ho, P.M.; McInnes, M.D.F.; Moss, A.; Juarez-Colunga, E.; Soni, N.J.; Miglioranza, M.H.; Platz, E.; DeSanto, K.; et al. Diagnostic Accuracy of Point-of-Care Lung Ultrasonography and Chest Radiography in Adults With Symptoms Suggestive of Acute Decompensated Heart Failure: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e190703. [Google Scholar] [CrossRef]
- Sconfienza, L.M.; Albano, D.; Allen, G.; Bazzocchi, A.; Bignotti, B.; Chianca, V.; Facal de Castro, F.; Drakonaki, E.E.; Gallardo, E.; Gielen, J.; et al. Clinical indications for musculoskeletal ultrasound updated in 2017 by European Society of Musculoskeletal Radiology (ESSR) consensus. Eur. Radiol. 2018, 28, 5338–5351. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Yoshida, T.; Noma, H.; Nomura, T.; Suzuki, A.; Mihara, T. Diagnostic accuracy of point-of-care ultrasound for shock: A systematic review and meta-analysis. Crit. Care. 2023, 27, 200. [Google Scholar] [CrossRef]
- Wu, J.; Ge, L.; Wang, X.; Jin, Y. Role of point-of-care ultrasound (POCUS) in the diagnosis of an abscess in paediatric skin and soft tissue infections: A systematic review and meta-analysis. Med. Ultrason. 2022, 24, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Wortsman, X. Sonography of Dermatologic Emergencies. J. Ultrasound Med. 2017, 36, 1905–1914. [Google Scholar] [CrossRef] [PubMed]
- Van Loon, F.H.J.; Buise, M.P.; Claassen, J.J.F.; Dierick-van Daele, A.T.M.; Bouwman, A.R.A. Comparison of ultrasound guidance with palpation and direct for peripheral vein cannulation in adult patients: A systematic review and meta-analysis. Br. J. Anaesth. 2018, 121, 358–366. [Google Scholar] [CrossRef]
- Sconfienza, L.M.; Adriaensen, M.; Albano, D.; Alcala-Galiano, A.; Allen, G.; Aparisi Gómez, M.P.; Aringhieri, G.; Bazzocchi, A.; Beggs, I.; Chianca, V.; et al. Clinical indications for image guided interventional procedures in the musculoskeletal system: A Delphi-based consensus paper from the European Society of Musculoskeletal Radiology (ESSR)-part III, nerves of the upper limb. Eur. Radiol. 2020, 30, 1498–1506. [Google Scholar] [CrossRef]
- Brousseau, A. Parent DMBET 3: Advantages of ultrasound-assisted lumbar puncture. Emerg. Med. J. 2016, 33, 163–165. [Google Scholar] [CrossRef]
- Labovitz, A.J.; Noble, V.E.; Bierig, M.; Goldstein, S.A.; Jones, R.; Kort, S.; Porter, T.R.; Spencer, K.T.; Tayal, V.S.; Wei, K. Focused cardiac ultrasound in the emergent setting: A consensus statement of the American Society of Echocardiography and American College of Emergency Physicians. J. Am. Soc. Echocardiogr. 2010, 23, 1225–1230. [Google Scholar] [CrossRef]
- Rubano, E.; Mehta, N.; Caputo, W.; Paladino, L.; Sinert, R. Systematic review: Emergency department bedside ultrasonography for diagnosing suspected abdominal aortic aneurysm. Acad. Emerg. Med. 2013, 20, 128–138. [Google Scholar] [CrossRef]
- Demi, L.; Wolfram, F.; Klersy, C.; De Silvestri, A.; Ferretti, V.V.; Muller, M.; Miller, D.; Feletti, F.; Wełnicki, M.; Buda, N.; et al. New International Guidelines and Consensus on the Use of Lung Ultrasound. J. Ultrasound Med. 2023, 42, 309–344. [Google Scholar] [CrossRef]
- Haji-Hassan, M.; Lenghel, L.M.; Bolboacă, S.D. Hand-Held Ultrasound of the Lung: A Systematic Review. Diagnostics 2021, 11, 1381. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, M.; Scorpiniti, M.; Gigli, C.; Nazerian, P.; Vanni, S.; Innocenti, F.; Stefanone, V.T.; Savinelli, C.; Coppa, A.; Bigiarini, S.; et al. Point-of-Care Ultrasonography for Evaluation of Acute Dyspnea in the ED. Chest 2017, 151, 1295–1301. [Google Scholar] [CrossRef]
- Gottlieb, M.; Patel, D.; Marks, A.; Peksa, G.D. Ultrasound for the diagnosis of shoulder dislocation and reduction: A systematic review and meta-analysis. Acad. Emerg. Med. 2022, 29, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Peksa, G.D.; Pandurangadu, A.V.; Nakitende, D.; Takhar, S.; Seethala, R.R. Utilization of ultrasound for the evaluation of small bowel obstruction: A systematic review and meta-analysis. Am. J. Emerg. Med. 2018, 36, 234–242. [Google Scholar] [CrossRef]
- Barr, L.; Hatch, N.; Roque, P.J.; Wu, T.S. Basic ultrasound-guided procedures. Crit. Care Clin. 2014, 30, 275–304. [Google Scholar] [CrossRef] [PubMed]
- Szabó, G.V.; Szigetváry, C.; Szabó, L.; Dembrovszky, F.; Rottler, M.; Ocskay, K.; Madzsar, S.; Hegyi, P.; Molnár, Z. Point-of-care ultrasound improves clinical outcomes in patients with acute onset dyspnea: A systematic review and meta-analysis. Intern. Emerg. Med. 2023, 18, 639–653. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.; Goldstein, I.; Mourgeon, E.; Cluzel, P.; Grenier, P.; Rouby, J.J. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 2004, 100, 9–15. [Google Scholar] [CrossRef]
- Kimura, B.J. Point-of-care cardiac ultrasound techniques in the physical examination: Better at the bedside. Heart 2017, 103, 987–994. [Google Scholar] [CrossRef]
- Chan, K.K.; Joo, D.A.; McRae, A.D.; Takwoingi, Y.; Premji, Z.A.; Lang, E.; Wakai, A. Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department. Cochrane Database Syst. Rev. 2020, 7, CD013031. [Google Scholar] [CrossRef]
- Huang, C.T.; Chang, C.H.; Chen, J.Y.; Ling, D.A.; Lee, A.F.; Wang, P.H.; Wu, C.K.; Ko, Y.C.; Hsiao, Y.T.; Lien, W.C.; et al. The effect of point-of-care ultrasound on length of stay and mortality in patients with chest pain/dyspnea. Ultraschall Med. 2023, 44, 389–394. [Google Scholar] [CrossRef]
- Wang, P.H.; Chen, J.Y.; Ling, D.A.; Lee, A.F.; Ko, Y.C.; Lien, W.C.; Huang, C.H. Earlier point-of-care ultrasound, shorter length of stay in patients with acute flank pain. Scand. J. Trauma Resusc. Emerg. Med. 2022, 30, 29. [Google Scholar] [CrossRef] [PubMed]
- Guner, N.G.; Yurumez, Y.; Yucel, M.; Alacam, M.; Guner, S.T.; Ercan, B. Effects of Point-of-care Ultrasonography on the Diagnostic Process of Patients Admitted to the Emergency Department with Chest Pain: A Randomised Controlled Trial. J. Coll. Physicians Surg. Pak. 2020, 30, 1262–1268. [Google Scholar] [PubMed]
- Gottlieb, M.; Holladay, D.; Peksa, G.D. Ultrasound-assisted Lumbar Punctures: A Systematic Review and Meta-Analysis. Acad. Emerg. Med. 2019, 26, 85–96. [Google Scholar] [CrossRef]
- Bhatt, M.; Braun, C.; Patel, P.; Patel, P.; Begum, H.; Wiercioch, W.; Varghese, J.; Wooldridge, D.; Alturkmani, H.J.; Thomas, M.; et al. Diagnosis of deep vein thrombosis of the lower extremity: A systematic review and meta-analysis of test accuracy. Blood Adv. 2020, 4, 1250–1264. [Google Scholar] [CrossRef]
- Patel, M.D.; Sill, A.P.; Dahiya, N.; Chen, F.; Eversman, W.G.; Kriegshauser, J.S.; Young, S.W. Performance of an algorithm for diagnosing acute cholecystitis using clinical and sonographic parameters. Abdom. Radiol. 2022, 47, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Ávila-Reyes, D.; Acevedo-Cardona, A.O.; Gómez-González, J.F.; Echeverry-Piedrahita, D.R.; Aguirre-Flórez, M.; Giraldo-Diaconeasa, A. Point-of-care ultrasound in cardiorespiratory arrest (POCUS-CA): Narrative review article. Ultrasound J. 2021, 13, 46. [Google Scholar] [CrossRef]
- American College of Emergency Physicians. Policy Statement. Definition of Clinical Ultrasonography. Approved April. 2023. Available online: https://www.acep.org/siteassets/new-pdfs/policy-statements/ultrasound-guidelines--emergency-point-of-care-and-clinical-ultrasound-guidelines-in-medicine.pdf (accessed on 3 October 2023).
- Frankel, H.L.; Kirkpatrick, A.W.; Elbarbary, M.; Blaivas, M.; Desai, H.; Evans, D.; Summerfield, D.T.; Slonim, A.; Breitkreutz, R.; Price, S.; et al. Guidelines for the Appropriate Use of Bedside General and Cardiac Ultrasonography in the Evaluation of Critically Ill Patients-Part I: General Ultrasonography. Crit. Care Med. 2015, 43, 2479–2502. [Google Scholar] [CrossRef]
- Levitov, A.; Frankel, H.L.; Blaivas, M.; Kirkpatrick, A.W.; Su, E.; Evans, D.; Summerfield, D.T.; Slonim, A.; Breitkreutz, R.; Price, S.; et al. Guidelines for the Appropriate Use of Bedside General and Cardiac Ultrasonography in the Evaluation of Critically Ill Patients-Part II: Cardiac Ultrasonography. Crit. Care Med. 2016, 44, 1206–1227. [Google Scholar] [CrossRef]
- Statement on ultrasound examinations by surgeons. Committee on Emerging Surgical Technology and Education, American College of Surgeons. Bull. Am. Coll. Surg. 1998, 83, 37–40. [Google Scholar]
- Dietrich, C.F.; Goudie, A.; Chiorean, L.; Cui, X.W.; Gilja, O.H.; Dong, Y.; Abramowicz, J.S.; Vinayak, S.; Westerway, S.C.; Nolsøe, C.P.; et al. Point of Care Ultrasound: A WFUMB Position Paper. Ultrasound Med. Biol. 2017, 43, 49–58. [Google Scholar] [CrossRef]
- IFEM Point-of-Care Ultrasound Curriculum Guidance. 2014. Available online: http://www.ifem.cc/Resources/PoliciesandGuidelines.aspx (accessed on 3 October 2023).
- Lewis, D.; Rang, L.; Kim, D.; Robichaud, L.; Kwan, C.; Pham, C.; Shefrin, A.; Ritcey, B.; Atkinson, P.; Woo, M.; et al. Recommendations for the use of point-of-care ultrasound (POCUS) by emergency physicians in Canada. CJEM 2019, 21, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Jarman, R.D.; McDermott, C.; Colclough, A.; Bøtker, M.; Knudsen, L.; Harris, T.; Albaroudi, B.; Albaroudi, O.; Haddad, M.; Darke, R.; et al. EFSUMB Clinical Practice Guidelines for Point-of-Care Ultrasound: Part One (Common Heart and Pulmonary Applications) LONG VERSION. Ultraschall Med. 2023, 44, e1–e24. [Google Scholar] [CrossRef]
- Patel, M.D.; Horrow, M.M.; Kamaya, A.; Frates, M.C.; Dahiya, N.; Golding, L.; Chong, W.K.; Gerena, M.; Ghate, S.; Glanc, P.; et al. Mapping the ultrasound landscape to define point-of-care ultrasound and diagnostic ultrasound: A proposal from the society of radiologists in ultrasound and ACR commission in ultrasound. J. Am. Radiol. 2021, 18, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Jehle, D.; Heller, M. Ultrasonography in Trauma: The FAST Exam; American College of Emergency Physicians: Dallas, TX, USA, 2003. [Google Scholar]
- Osterwalder, J.; Mathis, G.; Hoffmann, B. New Perspectives for Modern Trauma Management—Lessons Learned from 25 Years FAST and 15 Years E-FAST. Ultraschall Med. 2019, 40, 560–583. [Google Scholar] [CrossRef]
- Sutarjono, B.; Kessel, M.; Alexander, D.; Grewal, E. Is it time to re-think FAST? A systematic review and meta-analysis of Contrast-Enhanced Ultrasound (CEUS) and conventional ultrasound for initial assessment of abdominal trauma. BMC Emerg. Med. 2023, 23, 8. [Google Scholar] [CrossRef]
- Ackermann, O. Fraktursonografie; Springer Nature: Berlin, Germany, 2019. [Google Scholar]
- Chen, K.C.; Lin, A.C.; Chong, C.F.; Wang, T.L. An overview of point-of-care ultrasound for soft tissue and musculoskeletal applications in the emergency department. J. Intensive Care 2016, 4, 55. [Google Scholar] [CrossRef] [PubMed]
- Gaitini, D.; Razi, N.B.; Ghersin, E.; Ofer, A.; Soudack, M. Sonographic evaluation of vascular injuries. J. Ultrasound Med. 2008, 27, 95–107. [Google Scholar] [CrossRef]
- Ramsingh, D.; Mangunta, V.R. The Use of Point-of-Care Ultrasonography in Trauma Anesthesia. Anesthesiol. Clin. 2019, 37, 93–106. [Google Scholar] [CrossRef]
- Fernando, S.M.; Tran, A.; Cheng, W.; Rochwerg, B.; Taljaard, M.; Kyeremanteng, K.; English, S.W.; Sekhon, M.S.; Griesdale, D.E.G.; Dowlatshahi, D.; et al. Diagnosis of elevated intracranial pressure in critically ill adults: Systematic review and meta-analysis. BMJ 2019, 366, l4225. [Google Scholar] [CrossRef]
- Shin, S.S.; Huisman, T.A.G.M.; Hwang, M. Ultrasound Imaging for Traumatic Brain Injury. J. Ultrasound Med. 2018, 37, 1857–1867. [Google Scholar] [CrossRef]
- Polyzogopoulou, E.; Velliou, M.; Verras, C.; Ventoulis, I.; Parissis, J.; Osterwalder, J.; Hoffmann, B. Point-of-Care Ultrasound: A Multimodal Tool for the Management of Sepsis in the Emergency Department. Medicina 2023, 59, 1180. [Google Scholar] [CrossRef] [PubMed]
- Mathis, G. Vaskuläre Lungenkonsolidierungen: Lungenembolie und Lungeninfarkt. In Bildatlas der Lungensonographie Hrsg. Gebhard Mathis; Springer: Berlin/Heidelberg, Germany, 2022. [Google Scholar]
- Chen, W.; Xu, K.; Li, Y.; Hao, M.; Yang, Y.; Liu, X.; Huang, X.; Huang, Y.; Ye, Q. Clinical value of thoracic ultrasonography in the diagnosis of pulmonary embolism: A systematic review and meta-analysis. Med. Ultrason. 2022, 24, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Nazerian, P.; Vanni, S.; Volpicelli, G.; Gigli, C.; Zanobetti, M.; Bartolucci, M.; Ciavattone, A.; Lamorte, A.; Veltri, A.; Fabbri, A.; et al. Accuracy of point-of-care multiorgan ultrasonography for the diagnosis of pulmonary embolism. Chest 2014, 145, 950–957. [Google Scholar] [CrossRef] [PubMed]
- Kagima, J.; Stolbrink, M.; Masheti, S.; Mbaiyani, C.; Munubi, A.; Joekes, E.; Mortimer, K.; Rylance, J.; Morton, B. Diagnostic accuracy of combined thoracic and cardiac sonography for the diagnosis of pulmonary embolism: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0235940. [Google Scholar] [CrossRef] [PubMed]
- Koenig, S.; Chandra, S.; Alaverdian, A.; Dibello, C.; Mayo, P.H.; Narasimhan, M. Ultrasound assessment of pulmonary embolism in patients receiving CT pulmonary angiography. Chest 2014, 145, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Fily, R.A. Is it time for the sonoscope? if so, the let’s do it right. J. Ultrasound Med. 2003, 22, 323–325. [Google Scholar] [CrossRef] [PubMed]
- Kobal, S.L.; Trento, L.; Baharami, S.; Tolstrup, K.; Naqvi, T.Z.; Cercek, B.; Neuman, Y.; Mirocha, J.; Kar, S.; Forrester, J.S.; et al. Comparison of effectiveness of hand carried ultrasound to bedside cardiovascular physical examination. Am. J. Cardiol. 2005, 96, 1002–1006. [Google Scholar] [CrossRef]
- Martindale, J.L.; Wakai, A.; Collins, S.P.; Levy, P.D.; Diercks, D.; Hiestand, B.C.; Fermann, G.F.; de Souza, I.; Sinert, R. Diagnosing acute heart failure in the emergency department: A systematic review and meta-analyis. Acad. Emerg. Med. 2016, 23, 223–242. [Google Scholar] [CrossRef]
- Alzahran, S.A.; Al-Salamah, M.A.; Al-Madani, W.H.; Elbarbay, M. Systematic review and meta-analysis for the use of ultrasound versus radiology in diagnosing of pneumonia. Crit. Ultrasound J. 2017, 9, 6. [Google Scholar] [CrossRef]
- Fuster, V. The stethoscope’s prognosis. Very much alive and very necessary. J. Am. Coll. Cardiol. 2016, 67, 1118–1119. [Google Scholar] [CrossRef]
- Solomon, S.D.; Saldana, F. Point-of-Care Ultrasound in medical education—Stop listening and look. N. Engl. J. Med. 2014, 370, 1083–1085. [Google Scholar] [CrossRef]
- Mouratev, G.; Howe, D.; Hoppmann, R.; Poston, M.B.; Reid, R.; Varnadoe, J.; Smith, S.; McCallum, B.; Rao, V.; DeMarco, P. Teaching medical students ultrasound to measure liver size: Comparison with experienced clinicians using physical examination alone. Teach. Learn. Med. 2013, 25, 84–88. [Google Scholar] [CrossRef]
- Tran, T.T.; Hlaing, M.; Krause, M. Point-of-Care Ultrasound: Applications in Low- and Middle-Income Countries. Curr. Anesthesiol. Rep. 2021, 11, 69–75. [Google Scholar] [CrossRef]
- Osterwalder, J.; Tabakovic, S.; Jenssen, C.; Dietrich, C.F.; Connolly, J.; Polyzogopoulou, E.; Cantisani, V.; Wüstner, M.; Jarman, B.; Hoffmann, B. Emergency Point-of-Care Ultrasound Stewardship—A Joint Position Paper by EuSEM and EFSUMB and Endorsed by IFEM and WFUMB. Ultraschall Med. 2023, 44, 379–388, Erratum in Ultraschall Med. 28 April 2023. [Google Scholar] [CrossRef]
- Burleson, S.L.; Pigott, D.C.; Gullett, J.P.; Greene, C.; Gibson, C.B.; Irvine, S.; Kaminstein, D. Point-of-care ultrasound in resource-limited settings: The PURLS fellowship. Ultrasound J. 2020, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Persichini, R.; Lai, C.; Teboul, J.L.; Adda, I.; Guérin, L.; Monnet, X. Venous return and mean systemic filling pressure: Physiology and clinical applications. Crit. Care 2022, 26, 150. [Google Scholar] [CrossRef] [PubMed]
- Kenny, J.E. Assessing fluid intolerance with doppler ultrasonography: A physiological framework. Med. Sci. 2022, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Wang, X.T.; Long, Y.; Liu, D.W. Monitoring changes in hepatic venous velocities flow after a fluid challenge can identify shock patients who lack fluid responsiveness. Chin. Med. J. 2017, 130, 1202–1210. [Google Scholar] [CrossRef]
- Mathis, G.; Horn, R.; Morf, S.; Prosch, H.; Rovida, S.; Soldati, G. WFUMB position paper on reverberation artefacts in lung ultrasound: B-lines or comet-tails? Med. Ultrason. 2021, 23, 70–73. [Google Scholar] [CrossRef]
- Quarato, C.M.I.; Venuti, M.; Dimitri, L.; Lacedonia, D.; Simeone, A.; Mirijello, A.; De Cosmo, S.; Maiello, E.; Taurchini, M.; Scioscia, G.; et al. Transthoracic ultrasound shear wave elastography for the study of subpleural lung lesions. Ultrasonography 2022, 41, 93–105. [Google Scholar] [CrossRef]
- Lu, C.; Merrill, C.; Medellin, A.; Novak, K.; Wilson, S.R. Bowel Ultrasound State of the Art: Grayscale and Doppler Ultrasound, Contrast Enhancement, and Elastography in Crohn Disease. J. Ultrasound Med. 2019, 38, 271–288. [Google Scholar] [CrossRef] [PubMed]
- Michels, G.; Horn, R.; Helfen, A.; Hagendorff, A.; Jung, C.; Hoffmann, B.; Jaspers, N.; Kinkel, H.; Greim, C.A.; Knebel, F.; et al. Standardisierte Kontrastmittelsonographie (CEUS) in der klinischen Akut- und Notfallmedizin sowie Intensivmedizin (CEUS Akut): Konsensuspapier der DGIIN, DIVI, DGINA, DGAI, DGK, ÖGUM, SGUM und DEGUM [Standardized contrast-enhanced ultrasound (CEUS) in clinical acute and emergency medicine and critical care (CEUS Acute): Consensus statement of DGIIN, DIVI, DGINA, DGAI, DGK, ÖGUM, SGUM and DEGUM]. Med. Klin. Intensivmed. Notfmed. 2022, 117 (Suppl. S1), 1–23. Erratum in Med. Klin. Intensivmed. Notfmed. 2022, 117, 24. (In German) [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.U.; Eisenbrey, J.R.; Deganello, A.; Zahid, M.; Sharbidre, K.; Sidhu, P.; Robbin, M.L. Microvascular Flow Imaging: A State-of-the-Art Review of Clinical Use and Promise. Radiology 2022, 305, 250–264. [Google Scholar] [CrossRef] [PubMed]
- Ravishankar, S.M.; Tsumura, R.; Hardin, J.W.; Hoffmann, B.; Zhang, Z.; Zhang, H.K. Anatomical Feature-Based Lung Ultrasound Image Quality Assessment Using Deep Convolutional Neural Network. IEEE Int. Ultrason. Symp. 2021, 2021, 9593662. [Google Scholar] [CrossRef]
- Libon, J.; Ng, C.; Bailey, A.; Hareendranathan, A.; Joseph, R.; Dulai, S. Remote diagnostic imaging using artificial intelligence for diagnosing hip dysplasia in infants: Results from a mixed-methods feasibility pilot study. Paediatr. Child. Health. 2023, 28, 285–290. [Google Scholar] [CrossRef]
- Jang, Y.E.; Cho, S.A.; Ji, S.H.; Kim, E.H.; Lee, J.H.; Kim, H.S.; Kim, J.T. Smart Glasses for Radial Arterial Catheterization in Pediatric Patients: A Randomized Clinical Trial. Anesthesiology 2021, 135, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Ultrasound Guidelines: Emergency, Point-of-Care and Clinical Ultrasound Guidelines in Medicine. Ann. Emerg. Med. 2017, 69, e27–e54. [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Resuscitative | Diagnostic | Procedural Guidance | Symptom- or Sign-Based | Therapeutic |
|---|---|---|---|---|
| Core Applications | ||||
| Trauma | ||||
| Intrauterine pregnancy | ||||
| Abdominal aortic aneurysm | ||||
| Cardiac/Hemodynamic assessment | ||||
| Biliary tract | ||||
| Urinary tract | ||||
| Deep vein thrombosis | ||||
| Soft-tissue/Musculoskeletal | ||||
| Thoracic/Airway | ||||
| Ocular | ||||
| Bowel | ||||
| Procedural guidance | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osterwalder, J.; Polyzogopoulou, E.; Hoffmann, B. Point-of-Care Ultrasound—History, Current and Evolving Clinical Concepts in Emergency Medicine. Medicina 2023, 59, 2179. https://doi.org/10.3390/medicina59122179
Osterwalder J, Polyzogopoulou E, Hoffmann B. Point-of-Care Ultrasound—History, Current and Evolving Clinical Concepts in Emergency Medicine. Medicina. 2023; 59(12):2179. https://doi.org/10.3390/medicina59122179
Chicago/Turabian StyleOsterwalder, Joseph, Effie Polyzogopoulou, and Beatrice Hoffmann. 2023. "Point-of-Care Ultrasound—History, Current and Evolving Clinical Concepts in Emergency Medicine" Medicina 59, no. 12: 2179. https://doi.org/10.3390/medicina59122179
APA StyleOsterwalder, J., Polyzogopoulou, E., & Hoffmann, B. (2023). Point-of-Care Ultrasound—History, Current and Evolving Clinical Concepts in Emergency Medicine. Medicina, 59(12), 2179. https://doi.org/10.3390/medicina59122179