

Predictors of Higher Frequency of Atrial Fibrillation in Patients with Cardiac Resynchronization Therapy

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Study Protocol
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Clinical, Electrocardiographic, and Echocardiographic Effects of CRT
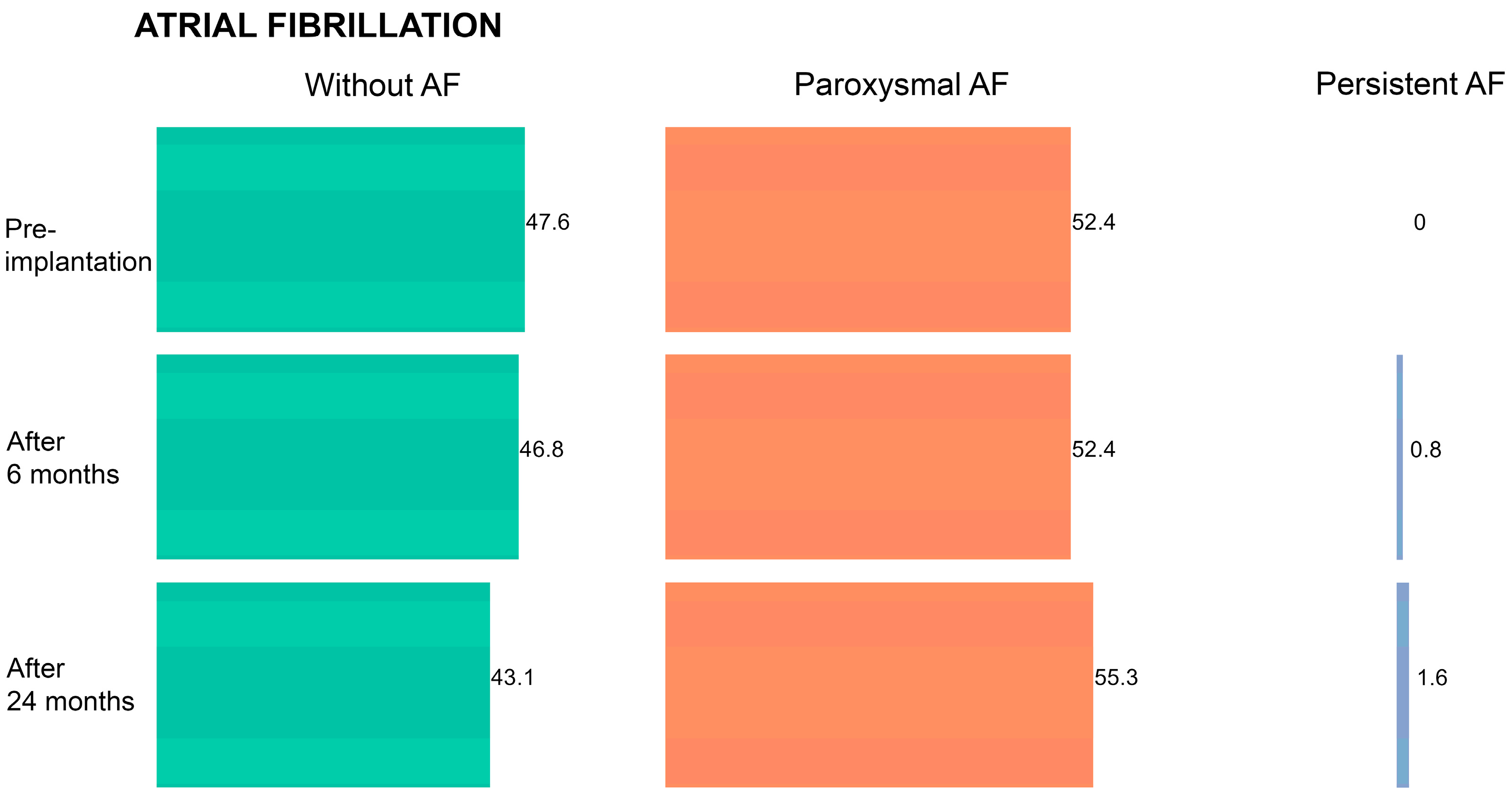
3.3. Atrial Fibrillation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A.J.S. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Res. 2023, 118, 3272–3287. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.G.; Daubert, J.C.; Erdmann, E.; Freemantle, N.; Gras, D.; Kappenberger, L.; Tavazzi, L. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N. Engl. J. Med. 2005, 352, 1539–1549. [Google Scholar] [CrossRef] [PubMed]
- McAlister, F.A.; Ezekowitz, J.; Hooton, N.; Vandermeer, B.; Spooner, C.; Dryden, D.M.; Page, R.L.; Hlatky, M.A.; Rowe, B.H. Cardiac resynchronization therapy for patients with left ventricular systolic dysfunction: A systematic review. JAMA 2007, 297, 2502–2514. [Google Scholar] [CrossRef] [PubMed]
- Cazeau, S.; Leclercq, C.; Lavergne, T.; Walker, S.; Varma, C.; Linde, C.; Garrigue, S.; Kappenberger, L.; Haywood, G.A.; Santini, M.; et al. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N. Engl. J. Med. 2001, 344, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Fisher, W.G.; Smith, A.L.; Delurgio, D.B.; Leon, A.R.; Loh, E.; Kocovic, D.Z.; Packer, M.; Clavell, A.L.; Hayes, D.L.; et al. Cardiac resynchronization in chronic heart failure. N. Engl. J. Med. 2002, 346, 1845–1853. [Google Scholar] [CrossRef] [PubMed]
- Bristow, M.R.; Saxon, L.A.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; DiCarlo, L.; DeMets, D.; White, B.G.; et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N. Engl. J. Med. 2004, 350, 2140–2150. [Google Scholar] [CrossRef]
- Linde, C.; Abraham, W.T.; Gold, M.R.; St John Sutton, M.; Ghio, S.; Daubert, C. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J. Am. Coll. Cardiol. 2008, 52, 1834–1843. [Google Scholar] [CrossRef]
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Klein, H.; Brown, M.W.; Daubert, J.P.; Estes, N.A., III; Foster, E.; Greenberg, H.; Higgins, S.L.; et al. Cardiac-resynchronization therapy for the prevention of heart-failure events. N. Engl. J. Med. 2009, 361, 1329–1338. [Google Scholar] [CrossRef]
- Tang, A.S.; Wells, G.A.; Talajic, M.; Arnold, M.O.; Sheldon, R.; Connolly, S.; Hohnloser, S.H.; Nichol, G.; Birnie, D.H.; Sapp, J.L.; et al. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N. Engl. J. Med. 2010, 363, 2385–2395. [Google Scholar] [CrossRef]
- Lyons, K.J.; Ezekowitz, J.A.; Liang, L.; Heidenreich, P.A.; Yancy, C.W.; DeVore, A.D.; Hernandez, A.F.; Fonarow, G.C. Impact of Current Versus Previous Cardiac Resynchronization Therapy Guidelines on the Proportion of Patients With Heart Failure Eligible for Therapy. JACC Heart Fail. 2017, 5, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Martignani, C.; Massaro, G.; Biffi, M.; Ziacchi, M.; Diemberger, I. Atrial fibrillation: An arrhythmia that makes healthcare systems tremble. J. Med. Econ. 2020, 23, 667–669. [Google Scholar] [CrossRef] [PubMed]
- Wilton, S.B.; Leung, A.A.; Ghali, W.A.; Faris, P.; Exner, D.V. Outcomes of cardiac resynchronization therapy in patients with versus those without atrial fibrillation: A systematic review and meta-analysis. Heart Rhythm. 2011, 8, 1088–1094. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, U.; Atkins, J.; Mina, G.; Dawson, D.; Vanchiere, C.; Duddyala, N.; Jones, R.; Reddy, P.; Dominic, P. Outcomes of cardiac resynchronisation therapy in patients with heart failure with atrial fibrillation: A systematic review and meta-analysis of observational studies. Open Heart 2019, 6, e000937. [Google Scholar] [CrossRef] [PubMed]
- Auricchio, A.; Metra, M.; Gasparini, M.; Lamp, B.; Klersy, C.; Curnis, A.; Fantoni, C.; Gronda, E.; Vogt, J. Long-term survival of patients with heart failure and ventricular conduction delay treated with cardiac resynchronization therapy. Am. J. Cardiol. 2007, 99, 232–238. [Google Scholar] [CrossRef]
- Dickstein, K.; Bogale, N.; Priori, S.; Auricchio, A.; Cleland, J.G.; Gitt, A.; Limbourg, T.; Linde, C.; van Veldhuisen, D.J.; Brugada, J. The European cardiac resynchronization therapy survey. Eur. Heart J. 2009, 30, 2450–2460. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Larson, M.G.; Levy, D.; Vasan, R.S.; Leip, E.P.; Wolf, P.A.; D’Agostino, R.B.; Murabito, J.M.; Kannel, W.B.; Benjamin, E.J. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: The Framingham Heart Study. Circulation 2003, 107, 2920–2925. [Google Scholar] [CrossRef] [PubMed]
- Carlisle, M.A.; Fudim, M.; DeVore, A.D.; Piccini, J.P. Heart Failure and Atrial Fibrillation, Like Fire and Fury. JACC Heart Fail. 2019, 7, 447–456. [Google Scholar] [CrossRef]
- Krijthe, B.P.; Kunst, A.; Benjamin, E.J.; Lip, G.Y.; Franco, O.H.; Hofman, A.; Witteman, J.C.; Stricker, B.H.; Heeringa, J. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur. Heart J. 2013, 34, 2746–2751. [Google Scholar] [CrossRef]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef]
- Maisel, W.H.; Stevenson, L.W. Atrial fibrillation in heart failure: Epidemiology, pathophysiology, and rationale for therapy. Am. J. Cardiol. 2003, 91, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.A.; Cleland, J.; Deharo, J.C.; Delgado, V.; Elliott, P.M.; et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: The Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur. Heart J. 2013, 34, 2281–2329. [Google Scholar] [CrossRef] [PubMed]
- Dickstein, K.; Normand, C.; Auricchio, A.; Bogale, N.; Cleland, J.G.; Gitt, A.K.; Stellbrink, C.; Anker, S.D.; Filippatos, G.; Gasparini, M.; et al. CRT Survey II: A European Society of Cardiology survey of cardiac resynchronisation therapy in 11 088 patients-who is doing what to whom and how? Eur. J. Heart Fail. 2018, 20, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Tolosana, J.M.; Hernandez Madrid, A.; Brugada, J.; Sitges, M.; Garcia Bolao, I.; Fernandez Lozano, I.; Martinez Ferrer, J.; Quesada, A.; Macias, A.; Marin, W.; et al. Comparison of benefits and mortality in cardiac resynchronization therapy in patients with atrial fibrillation versus patients in sinus rhythm (Results of the Spanish Atrial Fibrillation and Resynchronization [SPARE] Study). Am. J. Cardiol. 2008, 102, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Buck, S.; Rienstra, M.; Maass, A.H.; Nieuwland, W.; Van Veldhuisen, D.J.; Van Gelder, I.C. Cardiac resynchronization therapy in patients with heart failure and atrial fibrillation: Importance of new-onset atrial fibrillation and total atrial conduction time. Europace 2008, 10, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Santini, M.; Gasparini, M.; Landolina, M.; Lunati, M.; Proclemer, A.; Padeletti, L.; Catanzariti, D.; Molon, G.; Botto, G.L.; La Rocca, L.; et al. Device-detected atrial tachyarrhythmias predict adverse outcome in real-world patients with implantable biventricular defibrillators. J. Am. Coll. Cardiol. 2011, 57, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Mosterd, A.; Hoes, A.W. Clinical epidemiology of heart failure. Heart 2007, 93, 1137–1146. [Google Scholar] [CrossRef]
- Bosch, L.; Assmann, P.; de Grauw, W.J.C.; Schalk, B.W.M.; Biermans, M.C.J. Heart failure in primary care: Prevalence related to age and comorbidity. Prim. Health Care Res. Dev. 2019, 20, e79. [Google Scholar] [CrossRef]
- Pandey, A.; Omar, W.; Ayers, C.; LaMonte, M.; Klein, L.; Allen, N.B.; Kuller, L.H.; Greenland, P.; Eaton, C.B.; Gottdiener, J.S.; et al. Sex and Race Differences in Lifetime Risk of Heart Failure With Preserved Ejection Fraction and Heart Failure With Reduced Ejection Fraction. Circulation 2018, 137, 1814–1823. [Google Scholar] [CrossRef]
- Chaudhry, M.A. Heart Failure. Curr. Hypertens. Rev. 2019, 15, 7. [Google Scholar] [CrossRef]
- Kutyifa, V.; Kosztin, A.; Klein, H.U.; Biton, Y.; Nagy, V.K.; Solomon, S.D.; McNitt, S.; Zareba, W.; Goldenberg, I.; Roka, A.; et al. Left Ventricular Lead Location and Long-Term Outcomes in Cardiac Resynchronization Therapy Patients. JACC Clin. Electrophysiol. 2018, 4, 1410–1420. [Google Scholar] [CrossRef] [PubMed]
- Katbeh, A.; Van Camp, G.; Barbato, E.; Galderisi, M.; Trimarco, B.; Bartunek, J.; Vanderheyden, M.; Penicka, M. Cardiac Resynchronization Therapy Optimization: A Comprehensive Approach. Cardiology 2019, 142, 116–128. [Google Scholar] [CrossRef]
- Kronborg, M.B.; Johansen, J.B.; Riahi, S.; Petersen, H.H.; Haarbo, J.; Jørgensen, O.D.; Nielsen, J.C. An anterior left ventricular lead position is associated with increased mortality and non-response in cardiac resynchronization therapy. Int. J. Cardiol. 2016, 222, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Ypenburg, C.; van Bommel, R.J.; Borleffs, C.J.; Bleeker, G.B.; Boersma, E.; Schalij, M.J.; Bax, J.J. Long-term prognosis after cardiac resynchronization therapy is related to the extent of left ventricular reverse remodeling at midterm follow-up. J. Am. Coll. Cardiol. 2009, 53, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Daubert, C.; Behar, N.; Martins, R.P.; Mabo, P.; Leclercq, C. Avoiding non-responders to cardiac resynchronization therapy: A practical guide. Eur. Heart J. 2017, 38, 1463–1472. [Google Scholar] [CrossRef]
- Blendea, D.; Singh, J.P. Lead positioning strategies to enhance response to cardiac resynchronization therapy. Heart Fail. Rev. 2011, 16, 291–303. [Google Scholar] [CrossRef]
- Jaffe, L.M.; Morin, D.P. Cardiac resynchronization therapy: History, present status, and future directions. Ochsner J. 2014, 14, 596–607. [Google Scholar]
- Shenkman, H.J.; Pampati, V.; Khandelwal, A.K.; McKinnon, J.; Nori, D.; Kaatz, S.; Sandberg, K.R.; McCullough, P.A. Congestive heart failure and QRS duration: Establishing prognosis study. Chest 2002, 122, 528–534. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, Y.; Zhou, X.; Li, J.; Li, Y.; Zhang, Y.; Xu, G.; Xing, Q.; Lin, S.; Tang, B. QRS duration shortening predicts left ventricular reverse remodelling in patients with dilated cardiomyopathy after cardiac resynchronization therapy. Acta Cardiol. 2015, 70, 307–313. [Google Scholar] [CrossRef]
- van der Bijl, P.; Khidir, M.; Ajmone Marsan, N.; Delgado, V.; Leon, M.B.; Stone, G.W.; Bax, J.J. Effect of Functional Mitral Regurgitation on Outcome in Patients Receiving Cardiac Resynchronization Therapy for Heart Failure. Am. J. Cardiol. 2019, 123, 75–83. [Google Scholar] [CrossRef]
- Yu, C.M.; Fang, F.; Zhang, Q.; Yip, G.W.; Li, C.M.; Chan, J.Y.; Wu, L.; Fung, J.W. Improvement of atrial function and atrial reverse remodeling after cardiac resynchronization therapy for heart failure. J. Am. Coll. Cardiol. 2007, 50, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Valzania, C.; Gadler, F.; Boriani, G.; Rapezzi, C.; Eriksson, M.J. Effect of Cardiac Resynchronization Therapy on Left Atrial Size and Function as Expressed by Speckle Tracking 2-Dimensional Strain. Am. J. Cardiol. 2016, 118, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Badran, H.A.; Abdelhamid, M.A.; Ibrahim, M.T.; Abdelmoteleb, A.M.; Zarif, J.K. Left atrium in cardiac resynchronization therapy: Active participant or innocent bystander. J. Saudi Heart Assoc. 2017, 29, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Inciardi, R.M.; Rossi, A. Left atrium: A forgotten biomarker and a potential target in cardiovascular medicine. J. Cardiovasc. Med. (Hagerstown) 2019, 20, 797–808. [Google Scholar] [CrossRef] [PubMed]
- Nedios, S.; Doering, M.; Darma, A.; Lucas, J.; Dinov, B.; Arya, A.; Dagres, N.; Hindricks, G.; Bollmann, A.; Richter, S.; et al. Predictors of rhythm outcomes after cardiac resynchronization therapy in atrial fibrillation patients: When should we use an atrial lead? Clin. Cardiol. 2021, 44, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Sade, L.E.; Atar, I.; Özin, B.; Yüce, D.; Müderrisoğlu, H. Determinants of New-Onset Atrial Fibrillation in Patients Receiving CRT: Mechanistic Insights From Speckle Tracking Imaging. JACC Cardiovasc. Imaging 2016, 9, 99–111. [Google Scholar] [CrossRef]
- Thamilarasan, M.; Klein, A.L. Factors relating to left atrial enlargement in atrial fibrillation: "chicken or the egg" hypothesis. Am. Heart J. 1999, 137, 381–383. [Google Scholar] [CrossRef]
- Villecco, A.S.; Pilati, G.; Bianchi, G.; Zanardi, L. Left atrial size in paroxysmal atrial fibrillation: Echocardiographic evaluation and follow-up. Cardiology 1992, 80, 89–93. [Google Scholar] [CrossRef]
- Bytyçi, I.; Bajraktari, G.; Lindqvist, P.; Henein, M.Y. Improved Left Atrial Function in CRT Responders: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 298. [Google Scholar] [CrossRef]
- Zhao, L.; Jiang, W.; Zhou, L.; Gu, J.; Wang, Y.; Liu, Y.; Zhang, X.; Wu, S.; Liu, X. The role of valvular regurgitation in catheter ablation outcomes of patients with long-standing persistent atrial fibrillation. Europace 2014, 16, 848–854. [Google Scholar] [CrossRef]
- Butter, C.; Georgi, C.; Stockburger, M. Optimal CRT Implantation-Where and How To Place the Left-Ventricular Lead? Curr. Heart Fail. Rep. 2021, 18, 329–344. [Google Scholar] [CrossRef] [PubMed]
- Behon, A.; Schwertner, W.R.; Merkel, E.D.; Kovács, A.; Lakatos, B.K.; Zima, E.; Gellér, L.; Kutyifa, V.; Kosztin, A.; Merkely, B. Lateral left ventricular lead position is superior to posterior position in long-term outcome of patients who underwent cardiac resynchronization therapy. ESC Heart Fail. 2020, 7, 3374–3382. [Google Scholar] [CrossRef]
- Barold, S.S.; Herweg, B. Cardiac Resynchronization in Patients with Atrial Fibrillation. J. Atr. Fibrillation 2015, 8, 1383. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.K.; Mehta, V.S.; Martic, D.; Sidhu, B.S.; Niederer, S.; Rinaldi, C.A. Atrial fibrillation in cardiac resynchronization therapy. Heart Rhythm. O2 2021, 2, 784–795. [Google Scholar] [CrossRef] [PubMed]
- Nakai, T.; Ikeya, Y.; Kogawa, R.; Okumura, Y. Cardiac resynchronization therapy: Current status and near-future prospects. J. Cardiol. 2022, 79, 352–357. [Google Scholar] [CrossRef]
- Mullens, W.; Auricchio, A.; Martens, P.; Witte, K.; Cowie, M.R.; Delgado, V.; Dickstein, K.; Linde, C.; Vernooy, K.; Leyva, F.; et al. Optimized implementation of cardiac resynchronization therapy: A call for action for referral and optimization of care: A joint position statement from the Heart Failure Association (HFA), European Heart Rhythm Association (EHRA), and European Association of Cardiovascular Imaging (EACVI) of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 2349–2369. [Google Scholar] [CrossRef]
- Nakai, T.; Ikeya, Y.; Kogawa, R.; Otsuka, N.; Wakamatsu, Y.; Kurokawa, S.; Ohkubo, K.; Nagashima, K.; Okumura, Y. What Are the Expectations for Cardiac Resynchronization Therapy? A Validation of Two Response Definitions. J. Clin. Med. 2021, 10, 514. [Google Scholar] [CrossRef]

{kind=link}
| Age, years (x− ± SD) | 63.8 ± 9.1 |
| Sex, N (%) | |
| male | 98 (77.8%) |
| female | 28 (22.2%) |
| CMP, N (%) | |
| nonischemic | 64 (50.8%) |
| ischemic | 49 (38.9%) |
| heart valve disease | 13 (10.3%) |
| Pharmacotherapy N (%) | |
| HF | |
| beta-adrenergic blockers | 109 (86.5%) |
| ACE-I/ARB/ARNI | 114 (90.5%) |
| MRA | 97 (77.0%) |
| AF | |
| Amiodarone | 37 (29.4%) |
| OAC/NOAC | 74 (58.7%) |
| CS lead position, N (%) lateral anterior posterolateral | 61 (48.4%) 8 (6.3%) 57 (45.2%) |
| Response to CRT, N (%) R nonR | 100 (79.4%) 26 (20.6%) | |
| Ventricular pacing, % (x− ± SD) | ||
| Total | 96.4 ± 3.5 | |
| R | 96.65 ± 3.33 | p = 0.098 |
| nonR | 95.30 ± 4.09 |
| Pre-Implantation | 6 Months | 24 Months | p Overall | p Pre-Implant. vs 6 m | p Pre-Implant. vs 24 m | p 6 m–24 m | |
|---|---|---|---|---|---|---|---|
| NYHA, N (%) I II | |||||||
| 0 (0.0%) | 3 (2.4%) | 39 (31.7%) | |||||
| 16 (12.7%) | 116 (93.5%) | 83 (67.5%) | <0.001 | <0.001 | <0.001 | 0.014 | |
| III | 110 (87.3%) | 5 (4.0%) | 1 (0.8%) | ||||
| Diuretic, N (%) | |||||||
| thiazide | 0 (0.0%) | 3 (2.4%) | 58 (47.2%) | ||||
| furosemide | |||||||
| 40 mg | 79 (62.7%) | 99 (79.8%) | 57 (46.3%) | <0.001 | 0.005 | <0.001 | <0.001 |
| 80 mg | 23 (18.3%) | 20 (16.1%) | 7 (5.7%) | ||||
| 250 mg | 21 (16.7%) | 2 (1.6%) | 1 (0.8%) | ||||
| 500 mg | 3 (2.4%) | 0 (0.0%) | 0 (0.0%) | ||||
| QRS msec (x− ± SD) | 167.6 ± 14.3 | 135.5 ± 10.4 | 131.7 ± 11.7 | <0.001 | <0.001 | <0.001 | <0.001 |
| EDD mm (x− ± SD) | 66.1 ± 7.1 | 64.3 ± 6.7 | 62.2 ± 7.4 | <0.001 | <0.001 | <0.001 | <0.001 |
| ESD mm (x− ± SD) | 51.2 ± 8.0 | 49.6 ± 7.8 | 47.7 ± 7.6 | <0.001 | <0.001 | <0.001 | <0.001 |
| LVEF % (x− ± SD) | 20.6 ± 6.9 | 24.9 ± 7.8 | 32.9 ± 9.3 | <0.001 | <0.001 | <0.001 | <0.001 |
| LA mm (x− ± SD) | 44.8 ± 4.7 | 45.0 ± 4.7 | 45.3 ± 5.0 | 0.070 | |||
| MR, N (%) | |||||||
| 1 | 50 (39.7%) | 94 (75.8%) | 103 (83.7%) | ||||
| 2 | 55 (43.7%) | 29 (23.4%) | 19 (15.4%) | <0.001 | <0.001 | <0.001 | <0.001 |
| 3 | 21 (16.7%) | 1 (0.8%) | 1 (0.8%) |
| Group | Pre-Implantation | 6 Months | 24 Months | p-Value Overall | |
|---|---|---|---|---|---|
| NYHA, N (%) I II III | R | 0 (0.0%) 10 (10.0%) 90 (90.0%) | 3 (3.0%) 94 (94.0%) 3 (3.0%) | 37 (37.0%) 63 (63.0%) 0 (0.0%) | <0.001 |
| nonR | 0 (0.0%) 6 (23.1%) 20 (76.9%) | 0 (0.0%) 22 (91.7%) 2 (8.3%) | 2 (8.7%) 20 (87.0%) 1 (4.3%) | <0.001 | |
| p-value * | 0.076 | 0.150 | 0.004 | ||
| Diuretic. N (%) thiazide furosemide 40 mg furosemide 80 mg furosemide 250 mg furosemide 500 mg | R | 0 (0.0%) 67 (67.0%) 18 (18.0%) 13 (13.0%) 2 (2.0%) | 1 (1.0%) 84 (84.0%) 14 (14.0%) 1 (1.0%) 0 (0.0%) | 53 (53.0%) 43 (43.0%) 3 (3.0%) 1 (1.0%) 0 (0.0%) | <0.001 |
| nonR | 0 (0.0%) 12 (46.2%) 5 (19.2%) 8 (30.8%) 1 (3.8%) | 2 (8.3%) 15 (62.5%) 6 (25.0%) 1 (4.2%) 0 (0.0%) | 5 (21.7%) 14 (60.9%) 4 (17.4%) 0 (0.0%) 0 (0.0%) | <0.001 | |
| p-value * | 0.029 | 0.377 | 0.003 | ||
| QRS msec (x− ± SD) | R | 167.2 ± 14.1 | 135.4 ± 10.3 | 131.3 ± 11.7 | <0.001 |
| nonR | 169.1 ± 15.3 | 136.1 ± 11.2 | 133.5 ± 11.9 | <0.001 | |
| p-value * | 0.562 | 0.777 | 0.424 | ||
| EDD mm (x− ± SD) | R | 66.3 ± 7.2 | 64.3 ± 6.8 | 61.7 ± 7.3 | <0.001 |
| nonR | 65.4 ± 6.8 | 64.5 ± 6.8 | 64.2 ± 7.4 | 0.101 | |
| p-value * | 0.557 | 0.887 | 0.072 | ||
| ESD mm (x− ± SD) | R | 51.3 ± 8.0 | 49.6 ± 7.7 | 47.4 ± 7.3 | <0.001 |
| nonR | 50.7 ± 8.3 | 49.7 ± 8.1 | 49.0 ± 8.7 | 0.058 | |
| p-value * | 0.762 | 0.995 | 0.372 | ||
| LVEF % (x− ± SD) | R | 20.7 ± 6.6 | 25.8 ± 7.4 | 35.0 ± 8.2 | <0.001 |
| nonR | 20.4 ± 8.5 | 21.3 ± 8.7 | 23.7 ± 8.4 | <0.001 | |
| p-value * | 0.910 | 0.013 | <0.001 | ||
| LA mm (x− ± SD) | R | 44.5 ± 4.8 | 44.6 ± 4.8 | 44.8 ± 5.0 | 0.346 |
| nonR | 45.9 ± 3.8 | 46.3 ± 4.0 | 47.3 ± 4.7 | 0.022 | |
| p-value * | 0.197 | 0.123 | 0.017 | ||
| MR. N (%) 1 2 3 | R | 39 (39.0%) 43 (43.0%) 18 (18.0%) | 79 (79.0%) 21 (21.0%) 0 (0.0%) | 86 (86.0%) 14 (14.0%) 0 (0.0%) | <0.001 |
| nonR | 11 (42.3%) 12 (46.2%) 3 (11.5%) | 15 (62.5%) 8 (33.3%) 1 (4.2%) | 17 (73.9%) 5 (21.7%) 1 (4.3%) | <0.001 | |
| p-value * | 0.572 | 0.076 | 0.139 |
| Group | Pre-Implantation | 6 Months | 24 Months | p-Value Overall | |
|---|---|---|---|---|---|
| Atrial fibrillation N (%) | R | 45 (45.0%) | 46 (46.0%) | 50 (50.0%) | <0.001 |
| nonR | 21 (80.8%) | 20 (83.3%) | 20 (87.0%) | <0.001 | |
| p-value * | 0.001 | 0.001 | 0.001 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| B | p | B | p | |
| Age | 0.099 | 0.401 | ||
| Sex (male vs. female) | 24.360 | <0.001 | 2.263 | 0.061 |
| Response to CRT (non-responder/responder) | 25.683 | <0.001 | 8.134 | <0.001 |
| Ventricular pacing | −1.674 | <0.001 | −0.366 | 0.277 |
| CMP non-ischemic ischemic heart valve disease | ||||
| ref 23.979 24.472 | <0.001 <0.001 | 2.194 2.633 | 0.194 0.425 | |
| CS lead position lateral anterior posterolateral | ref 24.261 25.143 | <0.001 <0.001 | 1.650 5.159 | 0.566 0.005 |
| NYHA | 2.481 | <0.001 | ||
| Diuretic | 1.581 | 0.154 | ||
| QRS | 0.050 | 0.248 | ||
| EDD | 0.167 | <0.001 | 0.069 | 0.497 |
| ESD | 0.082 | 0.386 | ||
| LA | 3.001 | 0.005 | 0.813 | <0.001 |
| MR | 1.175 | <0.001 | 0.887 | 0.313 |
| LVEF | −0.030 | 0.703 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grbović, A.; Pavlović, S.; Žugić, V. Predictors of Higher Frequency of Atrial Fibrillation in Patients with Cardiac Resynchronization Therapy. Medicina 2023, 59, 2178. https://doi.org/10.3390/medicina59122178
Grbović A, Pavlović S, Žugić V. Predictors of Higher Frequency of Atrial Fibrillation in Patients with Cardiac Resynchronization Therapy. Medicina. 2023; 59(12):2178. https://doi.org/10.3390/medicina59122178
Chicago/Turabian StyleGrbović, Aleksandra, Siniša Pavlović, and Vasko Žugić. 2023. "Predictors of Higher Frequency of Atrial Fibrillation in Patients with Cardiac Resynchronization Therapy" Medicina 59, no. 12: 2178. https://doi.org/10.3390/medicina59122178
APA StyleGrbović, A., Pavlović, S., & Žugić, V. (2023). Predictors of Higher Frequency of Atrial Fibrillation in Patients with Cardiac Resynchronization Therapy. Medicina, 59(12), 2178. https://doi.org/10.3390/medicina59122178