
A Randomized Controlled Trial of Vertebral Body Decompression Procedure Versus Conservative Treatment for Painful Vertebral Compression Fracture




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Efficacy Evaluation
2.3. Study Treatment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, L.D. Fractures of the osteoporotic spine. Orthop. Clin. N. Am. 1990, 21, 143–150. [Google Scholar] [CrossRef]
- Farrokhi, M.R.; Alibai, E.; Maghami, Z. Randomized controlled trial of percutaneous vertebroplasty versus optimal medical management for the relief of pain and disability in acute osteoporotic vertebral compression fractures. J. Neurosurg. Spine 2011, 14, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.D.; Kim, E.H.; Lee, J.C.; Choi, S.W.; Kim, H.S.; Cha, J.S.; Shin, B.J. Management of Osteoporotic Vertebral Fracture: Review Update 2022. Asian Spine J. 2022, 16, 934–946. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.J.; Moon, S.H.; Lee, J.H.; Lee, J.H. Association between Osteoporotic Vertebral Compression Fractures and Age, Bone Mineral Density, and European Quality of Life-5 Dimensions in Korean Postmenopausal Women: A Nationwide Cross-sectional Observational Study. Clin. Orthop. Surg. 2021, 13, 207–215. [Google Scholar] [CrossRef]
- Alexandru, D.; So, W. Evaluation and management of vertebral compression fractures. Perm. J. 2012, 16, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Prather, H.; Hunt, D.; Watson, J.O.; Gilula, L.A. Conservative care for patients with osteoporotic vertebral compression fractures. Phys. Med. Rehabil. Clin. N. Am. 2007, 18, 577–591. [Google Scholar] [CrossRef]
- Cho, S.T.; Kim, S.J.; Nam, B.J.; Kim, K.W.; Lee, G.H.; Kim, J.H. Absolute Bed Rest Duration of 3 Days for Osteoporotic Vertebral Fractures: A Retrospective Study. Asian Spine J. 2022, 16, 898–905. [Google Scholar] [CrossRef]
- Park, S.M.; Park, C.; Kim, H.; Kim, H.J.; Yeom, J.S.; Lee, C.K.; Chang, B.S. Is Redo Vertebroplasty an Effective Treatment on the Same Vertebra? CardioVascular Interv. Radiol. 2018, 41, 1058–1066. [Google Scholar] [CrossRef]
- Park, S.M.; Park, J.W.; Kim, H.; Kim, H.J.; Yeom, J.S.; Lee, C.K.; Chang, B.S. Morphological changes of vertebral compression fracture with intra-vertebral cleft treated with percutaneous vertebroplasty. J. Orthop. Sci. 2018, 23, 237–247. [Google Scholar] [CrossRef]
- Arnoldi, C.C. Intraosseous hypertension. A possible cause of low back pain? Clin. Orthop. Relat. Res. 1976, 30–34. [Google Scholar]
- Lemperg, R.K.; Arnoldi, C.C. The significance of intraosseous pressure in normal and diseased states with special reference to the intraosseous engorgement-pain syndrome. Clin. Orthop. Relat. Res. 1978, 136, 143–156. [Google Scholar]
- Yeh, M.L.; Heggeness, M.H.; Chen, H.H.; Jassawalla, J.; Luo, Z.P. Compressive loading at the end plate directly regulates flow and deformation of the basivertebral vein: An analytical study. J. Orthop. Surg. Res. 2006, 1, 18. [Google Scholar] [CrossRef]
- Choi, J.Y.; Park, S.M.; Kim, H.J.; Yeom, J.S. Recent Updates on Minimally Invasive Spine Surgery: Techniques, Technologies, and Indications. Asian Spine J. 2022, 16, 1013–1021. [Google Scholar] [CrossRef]
- Pierce, T.P.; Jauregui, J.J.; Elmallah, R.K.; Lavernia, C.J.; Mont, M.A.; Nace, J. A current review of core decompression in the treatment of osteonecrosis of the femoral head. Curr. Rev. Musculoskelet. Med. 2015, 8, 228–232. [Google Scholar] [CrossRef]
- Kim, G.U.; Park, W.T.; Chang, M.C.; Lee, G.W. Diagnostic Technology for Spine Pathology. Asian Spine J. 2022, 16, 764–775. [Google Scholar] [CrossRef]
- Hua, K.C.; Yang, X.G.; Feng, J.T.; Wang, F.; Yang, L.; Zhang, H.; Hu, Y.C. The efficacy and safety of core decompression for the treatment of femoral head necrosis: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2019, 14, 306. [Google Scholar] [CrossRef] [PubMed]
- Mont, M.A.; Jones, L.C.; Hungerford, D.S. Nontraumatic osteonecrosis of the femoral head: Ten years later. J. Bone Joint Surg. Am. 2006, 88, 1117–1132. [Google Scholar]
- Mont, M.A.; Ragland, P.S.; Etienne, G. Core decompression of the femoral head for osteonecrosis using percutaneous multiple small-diameter drilling. Clin. Orthop. Relat. Res. 2004, 429, 131–138. [Google Scholar] [CrossRef]
- Zhang, H.J.; Liu, Y.W.; Du, Z.Q.; Guo, H.; Fan, K.J.; Liang, G.H.; Liu, X.C. Therapeutic effect of minimally invasive decompression combined with impaction bone grafting on osteonecrosis of the femoral head. Eur. J. Orthop. Surg. Traumatol. 2013, 23, 913–919. [Google Scholar] [CrossRef]
- Arnoldi, C.C. Intravertebral pressures in patients with lumbar pain. A preliminary communication. Acta Orthop. Scand. 1972, 43, 109–117. [Google Scholar] [CrossRef]
- Esses, S.I.; Moro, J.K. Intraosseous vertebral body pressures. Spine 1992, 17, S155–S159. [Google Scholar] [CrossRef] [PubMed]
- Ochia, R.S.; Ching, R.P. Internal pressure measurements during burst fracture formation in human lumbar vertebrae. Spine 2002, 27, 1160–1167. [Google Scholar] [CrossRef]
- Arnoldi, C.C.; Linderholm, H.; Mussbichler, H. Venous engorgement and intraosseous hypertension in osteoarthritis of the hip. J. Bone Joint Surg. Br. 1972, 54, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Lyles, K.W.; Gold, D.T.; Shipp, K.M.; Pieper, C.F.; Martinez, S.; Mulhausen, P.L. Association of osteoporotic vertebral compression fractures with impaired functional status. Am. J. Med. 1993, 94, 595–601. [Google Scholar] [CrossRef]
- Kendler, D.L.; Bauer, D.C.; Davison, K.S.; Dian, L.; Hanley, D.A.; Harris, S.T.; McClung, M.; Miller, P.; Schousboe, J.; Yuen, C.; et al. Vertebral Fractures: Clinical Importance and Management. Am. J. Med. 2016, 129, 221.e1–221.e10. [Google Scholar] [CrossRef]
- Ogihara, M. Core decompression of vertebral body for osteoporotic vertebral compression fracture. Pain Clinic 2006, 27, 898–903. [Google Scholar]
- Yokoyama, K.; Kawanishi, M.; Yamada, M.; Tanaka, H.; Ito, Y.; Hirano, M.; Kuroiwa, T. Comparative study of percutaneous vertebral body perforation and vertebroplasty for the treatment of painful vertebral compression fractures. AJNR Am. J. Neuroradiol. 2012, 33, 685–689. [Google Scholar] [CrossRef]
- Klazen, C.A.; Lohle, P.N.; de Vries, J.; Jansen, F.H.; Tielbeek, A.V.; Blonk, M.C.; Venmans, A.; van Rooij, W.J.J.; Schoemaker, M.C.; Juttmann, J.R.; et al. Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): An open-label randomised trial. Lancet 2010, 376, 1085–1092. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Core Decompression Group n = 48 | Conservative Group n = 50 | |
|---|---|---|
| Age (year) | 76.3 ± 6.7 | 79.9 ± 6.6 |
| Female sex—No. | 35 (72.9%) | 38 (76%) |
| Height (cm) | 156.0 ± 7.0 | 154.6 ± 8.2 |
| Weight (kg) | 60.8 ± 11.2 | 54.9 ± 8.5 |
| BMI a | 24.9 ± 4.0 | 23.0 ± 3.0 |
| Vitamin D (ng/mL) | 21.43 ± 12.30 | 22.40 ± 10.96 |
| No. of fractured vertebral bodies—mean | 1.02 | 1.06 |
| One—no. | 47 | 47 |
| Two—no. | 1 | 3 |
| Vertebral level | ||
| T10–T12 | 15 (30.0%) | 18 (34.0%) |
| L1–L2 | 24 (48%) | 28 (52.8%) |
| L3–L5 | 11 (22.0%) | 7 (13.2%) |
| Initial pain management | ||
| 0–1 (no prescription~non-opioid analgesics) | 17 | 21 |
| 2–3 (opioid analgesics) | 31 | 29 |
| Comorbidities influencing pain perception | 4 (8.3%) | 4 (8.0%) |
| Concomitant medication | ||
| Steroid usage | 0 | 0 |
| Medications influencing pain perception | 3 (6.2%) | 4 (8.0%) |
| VAS b score | 77.9 ± 16.4 | 74.1 ± 20.3 |
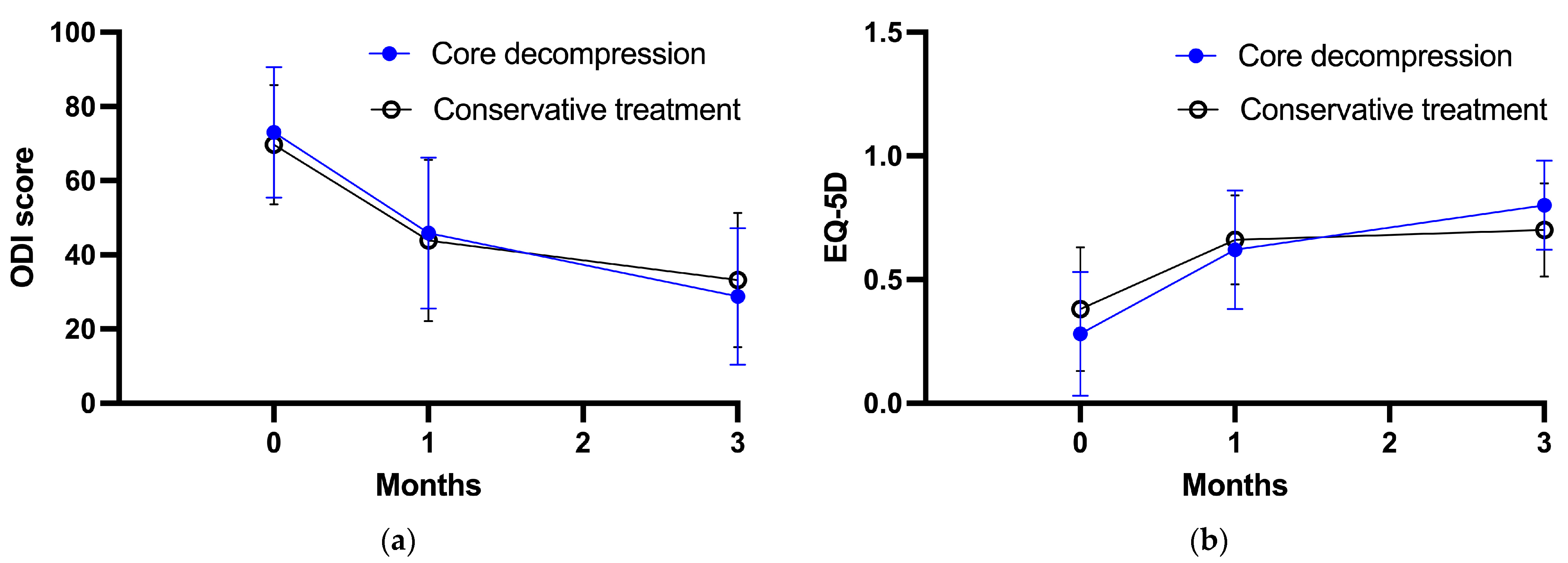
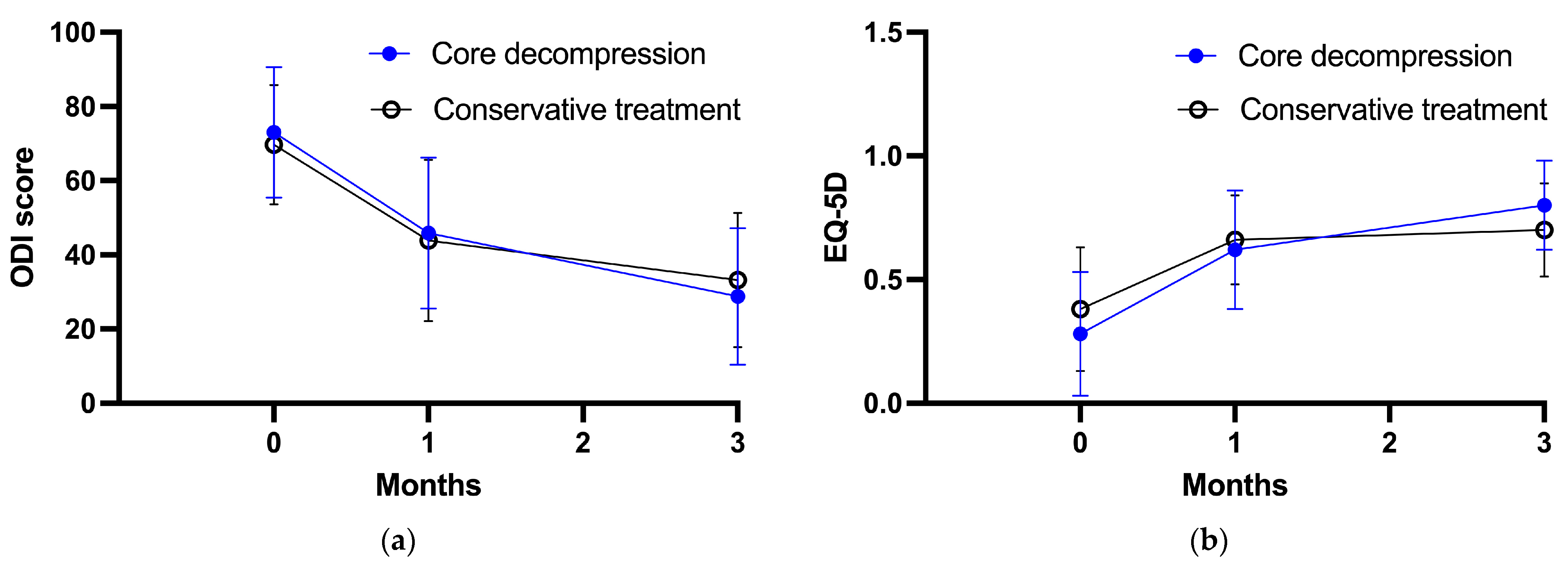
| ODI c score | 72.8 ± 17.8 | 70.1 ± 15.9 |
| EQ-5D d score | 0.30 ± 0.25 | 0.37 ± 0.26 |
| Core Decompression Group | Conservative Treatment Group | Treatment Effect (95% CI) * | p-Value | |
|---|---|---|---|---|
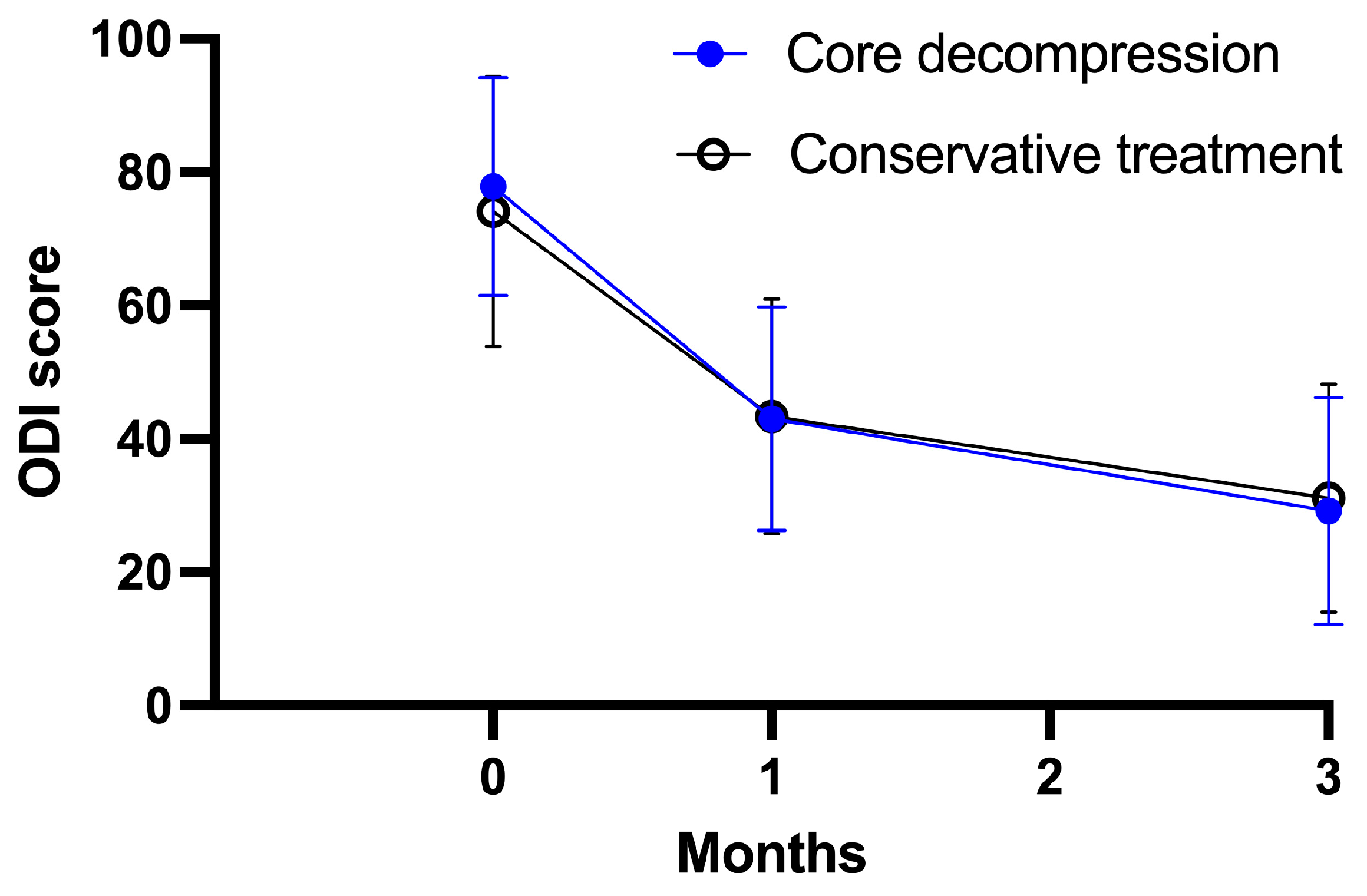
| VAS | ||||
| At baseline | 77.9 ± 16.4 | 74.1 ± 20.3 | ||
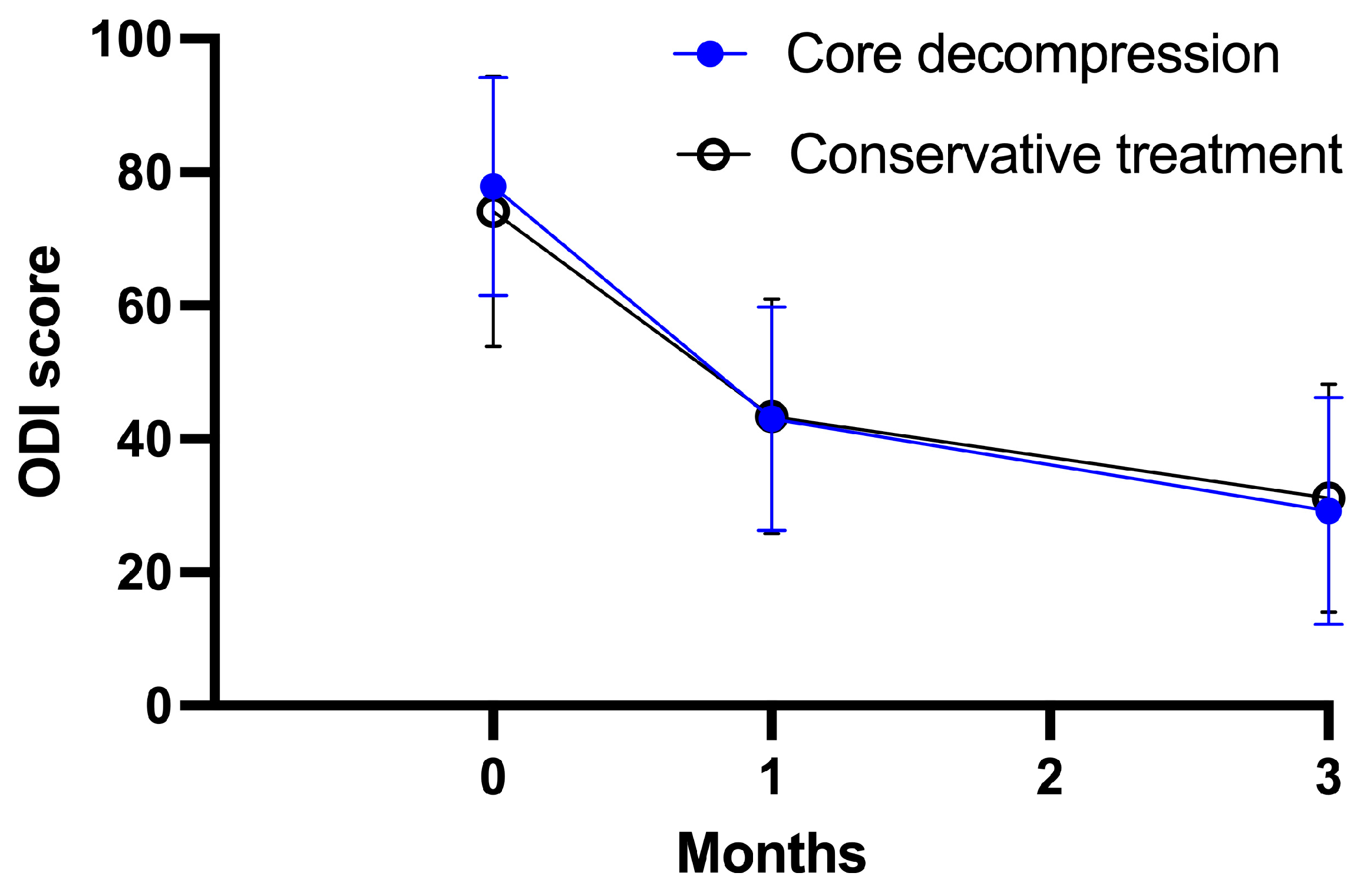
| At 1 month | 43.0 ± 16.8 | 43.4 ± 17.6 | −0.1 (−7.5 to 7.3) | 0.970 |
| At 3 months | 29.2 ± 17.0 | 31.1 ± 17.1 | 2.0 (−5.6 to 9.6) | 0.601 |
| Core Decompression Group | Conservative Group | p-Value | |
|---|---|---|---|
| Compression rate (%) | 0.560 | ||
| At baseline | 28.4 ± 18.4 | 28.8 ± 21.0 | |
| At 3 months | 42.2 ± 22.8 | 33.6 ± 26.0 | |
| Wedge angle (degrees) | 0.753 | ||
| At baseline | 12.2 ± 7.5 | 13.0 ± 7.1 | |
| At 3 months | 15.8 ± 9.0 | 14.0 ± 7.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Zheng, H.; Park, S.-M.; Kim, H.-J.; Yeom, J.S. A Randomized Controlled Trial of Vertebral Body Decompression Procedure Versus Conservative Treatment for Painful Vertebral Compression Fracture. Medicina 2023, 59, 1848. https://doi.org/10.3390/medicina59101848
Lee S, Zheng H, Park S-M, Kim H-J, Yeom JS. A Randomized Controlled Trial of Vertebral Body Decompression Procedure Versus Conservative Treatment for Painful Vertebral Compression Fracture. Medicina. 2023; 59(10):1848. https://doi.org/10.3390/medicina59101848
Chicago/Turabian StyleLee, Sanghoon, Haolin Zheng, Sang-Min Park, Ho-Joong Kim, and Jin S. Yeom. 2023. "A Randomized Controlled Trial of Vertebral Body Decompression Procedure Versus Conservative Treatment for Painful Vertebral Compression Fracture" Medicina 59, no. 10: 1848. https://doi.org/10.3390/medicina59101848
APA StyleLee, S., Zheng, H., Park, S.-M., Kim, H.-J., & Yeom, J. S. (2023). A Randomized Controlled Trial of Vertebral Body Decompression Procedure Versus Conservative Treatment for Painful Vertebral Compression Fracture. Medicina, 59(10), 1848. https://doi.org/10.3390/medicina59101848