

Is the Surface Anatomy of the Popliteal Crease Related to Lower Extremity Alignment or Knee Osseous Morphology? A Radiographic Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
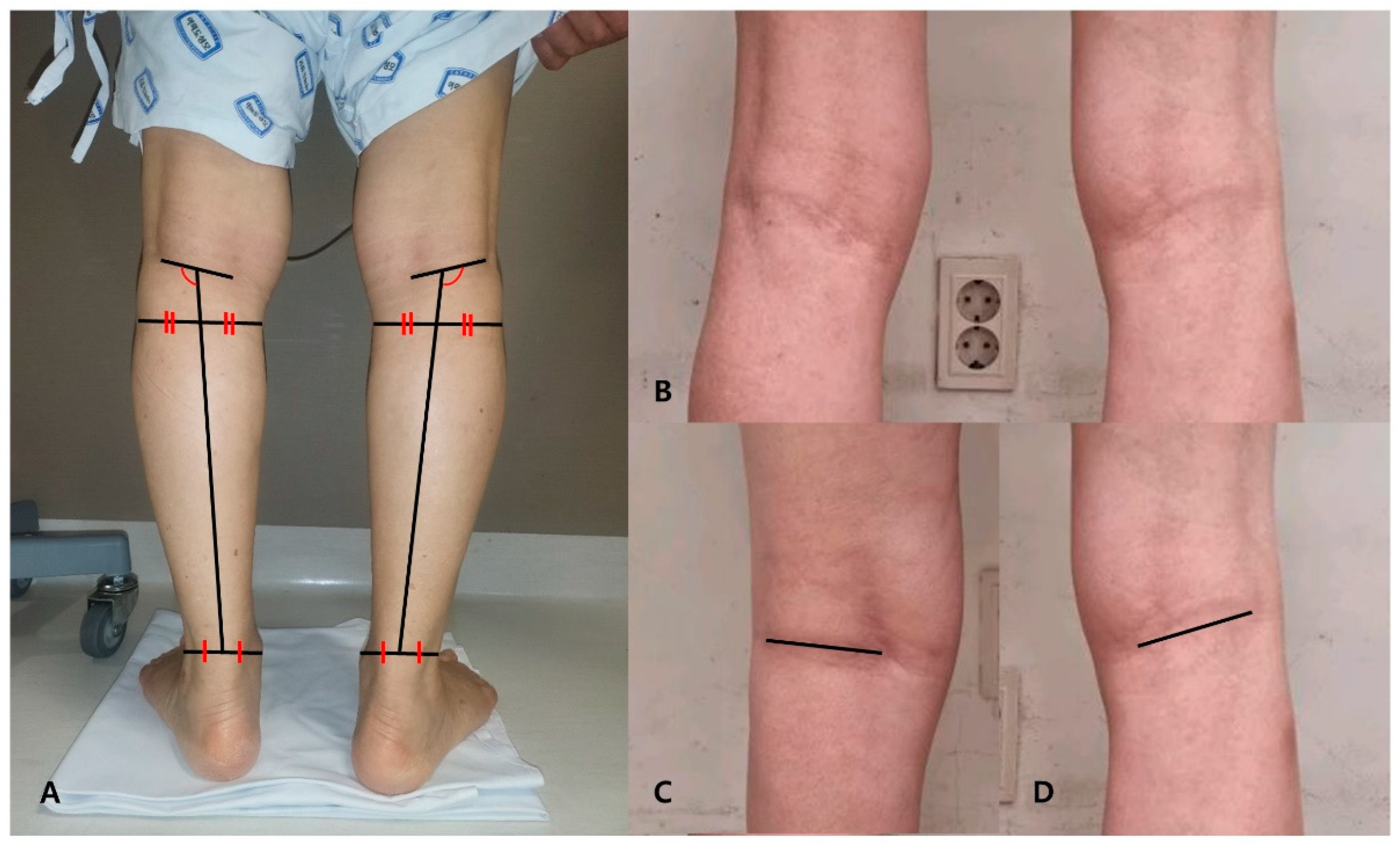
2.2. Popliteal Crease Obliquity Measurement
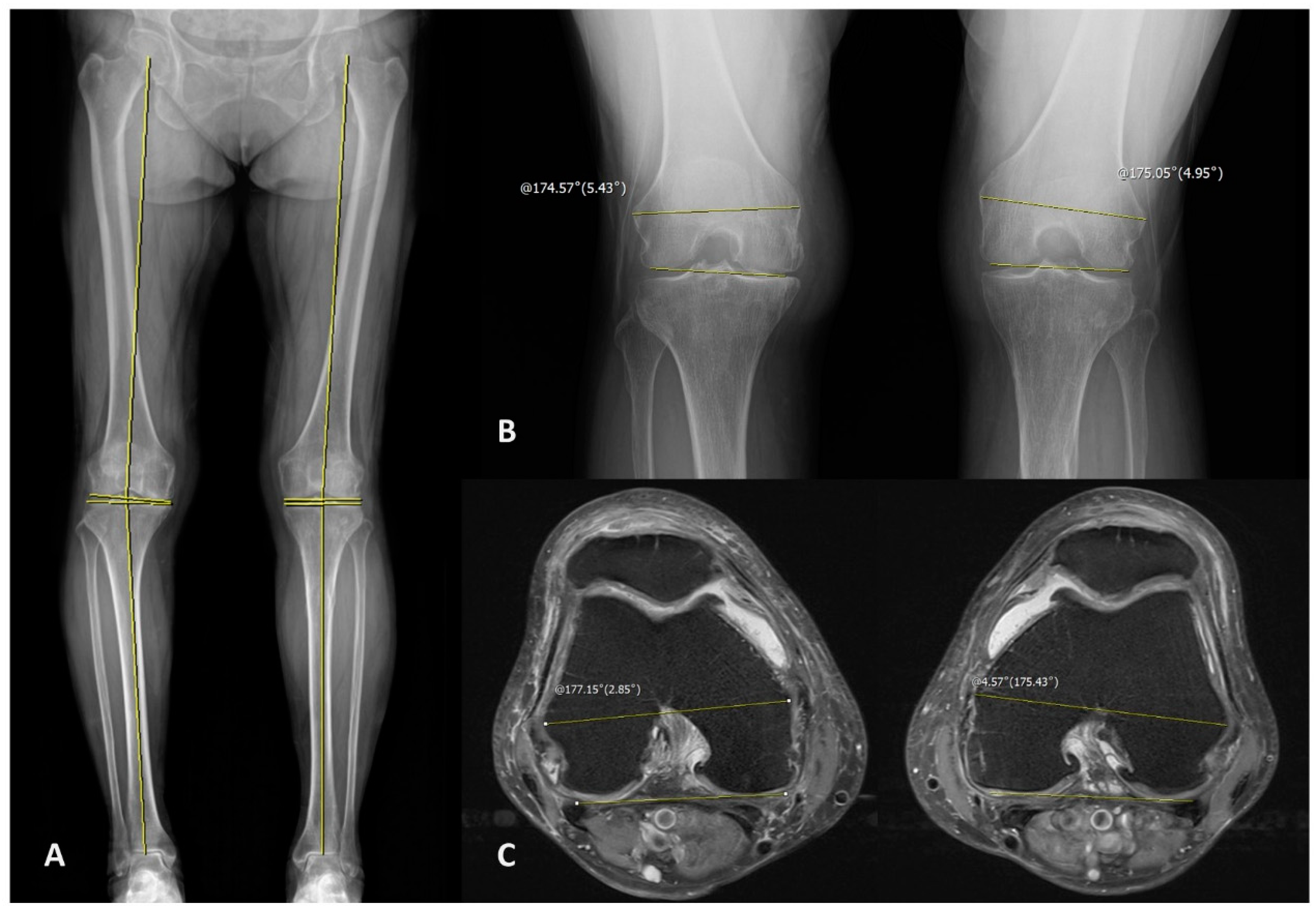
2.3. Radiologic Measurement
2.4. Reliability & Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Kimura, S.; Kitagawa, T. Embryological development of human palmar, plantar, and digital flexion creases. Anat. Rec. 1986, 216, 191–197. [Google Scholar] [CrossRef]
- Bugbee, W.D.; Botte, M.J. Surface Anatomy of the Hand: The Relationships Between Palmar Skin Creases and Osseous Anatomy. Clin. Orthop. Relat. Res. 1993, 296, 122–126. [Google Scholar] [CrossRef]
- Wilhelmi, B.J.; Snyder IV, N.; Verbesey, J.E.; Ganchi, P.A.; Lee, W.A. Trigger finger release with hand surface landmark ratios: An anatomic and clinical study. Plast. Reconstr. Surg. 2001, 108, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.-T.; Lee, H.-J.; Kim, T.-G.; Jeon, I.-H. Current approaches for carpal tunnel syndrome. Clin. Orthop. Surg. 2014, 6, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, P.; Kalra, S.; Jain, S.; Munjal, S.; Anurag, A. Relationship between palmar skin creases and osseous anatomy-a radiological study identification. J. Morphol. Sci. 2017, 28, 184–188. [Google Scholar]
- Belay, D.G.; Worku, M.G.; Dessie, M.A.; Asmare, Y.; Taye, M. Prevalence of palmar crease patterns and associated factors among students at University of Gondar, Northwest Ethiopia. Anat. Cell Biol. 2022, 55, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Itamura, J.M.; Papadakis, S.A.; Vaishnav, S.; Gurmet, R. The relationship between main elbow flexion skin crease and osseous anatomy of the elbow joint. Surg. Radiol. Anat. 2009, 31, 55–58. [Google Scholar] [CrossRef]
- Shrestha, U.; Lama Moktan, S.; Shrestha, S.B. Ultrasonographic Assessment of the Distance of Sciatic Nerve Bifurcation from the Popliteal Crease and its Depth from Skin in Volunteers. Kathmandu Univ. Med. J. (KUMJ) 2020, 18, 176–180. [Google Scholar] [CrossRef]
- Vloka, J.D.; Hadžic, A.; April, E.; Thys, D.M. The division of the sciatic nerve in the popliteal fossa: Anatomical implications for popliteal nerve blockade. Anesth. Analg. 2001, 92, 215–217. [Google Scholar] [CrossRef]
- Samet, R.E.; Dorsey, N.; Sappenfield, J.W.; Gold, A.K.; Hsiao, E.J.; Bentzen, S.M.; Bigeleisen, P.E. The influence of patient position on ultrasound examination of the sciatic nerve in the popliteal fossa: A cross-sectional study. Australas. J. Ultrasound Med. 2023, 26, 142–149. [Google Scholar] [CrossRef]
- Fan, J.; Huang, R.; Yang, J.; Zhang, T.; Zeng, Y.; Su, Z. Medial gastrocnemius resection for calf reduction by using a popliteal mini-incisional approach in Asians. J. Plast. Reconstr. Aesthetic. Surg. 2022, 75, 3568–3573. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-López, C.; Garlito-Díaz, H.; Madroñero-Mariscal, R.; Sánchez-Cervilla, P.J.; Graciani, A.; López-Sendón, J.L.; López-de-Sá, E. Earlobe crease shapes and cardiovascular events. Am. J. Cardiol. 2015, 116, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.; Malayko, G.; Pagliaro, T.; Journeaux, S. Elbow to digit measurements as a preoperative adjunct tool to aid intramedullary femoral nail selection–the rule of thumb. Injury 2023, 54, 683–686. [Google Scholar] [CrossRef] [PubMed]
- Moreland, J.R.; Bassett, L.W.; Hanker, G.J. Radiographic analysis of the axial alignment of the lower extremity. J. Bone Jt. Surg. 1987, 69, 745–749. [Google Scholar] [CrossRef]
- Rosenberg, T.D.; Paulos, L.E.; Parker, R.D.; Coward, D.B.; Scott, S.M. The forty-five-degree posteroanterior flexion weight-bearing radiograph of the knee. J. Bone Jt. Surg. 1988, 70, 1479–1483. [Google Scholar] [CrossRef]
- Zampogna, B.; Vasta, S.; Amendola, A.; Marbach, B.U.-E.; Gao, Y.; Papalia, R.; Denaro, V. Assessing lower limb alignment: Comparison of standard knee xray vs long leg view. Iowa Orthop. J. 2015, 35, 49. [Google Scholar]
- Sharma, L.; Song, J.; Felson, D.T.; Cahue, S.; Shamiyeh, E.; Dunlop, D.D. The role of knee alignment in disease progression and functional decline in knee osteoarthritis. JAMA 2001, 286, 188–195. [Google Scholar] [CrossRef]
- Hsu, R.W.W.; Himeno, S.; Coventry, M.B.; Chao, E.Y.S. Normal Axial Alignment of the Lower Extremity and Load-Bearing Distribution at the Knee. Clin. Orthop. Relat. Res. 1990, 255, 215–227. [Google Scholar] [CrossRef]
- Colyn, W.; Cleymans, A.; Bruckers, L.; Houben, R.; Smeets, K.; Bellemans, J. The lateral joint line opening: A radiographic indicative parameter for high grade varus knees. J. Exp. Orthop. 2022, 9, 51. [Google Scholar] [CrossRef]
- Kodama, Y.; Furumatsu, T.; Kamatsuki, Y.; Hiranaka, T.; Takahata, T.; Sadakane, M.; Ikuta, H.; Yasumitsu, M.; Ozaki, T. Preliminary diagnosis of medial meniscus posterior root tears using the Rosenberg radiographic view. Knee Surg. Relat. Res. 2019, 31, 9. [Google Scholar] [CrossRef]
- Babatunde, O.M.; Danoff, J.R.; Patrick, D.A., Jr.; Lee, J.H.; Kazam, J.K.; Macaulay, W. The Combination of the Tunnel View and Weight-Bearing Anteroposterior Radiographs Improves the Detection of Knee Arthritis. Arthritis 2016, 2016, 9786924. [Google Scholar] [CrossRef] [PubMed]
- Kanekasu, K.; Kondo, M.; Kadoya, Y. Axial radiography of the distal femur to assess rotational alignment in total knee arthroplasty. Clin. Orthop. Relat. Res. 2005, 434, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, S.; Miura, H.; Nagamine, R.; Mawatari, T.; Tokunaga, M.; Nabeyama, R.; Iwamoto, Y. Anatomical analysis of the femoral condyle in normal and osteoarthritic knees. J. Orthop. Res. 2004, 22, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.H.; Koh, Y.G.; Kim, P.S.; Park, J.H.; Kang, K.T. Effect of the presence of the articular cartilage on the femoral component rotation in total knee arthroplasty in female and varus osteoarthritis knees. J. Orthop. Surg. Res. 2020, 15, 499. [Google Scholar] [CrossRef]
- Konijn, L.; Van der Steenhoven, T.; van der Heide, H.; de Ruiter, M.; Nelissen, R. The inter-and intraindividual anatomical relationship of the femoral anteversion and distal femoral rotation. a cadaveric study on the femoral anteversion angle, posterior and inferior condylar angle using computed tomography. Adv. Comput. Tomogr. 2015, 4, 9. [Google Scholar]
- Kato, T.; Motoyama, M.; Adachi, N.; Deie, M. Cartilage assessment using preoperative planning MRI for femoral component rotational alignment. Knee 2022, 38, 107–116. [Google Scholar] [CrossRef]
- Xu, Z.; Chen, D.; Shi, D.; Dai, J.; Yao, Y.; Jiang, Q. Evaluation of posterior lateral femoral condylar hypoplasia using axial MRI images in patients with complete discoid meniscus. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 909–914. [Google Scholar] [CrossRef]
- Kubota, M.; Ohno, R.; Sato, T.; Yamaguchi, J.; Kaneko, H.; Kaneko, K.; Ishijima, M. The medial proximal tibial angle accurately corrects the limb alignment in open-wedge high tibial osteotomy. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2410–2416. [Google Scholar] [CrossRef]
- Tanzer, M.; Makhdom, A.M. Preoperative planning in primary total knee arthroplasty. JAAOS J. Am. Acad. Orthop. Surg. 2016, 24, 220–230. [Google Scholar] [CrossRef]
- Matsushita, T.; Watanabe, S.; Araki, D.; Nagai, K.; Hoshino, Y.; Kanzaki, N.; Matsumoto, T.; Niikura, T.; Kuroda, R. Differences in preoperative planning for high-tibial osteotomy between the standing and supine positions. Knee Surg. Relat. Res. 2021, 33, 8. [Google Scholar] [CrossRef]
- He, A.; Mao, Y.; Zhou, Y.; Kong, Q.; Zhang, H.; Chen, Y.; Liu, W.; Zhang, X. Preoperative planning by osteotomy master software helps to improve the accuracy of target limb alignment in high tibial osteotomy. J. Orthop. Surg. Res. 2020, 15, 504. [Google Scholar] [CrossRef]
- MacDessi, S.J.; Griffiths-Jones, W.; Harris, I.A.; Bellemans, J.; Chen, D.B. Coronal Plane Alignment of the Knee (CPAK) classification. Bone Jt. J. 2021, 103-b, 329–337. [Google Scholar] [CrossRef] [PubMed]
- MacDessi, S.J.; Griffiths-Jones, W.; Harris, I.A.; Bellemans, J.; Chen, D.B. The arithmetic HKA (aHKA) predicts the constitutional alignment of the arthritic knee compared to the normal contralateral knee: A matched-pairs radiographic study. Bone Jt. Open 2020, 1, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Hirvasniemi, J.; Runhaar, J.; van der Heijden, R.A.; Zokaeinikoo, M.; Yang, M.; Li, X.; Tan, J.; Rajamohan, H.R.; Zhou, Y.; Deniz, C.M.; et al. The KNee OsteoArthritis Prediction (KNOAP2020) challenge: An image analysis challenge to predict incident symptomatic radiographic knee osteoarthritis from MRI and X-ray images. Osteoarthr. Cartil. 2023, 31, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Oláh, T.; Reinhard, J.; Laschke, M.W.; Goebel, L.K.H.; Walter, F.; Schmitt, G.; Speicher-Mentges, S.; Menger, M.D.; Cucchiarini, M.; Pape, D.; et al. Axial alignment is a critical regulator of knee osteoarthritis. Sci. Transl. Med. 2022, 14, eabn0179. [Google Scholar] [CrossRef]
- Cooke, T.D.; Sled, E.A.; Scudamore, R.A. Frontal plane knee alignment: A call for standardized measurement. J. Rheumatol. 2007, 34, 1796–1801. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Numbers |
|---|---|
| Total | Patients: 63/Knee: 121 |
| Gender | Male: 10/Female: 53 |
| Age (mean ± SD) | 72.206 ± 9.587 years |
| Measurements (included numbers) | Mean ± SD (degrees) |
| HKA (n = 121) | 5.934 ± 5.853 (positive value when knee is varus alignment) |
| MPTA (n = 121) | 85.979 ± 2.493 |
| mLDFA (n = 121) | 87.784 ± 2.044 |
| JLCA (n = 121) | 3.748 ± 3.282 (positive value when lateral side is open) |
| MFCA/TEA (n = 121) | 5.630 ± 2.096 (positive value when medial side is open) |
| PCA/TEA (n = 69) | 5.591 ± 2.220 (positive value when medial side is open) |
| PCOA (n = 121) | 107.200 ± 21.254 |
| Parameter | ICC of Intraobserver (Observer1) | ICC of Interobserver |
|---|---|---|
| HKA | 0.983 (0.976–0.988) | 0.989 (0.977–0.994) |
| MPTA | 0.823 (0.746–0.876) | 0.906 (0.865–0.934) |
| mLDFA | 0.821 (0.744–0.875) | 0.837 (0.767–0.886) |
| JLCA | 0.976 (0.966–0.983) | 0.956 (0.933–0.970) |
| MFCA/TEA | 0.899 (0.855–0.929) | 0.819 (0.741–0.874) |
| PCA/TEA | 0.951 (0.921–0.970) | 0.813 (0.699–0.884) |
| PCOA | 0.957 (0.906–0.977) | 0.991 (0.987–0.994) |
| Variables | Coefficient of Correlation | p-Value |
|---|---|---|
| HKA | 0.568 | 0.0001 |
| MPTA | −0.308 | 0.001 |
| mLDFA | 0.369 | 0.0001 |
| JLCA | 0.513 | 0.0001 |
| MFCA/TEA | −0.226 | 0.013 |
| PCA/TEA | −0.228 | 0.058 |
| HKA | MPTA | mLDFA | JLCA | MFCA/TEA | PCA/TEA | |
|---|---|---|---|---|---|---|
| HKA | −0.610 (0.0001) | 0.591 (0.0001) | 0.810 (0.0001) | −0.311 (0.001) | −0.516 (0.0001) | |
| MPTA | −0.610 (0.0001) | −0.171 (0.061) | −0.267 (0.003) | 0.046 (0.616) | 0.241 (0.046) | |
| mLDFA | 0.591 (0.0001) | −0.171 (0.061) | 0.377 (0.0001) | −0.145 (0.112) | 0.063 (0.605) | |
| JLCA | 0.810 (0.0001) | −0.267 (0.003) | 0.377 (0.0001) | −0.431 (0.0001) | −0.478 (0.0001) | |
| MFCA/TEA | −0.311 (0.001) | 0.046 (0.616) | −0.145 (0.112) | −0.431 (0.0001) | 0.646 (0.0001) | |
| PCA/TEA | −0.516 (0.0001) | 0.241 (0.046) | 0.063 (0.605) | −0.478 (0.0001) | 0.646 (0.0001) |
| Associated Variable | Regression Coefficient | p-Value |
|---|---|---|
| HKA | 0.468 | 0.0001 |
| Multiple regression equation | PCOA = 104.754 + 0.468 HKA | |
| Not associated variables | MPTA, mLDFA, JLCA, MFCA/TEA, PCA/TEA | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.H.; Lee, H.S.; Kim, B.-H.; Lee, S.-W. Is the Surface Anatomy of the Popliteal Crease Related to Lower Extremity Alignment or Knee Osseous Morphology? A Radiographic Study. Medicina 2023, 59, 1849. https://doi.org/10.3390/medicina59101849
Lee DH, Lee HS, Kim B-H, Lee S-W. Is the Surface Anatomy of the Popliteal Crease Related to Lower Extremity Alignment or Knee Osseous Morphology? A Radiographic Study. Medicina. 2023; 59(10):1849. https://doi.org/10.3390/medicina59101849
Chicago/Turabian StyleLee, Dong Hwan, Hwa Sung Lee, Bo-Hyoung Kim, and Se-Won Lee. 2023. "Is the Surface Anatomy of the Popliteal Crease Related to Lower Extremity Alignment or Knee Osseous Morphology? A Radiographic Study" Medicina 59, no. 10: 1849. https://doi.org/10.3390/medicina59101849
APA StyleLee, D. H., Lee, H. S., Kim, B.-H., & Lee, S.-W. (2023). Is the Surface Anatomy of the Popliteal Crease Related to Lower Extremity Alignment or Knee Osseous Morphology? A Radiographic Study. Medicina, 59(10), 1849. https://doi.org/10.3390/medicina59101849