
Associations between Oral Glucose-Lowering Agents and Increased Risk for Life-Threatening Arrhythmias in Patients with Type 2 Diabetes Mellitus—A Literature Review

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
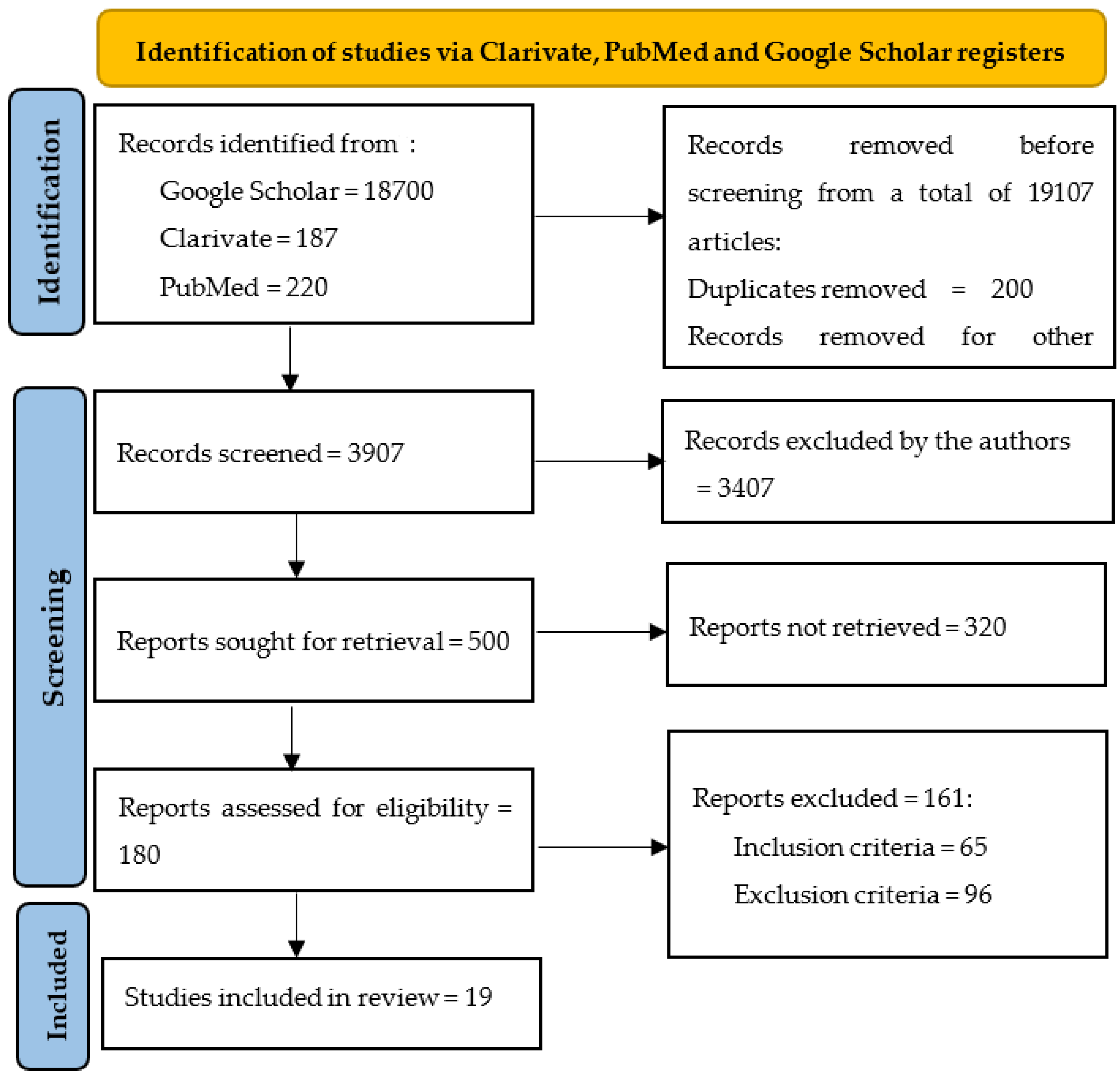
2. Materials and Methods
3. Results
3.1. Results Concerning the Arrhythmogenic Risk of Metformin Versus Sulfonylureas and Other oral GLA
3.2. Results Referring to Arrhytmogenic Risk of Thiazolidinediones
3.3. Results Concerning Dipeptidyl Peptidase-4 Inhibitors
3.4. Results Concerning the Efficacy of SGLT2i for the Reduction of Arrhythmias Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on Diabetes, Pre-Diabetes, and Cardiovascular Diseases Developed in Collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [PubMed]
- Abuelgasim, E.; Shah, S.; Abuelgasim, B.; Soni, N.; Thomas, A.; Elgasim, M.; Harky, A. Clinical Overview of Diabetes Mellitus as a Risk Factor for Cardiovascular Death. Rev. Cardiovasc. Med. 2021, 22, 301–314. [Google Scholar] [CrossRef] [PubMed]
- Kenny, H.C.; Abel, E.D. Heart Failure in Type 2 Diabetes Mellitus: Impact of Glucose-Lowering Agents, Heart Failure Therapies, and Novel Therapeutic Strategies. Circ. Res. 2019, 124, 121–141. [Google Scholar] [CrossRef] [PubMed]
- Zaveri, M.P.; Perry, J.C.; Schuetz, T.M.; Memon, M.D.; Faiz, S.; Cancarevic, I. Diabetic Cardiomyopathy as a Clinical Entity: Is It a Myth? Cureus 2020, 12, e11100. [Google Scholar] [CrossRef] [PubMed]
- Ferrini, M.; Johansson, I.; Aboyans, V. Heart Failure and Its Complications in Patients with Diabetes: Mounting Evidence for a Growing Burden. Eur. J. Prev. Cardiol. 2019, 26, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Jia, G.; Hill, M.A.; Sowers, J.R. Diabetic Cardiomyopathy: An Update of Mechanisms Contributing to This Clinical Entity. Circ. Res. 2018, 122, 624–638. [Google Scholar] [CrossRef]
- Tang, Z.; Wang, P.; Dong, C.; Zhang, J.; Wang, X.; Pei, H. Oxidative Stress Signaling Mediated Pathogenesis of Diabetic Cardiomyopathy. Oxidative Med. Cell. Longev. 2022, 2022, 5913374. [Google Scholar] [CrossRef]
- Weidner, K.; Behnes, M.; Schupp, T.; Rusnak, J.; Reiser, L.; Bollow, A.; Taton, G.; Reichelt, T.; Ellguth, D.; Engelke, N.; et al. Type 2 Diabetes Is Independently Associated with All-Cause Mortality Secondary to Ventricular Tachyarrhythmias. Cardiovasc. Diabetol. 2018, 17, 125. [Google Scholar] [CrossRef]
- Chen, H.-Y.; Huang, J.-Y.; Siao, W.-Z.; Jong, G.-P. The Association between SGLT2 Inhibitors and New-Onset Arrhythmias: A Nationwide Population-Based Longitudinal Cohort Study. Cardiovasc. Diabetol. 2020, 19, 73. [Google Scholar] [CrossRef]
- Ozturk, N.; Uslu, S.; Ozdemir, S. Diabetes-Induced Changes in Cardiac Voltage-Gated Ion Channels. World J. Diabetes 2021, 12, 1–18. [Google Scholar] [CrossRef]
- Hamilton, S.; Terentyev, D. Proarrhythmic Remodeling of Calcium Homeostasis in Cardiac Disease; Implications for Diabetes and Obesity. Front. Physiol. 2018, 9, 1517. [Google Scholar] [CrossRef] [PubMed]
- Gallego, M.; Zayas-Arrabal, J.; Alquiza, A.; Apellaniz, B.; Casis, O. Electrical Features of the Diabetic Myocardium. Arrhythmic and Cardiovascular Safety Considerations in Diabetes. Front. Pharmacol. 2021, 12, 687256. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, C.; Chatterjee, S.; Seidu, S.; Bodicoat, D.H.; Ng, G.A.; Davies, M.J.; Khunti, K. Association of Hypoglycaemia and Risk of Cardiac Arrhythmia in Patients with Diabetes Mellitus: A Systematic Review and Meta-Analysis. Diabetes Obes. Metab. 2018, 20, 2169–2178. [Google Scholar] [CrossRef] [PubMed]
- Sfairopoulos, D.; Zhang, N.; Wang, Y.; Chen, Z.; Letsas, K.P.; Tse, G.; Li, G.; Lip, G.Y.H.; Liu, T.; Korantzopoulos, P. Association between Sodium–Glucose Cotransporter-2 Inhibitors and Risk of Sudden Cardiac Death or Ventricular Arrhythmias: A Meta-Analysis of Randomized Controlled Trials. EP Eur. 2022, 24, 20–30. [Google Scholar] [CrossRef]
- Fernandes, G.C.; Fernandes, A.; Cardoso, R.; Penalver, J.; Knijnik, L.; Mitrani, R.D.; Myerburg, R.J.; Goldberger, J.J. Association of SGLT2 Inhibitors with Arrhythmias and Sudden Cardiac Death in Patients with Type 2 Diabetes or Heart Failure: A Meta-Analysis of 34 Randomized Controlled Trials. Heart Rhythm 2021, 18, 1098–1105. [Google Scholar] [CrossRef]
- Scheen, A.J. Glucose-Lowering Agents and Risk of Ventricular Arrhythmias and Sudden Cardiac Death: A Comprehensive Review Ranging from Sulphonylureas to SGLT2 Inhibitors. Diabetes Metab. 2022, 48, 101405. [Google Scholar] [CrossRef]
- Kolesnik, E.; Scherr, D.; Rohrer, U.; Benedikt, M.; Manninger, M.; Sourij, H.; von Lewinski, D. SGLT2 Inhibitors and Their Antiarrhythmic Properties. Int. J. Mol. Sci. 2022, 23, 1678. [Google Scholar] [CrossRef]
- Leonard, C.E.; Brensinger, C.M.; Dawwas, G.K.; Deo, R.; Bilker, W.B.; Soprano, S.E.; Dhopeshwarkar, N.; Flory, J.H.; Bloomgarden, Z.T.; Gagne, J.J.; et al. The Risk of Sudden Cardiac Arrest and Ventricular Arrhythmia with Rosiglitazone versus Pioglitazone: Real-World Evidence on Thiazolidinedione Safety. Cardiovasc. Diabetol. 2020, 19, 25. [Google Scholar] [CrossRef]
- Islam, N.; Ayele, H.T.; Yu, O.H.Y.; Douros, A.; Filion, K.B. Sulfonylureas and the Risk of Ventricular Arrhythmias Among People with Type 2 Diabetes: A Systematic Review of Observational Studies. Clin. Pharmacol. Ther. 2022, 111, 1248–1257. [Google Scholar] [CrossRef]
- Lim, V.G.; He, H.; Lachlan, T.; Ng, G.A.; Kyrou, I.; Randeva, H.S.; Osman, F. Impact of Sodium-Glucose Co-Transporter Inhibitors on Cardiac Autonomic Function and Mortality: No Time to Die. EP Eur. 2022, 24, 1052–1057. [Google Scholar] [CrossRef]
- Fawzy, A.M.; Rivera-Caravaca, J.M.; Underhill, P.; Fauchier, L.; Lip, G.Y.H. Incident Heart Failure, Arrhythmias and Cardiovascular Outcomes with Sodium-glucose Cotransporter 2 (SGLT2) Inhibitor Use in Patients with Diabetes: Insights from a Global Federated Electronic Medical Record Database. Diabetes Obes. Metab. 2023, 25, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Oates, C.P.; Santos-Gallego, C.G.; Smith, A.; Basyal, B.; Moss, N.; Kawamura, I.; Musikantow, D.R.; Turagam, M.K.; Miller, M.A.; Whang, W.; et al. SGLT2 Inhibitors Reduce Sudden Cardiac Death Risk in Heart Failure: Meta-analysis of Randomized Clinical Trials. Cardiovasc. Electrophysiol. 2023, 34, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Júlíusdóttir, Y.K.; Halili, A.; Coronel, R.; Folke, F.; Torp-Pedersen, C.; Gislason, G.H.; Eroglu, T.E. Sodium-Glucose Cotransporter-2 Inhibitors Compared with Glucagon-like-Peptide-1 Receptor Agonists and out-of-Hospital Cardiac Arrest in Type 2 Diabetes: A Nationwide Nested Case-Control Study. Eur. Heart J. Cardiovasc. Pharmacother. 2023, 9, pvad033. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Leonard, C.E.; Brensinger, C.M.; Aquilante, C.L.; Bilker, W.B.; Boudreau, D.M.; Deo, R.; Flory, J.H.; Gagne, J.J.; Mangaali, M.J.; Hennessy, S. Comparative Safety of Sulfonylureas and the Risk of Sudden Cardiac Arrest and Ventricular Arrhythmia. Diabetes Care 2018, 41, 713–722. [Google Scholar] [CrossRef]
- Persson, F.; Nyström, T.; Jørgensen, M.E.; Carstensen, B.; Gulseth, H.L.; Thuresson, M.; Fenici, P.; Nathanson, D.; Eriksson, J.W.; Norhammar, A.; et al. Dapagliflozin Is Associated with Lower Risk of Cardiovascular Events and All-cause Mortality in People with Type 2 Diabetes (CVD-REAL Nordic) When Compared with Dipeptidyl Peptidase-4 Inhibitor Therapy: A Multinational Observational Study. Diabetes Obes. Metab. 2018, 20, 344–351. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Shao, S.-C.; Chang, K.-C.; Hung, M.-J.; Yang, N.-I.; Chan, Y.-Y.; Chen, H.-Y.; Kao Yang, Y.-H.; Lai, E.C.-C. Comparative Risk Evaluation for Cardiovascular Events Associated with Dapagliflozin vs. Empagliflozin in Real-World Type 2 Diabetes Patients: A Multi-Institutional Cohort Study. Cardiovasc. Diabetol. 2019, 18, 120. [Google Scholar] [CrossRef]
- Dhopeshwarkar, N.; Brensinger, C.M.; Bilker, W.B.; Soprano, S.E.; Flory, J.H.; Dawwas, G.K.; Gagne, J.J.; Hennessy, S.; Leonard, C.E. Risk of Sudden Cardiac Arrest and Ventricular Arrhythmia with Sulfonylureas: An Experience with Conceptual Replication in Two Independent Populations. Sci. Rep. 2020, 10, 10070. [Google Scholar] [CrossRef]
- Hsieh, Y.; Liao, Y.; Li, C.; Lin, J.; Weng, C.; Lin, C.; Lo, C.; Huang, K.; Huang, J.; Lin, C.; et al. Hypoglycaemic Episodes Increase the Risk of Ventricular Arrhythmia and Sudden Cardiac Arrest in Patients with Type 2 Diabetes—A Nationwide Cohort Study. Diabetes Metab. Res. Rev. 2020, 36, e3226. [Google Scholar] [CrossRef]
- Ostropolets, A.; Elias, P.A.; Reyes, M.V.; Wan, E.Y.; Pajvani, U.B.; Hripcsak, G.; Morrow, J.P. Metformin Is Associated with a Lower Risk of Atrial Fibrillation and Ventricular Arrhythmias Compared With Sulfonylureas: An Observational Study. Circ. Arrhythmia Electrophysiol. 2021, 14, e009115. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wu, H.-Y.; Chien, K.-L. Cardioprotective Effects of Dipeptidyl Peptidase-4 Inhibitors versus Sulfonylureas in Addition to Metformin: A Nationwide Cohort Study of Patients with Type 2 Diabetes. Diabetes Metab. 2022, 48, 101299. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.T.L.; Hui, J.M.H.; Lee, Y.H.A.; Satti, D.I.; Shum, Y.K.L.; Kiu, P.T.H.; Wai, A.K.C.; Liu, T.; Wong, W.T.; Chan, J.S.K.; et al. Sulfonylurea Is Associated with Higher Risks of Ventricular Arrhythmia or Sudden Cardiac Death Compared With Metformin: A Population-Based Cohort Study. J. Am. Heart Assoc. 2022, 11, e026289. [Google Scholar] [CrossRef] [PubMed]
- Dawwas, G.K.; Hennessy, S.; Brensinger, C.M.; Deo, R.; Bilker, W.B.; Soprano, S.E.; Dhopeshwarkar, N.; Flory, J.H.; Bloomgarden, Z.T.; Aquilante, C.L.; et al. Comparative Safety of Dipeptidyl Peptidase-4 Inhibitors and Sudden Cardiac Arrest and Ventricular Arrhythmia: Population-Based Cohort Studies. Clin. Pharmacol. Ther. 2022, 111, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.-C.; Chiu, K.-P.; Wang, C.-L.; Hsu, C.-Y.; Tu, H.-T.; Huang, Y.-T.; Chang, C.-H.; Huang, C.-H.; Kuo, C.-F.; Chen, S.-W.; et al. Electrocardiographic Changes Associated with SGLT2 Inhibitors and Non-SGLT2 Inhibitors: A Multi-Center Retrospective Study. Front. Cardiovasc. Med. 2022, 9, 934193. [Google Scholar] [CrossRef]
- Jhuo, S.-J.; Lin, T.-H.; Lin, Y.-H.; Tsai, W.-C.; Liu, I.-H.; Wu, B.-N.; Lee, K.-T.; Lai, W.-T. Clinical Observation of SGLT2 Inhibitor Therapy for Cardiac Arrhythmia and Related Cardiovascular Disease in Diabetic Patients with Controlled Hypertension. J. Pers. Med. 2022, 12, 271. [Google Scholar] [CrossRef]
- Eroglu, T.E.; Coronel, R.; Zuurbier, C.J.; Blom, M.; De Boer, A.; Souverein, P.C. Use of Sodium-Glucose Cotransporter-2 Inhibitors and the Risk for Sudden Cardiac Arrest and for All-Cause Death in Patients with Type 2 Diabetes Mellitus. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 9, 18–25. [Google Scholar] [CrossRef]
- Islam, N.; Reynier, P.; Douros, A.; Yu, O.H.Y.; Filion, K.B. Sulphonylureas versus Metformin and the Risk of Ventricular Arrhythmias among People with Type 2 Diabetes: A Population-based Cohort Study. Diabetes Obes. Metab. 2023, 25, 1523–1533. [Google Scholar] [CrossRef]
- Zeppenfeld, K.; Tfelt-Hansen, J.; De Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; De Chillou, C.; et al. 2022 ESC Guidelines for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Savarese, G.; Butler, J.; Lund, L.H.; Bhatt, D.L.; Anker, S.D. Cardiovascular Effects of Non-Insulin Glucose-Lowering Agents: A Comprehensive Review of Trial Evidence and Potential Cardioprotective Mechanisms. Cardiovasc. Res. 2022, 118, 2231–2252. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Yu, X.; Zheng, Y.; Li, J.; Wang, Y.; Lin, Y.; He, Z.; Zhao, W.; Chen, C.; Qiu, K.; et al. Association of Glucose-Lowering Medications with Cardiovascular Outcomes: An Umbrella Review and Evidence Map. Lancet Diabetes Endocrinol. 2020, 8, 192–205. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S111–S124. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43 (Suppl. S1), S111–S134. [Google Scholar] [CrossRef]

{kind=link}
| Nr. | Article | Publi- cation Year | Study Population | Number of Patients | Objective of Follow Up | Observation |
|---|---|---|---|---|---|---|
| 1. | Weidner et al. Observational study [8] | 2018 | Patients with T2DM, treated mostly with metformin and sulfonylureea | 2411 patients with VA followed for 2 years | VA, SCA, CV events, all-cause mortality | T2DM represents an increased risk for VA, SCA and all-cause mortality. |
| 2. | Leonard et al. Nonexperimental comparable safty study [25] | 2018 | USA, 30–75 years, new users of second generation sulfonylureea | 519,272 adults | VA, SCA | Glyburide with 18% reduction of VA/SCA compared to glypizide. |
| 3. | Persson et al. A multinational observational study [26] | 2018 | Adults with T2DM, new users either of dapagliflozin or of DPP4i | 40,908 patients: 10,227 on dapagliflozin and 30,681 on a DPP4i | Major CV events, VA, SCA | SGLT2 were associated with lower CV morbidity and mortality, but not of arrhythmias |
| 4. | Wiviott et al. A multinational observational study [27] | 2019 | Patients with T2DM, treated with dapagliflozin | 17,160 patients followed for 4.2 years | Major CV events, VA, SCA | No reduction of major CV events, including VA and SCA, but a decrease on CV mortality and hospitalization |
| 5. | Shao et al. A multi-institutional cohort study [28] | 2019 | T2DM patients, new SGLT2i users: 10,442 on dapagliflozin and 12,096 on empagliflozin | 12,681 patients, mean age = 58.9 years, | Major CV events, VA, SCA | No significant difference between dapagliflozin and empagliflozin regarding major CV events |
| 6. | Leonard et al. Cohort study [18] | 2020 | Patients with T2DM, from 5 USA states, new users of thiazolidinediones | 500,091, aged 30–75 years, treated with thiazolidinediones | VA, SCA, precipitating hospital presentations | Rosiglitazone and pioglitazone are associated with a similar risk of VA and SCA |
| 7. | Dhopeshwarkar et al. Two cohort studies from five US states [29] | 2020 | Adult patients with T2DM newly tretead with second generation sulfonylureea drugs | 624,406 in Medicaid and 491940 in Optum | VA, SCA, precipitating hospital presentations | Conflicting results regarding VA/SCA for glimepiride and glyburide versus glipizide |
| 8. | Chen et al., Populational based longitudinal cohort study [9] | 2020 | Patients newely diagnosed T2DM | 399,810 P: 79,150 P with SGLT2i and 79,150 P without SGLT2i | SCA, VA | All cause mortality and arrhythmias were reduced. |
| 9. | Hsieh et al., A nationwide cohort study [30] | 2020 | Adults, newly diagnosed T2DM, identified from the Taiwan National Health Insurance Database, treated with GLA among which sulfonylureea | 1037 P with hypoglicemia due to GLA among wich sulfonylureea versus 4148 without hypoglycemia | VA, SCA | Hypoglicemia was assoviated with increased risk of VA/SCA |
| 10. | Ostropolets et al. Observational study [31] | 2021 | Patients with T2DM, but without advanced disease/complications, treated with oral GLA, excluding insuline | 645,785 P followed for 1 year | VA/SCA, atrial fibrillation | Patients on metformine monotherapy have a significanly reduced risk (34%) for VA compared to sulfonylureea. |
| 11. | Wang et al. National cohort study [32] | 2022 | Adult pacients with T2DM from Taiwan, without advanced disease/complications | 37,317 matched pairs of DPP4i and SU users, mean follow-up of 2.1 years. | Major CV events, VA, SCA and hospitalization | Sitagliptin and vildagliptin had a lower risk of hospitalization, VA and SCA |
| 12. | Lee et al. Cohort study from Hong Kong [33] | 2022 | Pacients over 40 years old, without MI, treated either with metformin or sulfonylureeas | 33,192 patients, followed 5 years | VA, SCA, death due to arrhytmias | Sulfonylureea was associated with higher risk of VA and SCA than metformin. |
| 13. | Daawas et al. Population based cohort study [34] | 2022 | USA, subjects with T2DM, 30–75 years, followed over 1 year | 48,388 patient treated with DPP-4i: saxagliptin, sitagliptin, linagliptin | VA, SCA | Discordand results regarding the association betweeeen SCA/VA and saxaglyptine compaired with sitaglyptine. |
| 14. | Wu et al. Cohort study [35] | 2022 | Over 18 years, without cardiovascular pathology | 1056 with SGLT2i inhibitors vs. 2119 controls | VA | No difference regarding VA between patients treated with SGLT2 inhibitors and those without SGLT2 inhibitors |
| 15. | Jhuo et al. Cohort study [36] | 2022 | Followed minumum 4 years | 9609–3203 with SGLT2i vs 6406 without SGLT2i | VA | Significant lower incidence of total cardiac arrhythmias and cardiovascular events. |
| 17. | Eroglu et al. Cohort study [37] | 2022 | Newly treated diabetic patients. Median follow up was 2.6 years. | 152591–15125 on SGLT2i treatment | VA, SCA | SGLT2i reduced all cause mortality but not SCD. |
| 16. | Fawzy et al., Retrospective cohort study [21] | 2023 | Worldwide, all adult patients registered with T2DM during 1 January 2018 and 31 December 2019 | 131,189 patients treated with SGLT2i versus 131,189 without SGLT2i followed for 2 years | VA, SCA, atrial fibrillation, major CV events | SGLT2i reduce significantly CV events, SCD but not VA |
| 18. | Júlíusdóttir et al. Nation wide case control study [23] | 2023 | Danish population | 21708P with T2 DM—3618 with SCA—593 on SGLT2i | SCA | SGLT2i had lower risk for SCA in comparison to glucagon-like-peptide-1 receptor agonist. |
| 19. | Islam et al. Cohort study from UK [38] | 2023 | Adult patients with T2DM, newly treated either with sulfonyl-urea or metformine | 92,638 new user of sulfonylurea and 506,882 new users of metformine | VA | Sulfonyluree is associated with increased risk of VA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tudoran, C.; Tudoran, M.; Giurgi-Oncu, C.; Abu-Awwad, A.; Abu-Awwad, S.-A.; Voiţă-Mekereş, F. Associations between Oral Glucose-Lowering Agents and Increased Risk for Life-Threatening Arrhythmias in Patients with Type 2 Diabetes Mellitus—A Literature Review. Medicina 2023, 59, 1760. https://doi.org/10.3390/medicina59101760
Tudoran C, Tudoran M, Giurgi-Oncu C, Abu-Awwad A, Abu-Awwad S-A, Voiţă-Mekereş F. Associations between Oral Glucose-Lowering Agents and Increased Risk for Life-Threatening Arrhythmias in Patients with Type 2 Diabetes Mellitus—A Literature Review. Medicina. 2023; 59(10):1760. https://doi.org/10.3390/medicina59101760
Chicago/Turabian StyleTudoran, Cristina, Mariana Tudoran, Catalina Giurgi-Oncu, Ahmed Abu-Awwad, Simona-Alina Abu-Awwad, and Florica Voiţă-Mekereş. 2023. "Associations between Oral Glucose-Lowering Agents and Increased Risk for Life-Threatening Arrhythmias in Patients with Type 2 Diabetes Mellitus—A Literature Review" Medicina 59, no. 10: 1760. https://doi.org/10.3390/medicina59101760
APA StyleTudoran, C., Tudoran, M., Giurgi-Oncu, C., Abu-Awwad, A., Abu-Awwad, S.-A., & Voiţă-Mekereş, F. (2023). Associations between Oral Glucose-Lowering Agents and Increased Risk for Life-Threatening Arrhythmias in Patients with Type 2 Diabetes Mellitus—A Literature Review. Medicina, 59(10), 1760. https://doi.org/10.3390/medicina59101760