
COVID-19 Associated Guillain–Barré Syndrome: A Report of Nine New Cases and a Review of the Literature


 and
and
Abstract
:1. Introduction
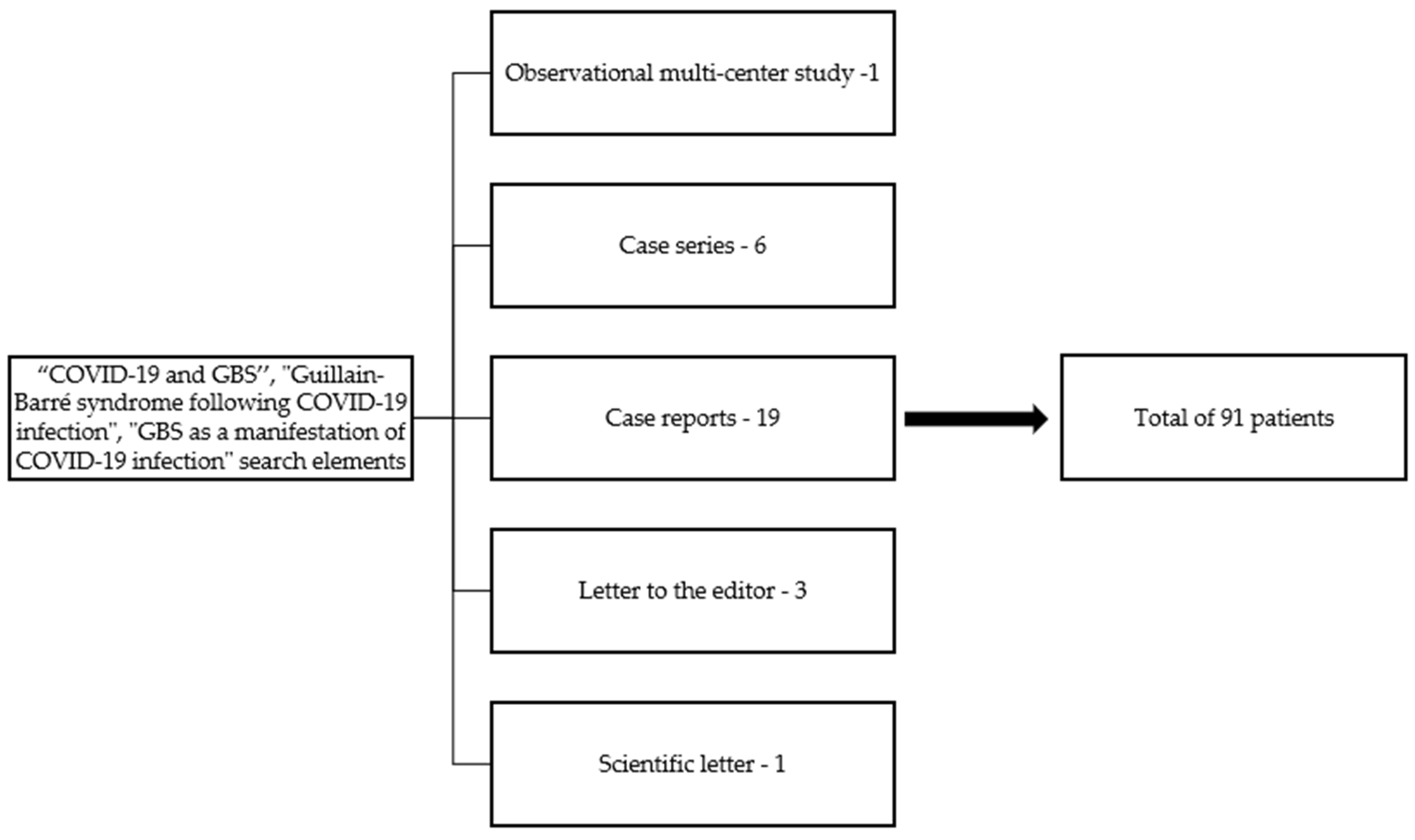
2. Materials and Methods
3. Results
3.1. Presentation
3.1.1. Clinical Presentation
3.1.2. Paraclinical Investigations
3.1.3. Treatment
3.1.4. Outcome
3.2. Literature Review
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization—WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 30 October 2021).
- Tsai, P.-H.; Lai, W.-Y.; Lin, Y.-Y.; Luo, Y.-H.; Chen, H.-K.; Chen, Y.-M.; Lai, Y.-C.; Kuo, L.-C.; Chen, S.-D.; Chang, K.-J.; et al. Clinical manifestation and disease progression in COVID-19 infection. J. Chin. Med. Assoc. 2020, 84, 3–8. [Google Scholar] [CrossRef]
- Salton, F.; Confalonieri, P.; Campisciano, G.; Cifaldi, R.; Rizzardi, C.; Generali, D.; Pozzan, R.; Tavano, S.; Bozzi, C.; Lapadula, G.; et al. Cytokine Profiles as Potential Prognostic and Therapeutic Markers in SARS-CoV-2-Induced ARDS. J. Clin. Med. 2022, 11, 2951. [Google Scholar] [CrossRef]
- Baratella, E.; Ruaro, B.; Marrocchio, C.; Starvaggi, N.; Salton, F.; Giudici, F.; Quaia, E.; Confalonieri, M.; Cova, M.A. Interstitial Lung Disease at High Resolution CT after SARS-CoV-2-Related Acute Respiratory Distress Syndrome According to Pulmonary Segmental Anatomy. J. Clin. Med. 2021, 10, 3985. [Google Scholar] [CrossRef]
- Alqahtani, M.; Abbas, M.; Alqahtani, A.; Alshahrani, M.; Alkulib, A.; Alelyani, M.; Almarhaby, A.; Alsabaani, A. A Novel Computational Model for Detecting the Severity of Inflammation in Confirmed COVID-19 Patients Using Chest X-ray Images. Diagnostics 2021, 11, 855. [Google Scholar] [CrossRef]
- Ricchio, M.; Tassone, B.; Pelle, M.; Mazzitelli, M.; Serapide, F.; Fusco, P.; Lionello, R.; Cancelliere, A.; Procopio, G.; Lio, E.; et al. Characteristics, Management, and Outcomes of Elderly Patients with Diabetes in a Covid-19 Unit: Lessons Learned from a Pilot Study. Medicina 2021, 57, 341. [Google Scholar] [CrossRef]
- Whittaker, A.; Anson, M.; Harky, A. Neurological Manifestations of COVID-19: A systematic review and current update. Acta Neurol. Scand. 2020, 142, 14–22. [Google Scholar] [CrossRef]
- Shahrizaila, N.; Lehmann, H.C.; Kuwabara, S. Guillain-Barré syndrome. Lancet 2021, 397, 1214–1228. [Google Scholar] [CrossRef]
- Ho, T.; Hsieh, S.-T.; Nachamkin, I.; Willison, H.J.; Sheikh, K.; Kiehlbauch, J.; Flanigan, K.; McArthur, J.C.; Cornblath, D.R.; McKhann, G.M.; et al. Motor nerve terminal degeneration provides a potential mechanism for rapid recovery in acute motor axonal neuropathy after campylobacter infection. Neurology 1997, 48, 717–724. [Google Scholar] [CrossRef]
- Doets, A.Y.; Verboon, C.; Berg, B.V.D.; Harbo, T.; Cornblath, D.R.; Willison, H.J.; Islam, Z.; Attarian, S.; Barroso, F.A.; Bateman, K.; et al. Regional variation of Guillain-Barré syndrome. Brain 2018, 141, 2866–2877. [Google Scholar] [CrossRef] [Green Version]
- Leonhard, S.E.; Mandarakas, M.R.; Gondim, F.A.A.; Bateman, K.; Ferreira, M.L.B.; Cornblath, D.R.; Van Doorn, P.A.; Dourado, M.E.; Hughes, R.A.C.; Islam, B.; et al. Diagnosis and management of Guillain–Barré syndrome in ten steps. Nat. Rev. Neurol. 2019, 15, 671–683. [Google Scholar] [CrossRef]
- Ray, S.; Jain, P.C. Acute bulbar palsy plus syndrome: A rare variant of Guillain–Barre syndrome. J. Pediatr. Neurosci. 2016, 11, 322–323. [Google Scholar] [CrossRef] [Green Version]
- Yuki, N.; Hartung, H.-P. Guillain–Barré Syndrome. N. Engl. J. Med. 2012, 366, 2294–2304. [Google Scholar] [CrossRef]
- Sejvar, J.J.; Baughman, A.L.; Wise, M.; Morgan, O.W. Population Incidence of Guillain-Barré Syndrome: A Systematic Review and Meta-Analysis. Neuroepidemiology 2011, 36, 123–133. [Google Scholar] [CrossRef] [Green Version]
- Filosto, M.; Piccinelli, S.C.; Gazzina, S.; Foresti, C.; Frigeni, B.; Servalli, M.C.; Sessa, M.; Cosentino, G.; Marchioni, E.; Ravaglia, S.; et al. Guillain-Barré syndrome and COVID-19: An observational multicentre study from two Italian hotspot regions. J. Neurol. Neurosurg. Psychiatry 2020, 92, 751–756. [Google Scholar] [CrossRef]
- Alshekhlee, A.; Hussain, Z.; Sultan, B.; Katirji, B. Guillain-Barre syndrome: Incidence and mortality rates in US hospitals. Neurology 2008, 70, 1608–1613. [Google Scholar] [CrossRef]
- Zhao, H.; Shen, D.; Zhou, H.; Liu, J.; Chen, S. Guillain-Barré syndrome associated with SARS-CoV-2 infection: Causality or coincidence? Lancet Neurol. 2020, 19, 383–384. [Google Scholar] [CrossRef]
- Fragiel, M.; Miró, Ò.; Llorens, P.; Jiménez, S.; Piñera, P.; Burillo, G.; Martín, A.; Martín-Sánchez, F.J.; Lamberechts, E.J.G.; Jacob, J.; et al. Incidence, clinical, risk factors and outcomes of Guillain-Barré in COVID-19. Ann. Neurol. 2020, 89, 598–603. [Google Scholar] [CrossRef]
- National Institute of Public Health, Romania. Available online: https://insp.gov.ro/centrul-national-de-supraveghere-si-control-al-bolilor-transmisibile-cnscbt/infectia-cu-noul-coronavirus-sars-cov-2/analiza-cazuri-confirmate-covid19/ (accessed on 17 July 2022).
- Davidescu, E.I.; Odajiu, I.; Ilie, M.D.; Bunea, T.; Sandu, G.; Stratan, L.; Iftode, N.; Aramă, V.; Popescu, B.O. Influence of tocilizumab on the outcome of patients with COVID-19. retrospective observational study. Farmacia 2020, 68, 792–799. [Google Scholar] [CrossRef]
- Davidescu, E.I.; Odajiu, I.; Ilie, M.D.; Bunea, T.; Sandu, G.; Stratan, L.; Aramă, V.; Popescu, B.O. Treatment with hydroxychloroquine in patients with covid-19. Experience of a neurology department. Farmacia 2020, 68, 597–605. [Google Scholar] [CrossRef]
- Molina, E.A.; Martínez, M.M.; Chueca, S.P.; López, C.A.; Sancho Val, I.; Sanjuan-Villarreal, T.A. Guillain-Barré syndrome associated with SARS-CoV-2 infection. Med. Intensiva 2020, 44, 513–514. [Google Scholar] [CrossRef]
- Svačina, M.K.R.; Kohle, F.; Sprenger, A.; Lehmann, H.C. Could symptom overlap of COVID-19 and Guillain–Barré syndrome mask an epidemiological association? J. Neurol. 2021, 268, 3595–3597. [Google Scholar] [CrossRef]
- Bueso, T.; Montalvan, V.; Lee, J.; Gomez, J.; Ball, S.; Shoustari, A.; Julayanont, P.; Jumper, C. Guillain-Barre Syndrome and COVID-19: A case report. Clin. Neurol. Neurosurg. 2020, 200, 106413. [Google Scholar] [CrossRef]
- Kamel, W.A.; Ismail, I.I.; Al-Hashel, J.Y. Guillain-Barre Syndrome following COVID-19 Infection: First Case Report from Kuwait and Review of the Literature. Dubai Med. J. 2021, 4, 42–46. [Google Scholar] [CrossRef]
- Singh, R.; Shiza, S.T.; Saadat, R.; Dawe, M.; Rehman, U. Association of Guillain-Barre Syndrome with COVID-19: A Case Report and Literature Review. Cureus 2021, 13, e13828. [Google Scholar] [CrossRef]
- Sidig, A.; Abbasher, K.; Abbasher, H.; Abbasher, M.H.A. COVID-19 and Guillain-Barre Syndrome Case Report. J. Neurol. Neurobiol. 2020, 7, e21246. [Google Scholar]
- Webb, S.; Wallace, V.C.; Martin-Lopez, D.; Yogarajah, M. Guillain-Barré syndrome following COVID-19: A newly emerging post-infectious complication. BMJ Case Rep. 2020, 13, e236182. [Google Scholar] [CrossRef]
- Korem, S.; Gandhi, H.; Dayag, D.B. Guillain-Barré syndrome associated with COVID-19 disease. BMJ Case Rep. 2020, 13, e237215. [Google Scholar] [CrossRef]
- Almutairi, A.; Bin Abdulqader, S.; Alhameed, M.; Alit, S.; Alosaimi, B. Guillain-BarrE Syndrome Following COVID-19: A Case Report. J. Res. Med. Dent. Sci. 2021, 9, 7–10. [Google Scholar]
- Mantefardo, B.; Gube, A.A.; Awlachew, E.; Sisay, G. Novel Coronavirus (COVID-19)-Associated Guillain–Barre’ Syndrome: Case Report. Int. Med. Case Rep. J. 2021, 14, 251–253. [Google Scholar] [CrossRef]
- Camdessanche, J.-P.; Morel, J.; Pozzetto, B.; Paul, S.; Tholance, Y.; Botelho-Nevers, E. COVID-19 may induce Guillain–Barré syndrome. Rev. Neurol. 2020, 176, 516–518. [Google Scholar] [CrossRef]
- Sedaghat, Z.; Karimi, N. Guillain Barre syndrome associated with COVID-19 infection: A case report. J. Clin. Neurosci. 2020, 76, 233–235. [Google Scholar] [CrossRef] [PubMed]
- Virani, A.; Rabold, E.; Hanson, T.; Haag, A.; Elrufay, R.; Cheema, T.; Balaan, M.; Bhanot, N. Guillain-Barré Syndrome associated with SARS-CoV-2 infection. IDCases 2020, 20, e00771. [Google Scholar] [CrossRef] [PubMed]
- Caamaño, D.S.J.; Beato, R.A. Facial diplegia, a possible atypical variant of Guillain-Barré Syndrome as a rare neurological complication of SARS-CoV-2. J. Clin. Neurosci. 2020, 77, 230–232. [Google Scholar] [CrossRef] [PubMed]
- Coen, M.; Jeanson, G.; Almeida, L.A.C.; Hübers, A.; Stierlin, F.; Najjar, I.; Ongaro, M.; Moulin, K.; Makrygianni, M.; Leemann, B.; et al. Guillain-Barré syndrome as a complication of SARS-CoV-2 infection. Brain Behav. Immun. 2020, 87, 111–112. [Google Scholar] [CrossRef]
- Alberti, P.; Beretta, S.; Piatti, M.; Karantzoulis, A.; Piatti, M.L.; Santoro, P.; Viganò, M.; Giovannelli, G.; Pirro, F.; Montisano, D.A.; et al. Guillain-Barré syndrome related to COVID-19 infection. Neurol. Neuroimmunol. Neuroinflamma. 2020, 7, e741. [Google Scholar] [CrossRef]
- Yakoby, J.; Litvak, I.; Yu, E. Guillain-Barré Syndrome after Novel Coronavirus Disease 2019. J. Emerg. Med. 2021, 61, e67–e70. [Google Scholar] [CrossRef]
- Diez-Porras, L.; Vergés, E.; Gil-López, F.J.; Vidal, M.J.; Massons, J.; Arboix, A. Guillain-Barré-Strohl syndrome and COVID-19: Case report and literature review. Neuromuscul. Disord. 2020, 30, 859–861. [Google Scholar] [CrossRef]
- Rajdev, K.; Victor, N.; Buckholtz, E.S.; Hariharan, P.; Saeed, M.A.; Hershberger, D.M.; Bista, S. A Case of Guillain-Barré Syndrome Associated With COVID-19. J. Investig. Med. High Impact Case Rep. 2020, 8, 2324709620961198. [Google Scholar] [CrossRef]
- Rana, S.; Lima, A.A.; Chandra, R.; Valeriano, J.; Desai, T.; Freiberg, W.; Small, G. Novel Coronavirus (COVID-19)-Associated Guillain–Barré Syndrome: Case Report. J. Clin. Neuromuscul. Dis. 2020, 21, 240–242. [Google Scholar] [CrossRef]
- Mackenzie, N.; Lopez-Coronel, E.; Dau, A.; Maloof, D.; Mattar, S.; Garcia, J.T.; Fontecha, B.; Lanata, C.M.; Guillen-Burgos, H.F. Concomitant Guillain-Barre syndrome with COVID-19: A case report. BMC Neurol. 2021, 21, 135. [Google Scholar] [CrossRef]
- Yiu, A.C.; Hussain, A.; Okonkwo, U.A.; Villacorta-Lyew, R.; McMahon, M.J.; Blattner, M. Guillain–Barre Syndrome Associated with COVID-19 Pneumonia—The First Documented Case in a U.S. Military Intensive Care Unit. Mil. Med. 2021, usab158. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.; Han, S.C.; Kelly, S.; Tamimi, M.; Giglio, B.; Lewis, A. A Case Series of Guillain-Barré Syndrome After COVID-19 Infection in New York. Neurol. Clin. Pract. 2020, 11, e576–e578. [Google Scholar] [CrossRef] [PubMed]
- Okhovat, A.A.; Ansari, B.; Hemasian, H.; Haghi-Ashtiani, B.; Advani, S.; Ziaadini, B.; Abdi, S.; Sikaroudi, H.; Nafissi, S.; Fatehi, F. Guillain-Barre syndrome in patients with coronavirus disease-2019: Report of six cases and review of literature. Curr. J. Neurol. 2021, 19, 122–130. [Google Scholar] [CrossRef]
- Gutiérrez-Ortiz, C.; Méndez-Guerrero, A.; Rodrigo-Rey, S.; Pedro-Murillo, E.S.; Bermejo-Guerrero, L.; Gordo-Mañas, R.; de Aragón-Gómez, F.; Benito-León, J. Miller Fisher syndrome and polyneuritis cranialis in COVID-19. Neurology 2020, 95, e601–e605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foresti, C.; Servalli, M.C.; Frigeni, B.; Rifino, N.; Storti, B.; Gritti, P.; Fabretti, F.; Grazioli, L.; Sessa, M. COVID-19 provoking Guillain–Barré syndrome: The Bergamo case series. Eur. J. Neurol. 2020, 28, e84–e85. [Google Scholar] [CrossRef]
- Toscano, G.; Palmerini, F.; Ravaglia, S.; Ruiz, L.; Invernizzi, P.; Cuzzoni, M.G.; Franciotta, D.; Baldanti, F.; Daturi, R.; Postorino, P.; et al. Guillain–Barré Syndrome Associated with SARS-CoV-2. N. Engl. J. Med. 2020, 382, 2574–2576. [Google Scholar] [CrossRef]
- Nanda, S.; Handa, R.; Prasad, A.; Anand, R.; Zutshi, D.; Dass, S.K.; Bedi, P.K.; Pahuja, A.; Shah, P.K.; Sharma, B. COVID-19 associated Guillain-Barre Syndrome: Contrasting tale of four patients from a tertiary care centre in India. Am. J. Emerg. Med. 2020, 39, 125–128. [Google Scholar] [CrossRef]
- Abu-Rumeileh, S.; Abdelhak, A.; Foschi, M.; Tumani, H.; Otto, M. Guillain–Barré syndrome spectrum associated with COVID-19: An up-to-date systematic review of 73 cases. J. Neurol. 2020, 268, 1133–1170. [Google Scholar] [CrossRef]
- Gu, B.; Yao, L.; Zhu, X.-Y.; Zou, T.; Feng, Y.-J.; Yan, J.-Y.; Zhang, J.-P.; Tang, P.-J.; Chen, C. Comparison of initial clinic characteristics of hospitalized patients in Suzhou City during the COVID-19 Omicron wave with ancestral variant wave. Ther. Adv. Respir. Dis. 2022, 16, 17534666221110346. [Google Scholar] [CrossRef]
- Abolmaali, M.; Heidari, M.; Zeinali, M.; Moghaddam, P.; Ghamsari, M.R.; Makiani, M.J.; Mirzaasgari, Z. Guillain–Barré syndrome as a parainfectious manifestation of SARS-CoV-2 infection: A case series. J. Clin. Neurosci. 2020, 83, 119–122. [Google Scholar] [CrossRef]
- Ottaviani, D.; Boso, F.; Tranquillini, E.; Gapeni, I.; Pedrotti, G.; Cozzio, S.; Guarrera, G.M.; Giometto, B. Early Guillain-Barré syndrome in coronavirus disease 2019 (COVID-19): A case report from an Italian COVID-hospital. Neurol. Sci. 2020, 41, 1351–1354. [Google Scholar] [CrossRef] [PubMed]
- Parra, B.; Lizarazo, J.; Jiménez-Arango, J.A.; Zea-Vera, A.F.; González-Manrique, G.; Vargas, J.; Angarita, J.A.; Zuñiga, G.; Lopez-Gonzalez, R.; Beltran, C.L.; et al. Guillain–Barré Syndrome Associated with Zika Virus Infection in Colombia. N. Engl. J. Med. 2016, 375, 1513–1523. [Google Scholar] [CrossRef] [PubMed]
- Berg, B.V.D.; Bunschoten, C.; van Doorn, P.A.; Jacobs, B.C. Mortality in Guillain-Barre syndrome. Neurology 2013, 80, 1650–1654. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Case | Sex | Age | Comorbidities | COVID-19 Symptoms | SaO2 (%) on Admission | Days between the Onset of Neurological Symptoms and Admission to Hospital | Days between COVID-19 Symptoms and Neurological Symptoms | Neurological Symptoms |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 56 | - | Dyspnea, cough myalgia | 96% with 3 L O2/min | 8 | 11 | Progressive ascending tetraparesis (1/5 LL, 3/5 UL), hyperreflexia, bilateral facial palsy, paresthesia, superficial and deep hypoesthesia, dysautonomia (paralytic ileus, urinary, and fecal incontinence) |
| 2 | F | 65 | Arterial hypertension, type 2 diabetes mellitus, obesity | Dyspnea | 95% with 2 L O2/min | 3 | - | Progressive ascending tetraparesis followed by paraplegia (0/5 LL, 1/5 UL), areflexia, paresthesia, lower limbs deep anesthesia, dysarthria, mixed dysphagia |
| 3 | M | 67 | - | Dyspnea, fever, chills | 99% on room air (o.r.a) | 3 | 1 | Progressive asymmetric paraparesis (LL 2.5/5), left upper limb weakness, lower back pain, areflexia, paresthesia, lower limbs superficial and deep hypoesthesia, dysphonia, constipation |
| 4 | M | 56 | Arterial hypertension | Fever, cough | 97% o.r.a | 14 | 14 | Progressive ascending paraparesis up to knee level (4/5), areflexia in lower limbs, “glove and stocking” paresthesia, lower limbs hypoesthesia |
| 5 | F | 56 | - | Cough, myalgia | 96% o.r.a | 7 | 7 | Progressive ascending flaccid tetraparesis (1/5 LL, 3/5 UL), areflexia, paresthesia, superficial hypoesthesia, deep anesthesia in lower limbs, dysphonia, mixed dysphagia, fecal and urinary incontinence |
| 6 | M | 41 | Obesity, Hypercholesterolemia history of AMSAN | - | 98% o.r.a | 1 | - | Progressive ascending flaccid tetraparesis (3/5 LL, 4/5 UL), hyporeflexia |
| 7 | M | 51 | Arterial hypertension, obesity | Fever, cough, myalgia, chills, diarrhea | 97% o.r.a | 7 | 21 | Progressive ascending tetraparesis (3/5 LL, 4/5 UL), areflexia |
| 8 | M | 39 | Stroke, central core disease, type 2 diabetes mellitus | Headache, loss of appetite | 98% o.r.a | 8 | 6 | Progressive ascending tetraparesis (3/5 LL, 4/5 UL), ataxia, lower limbs areflexia, upper limbs paresthesia, dysarthria |
| 9 | M | 51 | Epilepsy secondary to childhood meningoencephalitis | Hyposmia, hypogeusia, dyspnea | 97% o.r.a | 3 | 7 | Progressive ascending tetraparesis followed by paraplegia, areflexia, paresthesia, superficial and deep hypoesthesia, left side peripheral facial palsy, exhaustible right-beating nystagmus, mixed dysphagia, dysarthria |
| Admission | Mid-Hospitalization | Discharge | |
|---|---|---|---|
| White blood cell count (×1000/µL) | 9.2644 | 10.7500 | 7.3460 |
| Lymphocyte count (×1000/µL) | 1.5344 | 2.2700 | 3.0940 |
| Platelet count (×100/µL) | 342.5556 | 290.4286 | 308.0000 |
| D-dimers (µg/mL) | 0.6475 | 1.3967 | 1.0040 |
| Fibrinogen (mg/dL) | 566.2500 | 514.3333 | 518.7500 |
| INR | 1.0613 | 1.1467 | 1.0400 |
| C-reactive protein (mg/L) | 29.1722 | 89.7267 | 14.8040 |
| Ferritin (ng/mL) | 571.8333 | 642.7500 | 1410.6667 |
| Procalcitonin (ng/mL) | 0.0600 | 0.2200 | 0.1167 |
| IL-6 (pg/mL) | 26.5133 | 24.0367 | 19.6400 |
| LDH (IU/L) | 233.1667 | 347.0000 | 222.3333 |
| GBS Variant | CSF Findings | Ganglioside Autoantibodies | Thoracic CT—% of Pulmonary Involvement | Acute Respiratory Failure | Need for Intubation | G.B.S. Treatment | COVID-19 Treatment | Hospitalization (Days) | Outcome | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | AIDP | Normal | Absent | 70% | Yes | No | IVIG | Remdesivir, LMWH 8000 IU, DEXA | 32 | Significant motor function improvement—mMRC 2/5 LL, 4/5 UL, improved paresthesia |
| 2 | AIDP | CAD | - | 20% | Yes | Yes | PEX, IVIG | Remdesivir, LMWH 400 IU, DEXA | 36 | Gradual motor function improvement—mMRC 1/5 LL, 3/5 UL |
| 3 | AIDP | CAD | Absent | 50% | Yes | No | IVIG | Remdesivir, LMWH 4000 IU, DEXA | 18 | Gradual motor function improvement (can ambulate with unilateral support) |
| 4 | AIDP | CAD | - | 15% | No | No | IVIG | Favipiravir, LMWH 4000 IU | 10 | absent motor weakness, improved paresthesia, and hypoesthesia |
| 5 | AIDP | - | - | 20% | Yes | No | IVIG | LMWH 6000 IU | 2 | Exitus due to respiratory failure |
| 6 | AMAN | - | - | 15% | No | No | IVIG | LMWH 4000 IU | 5 | Favorable |
| 7 | AMAN | CAD | - | 50% | No | No | IVIG | Tocilizumab LMWH 4000 IU | 12 | Favorable |
| 8 | AIDP | CAD | - | 15% | No | No | IVIG | Hydroxycloroquine LMWH 4000 IU | 9 | residual tetra-ataxia (predominantly in the lower limbs), can ambulate with unilateral support, no sensitive impairment |
| 9 | AIDP | CAD | - | 45% | Yes | Yes | PEX, IVIG | LMWH 4000 IU, DEXA | 52 | improved motor function (cannot ambulate), residual hypoesthesia, residual nystagmus, postural and intentional tremor, dysphonia |
| Article | Type of Study | No. of Cases | Mean Age | Sex | COVID-19 Symptoms | Days between COVID-19 Symptoms and Neurological Symptoms | Neurological Symptoms |
|---|---|---|---|---|---|---|---|
| Bueso et al. [24] | Case report | 1 | 60 | F | Fever, cough, myalgia, dysgeusia | 22 | Symmetrical tetraparesis, inability to walk, lower limbs areflexia, UL hyporeflexia, sacro-lumbar pain, paresthesia dysautonomia (fluctuations in HR and mean arterial pressure, fecal incontinence, urinary retention) |
| Kamel et al. [25] | Case report | 1 | 72 | M | Fever, cough, myalgia, dyspnea | 21 | Tetraparesis, unsteady, stamping gait, global areflexia, “glove and stocking” hypoesthesia, sensory ataxia, hypoesthesia to fine touch, and vibration distal to clavicle |
| Singh et al. [26] | Case report | 1 | 45 | M | Fever, cough, dyspnea | 7 | Tetraparesis, LL areflexia, UL hyporeflexia, bilateral facial paresis, paresthesia, hypoesthesia to fine touch, and vibration distal to calf |
| Sidig et al. [27] | Case report | 1 | 65 | M | Fever, cough, sore throat, headache, generalized fatigue | 5 | Ascending tetramelic tetraparesis and paresthesia, generalized hypotonia and areflexia, truncal weakness, bilateral papilledema, olfactory nerve involvement, bilateral facial nerve involvement, slight palatal muscle weakness, facial paresthesia with the inability to close his mouth and his both eyes, urinary incontinence |
| Webb et al. [28] | Case report | 1 | 57 | M | Fever, cough, myalgia, headache, malaise, diarrhea | 7 | Progressive tetraparesis, hypotonia, areflexia, foot dysesthesia, and hypoesthesia |
| Korem et al. [29] | Case report | 1 | 58 | F | Fever, cough, back pain | 14 | Tetraparesis, unstable gait, persistent back pain radiating to both lower extremities, foot paresthesia, hyporeflexia |
| Almutairi et al. [30] | Case report | 1 | 36 | M | Cough, diarrhea | 14 | Bilateral progressive distal extremity numbness, LL areflexia, UL hyporeflexia, tetramelic hypoesthesia, speech impairments, bilateral facial weakness |
| Mantefardo et al. [31] | Case report | 1 | 17 | F | Dyspnea, right flank pain, vomiting | N/A | Paraplegia, areflexia |
| Camdessanche et al. [32] | Case report | 1 | 64 | M | Fever, dyspnea | 11 | Flaccid tetraparesis, paresthesia in feet and hands, global areflexia, dysphagia |
| Sedaghat et al. [33] | Case report | 1 | 65 | M | Cough, fever, occasional dyspnea | 14 | Ascending symmetric tetraparesis, global areflexia, bilateral facial paresis, reduction in the vibration, and fine touch sensation distal to the ankle joints |
| Virani et al. [34] | Case report | 1 | 54 | M | Cough | 10 | Ascending tetraparesis, global areflexia, LL paresthesia |
| Zhao et al. [17] | Letter to editor | 1 | 61 | F | Fever, cough | 8 days after neurologic symptoms onset | Progressive tetraparesis, LL areflexia, distal hypoesthesia |
| Caamaño et al. [35] | Case report | 1 | 61 | M | Fever, cough | 10 | Peripheral bilateral facial paresis |
| Coen et al. [36] | Letter to editor | 1 | 70 | M | Cough, myalgia, generalized fatigue | 10 | Paraparesis, distal allodynia, urinary retention, constipation |
| Alberti et al. [37] | Case report | 1 | 71 | M | Fever | 7 | Progressive flaccid tetraparesis, paresthesia, global areflexia |
| Yakoby et al. [38] | Case report | 1 | 35 | M | Fever, cough | 9 | Tetramelic motor deficit, left LL areflexia, right LL hyporeflexia, intermittent fasciculations, UL coarse resting tremor, LL sensory deficit to light touch, and pinprick |
| Diez-Porras et al. [39] | Case report | 1 | 54 | M | Fever, cough, myalgia | 5 | Severe flaccid tetraparesis, global areflexia, bilateral facial palsy, dysphagia, hypoesthesia in the left mandibular region, and distal UL region |
| Rajdev et al. [40] | Case report | 1 | 36 | M | Fever, respiratory distress, cough, chills, myalgia | 18 | Ascending tetraparesis, difficulty walking, LL areflexia and paresthesia, UL hyporeflexia, |
| Rana et al. [41] | Case report | 1 | 54 | M | Fever, rhinorrhea, odynophagia, chills, night sweats | 14 | Ascending tetraparesis, areflexia, facial diplegia, ophthalmoparesis, resting tachycardia, urinary retention |
| Mackenzie et al. [42] | Case report | 1 | 39 | F | Ageusia, anosmia, headache, myalgia | 20 | Ascending tetraparesis, inability to walk, generalized areflexia, left arm paresthesia |
| Molina et al. [22] | Scientific letter | 1 | 55 | F | Fever, dry cough, dyspnea | 14 | Progressive tetraparesis, areflexia, hands and feet paresthesia, intense lumbar pain irradiating to both legs, dysphagia, bilateral facial diplegia, eyelid closing weakness, tongue, and perioral paresthesia |
| Yiu et al. [43] | Case report | 1 | 69 | M | Hypoxemic respiratory failure, fever, headache, dyspnea, decreased oral intake, diarrhea | 36 | Symmetric flaccid tetraparesis, generalized areflexia |
| Chan et al. [44] | Case series | 2 | 1. 68 2. 84 | 2M | 1.- Fever, upper respiratory symptoms 2.- Fever | 1–18 2–23 | Patient 1: Progressive gait disturbance and hands and feet paresthesia, weakness, inability to ambulate, bilateral facial weakness, dysphagia, dysarthria, neck flexion Patient 2: Progressive arm weakness, progressive gait disturbance (inability to stand or ambulate independently), UL hyporeflexia, LL areflexia, bilateral facial paresis, hands, and feet paresthesia, toes diminished vibration and proprioception, autonomic dysfunction |
| Okhovat et al. [45] | Case series | 6 | 56 | 4F 2M | Fever (4 patients), dyspnoea (4 patients), cough (2 patients), malaise (1 patient), headache (1 patient) | 14 | Ascending tetraparesis (6 patients), areflexia (5 patients), facial weakness (1 patient), paresthesia (3 patients), hypoesthesia (5 patients) |
| Gutierrez-Ortiz et al. [46] | Case series | 2 | 1. 50 2. 39 | 2M | 1. fever, cough, malaise, headache, low back pain, anosmia, ageusia 2. fever, diarrhea, generally poor condition | Patient 1 and 2: 3 | Patient 1: Gait instability, vertical diplopia, perioral paresthesia Patient 2: Diplopia |
| Foresti et al. [47] | Case series | 17 | 53 | 11M 6F | N/A | 12 h–28 days | N/A |
| Toscano et al. [48] | Case series | 5 | 61 | 4M 1F | Fever (3), cough (4), hypogeusia (2), anosmia (2), sore throat (1), asthenia (1) | 5–10 | Tetraplegia (2 patients), tetraparesis (2 patients), areflexia (5 patients), bulbar symptoms (1 patient), facial weakness (1 patient), facial diplegia (1 patient), paresthesia (3 patients) |
| Nanda et al. [49] | Case series | 4 | 55 | 3M 1F | Fever (2), abdominal pain (1), cough (2), sore throat (1) | 8.5 | Progressive tetraparesis (3 patients), paraparesis (1 patient), generalized areflexia (2 patient), bilateral facial palsy (1 patient), hypoesthesia (1 patient) |
| Svačina et al. [23] | Letter to editor | 3 | 68 | 2M 1F | Patient 1: Reduction of general condition, dyspnea Patient 2: Rhinorrhea, headache Patient 3: dyspnea | Patient 1 and 2: 4 Patient 3: N/A | Patient 1: Progressive flaccid tetraparesis, general areflexia, phrenic-bulbar involvement Patient 2: Facial palsy, oculomotor palsy, hypoglossal palsy Patient 3: Tetraparesis, areflexia, distal paresthesia |
| Abu-Rumeileh et al. [50] | Observational multicenter study | 30 | 59 0.2 | 22M 8F | Fever, cough, dyspnea, dysgeusia, anosmia, gastrointestinal symptoms | Median 16–35 | Tetraparesis—25, predominant paraparesis—1, predominant upper limb paresis—3 + sensory symptoms in all patients |
| Article | GBS Variant | CSF Findings | Electromyographic Findings | Spinal MRI. | Serum Antiganglioside Antibodies | Respiratory Dysfunction/ Need for Intubation (+/−) | Treatment for G.B.S. | Outcome |
|---|---|---|---|---|---|---|---|---|
| Bueso et al. [24] | N/A | CAD | - | N/A | N/A | Yes/(−) | IVIG | Respiratory improvement, ambulating with assistance, persistent LL neuropathic pain |
| Kamel et al. [25] | AIDP | CAD | Decreased velocity, decreased CMAP, less prominent focal slowing, significantly delayed late responses | Degenerative changes | Negative anti-GD1a and anti-GQ1b antibodies | No | IVIG | After one month: no motor weakness (patient could walk without support), marked improvement in deep sensation examination |
| Singh et al. [26] | AMSAN | CAD | Decreased amplitude, normal distal latencies, and prolonged F-wave latencies, decreased recruitment, decreased response in sensory and motor nerves | Degenerative changes | N/A | No | IVIG | Motor and sensory function improved significantly |
| Sidig et al. [27] | AIDP | N/A | Predominant demyelination pattern | Normal | N/A | Yes/(+) | IVIG | Exitus after seven days due to progressive respiratory failure |
| Webb et al. [23] | AIDP | CAD | Decreased velocity, prolonged distal motor latencies in motor and sensory nerves, dispersed motor action potentials, prolonged or absent F-waves, reduced velocities in sensory nerves, absent sensory action potentials in the right median nerve | N/A | N/A | Yes/(+) | IVIG | N/A |
| Korem et al. [29] | N/A | CAD | - | Degenerative changes | - | No | IVIG | About 80% improvement in motor strength of all limbs, complete resolution of paresthesia |
| Almuitairi et al. [30] | N/A | Normal | Absent SNAP of median and superficial peroneal nerves, delayed distal motor latency, borderline low CMAP of right median nerve, slow conduction velocities, prolonged F-wave latencies | N/A | N/A | No | IVIG | After one month: mild residual bilateral lower motor neuron facial weakness |
| Mantefardo et al. [31] | N/A | CAD | - | - | - | Yes/N/A | No | Exitus due to respiratory failure |
| Camdessanche et al. [37] | AIDP | CAD | Demyelinating pattern | - | Negative | Yes/(+) | IVIG | N/A |
| Sedaghat et al. [33] | AMSAN | - | Decreased amplitude CMAP, no response for SNAP, decreased recruitment | - | - | No | IVIG | N/A |
| Virani et al. [34] | N/A | - | - | Normal | - | Yes/(+) | IVIG | Residual LL weakness |
| Zhao et al. [17] | AIDP | - | Delayed distal latencies, absent F waves | - | - | No | No | Symptoms completely resolved |
| Caamaño et al. [27] | N/A | CAD | - | - | - | No | Low dose oral prednisone for 2 weeks | After two weeks: barely notable improvement on both sides |
| Coen et al. [36] | AIDP | CAD | Sensorimotor demyelinating polyneuropathy with “sural sparing pattern”, decreased persistence, or absent F-waves | Normal | Negative | No | IVIG | Rapid improvement |
| Alberti et al. [28] | AIDP | CAD | Absent sural nerve SNAP, absent tibial nerve CMAP, markedly increased common peroneal CMAP distal latency, markedly decreased velocity, moderately decreased CMAP amplitude (with spatial and temporal dispersion) for the same nerve, decreased ulnar SAP amplitude | - | - | Yes/(−) | IVIG | Patient died due to respiratory failure |
| Yakoby et al. [38] | N/A | CAD | - | Normal | Negative | No | IVIG | Noticeable improvement |
| Diez-Porras et al. [39] | AIDP | CAD | Conduction blocks, absence of F waves in the right ulnar nerve and axon potentials in the F response of the right tibial nerve) of diffuse distribution | - | IgM for GM2 and GD3 | Yes/(+) | IVIG | Seven weeks later: the patient was able to walk independently with support |
| Rajdev et al. [40] | AIDP | CAD | Patchy, multifocal demyelination with unequivocal conduction block, prolonged F-wave latencies, sural sparing | Normal | N/A | Yes/(+) | IVIG | Before discharge: motor strength continued to improve (muscle strength of 4/5 in proximal and 5/5 in distal muscle groups bilaterally) following extubation |
| Rana et al. [41] | AIDP, Miller Fisher syndrome | - | Consistent with the demyelinating form of GBS with secondary axonal degeneration | Normal | - | Yes/(+) | IVIG | N/A |
| Mackenzie et al. [42] | N/A | CAD | Prolonged distal motor latencies and action potential amplitudes, sural sparing | Degenerative changes | - | Yes/N/A | P.E.X. | Discharged after 20 days with the improvement of neurological status (LL—4/5(MRC)) and respiratory symptoms |
| Molina et al. [21] | AIDP | CAD | Prolonged distal motor latencies, absent F waves in the posterior tibial or cubital nerves, prolonged distal latencies in the left and right facial nerves with potential time dispersion. Potential desynchronization of the sensory nerve trunks of the arms with reduced velocities | Slightly enhanced leptomeningeal uptake in brainstem and cervical spinal cord level | - | No | IVIG | Motor balance 5/5 of the right arm, 3/5 of the left arm and 4/5 of both legs, persistence of paresthesia |
| Yiu et al. [43] | N/A | CAD | Prolonged sensory and motor amplitudes, widespread, reduced sensory nerve and CMAP amplitudes, slowing of conduction velocities in the left median and ulnar nerves with severe, demyelinating range slowing of left tibial NCV, reduced recruitment | - | - | Yes/(+) | IVIG | Fully independent patient 100 days after GBS diagnosis and able to walk 3.21 Kilometers independently with frequent breaks |
| Chan et al. [44] | Patient 1—N/A | CAD | - | Normal | Negative | No | PEX. | After 28 days: dysphagia has resolved, can ambulate with minimal assistance |
| Patient 2—N/A | CAD | - | N/A | Elevated GM2 IgG/IgM antibodies | Yes/(+) | PEX IVIG | N/A | |
| Okhovat et al. [45] | AIDP (2) AMAN (2) AMSAN (2) | CAD (1) | Consistent with GBS (6) | Normal (3) | Negative (1) | Yes/(+) (1) 2. No (5) | IVIG (3 patients) PEX (3) | Favorable (6 patients) |
| Gutierrez-Ortiz et al. [46] | MFS. | Patient 1: CAD | - | - | Positive for anti- GD1b IgG antibody | No | IVIG | Marked improvement |
| Foresti et al. [47] | AIDP (16) | N/A | Consistent with GBS (16) | N/A | N/A | N/A | IVIG (15) PEX (2) | Discharged (16 patients) Death (1 patient) |
| Toscano et al. [48] | AMSAN (2) AMAN (1) AIDP (2) | Normal (2) | Consistent with GBS (5) | Enhancement of caudal nerve roots (2), Enhancement of the the facial nerve (1), normal (2) | Negative (3 patients) | Yes (3)/(2+) No (2) | IVIG (5) PEX (1) | After four weeks: Two patients remained in the ICU. Two patients had flaccid paraplegia One patient was walking independently |
| Nanda et al. [49] | AMAN (2) AIDP (1) AMSAN (1) | CAD | Consistent with GBS (4) | Degenerative changes (4) | N/A | Yes (1)/(+) No (3) | IVIG (4) | 1 patient: death 3 patients: significant improvement |
| Svačina et al. [22] | Patients 1, 3: Axonal-demyelinating sensorimotor polyradiculoneuropathy Patient 2: polyneuritis cranialis | CAD (3) | Consistent with GBS (3) | N/A | Patient 1: anti-sulfatide IgM autoantibodies Patient 2, 3: negative | Yes (1) N/A(2) | IVIG (3) | Patient 1: Sever tetraparesis Patient 2: Mild oculomotor palsy Patient 3: Severe tetraparesis |
| Abu-Rumeileh et al. [50] | Classical GBS (27), Facial diplegia (1), Pure sensory form (1), Pharyngeal-cervical-brachial (1) | CAD—7 Normal—14 | AIDP (23), AMAN(2) Equivocal (5) | N/A | N/A | Yes (5) | PEX(2), IVIG(25), None(3) | Response to treatment(23) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ivan, A.P.; Odajiu, I.; Popescu, B.O.; Davidescu, E.I. COVID-19 Associated Guillain–Barré Syndrome: A Report of Nine New Cases and a Review of the Literature. Medicina 2022, 58, 977. https://doi.org/10.3390/medicina58080977
Ivan AP, Odajiu I, Popescu BO, Davidescu EI. COVID-19 Associated Guillain–Barré Syndrome: A Report of Nine New Cases and a Review of the Literature. Medicina. 2022; 58(8):977. https://doi.org/10.3390/medicina58080977
Chicago/Turabian StyleIvan, Andreea Paula, Irina Odajiu, Bogdan Ovidiu Popescu, and Eugenia Irene Davidescu. 2022. "COVID-19 Associated Guillain–Barré Syndrome: A Report of Nine New Cases and a Review of the Literature" Medicina 58, no. 8: 977. https://doi.org/10.3390/medicina58080977
APA StyleIvan, A. P., Odajiu, I., Popescu, B. O., & Davidescu, E. I. (2022). COVID-19 Associated Guillain–Barré Syndrome: A Report of Nine New Cases and a Review of the Literature. Medicina, 58(8), 977. https://doi.org/10.3390/medicina58080977