
Pre-Hospital Delay in Acute Ischemic Stroke Care: Current Findings and Future Perspectives in a Tertiary Stroke Center from Romania—A Cross-Sectional Study

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
3.2. General Characteristics of the Study Population
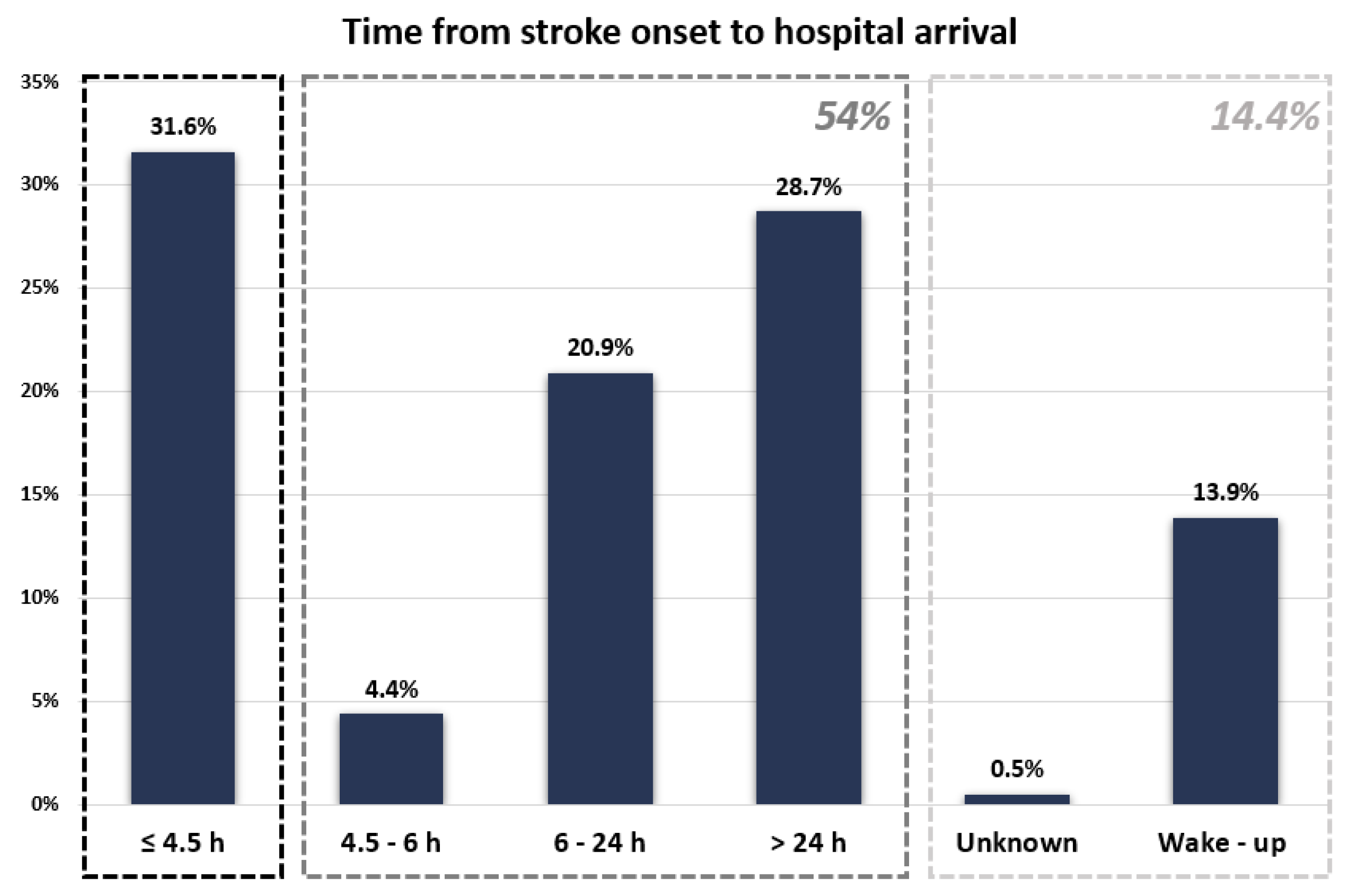
3.3. Time Intervals between Stroke Onset and Hospital Arrival
3.4. Factors Associated with Late Arrival to Hospital
3.5. Factors Associated with Very Late Arrival to Hospital
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, C.O.; Nguyen, M.; Roth, G.A.; Nichols, E.; Alam, T.; Abate, D. GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 439–458. [Google Scholar] [CrossRef]
- Lancet, T. Life, death, and disability in 2016. Lancet 2017, 390, 1083. [Google Scholar] [CrossRef]
- Avan, A.; Digaleh, H.; Di Napoli, M.; Stranges, S.; Behrouz, R.; Shojaeianbabaei, G.; Amiri, A.; Tabrizi, R.; Mokhber, N.; Spence, J.D.; et al. Socioeconomic status and stroke incidence, prevalence, mortality, and worldwide burden: An ecological analysis from the Global Burden of Disease Study 2017. BMC Med. 2019, 17, 1–30. [Google Scholar] [CrossRef]
- Fisher, M. The Ischemic Penumbra: Identification, Evolution and Treatment Concepts. Cerebrovasc. Dis. 2003, 17, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Berge, E.; Whiteley, W.; Audebert, H.; De Marchis, G.M.; Fonseca, A.C.; Padiglioni, C.; de la Ossa, N.P.; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur. Stroke J. 2021, 6, I–LXII. [Google Scholar] [CrossRef]
- Turc, G.; Bhogal, P.; Fischer, U.; Khatri, P.; Lobotesis, K.; Mazighi, M.; Schellinger, P.D.; Toni, D.; De Vries, J.; White, P.; et al. European Stroke Organisation (ESO)—European Society for Minimally Invasive Neurological Therapy (ESMINT) Guidelines on Mechanical Thrombectomy in Acute Ischemic Stroke. J. Neurointerv. Surg. 2019, 11, 535–538. [Google Scholar] [CrossRef]
- Vanacker, P.; Lambrou, D.; Eskandari, A.; Mosimann, P.J.; Maghraoui, A.; Michel, P. Eligibility and Predictors for Acute Revascularization Procedures in a Stroke Center. Stroke 2016, 47, 1844–1849. [Google Scholar] [CrossRef]
- Reiff, T.; Michel, P. Reasons and evolution of non-thrombolysis in acute ischaemic stroke. Emerg. Med. J. 2016, 34, 219–226. [Google Scholar] [CrossRef]
- Pulvers, J.N.; Watson, J.D.G. If Time Is Brain Where Is the Improvement in Prehospital Time after Stroke? Front. Neurol. 2017, 8, 617. [Google Scholar] [CrossRef]
- Majersik, J.J.; Smith, M.A.; Zahuranec, D.B.; Sánchez, B.N.; Morgenstern, L.B. Population-Based Analysis of the Impact of Expanding the Time Window for Acute Stroke Treatment. Stroke 2007, 38, 3213–3217. [Google Scholar] [CrossRef]
- Zhou, Y.; Yan, S.; Song, X.; Gong, Y.; Li, W.; Wang, M.; Yin, X.; Hu, B.; Lu, Z. Intravenous thrombolytic therapy for acute ischemic stroke in Hubei, China: A survey of thrombolysis rate and barriers. BMC Neurol. 2019, 19, 1–9. [Google Scholar] [CrossRef]
- de Sousa, D.A.; von Martial, R.; Abilleira, S.; Gattringer, T.; Kobayashi, A.; Gallofré, M.; Fazekas, F.; Szikora, I.; Feigin, V.; Caso, V.; et al. Access to and delivery of acute ischaemic stroke treatments: A survey of national scientific societies and stroke experts in 44 European countries. Eur. Stroke J. 2018, 4, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Lachkhem, Y.; Rican, S.; Minvielle, E. Understanding delays in acute stroke care: A systematic review of reviews. Eur. J. Public Health 2018, 28, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Foraker, R.E.; Morris, D.L.; Rosamond, W.D. A Comprehensive Review of Prehospital and In-Hospital Delay Times in Acute Stroke Care. Int. J. Stroke 2009, 4, 187–199. [Google Scholar] [CrossRef]
- Tong, D.; Reeves, M.J.; Hernandez, A.F.; Zhao, X.; Olson, D.W.M.; Fonarow, G.C.; Schwamm, L.H.; Smith, E.E. Times from symptom onset to hospital arrival in the get with the guidelines-stroke program 2002 to 2009: Temporal trends and implications. Stroke 2012, 43, 1912–1917. [Google Scholar] [CrossRef]
- Teuschl, Y.; Brainin, M. Stroke Education: Discrepancies among Factors Influencing Prehospital Delay and Stroke Knowledge. Int. J. Stroke 2010, 5, 187–208. [Google Scholar] [CrossRef] [PubMed]
- Xirasagar, S.; Tsai, M.-H.; Heidari, K.; Hardin, J.W.; Wu, Y.; Wronski, R.; Hurley, D.; Jauch, E.C.; Sen, S. Why acute ischemic stroke patients in the United States use or do not use emergency medical services transport? Findings of an inpatient survey. BMC Health Serv. Res. 2019, 19, 1–11. [Google Scholar] [CrossRef]
- Arrate, A.O.; Guerrero, M.F.; Maiztegi, C.F.; Calle, I.A.; Fernández, R.S.; Rodríguez, M.F.; Naveira, P.V.; Elena, A.A.; González, I.I.; Díez, Y.P.; et al. Utilización de transporte sanitario urgente por los pacientes con ictus isquémico e impacto en los tiempos de atención. Neurologia 2019, 34, 80–88. [Google Scholar] [CrossRef]
- Ekundayo, O.J.; Saver, J.L.; Fonarow, G.C.; Schwamm, L.H.; Xian, Y.; Zhao, X.; Hernandez, A.F.; Peterson, E.D.; Cheng, E.M. Patterns of Emergency Medical Services Use and Its Association With Timely Stroke Treatment. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 262–269. [Google Scholar] [CrossRef]
- Yin, X.; Yang, T.; Gong, Y.; Zhou, Y.; Li, W.; Song, X.; Wang, M.; Hu, B.; Lu, Z. Determinants of Emergency Medical Services Utilization Among Acute Ischemic Stroke Patients in Hubei Province in China. Stroke 2016, 47, 891–894. [Google Scholar] [CrossRef]
- Minnerup, J.; Wersching, H.; Unrath, M.; Berger, K. Effects of emergency medical service transport on acute stroke care. Eur. J. Neurol. 2014, 21, 1344–1347. [Google Scholar] [CrossRef] [PubMed]
- Price, C.I.; Rae, V.; Duckett, J.; Wood, R.; Gray, J.; McMeekin, P.; Rodgers, H.; Portas, K.; Ford, G.A. An Observational Study of Patient Characteristics Associated with the Mode of Admission to Acute Stroke Services in North East, England. PLoS ONE 2013, 8, e76997. [Google Scholar] [CrossRef]
- Kamel, H.; Navi, B.B.; Fahimi, J. National Trends in Ambulance Use by Patients With Stroke, 1997–2008. JAMA 2012, 307, 1026–1028. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Castillo, J.K.; Arista, M.C.; Barbarán, M.T.; Escobar, D.V. Factores asociados a la demora del tratamiento hospitalario de los pacientes con enfermedad cerebrovascular aguda. Rev. Neurol. 2007, 44, 264. [Google Scholar] [CrossRef]
- Nolte, C.H.; Rossnagel, K.; Jungehuelsing, G.J.; Müller-Nordhorn, J.; Roll, S.; Reich, A.; Willich, S.N.; Villringer, A. Gender differences in knowledge of stroke in patients with atrial fibrillation. Prev. Med. 2005, 41, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Bahnasy, W.S.; Ragab, O.A.A.; Elhassanien, M.E. Stroke onset to needle delay: Where these golden hours are lost? An Egyptian center experience. eNeurologicalSci 2019, 14, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Dhand, A.; Luke, D.; Lang, C.; Tsiaklides, M.; Feske, S.; Lee, J.-M. Social networks and risk of delayed hospital arrival after acute stroke. Nat. Commun. 2019, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- OECD. Romania: Country Health Profile 2019, State of Health in the EU; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Norrving, B.; Barrick, J.; Davalos, A.; Dichgans, M.; Cordonnier, C.; Guekht, A.; Kutluk, K.; Mikulik, R.; Wardlaw, J.; Richard, E.; et al. Action Plan for Stroke in Europe 2018–2030. Eur. Stroke J. 2018, 3, 309–336. [Google Scholar] [CrossRef] [PubMed]
- Fassbender, K.; Walter, S.; Grunwald, I.Q.; Merzou, F.; Mathur, S.; Lesmeister, M.; Liu, Y.; Bertsch, T.; Grotta, J.C. Prehospital stroke management in the thrombectomy era. Lancet Neurol. 2020, 19, 601–610. [Google Scholar] [CrossRef]
- Paul, C.L.; Ryan, A.; Rose, S.; Attia, J.R.; Kerr, E.; Koller, C.; Levi, C.R. How can we improve stroke thrombolysis rates? A review of health system factors and approaches associated with thrombolysis administration rates in acute stroke care. Implement. Sci. 2015, 11, 1–12. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Arrival ≤ 4.5 h after Stroke Onset (n = 243) | Arrival > 4.5 h after Stroke Onset (n = 416) | p Value | |
|---|---|---|---|
| Age, median (25–75 IQR) | 73.5 (64–81) | 72 (65–80) | 0.7 |
| Male sex | 111 (45.7%) | 206 (49.5%) | 0.3 |
| Higher education | 39 (16.04) | 81 (19.4) | 0.4 |
| Place of living and living status | |||
| Living in rural areas * | 58 (23.9%) | 130 (31.2%) | 0.04 |
| Living alone | 45 (18.9%) | 96 (24.1%) | 0.13 |
| Previous history | |||
| Prior stroke/TIA | 54 (22.2%) | 96 (23.1%) | 0.8 |
| Hypertension | 171 (70.4%) | 286 (68.7%) | 0.6 |
| Diabetes mellitus | 55 (22.6%) | 108 (25.9%) | 0.3 |
| Atrial fibrillation (previously diagnosed) * | 72 (29.6%) | 65 (15.6%) | <0.0001 |
| Ischemic heart disease * | 50 (20.6%) | 59 (14.2%) | 0.03 |
| Current smoking | 46 (19.3%) | 99 (23.9%) | 0.16 |
| Cognitive impairment | 27 (11.1%) | 49 (11.8%) | 0.8 |
| BMI ≥ 30 | 63 (25.9%) | 101 (24.3%) | 0.6 |
| Alcohol drinking | 43 (17.9%) | 84 (20.5%) | 0.4 |
| Previous therapy | |||
| Antiplatelets | 76 (31.5%) | 134 (32.7%) | 0.7 |
| Anticoagulants * | 44 (18.2%) | 44 (10.7%) | 0.006 |
| Antihypertensives | 149 (61.8%) | 231 (56.3%) | 0.17 |
| Statins | 66 (27.4%) | 102 (24.9%) | 0.5 |
| Previous level of dependence | 0.3 | ||
| mRS 0–1 | 166 (70.6%) | 280 (70.3%) | |
| mRS 2–3 | 38 (16.2%) | 78 (19.6%) | |
| mRS 4–5 | 31 (13.2%) | 40 (10.1%) | |
| Transport to hospital * | <0.0001 * | ||
| By ambulance | 208 (85.6%) | 282 (67.8%) | |
| By own means | 35 (14.4%) | 134 (32.2%) | |
| NIHSS at admission, median (25–75 IQR) * | 10 (5–19) | 5 (2–9) | <0.0001 * |
| Stroke severity * | <0.0001 * | ||
| NIHSS ≤ 5 | 74 (30.4%) | 239 (57.4%) | |
| NIHSS 6–15 | 87 (35.8%) | 120 (28.8%) | |
| NIHSS ≥ 16 | 82 (33.7%) | 57 (13.7%) | |
| Stroke territory * | <0.0001 * | ||
| Left MCA or ACA | 90 (37.2%) | 136 (32.7%) | |
| Right MCA or ACA | 97 (40.1%) | 114 (27.4%) | |
| Vertebro-basilar | 44 (18.2%) | 152 (36.5%) | |
| Multiple territories | 11 (4.5%) | 14 (3.4%) | |
| Stroke signs and symptoms | |||
| Altered level of consciousness | 34 (13.9%) | 41 (9.8%) | 0.13 |
| Hemianopsia * | 123 (50.6%) | 106 (25.7%) | <0.0001 |
| Facial palsy * | 183 (75.3%) | 222 (53.6%) | <0.0001 |
| Vertigo | 11 (4.5%) | 30 (7.2%) | 0.2 |
| Motor weakness * | 204 (83.9%) | 296 (71.3%) | 0.0002 |
| Ataxia * | 28 (11.6%) | 72 (17.3%) | 0.04 |
| Sensory disturbance * | 97 (39.9%) | 88 (21.5%) | <0.0001 |
| Speech disturbance | 180 (74.1%) | 236 (57%) | <0.0001 |
| Dysarthria * | 127 (52.3%) | 174 (42.1%) | |
| Aphasia | 53 (21.8%) | 62 (14.9%) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| p Value | OR (95% CI) | p Value | OR (95% CI) | |
| Living in rural areas | 0.04 | 1.4 (1–2.1) | NI | - |
| Atrial fibrillation (previously diagnosed) | <0.0001 | 0.4 (0.3–0.6) | 0.001 * | 0.5 (0.3–0.7) |
| Ischemic heart disease (previously diagnosed) | 0.03 | 0.6 (0.4–0.9) | NI | - |
| Prior treatment with anticoagulants | 0.007 | 0.5 (0.3–0.8) | NI | - |
| Transport to hospital by own means | <0.0001 | 2.8 (1.8–4.2) | 0.0003 * | 2.2 (1.4–3.6) |
| Stroke severity at admission | ||||
| NIHSS < 5 | Ref. | Ref. | Ref. | Ref. |
| NIHSS 5–15 | <0.0001 | 0.4 (0.3–0.6) | NI | NI |
| NIHSS ≥ 16 | <0.0001 | 0.2 (0.1–0.3) | 0.04 * | 0.6 (0.3–0.9) |
| Stroke territory (posterior vs. anterior) | <0.0001 | 2.6 (1.8–3.8) | 0.05 | 1.5 (0.9–2.3) |
| Hemianopsia | <0.0001 | 0.3 (0.2–0.5) | 0.03 * | 0.6 (0.4–0.9) |
| Facial palsy | <0.0001 | 0.4 (0.3–0.5) | 0.04 * | 0.6 (0.4–0.9) |
| Motor weakness | 0.0002 | 0.5 (0.3–0.7) | NI | - |
| Sensory disturbance | <0.0001 | 0.4 (0.3–0.6) | 0.0001* | 0.4 (0.3–0.6) |
| Speech disturbance | <0.0001 | 0.4 (0.3–0.6) | NI | - |
| Ataxia | 0.04 | 1.5 (1.01–2.5) | NI | - |
| Arrival ≤ 24 h after Stroke Onset (n = 545) | Arrival > 24 h after Stroke Onset (n = 221) | p Value | |
|---|---|---|---|
| Age, median (25–75 IQR) | 73 (64–81) | 72 (64–78) | 0.7 |
| Male sex | 274 (50.3%) | 101 (45.7%) | 0.2 |
| Higher education | 106 (19.4%) | 38 (17.2%) | 0.6 |
| Place of living and living status | |||
| Living in rural areas * | 139 (25.5%) | 74 (33.5%) | 0.02 |
| Living alone * | 100 (19.1%) | 58 (27.4%) | 0.01 |
| Previous history | |||
| Prior stroke/TIA | 120 (22.1%) | 55 (24.9%) | 0.4 |
| Hypertension | 383 (70.3%) | 153 (69.2%) | 0.7 |
| Diabetes mellitus | 131 (24.1%) | 61 (27.6%) | 0.3 |
| Atrial fibrillation (previously diagnosed) * | 128 (23.5%) | 32 (14.5%) | 0.005 |
| Ischemic heart disease | 94 (17.2%) | 30 (13.6%) | 0.2 |
| Current smoking | 121 (22.6%) | 48 (21.7) | 0.8 |
| Cognitive impairment | 57 (10.4%) | 29 (13.1%) | 0.3 |
| BMI ≥ 30 | 143 (26.2%) | 54 (24.4%) | 0.6 |
| Alcohol drinking | 108 (20.2%) | 41 (18.8%) | 0.6 |
| Previous therapy | |||
| Antiplatelets | 165 (30.6%) | 70 (32.1%) | 0.7 |
| Anticoagulants | 78 (14.5%) | 27 (12.4%) | 0.4 |
| Antihypertensives | 324 (60.1%) | 117 (53.6%) | 0.1 |
| Statins | 139 (25.8%) | 56 (25.7%) | 0.9 |
| Previous level of dependence | 0.7 | ||
| mRS 0–1 | 357 (67.9%) | 149 (70.9%) | |
| mRS 2–3 | 104 (19.8%) | 39 (18.6%) | |
| mRS 4–5 | 65 (12.4%) | 22 (10.5%) | |
| Transport to hospital * | <0.0001 | ||
| By ambulance | 445 (81.6%) | 133 (60.2%) | |
| By own means | 100 (18.4%) | 88 (39.8%) | |
| NIHSS score at admission, median (25–75 IQR) * | 7 (4–16) | 4 (2–8) | <0.0001 |
| Stroke severity * | <0.0001 | ||
| NIHSS ≤ 5 | 215 (39.4%) | 137 (61.9%) | |
| NIHSS 6–15 | 182 (33.4%) | 61 (27.6%) | |
| NIHSS ≥ 16 | 148 (27.2%) | 23 (10.4%) | |
| Stroke territory * | 0.0001 | ||
| Left MCA or ACA | 201 (36.9%) | 68 (30.8%) | |
| Right MCA or ACA | 188 (34.5%) | 55 (24.9%) | |
| Vertebro-basilar | 134 (24.6%) | 91 (41.2%) | |
| Multiple territories | 21 (3.8%) | 7 (3.2%) | |
| Stroke signs and symptoms | |||
| Altered level of consciousness | 72 (13.2%) | 20 (9.1%) | 0.1 |
| Hemianopsia * | 223 (40.9%) | 48 (21.9%) | <0.0001 |
| Facial palsy * | 375 (68.9%) | 106 (48.2%) | <0.0001 |
| Vertigo | 33 (6.1%) | 16 (7.3%) | 0.5 |
| Motor weakness * | 436 (80%) | 150 (68.2%) | 0.0004 |
| Ataxia * | 69 (12.7%) | 42 (19%) | 0.02 |
| Sensory disturbance * | 169 (31.12%) | 50 (22.7%) | 0.02 |
| Speech disturbance | 393 (72.2%) | 106 (48.2%) | <0.0001 |
| Dysarthria * | 292 (53.7%) | 78 (35.5%) | |
| Aphasia | 101 (18.5%) | 28 (12.7%) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| p Value | OR (95% CI) | p Value | OR (95% CI) | |
| Living alone | 0.01 | 1.6 (1.1–2.3) | 0.001 * | 1.7 (1.8–2.6) |
| Living in rural area | 0.02 | 1.5 (1.1–2.1) | 0.04 * | 1.4 (1.01–2.1) |
| Atrial fibrillation | 0.005 | 0.5 (0.3–0.8) | 0.03 * | 0.6 (0.4–0.9) |
| Transport to hospital by ambulance | <0.0001 | 0.3 (0.2–0.4) | <0.0001 * | 0.4 (0.3–0.6) |
| Stroke severity at admission | ||||
| NIHSS ≤ 5 | Ref. | Ref. | Ref. | Ref. |
| NIHSS 6–15 | 0.001 | 1.9 (1.2–2.8) | NI | NI |
| NIHSS ≥ 16 | <0.0001 | 4.1 (2.3–6.7) | 0.03 * | 0.5 (0.3–0.9) |
| Stroke territory (posterior vs. anterior) | <0.0001 | 2.1 (1.5–2.9) | NS | NS |
| Hemianopsia | <0.0001 | 0.4 (0.2–0.5) | NI | NI |
| Facial palsy | <0.0001 | 0.4 (0.3–0.6) | NI | NI |
| Motor weakness | 0.0005 | 0.5 (0.3–0.7) | NI | NI |
| Sensory disturbance | 0.02 | 0.6 (0.4–0.9) | NS | NS |
| Speech disturbance | <0.0001 | 0.3 (0.2–0.4) | 0.002 * | 0.4 (0.3–0.7) |
| Ataxia | 0.02 | 0.6 (0.4–0.9) | NI | NI |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terecoasă, E.O.; Radu, R.A.; Negrilă, A.; Enache, I.; Cășaru, B.; Tiu, C. Pre-Hospital Delay in Acute Ischemic Stroke Care: Current Findings and Future Perspectives in a Tertiary Stroke Center from Romania—A Cross-Sectional Study. Medicina 2022, 58, 1003. https://doi.org/10.3390/medicina58081003
Terecoasă EO, Radu RA, Negrilă A, Enache I, Cășaru B, Tiu C. Pre-Hospital Delay in Acute Ischemic Stroke Care: Current Findings and Future Perspectives in a Tertiary Stroke Center from Romania—A Cross-Sectional Study. Medicina. 2022; 58(8):1003. https://doi.org/10.3390/medicina58081003
Chicago/Turabian StyleTerecoasă, Elena Oana, Răzvan Alexandru Radu, Anca Negrilă, Iulian Enache, Bogdan Cășaru, and Cristina Tiu. 2022. "Pre-Hospital Delay in Acute Ischemic Stroke Care: Current Findings and Future Perspectives in a Tertiary Stroke Center from Romania—A Cross-Sectional Study" Medicina 58, no. 8: 1003. https://doi.org/10.3390/medicina58081003
APA StyleTerecoasă, E. O., Radu, R. A., Negrilă, A., Enache, I., Cășaru, B., & Tiu, C. (2022). Pre-Hospital Delay in Acute Ischemic Stroke Care: Current Findings and Future Perspectives in a Tertiary Stroke Center from Romania—A Cross-Sectional Study. Medicina, 58(8), 1003. https://doi.org/10.3390/medicina58081003