
The Need for Standardizing Diagnosis, Treatment and Clinical Care of Cholecystitis and Biliary Colic in Gallbladder Disease

 , ,
, , 
Abstract
1. Introduction
2. Pathophysiology and Risk Factors
3. The Burden of Gallbladder Diseases
4. Symptoms and Diagnosis
4.1. Physical Presentation
4.2. Haematology
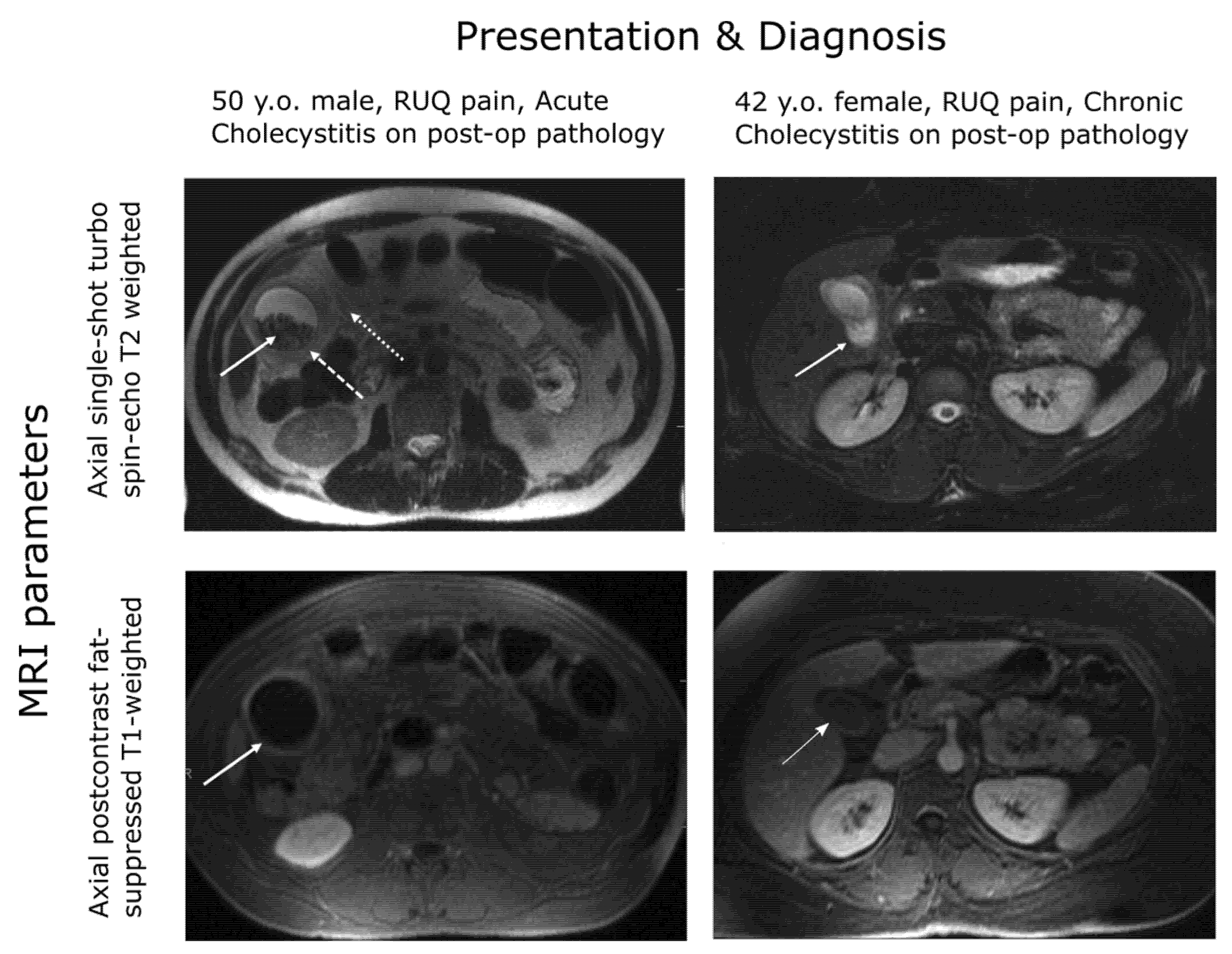
4.3. Imaging
5. Treatment and Outcomes
6. Surgical Risk Factors
7. Healthcare Delivery
8. Discussion
- (1)
- The consensus-framed, evidence-based approach taken to diagnosis and treatment of acute cholecystitis should be extended to consider the case definition and aetiology of the related pathologies of biliary colic and chronic cholecystitis.
- (2)
- This approach should have regard for operative findings and a patient’s clinical history. Furthermore, they should ideally assess the potential for biochemical or genetic markers to stratify patients according to their operative findings.
- (3)
- High-quality evidence should be accumulated on the potential of imaging technologies, leveraging the use of MRI and MRCP that is now commonplace in many health systems.
- (1)
- The relevance to practice of any derived classification of GD;
- (2)
- Facilitating optimisation of the treatment pathway, undertaken on exclusion of the urgent pathologies of acute cholecystitis and common bile duct obstruction;
- (3)
- A better understanding of the relationship between acute and chronic forms of GD and the implications of this for resource allocation.
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
List of Abbreviations
| AAFPI | American Academy of Family Physicians |
| ABCG5/G8 | ATP-binding cassette sub-family G member 5/member 8 |
| AC | Acute cholecystitis |
| ALT | Alanin transminase |
| ASA-PS | American Society of Anesthesiologists Physical Status |
| AST | Asparate transaminase |
| AUC | Area under the curve |
| BC | Biliary colic |
| BMI | Body mass index |
| CBD | Common bile duct |
| CCI | Charlson comorbidity index |
| CRP | C-reactive protein |
| CT | Computed tomography |
| DAS | Dutch Association of Surgery |
| ERCP | Endoscopic retrograde cholangiography |
| ES | Endoscopic sphincterotomy |
| GD | Gallbladder |
| HCV | Hepatitis C virus |
| HDL | High-density lipoprotein |
| HIDA | Hepatobiliary iminodiacetic acid |
| IDDM | Insulin-dependent diabetes mellitus |
| LC | Laparoscopic cholecystectomy |
| LDL | Low-density lipoprotein |
| MRCP | Magnetic resonance cholangiography |
| MS | Metabolic syndrome |
| NAFLD | Non-alcoholic ratty liver disease |
| NIDDM | Non-insulin-dependent diabetes mellitus |
| OR | Odds ratio |
| PCGBD | Percutaneous gallbladder drainage |
| PROM | Patient-reported outcome measures |
| PT-INR | Prothrombin time test—international normalized ratio |
| ROC | Receiver operator characteristic |
| TG07F | Tokyo Guidelines 2007 |
| TG18 | Tokyo Guidelines 2018 |
| WCC | White blood cell count |
References
- Jones, M.W.; Deppen, J.G. Open Cholecystectomy. [Updated 27 April 2020]. In StatPearls [Internet]; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Warttig, S.; Ward, S.; Rogers, G. Diagnosis and management of gallstone disease: Summary of NICE guidance. BMJ 2014, 349, 6241. [Google Scholar] [CrossRef] [PubMed]
- Sanders, G.; Kingsnorth, A.N. Gallstones. BMJ 2007, 335, 295–299. [Google Scholar] [CrossRef] [PubMed]
- NICE, National Institute for Health and Care Excellence. Costing Statement: Gallstone Disease. Implementing the NICE Guideline on Gallstone Disease (CG188). 2014. Available online: https://www.nice.org.uk/guidance/cg188/resources/costing-statement-pdf-193298365; https://web.archive.org/web/20200810153323/ (accessed on 4 February 2020).
- NICE, National Institute for Health and Care Excellence. Gallstone Disease: Diagnosis and Gallstone Disease: Diagnosis and Management [Online]. 2014. Available online: http://www.nice.org.uk/guidance/cg188 (accessed on 9 February 2022).
- Lammert, F.; Neubrand, M.W.; Bittner, R.; Feussner, H.; Greiner, L.; Hagenmüller, F.; Kiehne, K.H.; Ludwig, K.; Neuhaus, H.; Paumgartner, G.; et al. S3-guidelines for diagnosis and treatment of gallstones. German Society for Digestive and Metabolic Diseases and German Society for Surgery of the Alimentary, Tract. Z. Gastroenterol. 2007, 45, 971–1001. [Google Scholar] [CrossRef] [PubMed]
- Godrey, P.J.; Bates, T.; Harrison, M.; King, M.B.; Padley, N.R. Gall stones and mortality: A study of all gall stone related deaths in a single health district. Gut 1984, 25, 1029–1033. [Google Scholar] [CrossRef]
- Di Ciaula, A.; Wang, D.Q.H.; Portincasa, P. An update on the pathogenesis of cholesterol gallstone disease. Curr. Opin. Gastroenterol. 2018, 34, 71–80. [Google Scholar] [CrossRef]
- Lammert, F.; Acalovschi, M.; Ercolani, G.; van Erpecum, K.J.; Gurusamy, K.; van Laarhoven, C.J.; Portincasa, P. EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J. Hepatol. 2015, 65, 146–181. [Google Scholar]
- Nervi, F.; Duarte, I.; Gómez, G.; Rodríguez, G.; Pino, G.D.; Ferrerio, O.; Covarrubias, C.; Valdivieso, V.; Torres, M.I.; Urzúa, A. Frequency of gallbladder cancer in Chile, a high-risk area. Int. J. Cancer 1988, 41, 657–660. [Google Scholar] [CrossRef]
- Katsika, D.; Grjobovski, A.; Einarsson, C.; Lammert, F.; Lichtenstein, P.; Marschall, H.U. Gentic and environmental influences on symptomatic gallstone disease: A Swedish study of 43,141 twin pairs. Hepatology 2005, 41, 1138–1143. [Google Scholar] [CrossRef]
- Bohr, U.R.; Kuester, D.; Meyer, F.; Wex, T.; Stillert, M.; Csepregi, A.; Lippert, H.; Roessner, A.; Malfertheiner, P. Low prevalence of Helicobacteraceae in gall-stone disease and gall-bladder carcinoma in the German population. Clin. Microbiol. Infect. 2007, 13, 525–531. [Google Scholar] [CrossRef]
- Ruhl, C.E.; Everhart, J.E. Gallstone disease is associated with increased mortality in the United States. Gastroenterology 2013, 140, 508–516. [Google Scholar] [CrossRef]
- Kratzer, W.; Mason, R.A. Prevalence of gallstones in sonographic surveys worldwide. J. Clin. Ultrasound 1999, 27, 1–7. [Google Scholar] [CrossRef]
- Health Information and Quality Authority. Health Technology Assessment of Scheduled Procedures. Referral Thresholds for Adult Patients Suspected of Having Gallstone Disease; Health Information and Quality Authority: Dublin, Ireland, 2014. [Google Scholar]
- Busse, R.; Geissler, A.; Quentin, W.; Wiley, M. Diagnosis Related Groups in Europe: Moving towards Transparency, Efficiency and Quality in Hospitals; Open University Press: Maidenhead, UK, 2011. [Google Scholar]
- Ahmed, M.; Diggory, R. The Correlation between Ultrasonography and Histology in the Search for Gallstones. Ann. R. Coll. Surg. Engl. 2011, 93, 81–83. [Google Scholar] [CrossRef] [PubMed]
- Gutt, C.; Jenssen, C.; Barreiros, A.P.; Götze, T.O.; Stokes, C.S.; Jansen, P.L.; Neubrand, M.; Lammert, F. Updated S3-Guideline for Prophylaxis, Diagnosis and Treatment of Gallstones. German Society for Digestive and Metabolic Diseases (DGVS) and German Society for Surgery of the Alimentary Tract (DGAV)-AWMF Registry 021/008. Z. Gastroenterol. 2018, 56, 912–966. [Google Scholar] [PubMed]
- Ellis, H.; Calne, R.; Watson, C. Lecture Notes on General Surgery, 10th ed.; Blackwell Science: Oxford, UK, 2002; pp. 194–260. [Google Scholar]
- Wang, L.; Chen, J.; Jiang, W.; Cen, L.; Pan, J.; Yu, C.; Li, Y.; Chen, W.; Chen, C.; Shen, Z. The Relationship between Helicobacter pylori Infection of the Gallbladder and Chronic Cholecystitis and Cholelithiasis: A Systematic Review and Meta-Analysis. Can. J. Gastroenterol. Hepatol. 2021, 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Small, D.M. Cholesterol Nucleation and Growth in Gallstone Formation. N. Engl. J. Med. 1980, 302, 1305–1307. [Google Scholar] [CrossRef]
- Paumgartner, G.; Greenberger, N. Gallstone disease. In Current Diagnosis and Treatment: Gastroenterology, Hepatology, Endoscopy; Greenberger, N., Blumberg, R.S., Burakoff, R., Eds.; McGraw-Hill: New York, NY, USA, 2009; pp. 537–546. [Google Scholar]
- Watterson, S.; Guerriero, M.L.; Blanc, M.; Mazein, A.; Loewe, L.; Robertson, K.A.; Gibbs, H.; Shui, G.; Wenk, M.R.; Hillston, J.; et al. A model of flux regulation in the cholesterol biosynthesis pathway: Immune mediated graduated flux reduction versus statin-like led stepped flux reduction. Biochimie 2013, 95, 613–621. [Google Scholar] [CrossRef]
- Benson, H.; Watterson, S.; Sharman, J.L.; Mpamhanga, C.P.; Parton, A.; Southan, C.; Harmar, A.J.; Ghazal, P. Is systems pharmacology ready to impact upon therapy development? A study on the cholesterol biosynthesis pathway. Br. J. Pharm. 2017, 174, 4362–4382. [Google Scholar] [CrossRef]
- Warren, T.; McAllister, R.; Morgan, A.; Rai, T.S.; McGilligan, V.; Ennis, M.; Page, C.; Kelly, C.; Peace, A.; Corfe, B.M.; et al. The Interdependency and Co-Regulation of the Vitamin D and Cholesterol Metabolism. Cells 2021, 10, 2007. [Google Scholar] [CrossRef]
- Buhman, K.; Accad, M.; Novak, S.; Choi, R.S.; Wong, J.S.; Hamilton, R.L.; Turley, S.; Farese, R.V. Resistance to diet-induced hypercholesterolemia and gallstone formation in ACAT2-deficient mice. Nat. Med. 2000, 6, 1341–1347. [Google Scholar] [CrossRef]
- Wang, H.H.; Portincasa, P.; Mendez-Sanchez, N.; Uribe, M.; Wang, D.Q. Effect of ezetimibe on the prevention and dissolution of cholesterol gallstones. Gastroenterology 2008, 134, 2101–2110. [Google Scholar] [CrossRef]
- Levy, P.F.; Smith, B.F.; LaMont, J. Human gallbladder mucin accelerates nucleation of cholesterol in artificial bile. Gastroenterology 1984, 87, 270–275. [Google Scholar] [CrossRef]
- Portincasa, P.; Moschetta, A.; Palasciano, G. Cholesterol gallstone disease. Lancet 2016, 368, 230–239. [Google Scholar] [CrossRef]
- Wittenburg, H. Hereditary liver disease: Gallstones. Best Pract. Res. Clin. Gastroenterol. 2010, 24, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Portincasa, P.; Van Erpecum, K.J.; Vanberge-Henegouwen, G.P. Cholesterol crystallisation in bile. Gut 1997, 41, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Van Erpecum, K.J.; Van Berge-Henegouwen, G.P. Gallstones: An intestinal disease? Gut 1999, 44, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.; Nomura, A.; Stemmermann, G.N.; Chyou, P.H. Prospective study of clinical gallbladder disease and its association with obesity, physical activity, and other factors. Dig. Dis. Sci. 1992, 37, 784–790. [Google Scholar] [CrossRef]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Acalovschi, M.; Buzas, C.; Radu, C.; Grigorescu, M. Hepatitis C virus infection is a risk factor for gallstone disease: A prospective hospital-based study of patients with chronic viral C hepatitis. J. Viral Hepat. 2009, 16, 860–866. [Google Scholar] [CrossRef]
- Bini, E.J.; McGready, J. Prevalence of gallbladder disease among persons with hepatitis C virus infection in the United States. Hepatology 2005, 41, 1029–1036. [Google Scholar] [CrossRef]
- Everhart, J.E.; Khare, M.; Hill, M.; Maurer, K.R. Prevalence and ethic differences in gallbladder disease in the United States. Gastorenterology 1999, 117, 632–639. [Google Scholar] [CrossRef]
- Paigen, B.; Carey, M.C. Gallstones. In The Genetic Basis of Common Diseases, 2nd ed.; King, R.A., Rotter, J.I., Motulsky, A.G., Eds.; Oxford Univesity Press: Oxford, UK, 2002. [Google Scholar]
- Lammert, F.; Carey, M.C.; Paigen, B. Chromosomal organization of candidate genes involved in cholesterol gallstone formation: A murine gallstone map. Gastroenterology 2001, 120, 221–238. [Google Scholar] [CrossRef] [PubMed]
- Nakeeb, A.; Comuzzie, A.G.; Martin, L.; Sonnenberg, G.E.; Swartz-Basile, D.; Kissebah, A.H.; Pitt, H.A. Gallstones: Genetics versus environment. Ann. Surg. 2002, 235, 842. [Google Scholar] [CrossRef] [PubMed]
- Lyons, M.A.; Wittenburg, H. Cholesterol Gallstone Susceptibility Loci: A Mouse Map, Candidate Gene Evaluation, and Guide to Human LITH Genes. Gastroenterology 2006, 131, 1943–1970. [Google Scholar] [CrossRef] [PubMed]
- Marschall, H.U.; Katsika, D.; Rudling, M.; Einarsson, C. The genetic background of gallstone formation: An update. Biochem. Biophys. Res. Commun. 2010, 396, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Van der Linden, W.; Lindelof, G. The familial occurrence of gallstone disease. Acta Genet. Basel 1965, 15, 159–164. [Google Scholar] [CrossRef]
- Van der Linden, W.; Simonson, N. Familial occurrence of gallstone disease: Incidence in parents of young patients. Hum. Hered. 1973, 23, 123–127. [Google Scholar] [CrossRef]
- Gilat, T.; Feldman, C.; Halpern, Z.; Dan, M.; Bar-Meir, S. An Increased Familial Frequency of Gallstones. Gastroenterology 1983, 84, 242–246. [Google Scholar] [CrossRef]
- Sarin, S.K.; Negi, V.S.; Dewan, R.; Sasan, S.; Saraya, A. High familial prevalence of gallstones in the first-degree relatives of gallstone patients. Hepatology 1995, 22, 138–141. [Google Scholar] [CrossRef]
- Harvald, B.; Hauge, M. A catamnestic investigation of Danish twins: A preliminary report. Dan. Med. Bull. 1956, 3, 151–158. [Google Scholar]
- Gustavsson, M.L.; Ung, K.A.; Nilsson, Å.; Jakobsson, E. Patients’ experiences of gallstone disease. Gastrointest. Nurs. 2011, 9, 23–27. [Google Scholar] [CrossRef]
- Lamberts, M.P.; Lugtenberg, M.; Rovers, M.; Roukema, A.J.; Drenth, J.P.H.; Westert, G.P.; Van Laarhoven, C.J.H.M. Persistent and de novo symptoms after cholecystectomy: A systematic review of cholecystectomy effectiveness. Surg. Endosc. 2012, 27, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Brazzelli, M.; Cruickshank, M.; Kilonzo, M.; Ahmed, I.; Stewart, F.; McNamee, P.; Elders, A.; Fraser, C.; Avenell, A.; Ramsay, C. Clinical effectiveness and cost-effectiveness of cholecystectomy compared with observation/conservative management for preventing recurrent symptoms and complications in adults presenting with uncomplicated symptomatic gallstones or cholecystitis: A systematic review and economic evaluation. Health Technol. Assess. 2014, 18, 1–102. [Google Scholar] [PubMed]
- Ahmed, I.; Innes, K.; Brazzelli, M.; Gillies, K.; Newlands, R.; Avenell, A.; Hernández, R.; Blazeby, J.; Croal, B.; Hudson, J.; et al. Protocol for a randomised controlled trial comparing laparoscopic cholecystectomy with observation/conservative management for preventing recurrent symptoms and complications in adults with uncomplicated symptomatic gallstones (C-Gall trial). BMJ Open 2021, 11, e039781. [Google Scholar] [CrossRef] [PubMed]
- Wanjura, V.; Sandblom, G. How do quality-of-life and gastrointestinal symptoms differ between post-cholecystectomy patients and the background population? World J. Surg. 2016, 40, 81–88. [Google Scholar] [CrossRef]
- Wanjura, V. Register-Based Studies on Cholecystectomy: Quality of Life after Cholecystectomy, and Cholecystectomy Incidence and Complications after Gastric Bypass. Doctoral Dissertation, Örebro University, Orebro, Sweden, 2017. [Google Scholar]
- Daliya, P.; Gemmill, E.H.; Lobo, D.N.; Parsons, S.L. A systematic review of patient reported outcome measures (PROMs) and quality of life reporting in patients undergoing laparoscopic cholecystectomy. Hepatobiliary Surg. Nutr. 2019, 8, 228. [Google Scholar] [CrossRef]
- Everhart, J.E. Gallstones. In Digestive Diseases in the United States: Epidemiology and Impact; Everhart, J.E., Ed.; US Government Printing Office: Washington, DC, USA, 1994. [Google Scholar]
- Scott, J.W.; Olufajo, O.A.; Brat, G.A.; Rose, J.A.; Zogg, C.K.; Haider, A.H.; Salim, A.; Havens, J.M. Use of national burden to define operative emergency general surgery. JAMA Surg. 2016, 151, e160480. [Google Scholar] [CrossRef]
- Everhart, J.E.; Ruhl, C.E. Burden of digestive diseases in the United States Part III: Liver, biliary tract, and pancreas. Gastroenterology 2009, 136, 1134–1144. [Google Scholar] [CrossRef]
- Rome Group for Epidemiology and Prevention of Cholelithiasis. The epidemiology of gallstone disease in Rome, Italy. Part II. Factors associated with the disease. Hepatology 1988, 8, 907–913. [Google Scholar] [CrossRef]
- De Boer, E.; Boerma, D.; Van Erpecum, K.; Hermans, J.; Lamberts, M.; Rauws, E. Gallstone (Galsteen). 2017, pp. 68–69. Available online: https://www.mdl.nl/sites/www.mdl.nl/files/richlijnen/Galsteenlijden%20-%20definitief.pdf (accessed on 12 February 2021).
- Van Dijk, A.H. Evidence based medicine in complicated and uncomplicated gallstone disease. Ph.D. Thesis, University of Amsterdam, Amsterdam, The Netherlands, 2018. Available online: https://hdl.handle.net/11245.1/651f49ee-f507-4f1c-bdf6-61631fbd7e43 (accessed on 16 February 2022).
- Bellows, C.F.; Berger, D.H.; Crass, R.A. Management of gallstones. Am. Fam. Physician 2005, 72, 637–642. [Google Scholar]
- Takada, T.; Kawarada, Y.; Nimura, Y.; Yoshida, M.; Mayumi, T.; Sekimoto, M.; Miura, F.; Wada, K.; Hirota, M.; Yamashita, Y.; et al. Background: Tokyo Guidelines for the management of acute cholangitis and cholecystitis. J. Hepato-Biliary-Pancreat. Surg. 2007, 14, 1–10. [Google Scholar] [CrossRef]
- Hirota, M.; Takada, T.; Kawarada, Y.; Nimura, Y.; Miura, F.; Hirata, K.; Mayumi, T.; Yoshida, M.; Strasberg, S.; Pitt, H.; et al. Diagnostic criteria and severity assessment of acute cholecystitis: Tokyo Guidelines. J. Hepato-Biliary-Pancreat. Surg. 2007, 14, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Takada, T.; Kawarada, Y.; Nimura, Y.; Hirota, M.; Miura, F.; Mayumi, T.; Yoshida, M.; Strasberg, S.; Pitt, H.A.; et al. Surgical treatment of patients with acute cholecystitis: Tokyo Guidelines. J. Hepato-Biliary-Pancreat. Surg. 2007, 14, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Miura, F.; Takada, T.; Kawarada, Y.; Nimura, Y.; Wada, K.; Hirota, M.; Nagino, M.; Tsuyuguchi, T.; Mayumi, T.; Yoshida, M.; et al. Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines. J. Hepato-Biliary-Pancreat. Surg. 2007, 14, 27–34. [Google Scholar] [CrossRef]
- Yokoe, M.; Hata, J.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Wakabayashi, G.; Kozaka, K.; Endo, I.; Deziel, D.J.; Miura, F.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholecystitis (with videos). J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.B. The diagnosis of gallstones. Am. Med. News 1903, 82, 825–833. [Google Scholar]
- Trowbridge, R.L.; Rutkowski, N.K.; Shojania, K.G. Does this patient have acute cholecystitis? JAMA 2003, 289, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Yokoe, M.; Takada, T.; Strasberg, S.M.; Solomkin, J.; Mayumi, T.; Gomi, H.; Pitt, H.A.; Garden, O.J.; Kiriyama, S.; Hata, J.; et al. TG13 diagnostic criteria and severity grading of acute cholecystitis (with videos). J. Hepato-Biliary-Pancreat. Sci. 2013, 20, 35–46. [Google Scholar] [CrossRef]
- Gurbulak, E.K.; Gurbulak, B.; Akgun, I.E.; Duzkoylu, Y.; Battal, M.; Celayir, M.F.; Demir, U. Prediction of the Grade of Acute Cholecystitis by Plasma Level of C-Reactive Protein. Iran. Red Crescent Med. J. 2015, 17, e28091. [Google Scholar] [CrossRef]
- Beliaev, A.M.; Marshall, R.J.; Booth, M. C-reactive protein has a better discriminative power than white cell count in the diagnosis of acute cholecystitis. J. Surg. Res. 2015, 198, 66–72. [Google Scholar] [CrossRef]
- Smith, J. Biliary Colic & Cholecystitis. 2021. Available online: http://www.jjs.me.uk/teaching/gallbladder.html (accessed on 12 February 2021).
- NICE, National Institute for Health and Clinical Excellence. Guideline Development Group Pre-Operative Tests. The Use of Pre-Operative Tests for Elective Surgery: Evidence, Methods and Guidance 2003; NICE: London, UK, 2003. [Google Scholar]
- Biesterveld, B.E.; Alam, H.B.; Kronick, S.L.; Pomerantz, B.; Repaskey, W.T.; Rice, M.D.; Evaluation and management of gallstone-related diseases in non-pregnant adults. Ann Arbor (MI): Michigan Medicine, University of Michigan 2020. Available online: http://www.ncbi.nlm.nih.gov/books/NBK569245 (accessed on 16 February 2022).
- Pinto, A.; Reginelli, A.; Cagini, L.; Coppolino, F.; Ianora, A.A.S.; Bracale, R.; Giganti, M.; Romano, L. Accuracy of ultrasonography in the diagnosis of acute calculous cholecystitis: Review of the literature. Crit. Ultrasound J. 2013, 5 (Suppl. S1), S11. [Google Scholar] [CrossRef]
- Nino-Marcia, M.; Jeffrey, R.B. Imaging the patient with right upper quadrant pain. Semin. Roentgenol. 2001, 36, 81–91. [Google Scholar] [CrossRef]
- Kaura, S.H.; Haghighi, M.; Matza, B.W.; Hajdu, C.H.; Rosenkrantz, A.B. Comparison of CT and MRI findings in the differentiation of acute from chronic cholecystitis. Clin. Imaging 2013, 37, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Shea, J.A.; Berlin, J.A.; Escarce, J.J.; Clarke, J.R.; Kinosian, B.P.; Cabana, M.D.; Tsai, W.W.; Horangic, N.; Malet, P.F.; Schwartz, J.S.; et al. Revised estimates of diagnostic test sensitivity and specificity in suspected biliary tract disease. Arch. Intern. Med. 1994, 154, 2573–2581. [Google Scholar] [CrossRef] [PubMed]
- Kiewiet, J.J.; Leeuwenburgh, M.M.; Bipat, S.; Bossuyt, P.M.; Stoker, J.; Boermeester, M.A. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology 2012, 264, 708–720. [Google Scholar] [CrossRef] [PubMed]
- Yokoe, M.; Takada, T.; Mayumi, T.; Yoshida, M.; Hasegawa, H.; Norimizu, S.; Hayashi, K.; Umemura, S.; Orito, E. Accuracy of the Tokyo Guidelines for the diagnosis of acute cholangitis and cholecystitis taking into consideration the clinical practice pattern in Japan. J. Hepato-Biliary-Pancreat. Sci. 2011, 18, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.; Marsh, I.; Doyle, J. Does ultrasonography accurately diagnose acute cholecystitis? Improving diagnostic accuracy based on a review at a regional hospital. Can. J. Surg. 2014, 57, 162. [Google Scholar] [CrossRef]
- Pereira, J.; Bass, G.A.; Mariani, D.; Dumbrava, B.D.; Casamassima, A.; Da Silva, A.R.; Pinheiro, L.; Martinez-Casas, I.; Zago, M. Surgeon-performed point-of-care ultrasound for acute cholecystitis: Indications and limitations: A European Society for Trauma and Emergency Surgery (ESTES) consensus statement. Eur. J. Trauma Emerg. Surg. 2020, 46, 173–183. [Google Scholar] [CrossRef]
- Bree, R.L. Further observations on the usefulness of the sonographic Murphy sign in the evaluation of suspected acute cholecystitis. J. Clin. Ultrasound 1995, 23, 169–172. [Google Scholar] [CrossRef]
- Gutt, C.; Schläfer, S.; Lammert, F. The treatment of gallstone disease. Dtsch Arztebl. Int. 2020, 117, 148–158. [Google Scholar] [CrossRef]
- Buxbaum, J.L.; Fehmi, S.M.; Sultan, S.; Fishman, D.S.; Qumseya, B.J.; Cortessis, V.K.; Schilperoort, H.; Kysh, L.; Matsuoka, L.; Yachimski, P.; et al. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis. Gastrointest. Endosc. 2019, 89, 1075–1105. [Google Scholar] [CrossRef]
- Manes, G.; Paspatis, G.; Aabakken, L.; Anderloni, A.; Arvanitakis, M.; Ah-Soune, P.; Barthet, M.; Domagk, D.; Dumonceau, J.-M.; Gigot, J.-F.; et al. Endoscopic management of common bile duct stones: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy 2019, 51, 472–491. [Google Scholar] [CrossRef] [PubMed]
- Dolan, J.P.; Diggs, B.S.; Sheppard, B.C.; Hunter, J.G. Ten-year trend in the national volume of bile duct injuries requiring operative repair. Surg. Endosc. 2005, 19, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Bingener-Casey, J.; Richards, M.L.; Strodel, W.E.; Schwesinger, W.H.; Sirinek, K.R. Reasons for conversion from laparoscopic to open cholecystectomy: A 10-year review. J. Gastrointest. Surg. 2002, 6, 800–805. [Google Scholar] [CrossRef]
- Overby, D.W.; Apelgren, K.N.; Richardson, W.; Fanelli, R. SAGES guidelines for the clinical application of laparoscopic biliary tract surgery. Surg. Endosc. 2010, 24, 2368–2386. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, K.; Suzuki, K.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Endo, I.; Iwashita, Y.; Hibi, T.; Pitt, H.A.; Umezawa, A.; et al. Tokyo Guidelines 2018: Flowchart for the management of acute cholecystitis. J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 55–72. [Google Scholar] [CrossRef]
- Shea, J.A.; Healey, M.J.; Berlin, J.A.; Clarke, J.R.; Malet, P.F.; Staroscik, R.N.; Schwartz, J.S.; Williams, S.V. Mortality and complications associated with laparoscopic cholecystectomy. A meta-analysis. Ann. Surg. 1996, 224, 609. [Google Scholar] [CrossRef]
- David, G.G.; Al-Sarira, A.A.; Willmott, S.; Deakin, M.; Corless, D.J.; Slavin, J.P. Management of acute gallbladder disease in England. Br. J. Surg. 2008, 95, 472–476. [Google Scholar] [CrossRef]
- Gurusamy, K.; Samraj, K.; Gluud, C.; Wilson, E.; Davidson, B.R. Meta-analysis of randomized controlled trials on the safety and effectiveness of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br. J. Surg. 2009, 97, 141–150. [Google Scholar] [CrossRef]
- Kum, C.K.; Eypasch, E.; Lefering, R.; Paul, A.; Neugebauer, E.; Troidl, H. Laparoscopic cholecystectomy for acute cholecystitis: Is it really safe? World J. Surg. 1996, 20, 43–48. [Google Scholar] [CrossRef]
- Coccolini, F.; Catena, F.; Pisano, M.; Gheza, F.; Fagiouli, S.; Di Saverio, S.; Leandro, G.; Montori, G.; Ceresoli, M.; Corbella, D.; et al. Open versus laparoscopic cholecystectomy in acute cholecystitis. Systematic review and meta-analysis. Int. J. Surg. 2015, 18, 196–204. [Google Scholar] [CrossRef]
- Hosseini, S.N.; Mousavinasab, S.N.; Rahmanpour, H. Evaluate the outcome and identify predictive failure of outpatient laparoscopic cholecystectomy. JPMA J. Pak. Med. Assoc. 2009, 59, 452. [Google Scholar] [PubMed]
- Ansaloni, L.; Pisano, M.; Coccolini, F.; Peitzmann, A.B.; Fingerhut, A.; Catena, F.; Agresta, F.; Allegri, A.; Bailey, I.; Balogh, Z.J.; et al. 2016 WSES guidelines on acute calculous cholecystitis. World J Emerg Surg. 2016, 11, 25, Erratum in World J. Emerg. Surg. 2016, 11, 52. [Google Scholar] [CrossRef]
- Tan, J.K.; Goh, J.C.; Lim, J.W.; Shridhar, I.G.; Madhavan, K.; Kow, A.W. Same admission laparoscopic cholecystectomy for acute cholecystitis: Is the “golden 72 hours” rule still relevant? HPB 2017, 19, 47–51. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Krishna, S.G.; Kruger, A.J.; Patel, N.; Hinton, A.; Yadav, D.; Conwell, D.L. Cholecystectomy During Index Admission for Acute Biliary Pancreatitis Lowers 30-Day Readmission Rates. Pancreas 2018, 47, 996–1002. [Google Scholar] [CrossRef]
- Rffman, C.; Buchanan, J.; Allison, G. Charlson comorbidities index. J. Physiother. 2016, 62, 171. [Google Scholar] [CrossRef]
- Saklad, M. Grading of patients for surgical procedures. Anesthesiol. J. Am. Soc. Anesthesiol. 1941, 2, 281–284. [Google Scholar] [CrossRef]
- Daabiss, M. American Society of Anaesthesiologists physical status classification. Indian J. Anaesth. 2011, 55, 111. [Google Scholar] [CrossRef]
- Lee, R.; Ha, H.; Han, Y.S.; Kwon, H.J.; Ryeom, H.; Chun, J.M. Percutaneous transhepatic gallbladder drainage followed by elective laparoscopic cholecystectomy for patients with moderate to severe acute cholecystitis. Medicine 2017, 96, e8533. [Google Scholar] [CrossRef]
- Elmunzer, B.J.; Noureldin, M.; Morgan, K.A.; Adams, D.B.; Coté, G.A.; Waljee, A.K. The impact of cholecystectomy after endoscopic sphincterotomy for complicated gallstone disease. Am. J. Gastroenterol. 2017, 112, 1596. [Google Scholar] [CrossRef]
- Lin, W.-C.; Chang, C.-W.; Chu, C.-H. Percutaneous cholecystostomy for acute cholecystitis in high-risk elderly patients. Kaohsiung J. Med. Sci. 2016, 32, 518–525. [Google Scholar] [CrossRef]
- Brooks, K.R.; Scarborough, J.E.; Vaslef, S.N.; Shapiro, M.L. No need to wait: An analysis of the timing of cholecystectomy during admission for acute cholecystitis using the American College of Surgeons National Surgical Quality Improvement Program database. J. Trauma Acute Care Surg. 2013, 74, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Arellano, F.M.; Yood, M.U.; Wentworth, C.E.; Oliveria, S.A.; Rivero, E.; Verma, A.; Rothman, K.J. Use of cyclo-oxygenase 2 inhibitors (COX-2) and prescription non-steroidal anti-inflammatory drugs (NSAIDS) in UK and USA populations. Implications for COX-2 cardiovascular profile. Pharmacoepidemiol. Drug Saf. 2006, 15, 861–872. [Google Scholar] [CrossRef] [PubMed]
- De Mestral, C.; Laupacis, A.; Rotstein, O.D.; Hoch, J.S.; Haas, B.; Gomez, D.; Zagorsk, B.; Nathens, A.B. Early cholecystectomy for acute cholecystitis: A population-based retrospective cohort study of variation in practice. CMAJ Open 2013, 1, E62–E67. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Weeks, W.B.; Paraponaris, A.; Ventelou, B. Geographic variation in rates of common surgical procedures in France in 2008–2010, and comparison to the US and Britain. Health Policy 2014, 118, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Grimshaw, J.; Russell, I. Achieving health gain through clinical guidelines. I: Developing scientifically valid guidelines. Qual. Health Care 1993, 2, 243–248. [Google Scholar] [CrossRef]
- Sinha, S.; Hofman, D.; Stoker, D.L.; Friend, P.J.; Poloniecki, J.D.; Thompson, M.M.; Holt, P. Epidemiological study of provision of cholecystectomy in England from 2000 to 2009: Retrospective analysis of Hospital Episode Statistics. Surg. Endosc. 2012, 27, 162–175. [Google Scholar] [CrossRef]
- Harrison, E.M.; O’Neill, S.; Meurs, T.S.; Wong, P.L.; Duxbury, M.; Paterson-Brown, S.; Wigmore, S.J.; Garden, O.J. Hospital volume and patient outcomes after cholecystectomy in Scotland: Retrospective, national population based study. BMJ 2012, 344, e3330. [Google Scholar] [CrossRef]
- Tsai, T.C.; Joynt, K.E.; Orav, E.J.; Gawande, A.; Jha, A.K. Variation in Surgical-Readmission Rates and Quality of Hospital Care. N. Engl. J. Med. 2013, 369, 1134–1142. [Google Scholar] [CrossRef]
- Simopoulos, C.; Botaitis, S.; Polychronidis, A.; Tripsianis, G.; Karayiannakis, A.J. Risk factors for conversion of laparoscopic cholecystectomy to open cholecystectomy. Surg. Endosc. Other Interv. Tech. 2005, 19, 905–909. [Google Scholar] [CrossRef]
- Nassar, A.H.M.; Hodson, J.; Wijetunga, I.; Vohra, R.S.; Katbeh, T.; Zino, S.; Griffiths, E.A. Predicting the difficult laparoscopic cholecystectomy: Development and validation of a pre-operative risk score using an objective operative difficulty grading system. Surg. Endosc. 2019, 34, 1–13. [Google Scholar] [CrossRef]
- Griffiths, E.A.; West Midlands Research Collaborative; Hodson, J.; Vohra, R.S.; Marriott, P.; Katbeh, T.; Zino, S.; Nassar, A.H.M. Utilisation of an operative difficulty grading scale for laparoscopic cholecystectomy. Surg. Endosc. 2018, 33, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Sutcliffe, R.P.; Hollyman, M.; Hodson, J.; Bonney, G.; Vohra, R.S.; Griffiths, E.A.; Fenwick, S.; Elmasry, M.; Nunes, Q.; Kennedy, D.; et al. Preoperative risk factors for conversion from laparoscopic to open cholecystectomy: A validated risk score derived from a prospective UK database of 8820 patients. HPB 2016, 18, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Bharamgoudar, R.; Sonsale, A.; Hodson, J.; Griffiths, E. The development and validation of a scoring tool to predict the operative duration of elective laparoscopic cholecystectomy. Surg. Endosc. 2018, 32, 3149–3157. [Google Scholar] [CrossRef] [PubMed]
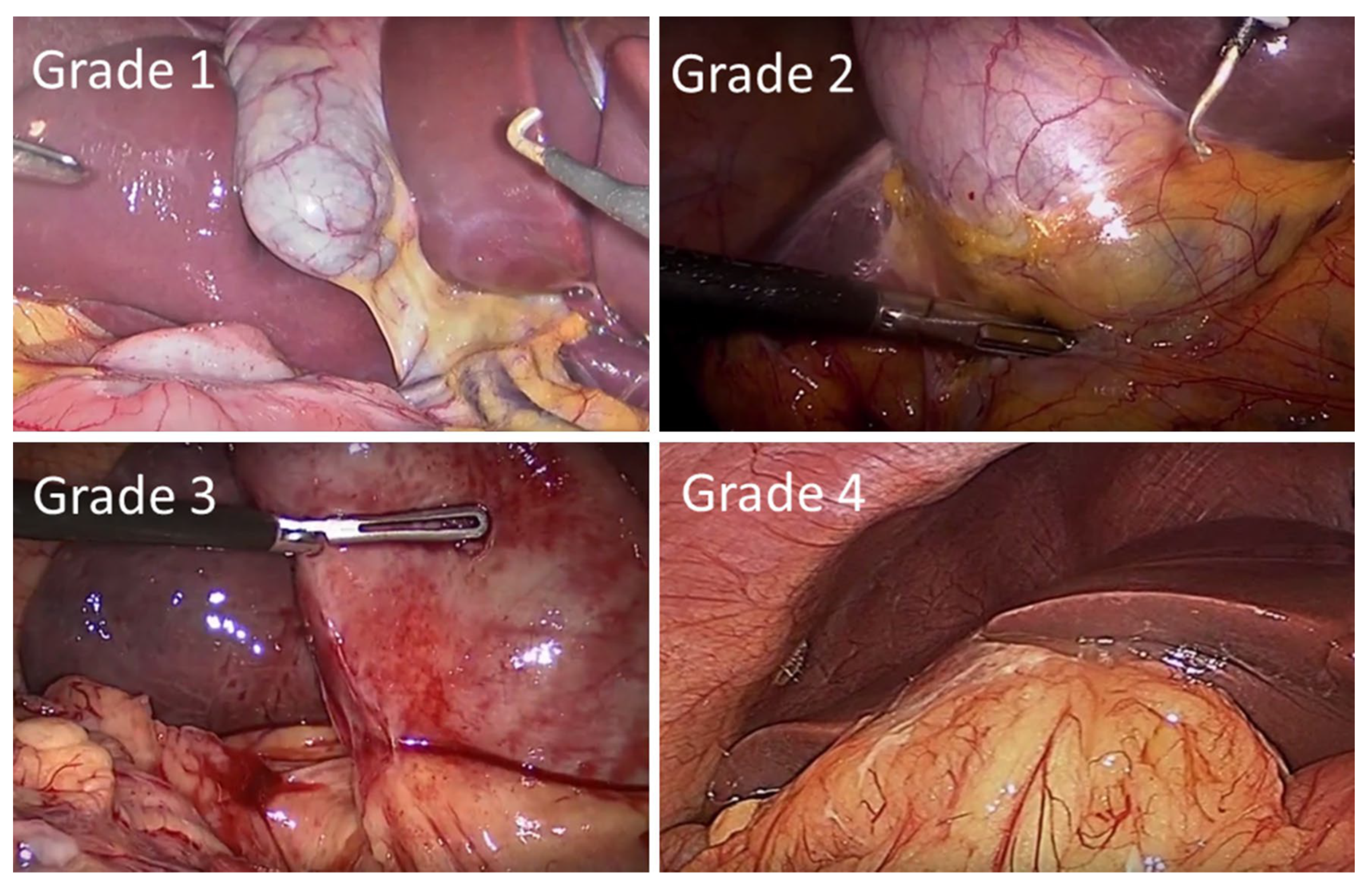
- Sugrue, M.; Sahebally, S.M.; Ansaloni, L.; Zielinski, M.D. Grading operative findings at laparoscopic cholecystectomy-a new scoring system. World J. Emerg. Surg. 2015, 10, 14. [Google Scholar] [CrossRef] [PubMed]
- Grocott, M.P.; Plumb, J.O.; Edwards, M.; Fecher-Jones, I.; Levett, D.Z. Re-designing the pathway to surgery: Better care and added value. Perioper. Med. 2017, 6, 9. [Google Scholar] [CrossRef]
- Lai, P.B.-S.; Kwong, K.H.; Leung, K.L.; Kwok, S.P.Y.; Chan, A.C.W.; Chung, S.C.S.; Lau, W.Y. Randomized trial of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br. J. Surg. 1998, 85, 764–767. [Google Scholar] [CrossRef]
- Chen, T.C.; Wanniarachige, D.; Murphy, S.; Lockhart, K.; O’Mahony, J. Surveying the Cost Effectiveness of the 20 Procedures with the Largest Public Health Services Waiting Lists in Ireland: Implications for Ireland’s Cost-Effectiveness Threshold. Value Health 2018, 21, 897–904. [Google Scholar] [CrossRef]
- Garner, J.P.; Sood, S.K.; Robinson, J.; Barber, W.; Ravi, K. The cost of ignoring acute cholecystectomy. Ann. R. Coll. Surg. Engl. 2009, 91, 39–42. [Google Scholar] [CrossRef]
- CholeS Study Group; West Midlands Research Collaborative; Vohra, R.S.; Pasquali, S.; Kirkham, A.J.; Marriott, P.; Johnstone, M.; Spreadborough, P.; Alderson, D.; Griffiths, E.A.; et al. Population-based cohort study of outcomes following cholecystectomy for benign gallbladder diseases. Br. J. Surg. 2016, 103, 1704–1715. [Google Scholar]
- Sutherland, J.M.; Mok, J.; Liu, G.; Karimuddin, A.; Crump, T. A Cost-Utility Study of Laparoscopic Cholecystectomy for the Treatment of Symptomatic Gallstones. J. Gastrointest. Surg. 2019, 24, 1314–1319. [Google Scholar] [CrossRef]
- Jones, C.; Mawhinney, A.; Brown, R. The true cost of gallstone disease. Ulst. Med. J. 2012, 81, 10–13. [Google Scholar]
- Borowski, D.; Knox, M.; Kanakala, V.; Richardson, S.; Seymour, K.; Attwood, S.; Slater, B. Referral pathways of patients with gallstones: A potential source of financial waste in the UK National Health Service? Int. J. Health Care Qual. Assur. 2010, 23, 248–257. [Google Scholar] [CrossRef] [PubMed]
- De Mestral, C.; Hoch, J.S.; Laupacis, A.; Winjeysundera, H.C.; Rotstein, O.D.; Alali, A.S.; Nathens, A.B. Early Cholecystectomy for Acute Cholecystitis Offers the Best Outcomes at the Least Cost: A Model-based Cost-Utility Analysis. J. Am. Coll. Surg. 2015, 222, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Jarrod, K.; Tan, H.; Joel, C.; Goh, I.; Janice, W.; Lim, L.; Lyer, G.; Shridar Krishnakumar Madhavan Alfred, W.; Kow, C. Same admission laparoscopic cholecystectomy for acute cholecystitis: Is the “golden 72 hours” rule still relevant? HPB 2016, 19, 47–51. [Google Scholar]
- Morris, S.; Gurusamy, K.S.; Patel, N.; Davidson, B.R. Cost-effectiveness of early laparoscopic cholecystectomy for mild acute gallstone pancreatitis. Br. J. Surg. 2014, 101, 828–835. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Diagnostic Guidelines |
|---|---|
| Dutch Association of Surgery (DAS) [59] | Pain radiating to back. Positive response to analgesia. |
| The German Society for Digestive and Metabolic Diseases’ S3 [6] | Biliary colic pain accompanied by nausea and vomiting. |
| The American Academy of Family Physicians (AAFPI) [61] | Steady pain moderate to severe in epigastrium/right upper quadrant, reaching plateau lasting 1 to 5 h, radiating to upper back at times. If persists with fever and high white blood cell count should raise suspicions of acute cholecystitis, gallstone pancreatitis and ascending cholangitis. Pain in the right upper quadrant of the abdomen; however, pain in this area is not specific for gallstones. The physician must rely on the patient’s description of the pain and on the results of laboratory testing and diagnostic imaging to make a correct diagnosis. |
| Signs or Symptoms | Conclusion |
|---|---|
| (Murphy’s Sign *) OR (RUQ ** mass/pain/tenderness) | Local signs of inflammation |
| (Fever) OR (Elevated CRP) OR (Elevated WCC **) | Systemic signs of inflammation |
| (Local signs of inflammation) AND (Systemic signs of inflammation) | Suspected diagnosis of acute cholecystitis |
| (Suspected diagnosis of acute cholecystitis) AND (Imaging findings characteristic of acute cholecystitis) | Definite diagnosis of acute chlecystitis |
| Severity | Criteria |
|---|---|
| Grade 1—Mild |
|
| Grade 2—Moderate | Acute cholecystitis with any of the following but no organ/system dysfunction:
|
| Grade 3—Severe | Acute cholecystitis with dysfunction of any one of the following organs/systems:
|
| Biliary Colic | Cholecystitis |
|---|---|
| Spasmodic central epigastric pain, sometimes felt on the right | Constant sharp/stabbing pain in right upper quadrant |
| No fever, but may have tachycardia if the pain is severe | Pain may radiate to right shoulder and/or back |
| Tender region over the gallbladder if it is distended | Fever, tachycardia |
| Tenderness in the right upper quadrant | |
| Murphy’s sign—guarding in the right upper quadrant on inspiration |
| Optimal Timing of Treatment after Diagnosis of Acute Cholecystitis | Treatment of Patients with Both Choledocholithiasis and Cholelithiasis | Surgical Strategy | |
|---|---|---|---|
| German clinical practice guideline [84] | Laparoscopic cholecystectomy should be carried out within 24 h of hospital admission | Therapeutic splitting (pre- or intraoperatively) is recommended. Cholelithiasis should be treated by cholecystectomy, within 72 h and a stone-free functioning gallbladder can be left in place. | Laparoscopic cholecystectomy using the four-trocar technique both for symptomatic gallstones and in acute cholecystitis |
| European Association for the Study of the Liver [9] | Cholecystectomy should be carried out preferably within 72 h of admission | Early laparoscopic cholecystectomy should be performed within 72 h of preoperative ERCP. | Laparoscopic cholecystectomy using the four-trocar technique both for symptomatic gallstones and in acute cholecystitis |
| Society of American Gastrointestinal and Endoscopic Surgeons [89] | Cholecystectomy can be carried out within 72 h of diagnosis | ERCP with stone extraction may be performed either before, during, or after cholecystectomy. | Patients with symptomatic cholelithiasis are suitable for laparoscopic cholecystectomy |
| Tokyo Guideline 2018 [90] | For both grade I (mild) and grade II (moderate), laparoscopic cholecystectomy should be carried out soon after the onset of symptoms. For Grade III (severe), the degree of organ dysfunction should be determined normalized | N/A | Laparoscopic surgery, even in the presence of severe inflammation (grade III). |
| Grade | Gallbladder | Cystic Pedicle | Adhesions |
|---|---|---|---|
| 1 | Floppy, non-adherent | Thin and clear | Simple up to the neck/Hartmann’s pouch |
| 2 | Mucocele, packed with stones | Fat-laden | Simple up to the body |
| 3 | Deep fossa, acute cholecystitis, contracted, fibrosis, Hartman’s adherent to CBD, im-paction | Abnormal anatomy or cystic duct short, dilated or obscured | Dense up to fundus; involving hepatic flexure or duodenum |
| 4 | Completely obscured, empyema, gangrene, mass | Impossible to clarify | Dense, fibrosis, wrapping the gallbladder, duodenum or hepatic flexure difficult to separate |
| Gallbladder Appearance | Points | |
| Adhesions < 50% of GB | 1 | |
| Adhesions burying GB | 3 | |
| Distension/Contraction | Points | |
| Distended GB (or contracted shrivelled GB) | 1 | |
| Unable to grasp with atraumatic laparoscopic forceps | 1 | |
| Stone ≥ 1 cm impacted in Hartman’s pouch | 1 | |
| Access | Points | |
| BMI > 30 | 1 | |
| Adhesions from previous surgery limiting access | 1 | |
| Severe Sepsis/Complications | Points | |
| Bile or pus outside GB | 1 | |
| Time to identify cystic artery and duct > 90 min | Points | |
| Yes | 1 | |
| Total Score vs. Degree of difficulty:- | Total score | |
| Mild degree of difficulty | <2 | |
| Moderate degree of difficulty | 2–4 | |
| Severe degree of difficulty | 5–7 | |
| Extreme degree of difficulty | 8–10 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doherty, G.; Manktelow, M.; Skelly, B.; Gillespie, P.; Bjourson, A.J.; Watterson, S. The Need for Standardizing Diagnosis, Treatment and Clinical Care of Cholecystitis and Biliary Colic in Gallbladder Disease. Medicina 2022, 58, 388. https://doi.org/10.3390/medicina58030388
Doherty G, Manktelow M, Skelly B, Gillespie P, Bjourson AJ, Watterson S. The Need for Standardizing Diagnosis, Treatment and Clinical Care of Cholecystitis and Biliary Colic in Gallbladder Disease. Medicina. 2022; 58(3):388. https://doi.org/10.3390/medicina58030388
Chicago/Turabian StyleDoherty, Gerard, Matthew Manktelow, Brendan Skelly, Paddy Gillespie, Anthony J. Bjourson, and Steven Watterson. 2022. "The Need for Standardizing Diagnosis, Treatment and Clinical Care of Cholecystitis and Biliary Colic in Gallbladder Disease" Medicina 58, no. 3: 388. https://doi.org/10.3390/medicina58030388
APA StyleDoherty, G., Manktelow, M., Skelly, B., Gillespie, P., Bjourson, A. J., & Watterson, S. (2022). The Need for Standardizing Diagnosis, Treatment and Clinical Care of Cholecystitis and Biliary Colic in Gallbladder Disease. Medicina, 58(3), 388. https://doi.org/10.3390/medicina58030388