Overlapping Pure LIVS Jr. Stents for Isolated Ruptured Dissecting Aneurysm of the Proximal Posterior Inferior Cerebellar Artery


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
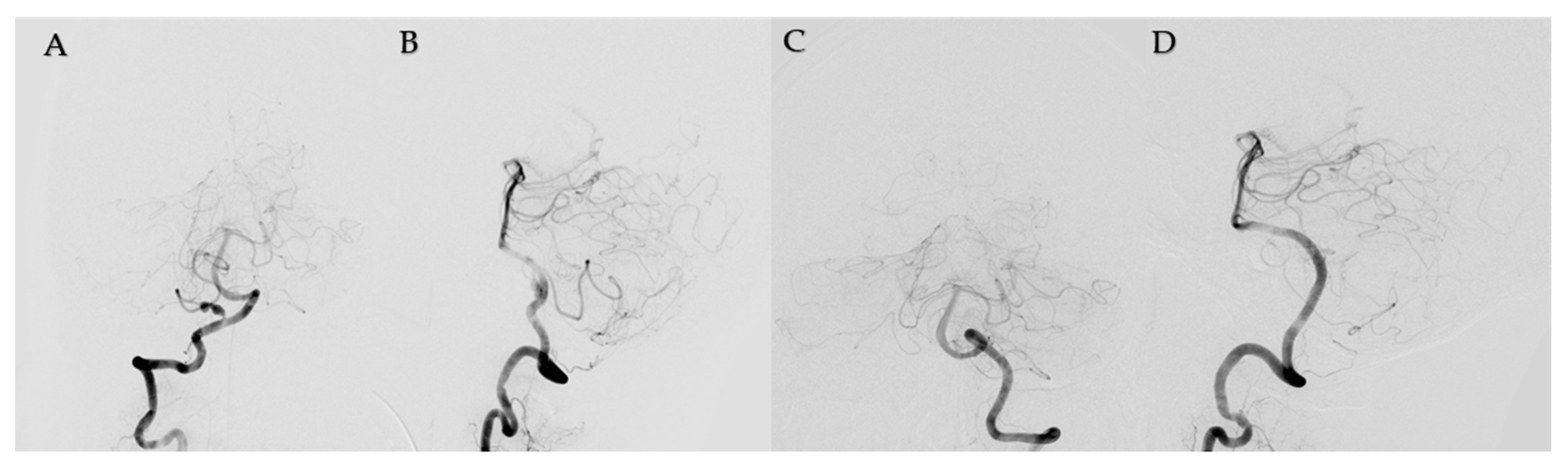
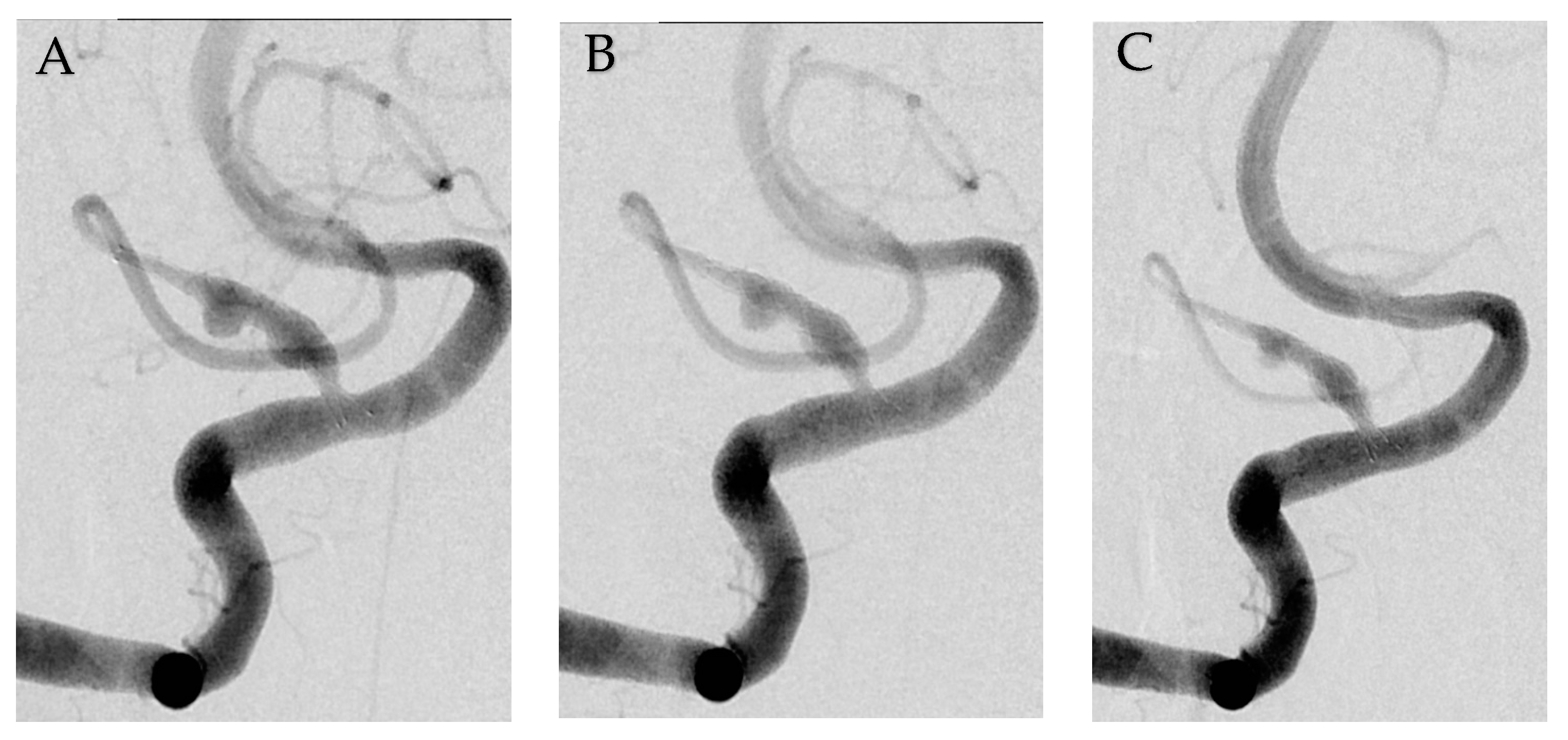
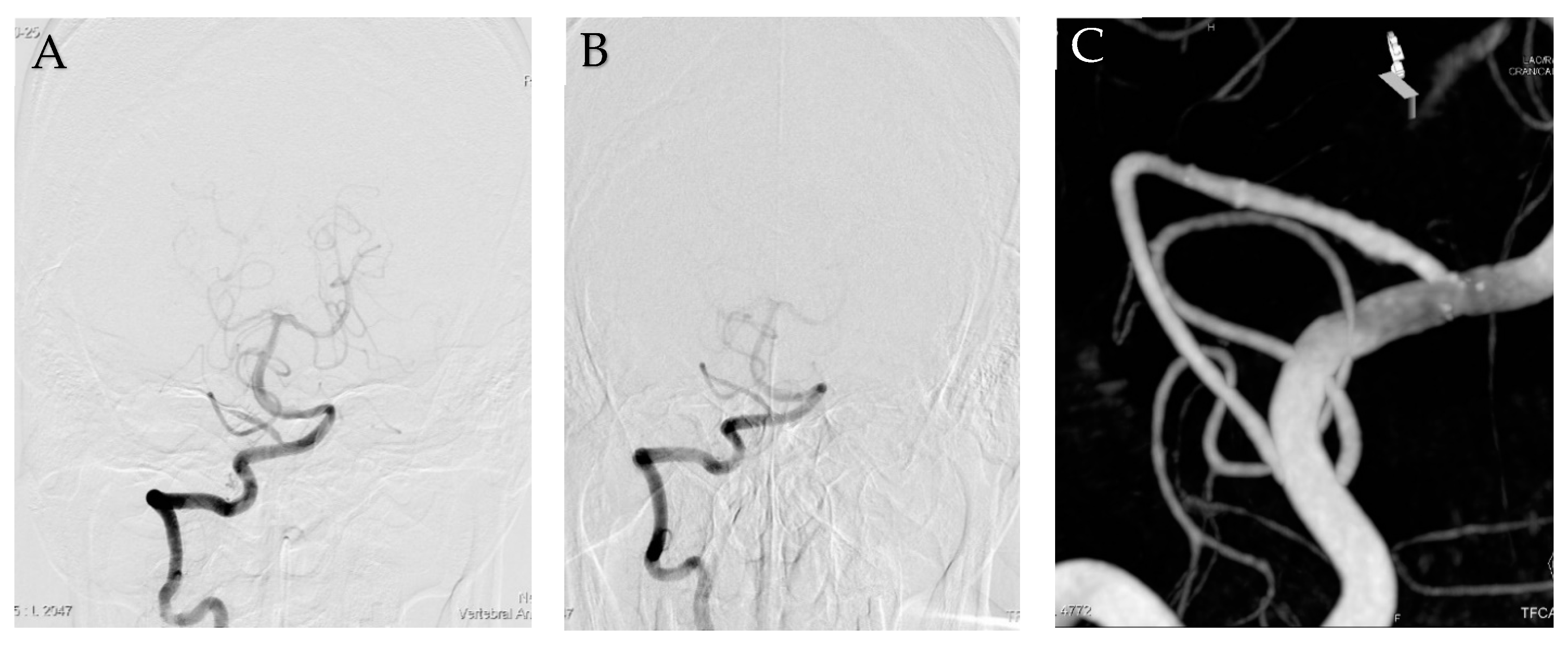
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dinichert, A.; Rufenacht, D.A.; Tribolet, N. Dissecting aneurysms of the posterior inferior cerebellar artery: Report of four cases and review of the literature. J. Clin. Neurosci. 2000, 7, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Jafar, J.; Kamiryo, T.; Chiles, B.W.; Nelson, P.K. A dissecting aneurysm of the posterior inferior cerebellar artery: Case report. Neurosurgery 1998, 43, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Locksley, H.B. Natural history of subarachnoid hemorrhage, intracranial aneurysms and arteriovenous malformation. Based on 6368 cases in the cooperative study. J. Neurosurg. 1966, 25, 219–239. [Google Scholar] [CrossRef]
- Maimon, S.; Saraf-Lavi, E.; Rappaport, Z.H.; Bachar, G. Endovascular treatment of isolated dissecting aneurysm of the posterior inferior cerebellar artery. AJNR Am. J. Neuroradiol. 2006, 27, 527–532. [Google Scholar] [PubMed]
- Ali, M.J.; Bendok, B.R.; Tawk, R.G.; Getch, C.C.; Batjer, H.H. Trapping and revascularization for a dissecting aneurysm of the proximal posterior inferior cerebellar artery: Technical case report and review of the literature. Neurosurgery 2002, 51, 258–263. [Google Scholar] [CrossRef]
- Tikkakoski, T.; Leinonen, S.; Siniluoto, T.; Koivukangas, J. Isolated dissecting aneurysm of the left posterior inferior cerebellar artery: Endovascular treatment with a Guglielmi detachable coil. AJNR Am. J. Neuroradiol. 1997, 18, 936–938. [Google Scholar]
- Tawk, R.G.; Bendok, B.R.; Qureshi, A.I.; Getch, C.C.; Srinivasan, J.; Alberts, M.; Russell, E.J.; Batjer, H.H. Isolated dissections and dissecting aneurysms of the posterior inferior cerebellar artery: Topic and literature review. Neurosurg. Rev. 2003, 26, 180–187. [Google Scholar] [CrossRef]
- Sedat, J.; Chau, Y.; Mahagne, M.H.; Bourg, V.; Lonjon, M.; Paquis, P. Dissection of the posteroinferior cerebellar artery: Clinical characteristics and long-term follow-up in five cases. Cerebrovasc. Dis. 2007, 24, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Kleinpeter, G. Why are aneurysms of the posterior inferior cerebellar artery so unique? Clinical experience and review of the literature. Minim. Invasive Neurosurg. 2004, 47, 93–101. [Google Scholar] [CrossRef]
- Yamakawa, H.; Kaku, Y.; Yoshimura, S.; Yoshimura, S.; Ohkumuc, A.; Sakai, N. Two cases of dissecting aneurysm of the distal posterior inferior Cerebellar artery: Possible involvement of segmental mediolytic arteriopathy in the pathogenesis. Clin. Neurol. Neurosurg. 2005, 107, 117–122. [Google Scholar] [CrossRef]
- Yamaura, A. Diagnosis and treatment of vertebra aneurysms. J. Neurosurg. 1988, 69, 345–349. [Google Scholar] [CrossRef]
- Wetjen, N.M.; Link, M.J.; Reimer, R.; Nichols, D.A.; Giannini, C. Clinical presentation and surgical management of dissecting posterior inferior cerebellar artery aneurysms: 2 case reports. Surg. Neurol. 2005, 64, 462–467. [Google Scholar] [CrossRef]
- Shinoda, S.; Murata, H.; Waga, S.; Kojima, T. Bilateral spontaneous dissection of the posteroinferior cerebellar arteries: Case report. Neurosurgery 1998, 43, 357–359. [Google Scholar] [CrossRef]
- Horowitz, M.; Kopitnik, T.; Landreneau, F.; Krummerman, J.; Batjer, H.H.; Thomas, G.; Samson, D. Posteroinferior cerebellar artery aneurysms: Surgical results for 38 patients. Neurosurgery 1998, 43, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.G.; Tymianski, M.; Terbrugge, K. A dissecting aneurysm of the posterior inferior cerbellar artery. Int. Neuroradiol. 2001, 7, 253–257. [Google Scholar] [CrossRef]
- Al-Khayat, H.; Al-Khayat, H.; Beshay, J.; Manner, D.; White, J.; Samson, D.S. Vertebral artery-posteroinferior cerebellar artery aneurysms: Clinical and lower cranial nerve outcomes in 52 patients. Neurosurgery 2005, 56, 2–11. [Google Scholar] [CrossRef]
- Yamaura, I.; Tani, E.; Yokota, M. Endovascular treatment of ruptured dissecting aneurysms aimed at occlusion of the dissected site by using Guglielmi detachable coils. Neurosurgery 1999, 90, 853–856. [Google Scholar] [CrossRef] [PubMed]
- Lefkowitz, M.A.; Teitelbaum, G.P.; Giannotta, S.L. Endovascular treatment of dissecting posterior inferior cerebellar artery: A clinical series. Surg. Neurol. 1989, 31, 85–91. [Google Scholar] [CrossRef]
- Lister, J.R.; Rhoton, A.L.; Matsushima, T.; Peace, D.A. Microsurgical anatomy of the posterior inferior cerebellar artery. Neurosurgery 1982, 10, 170–199. [Google Scholar] [CrossRef]
- Bhogal, P.; Chudyk, J.; Bleise, C.; Lylyk, I.; Henkes, H.; Lylyk, P. The use of flow diverters to treat aneurysms of the posterior inferior cerebellar artery: Report of three cases. Interv. Neuroradiol. 2018, 24, 489–498. [Google Scholar] [CrossRef]
- Wang, C.; Tian, Z.; Liu, J.; Jing, L.; Paliwal, N.; Wang, S.; Zhang, Y.; Xiang, J.; Siddiqui, A.H.; Meng, H.; et al. Flow diverter effect of LVIS stent on cerebral aneurysm hemodynamics: A comparison with Enterprise stents and the Pipeline device. J. Transl. Med. 2016, 14, 199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.; Lee, K.; Park, H.; Heo, W.; Hwang, S.-H. Overlapping Pure LIVS Jr. Stents for Isolated Ruptured Dissecting Aneurysm of the Proximal Posterior Inferior Cerebellar Artery. Medicina 2022, 58, 240. https://doi.org/10.3390/medicina58020240
Lim S, Lee K, Park H, Heo W, Hwang S-H. Overlapping Pure LIVS Jr. Stents for Isolated Ruptured Dissecting Aneurysm of the Proximal Posterior Inferior Cerebellar Artery. Medicina. 2022; 58(2):240. https://doi.org/10.3390/medicina58020240
Chicago/Turabian StyleLim, Sungdae, Kwangho Lee, Hyun Park, Won Heo, and Soo-Hyun Hwang. 2022. "Overlapping Pure LIVS Jr. Stents for Isolated Ruptured Dissecting Aneurysm of the Proximal Posterior Inferior Cerebellar Artery" Medicina 58, no. 2: 240. https://doi.org/10.3390/medicina58020240
APA StyleLim, S., Lee, K., Park, H., Heo, W., & Hwang, S.-H. (2022). Overlapping Pure LIVS Jr. Stents for Isolated Ruptured Dissecting Aneurysm of the Proximal Posterior Inferior Cerebellar Artery. Medicina, 58(2), 240. https://doi.org/10.3390/medicina58020240