
Temporary Trends Concerning the Extent and Efficacy of Atrial Fibrillation Ablation Using Radiofrequency Energy in a Polish Single-Center Experience

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
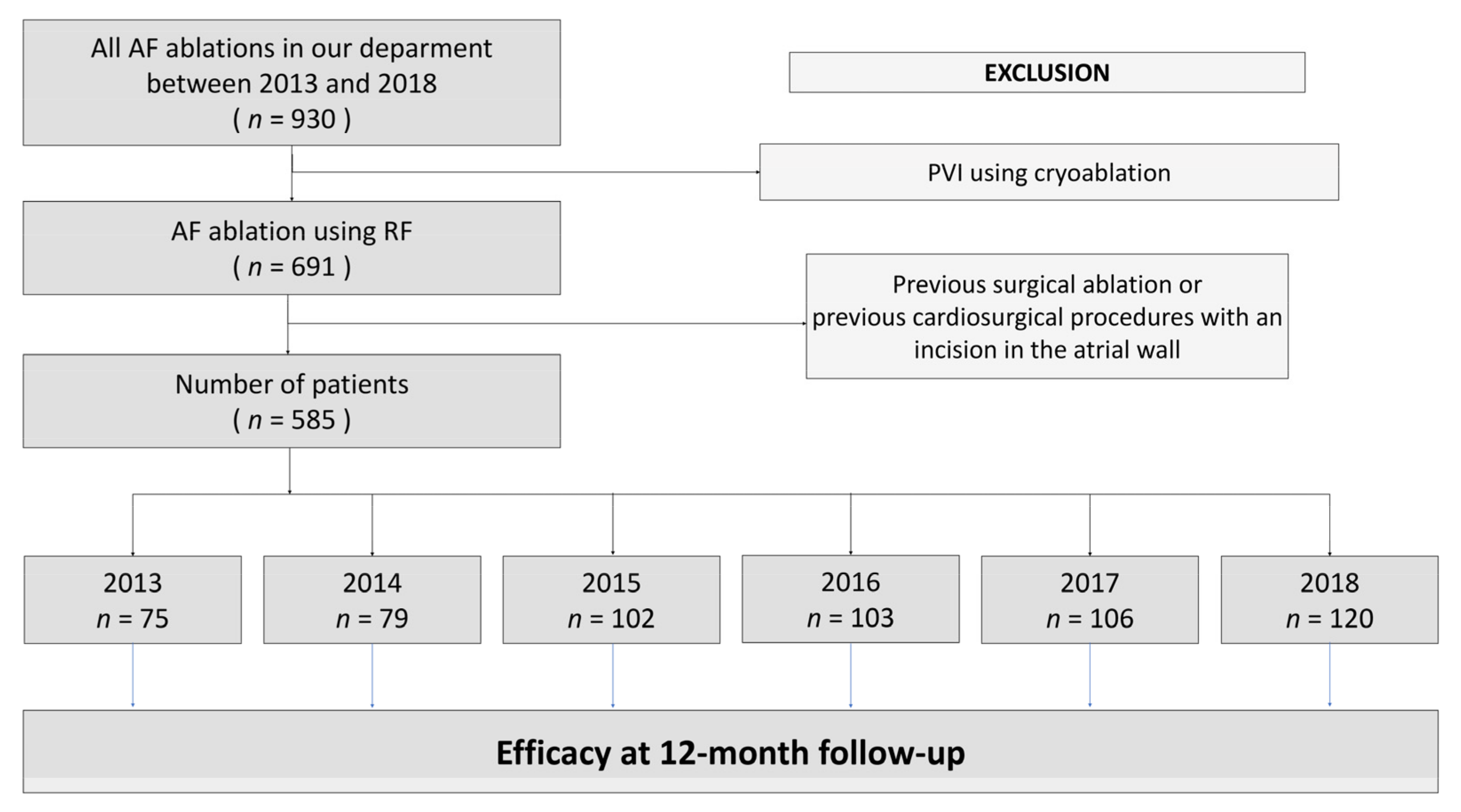
2.1. Study Design and Study Population
2.2. Pre-Ablation Procedure
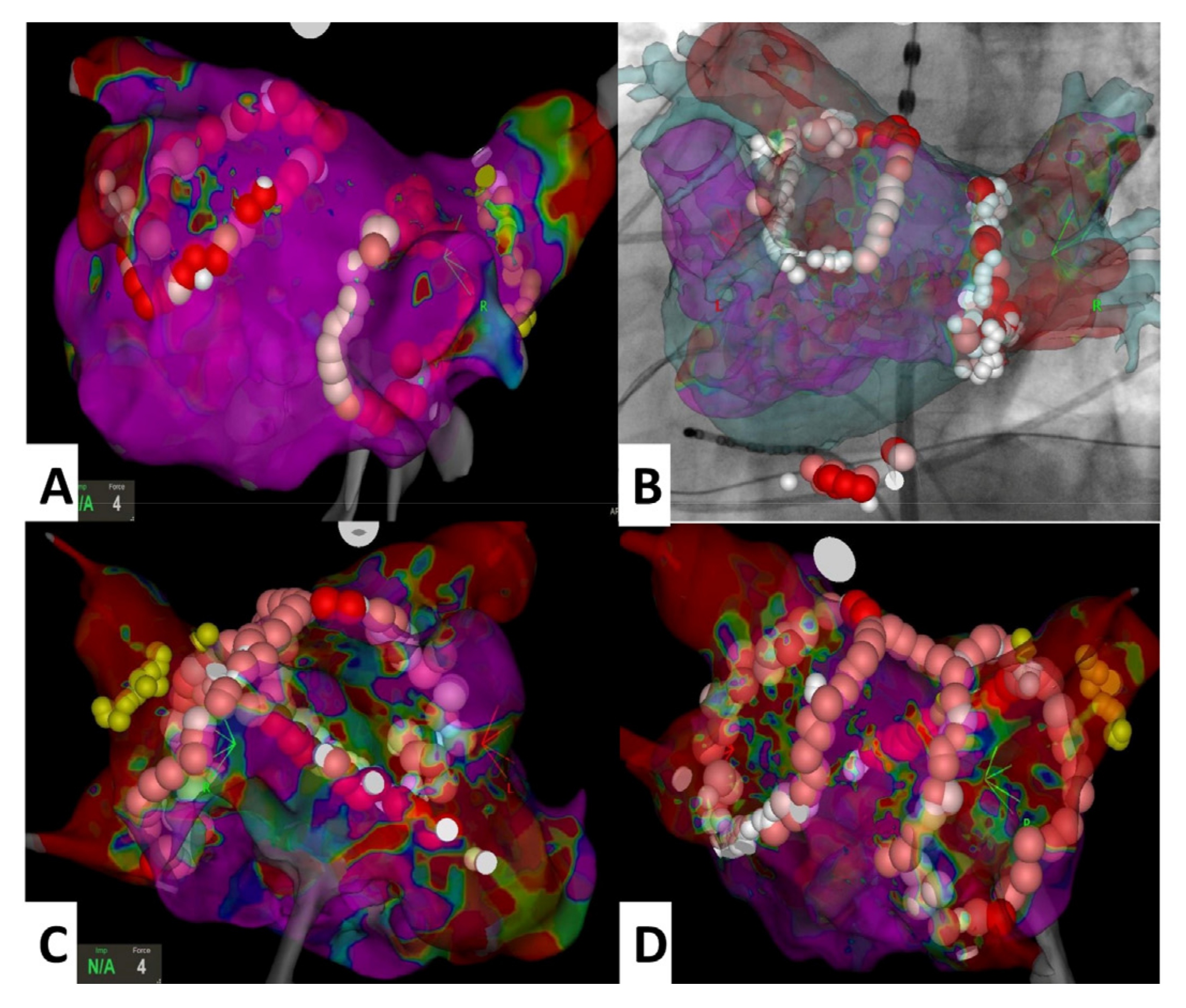
2.3. Catheter Ablation and Post-Ablation Hospital Management
2.4. Procedure after Discharge
2.5. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Stewart, S.; Murphy, N.F.; Walker, A.; McGuire, A.; McMurray, J.J. Cost of an emerging epidemic: An economic analysis of atrial fibrillation in the UK. Heart 2004, 90, 286–292. [Google Scholar] [CrossRef]
- Blomstrom Lundqvist, C.; Lip, G.Y.; Kirchhof, P. What are the costs of atrial fibrillation? Europace 2011, 13. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. Fifty-Year Trends in Atrial Fibrillation Prevalence, Incidence, Risk Factors, and Mortality in the Community Renate. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef]
- Heeringa, J.; Van Der Kuip, D.A.M.; Hofman, A.; Kors, J.A.; Van Herpen, G.; Stricker, B.H.C.; Stijnen, T.; Lip, G.Y.H.; Witteman, J.C.M. Prevalence, incidence and lifetime risk of atrial fibrillation: The Rotterdam study. Eur. Heart J. 2006, 27, 949–953. [Google Scholar] [CrossRef]
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.H.; McAnulty, J.H., Jr.; Zheng, Z.J.; et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef]
- Wilke, T.; Groth, A.; Mueller, S.; Pfannkuche, M.; Verheyen, F.; Linder, R.; Maywald, U.; Bauersachs, R.; Breithardt, G. Incidence and prevalence of atrial fibrillation: An analysis based on 8.3 million patients. Europace 2013, 15, 486–493. [Google Scholar] [CrossRef]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef]
- Kozieł, M.; Mihajlovic, M.; Nedeljkovic, M.; Pavlovic, N.; Paparisto, V.; Music, L.; Trendafilova, E.; Rodica Dan, A.; Kusljugic, Z.; Dan, G.A.; et al. Symptom management strategies: Rhythm vs rate control in patients with atrial fibrillation in the Balkan region: Data from the BALKAN-AF survey. Int. J. Clin. Pract. 2021, 75, e14080. [Google Scholar] [CrossRef]
- Lip, G.Y.; Laroche, C.; Boriani, G.; Dan, G.A.; Santini, M.; Kalarus, Z.; Rasmussen, L.H.; Oliveira, M.M.; Mairesse, G.; Crijns, H.J.; et al. Regional differences in presentation and treatment of patients with atrial fibrillation in Europe: A report from the EURObservational Research Programme Atrial Fibrillation (EORP-AF) Pilot General Registry. Europace 2015, 17, 194–206. [Google Scholar] [CrossRef]
- Lip, G.Y.; Laroche, C.; Ioachim, P.M.; Rasmussen, L.H.; Vitali-Serdoz, L.; Petrescu, L.; Darabantiu, D.; Crijns, H.J.; Kirchhof, P.; Vardas, P.; et al. Prognosis and treatment of atrial fibrillation patients by European cardiologists: One year follow-up of the EURObservational Research Programme-Atrial Fibrillation General Registry Pilot Phase (EORP-AF Pilot registry). Eur. Heart J. 2014, 35, 3365–3376. [Google Scholar] [CrossRef]
- McManus, D.D.; Yin, X.; Gladstone, R.; Vittinghoff, E.; Vasan, R.S.; Larson, M.G.; Benjamin, E.J.; Marcus, G.M. Alcohol Consumption, Left Atrial Diameter, and Atrial Fibrillation. J. Am. Heart Assoc. 2016, 5, e004060. [Google Scholar] [CrossRef] [PubMed]
- Faryan, M.; Buchta, P.; Kowalski, O.; Wybraniec, M.T.; Cieśla, D.; Myrda, K.; Wnuk-Wojnar, A.; Kalarus, Z.; Gąsior, M.; Mizia-Stec, K. Temporal trends in the availability and efficacy of catheter ablation for atrial fibrillation and atrial flutter in a highly populated urban area. Kardiol. Pol. 2020, 78, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Schmalowsky, J.; Pittrow, D.; Rosin, L.; Kirch, W.; Wegscheider, K.; Meinertz, T.; ATRIUM Study Group. Quality and Outcomes Management of Patients With Atrial Fibrillation by Primary-Care Physicians in Germany: 1-Year Results of the ATRIUM Registry. Clin. Cardiol. 2014, 37, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Ammentorp, B.; Darius, H.; De Caterina, R.; Le Heuzey, J.-Y.; Schilling, R.J.; Schmitt, J.; Zamorano, J.L. Management of atrial fibrillation in seven European countries after the publication of the 2010 ESC Guidelines on atrial fibrillation: Primary results of the PREvention oF thromboemolic events—European Registry in Atrial Fibrillation (PREFER in AF). Europace 2014, 16, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Kummer, B.R.; Bhave, P.D.; Merkler, A.E.; Gialdini, G.; Okin, P.M.; Kamel, H. Demographic Differences in Catheter Ablation After Hospital Presentation with Symptomatic Atrial Fibrillation. J. Am. Hear. Assoc. 2015, 4, e002097. [Google Scholar] [CrossRef]
- Dudek, D.; Banasiak, W.; Braksator, W.; Dubiel, J.; Grodzicki, T.; Hoffman, P.; Kuśmierczyk, M.; Opolski, G.; Ponikowski, P.; Różański, J.; et al. Recommendations on the use of innovative medical technologies in cardiology and cardiac surgery and solutions leading to increased availability for Polish patients. Cardiol. J. 2019, 26, 114–129. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 42, 373–498. [Google Scholar] [CrossRef]
- Natale, A.; Reddy, V.Y.; Monir, G.; Wilber, D.J.; Lindsay, B.D.; McElderry, H.T.; Kantipudi, C.; Mansour, M.C.; Melby, D.P.; Packer, D.L.; et al. Paroxysmal AF catheter ablation with a contact force sensing catheter: Results of the prospective, multicenter SMART-AF trial. J. Am. Coll. Cardiol. 2014, 64, 647–656. [Google Scholar] [CrossRef]
- Packer, D.L.; Mark, D.B.; Robb, R.A.; Monahan, K.H.; Bahnson, T.D.; Poole, J.E.; Noseworthy, P.A.; Rosenberg, Y.D.; Jeffries, N.; Mitchell, L.B.; et al. Effect of Catheter Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients with Atrial Fibrillation The CABANA Randomized Clinical Trial. JAMA 2019, 321, 1261–1274. [Google Scholar] [CrossRef]
- Verma, A.; Wazni, O.M.; Marrouche, N.F.; Martin, D.O.; Kilicaslan, F.; Minor, S.; Schweikert, R.A.; Saliba, W.; Cummings, J.; Burkhardt, J.D.; et al. Pre-existent left atrial scarring in patients undergoing pulmonary vein antrum isolation: An independent predictor of procedural failure. J. Am. Coll. Cardiol. 2005, 45, 285–292. [Google Scholar] [CrossRef]
- Sanders, P.; Morton, J.B.; Davidson, N.C.; Spence, S.J.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Electrical remodeling of the atria in congestive heart failure: Electrophysiological and electroanatomic mapping in humans. Circulation 2003, 108, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Halm, U.; Gaspar, T.; Zachäus, M.; Sack, S.; Arya, A.; Piorkowski, C.; Knigge, I.; Hindricks, G.; Husser, D. Thermal Esophageal Lesions After Radiofrequency Catheter Ablation of Left Atrial Arrhythmias. Am. J. Gastroenterol. 2010, 105, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Wojdyła-Hordyńska, A.; Baran, J.; Mazurek, M.; Derejko, P. Results of a survey concerning atrial fibrillation ablation strategies in Poland. Kardiol. Pol. 2020, 78, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Tilz, R.R.; Dagres, N.; Arbelo, E.; Blomström-Lundqvist, C.; Crijns, H.J.; Kirchhof, P.; Kautzner, J.; Temporelli, P.L.; Laroche, C.; Roberts, P.R.; et al. Atrial Fibrillation Ablation and Atrial Fibrillation Registries Investigators Groups. Which patients with atrial fibrillation undergo an ablation procedure today in Europe? A report from the ESC-EHRA-EORP Atrial Fibrillation Ablation Long-Term and Atrial Fibrillation General Pilot Registries. Europace 2020, 22, 250–258. [Google Scholar] [CrossRef]
- Niedziela, J.T.; Parma, Z.; Pawlowski, T.; Rozentryt, P.; Gasior, M.; Wojakowski, W. Secular trends in first-time hospitalization for heart failure with following one-year readmission and mortality rates in the 3.8 million adult population of Silesia, Poland between 2010 and 2016. The SILCARD database. Inter. J. Cardiol. 2018, 271, 146–151. [Google Scholar] [CrossRef]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef]
- Pruszkowska, P.; Lenarczyk, R.; Gumprecht, J.; Jedrzejczyk-Patej, E.; Mazurek, M.; Kowalski, O.; Sokal, A.; Podolecki, T.; Morawski, S.; Streb, W.; et al. Cryoballoon ablation of atrial fibrillation in patients with advanced systolic heart failure and cardiac implantable electronic devices. Kardiol. Pol. 2018, 76, 1081–1088. [Google Scholar] [CrossRef]
- Hunter, R.J.; Berriman, T.J.; Diab, I.; Kamdar, R.; Richmond, L.; Baker, V.; Goromonzi, F.; Sawhney, V.; Duncan, E.; Page, S.P.; et al. A Randomized Controlled Trial of Catheter Ablation Versus Medical Treatment of Atrial Fibrillation in Heart Failure (The CAMTAF Trial). Circ. Arrhythmia Electrophysiol. 2014, 7, 31–38. [Google Scholar] [CrossRef]
- Mont, L.; Bisbal, F.; Hernández-Madrid, A.; Pérez-Castellano, N.; Viñolas, X.; Arenal, A.; Arribas, F.; Lozano, I.F.; Bodegas, A.; Cobos, A.; et al. Catheter ablation vs. antiarrhythmic drug treatment of persistent atrial fibrillation: A multicentre, randomized, controlled trial (SARA study). Eur. Heart J. 2014, 35, 501–507. [Google Scholar] [CrossRef]
- Buchta, P.; Sierpiński, R.; Myrda, K.; Filipiak, K.; Kowalski, O.; Bratkowski, W.; Kalarus, Z.; Gąsior, M.; Zembala, M.O. New hope for patients and challenges for the multidisciplinary arrhythmia team: A hybrid convergent approach for atrial fibrillation treatment. Kardiol. Pol. 2020, 78, 1243–1253. [Google Scholar] [CrossRef]
- Janusauskas, V.; Puodziukaite, L.; Maneikiene, V.V.; Zuoziene, G.; Radauskaite, G.; Burneikaite, G.; Stasys Samalavicius, R.; Aidietiene, S.; Rucinskas, K.; Aidietis, A. Long-term results of minimally invasive stand-alone bi-atrial surgical ablation with a bipolar ablation device for persistent and longstanding persistent AF: A single-center case series of 91 patients. J. Cardiothorac. Surg. 2016, 11, 23. [Google Scholar] [CrossRef] [PubMed]
- Dagres, N.; Hindricks, G.; Kottkamp, H.; Sommer, P.; Gaspar, T.; Bode, K.; Arya, A.; Husser, D.; Rallidis, L.S.; Kremastinos, D.T.; et al. Complications of Atrial Fibrillation Ablation in a High-Volume Center in 1000 Procedures: Still Cause for Concern? J. Cardiovasc. Electrophysiol. 2009, 20, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Cappato, R.; Calkins, H.; Chen, S.-A.; Davies, W.; Iesaka, Y.; Kalman, J.; Kim, Y.-H.; Klein, G.; Natale, A.; Packer, D.; et al. Prevalence and Causes of Fatal Outcome in Catheter Ablation of Atrial Fibrillation. J. Am. Coll. Cardiol. 2009, 53, 1798–1803. [Google Scholar] [CrossRef] [PubMed]
- Buchta, P.; Myrda, K.; Gąsior, M.; Poloński, L. Image integration of cine-angiography with 3D electroanatomical mapping. Atrial flutter ablation with CARTO UniVu™ module support. Kardiol. Pol. 2015, 73, 941. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tahin, T.; Riba, A.; Nemeth, B.; Arvai, F.; Lupkovics, G.; Szeplaki, G.; Geller, L. Implementation of a zero fluoroscopic workflow using a simplified intracardiac echocardiography guided method for catheter ablation of atrial fibrillation, including repeat procedures. BMC Cardiovasc. Disord. 2021, 21, 407. [Google Scholar] [CrossRef]
- Kircher, S.; Arya, A.; Altmann, D.; Rolf, S.; Bollmann, A.; Sommer, P.; Dagres, N.; Richter, S.; Breithardt, O.-A.; Dinov, B.; et al. Individually tailored vs. standardized substrate modification during radiofrequency catheter ablation for atrial fibrillation: A randomized study. Europace 2018, 20, 1766–1775. [Google Scholar] [CrossRef]
- Huisman, M.V.; Ma, C.S.; Diener, H.C.; Dubner, S.J.; Halperin, J.L.; Rothman, K.J.; Teutsch, C.; Schoof, N.; Kleine, E.; Bartels, D.B.; et al. Antithrombotic therapy use in patients with atrial fibrillation before the era of non-vitamin K antagonist oral anticoagulants: The Global Registry on Long-Term Oral Antithrombotic Treatment in Patients with Atrial Fibrillation (GLORIA-AF) Phase I coho. Europace 2016, 18, 1308–1318. [Google Scholar] [CrossRef]
- Lenarczyk, R.; Mitręga, K.; Mazurek, M.; Janion, M.; Opolski, G.; Drożdż, J.; Streb, W.; Fuglewicz, A.; Sokal, A.; Laroche, C.; et al. Polish and European management strategies in patients with atrial fibrillation. Data from the EURObservational Research Programme-Atrial Fibrillation General Registry Pilot Phase (EORP-AF Pilot). Pol. Arch. Intern. Med. 2016, 126, 138–148. [Google Scholar] [CrossRef]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace 2018, 20, e1–e160. [Google Scholar] [CrossRef]
- Andrade, J.G.; Wells, G.A.; Deyell, M.W.; Bennett, M.; Essebag, V.; Champagne, J.; Roux, J.-F.; Yung, D.; Skanes, A.; Khaykin, Y.; et al. Cryoablation or Drug Therapy for Initial Treatment of Atrial Fibrillation. N. Engl. J. Med. 2021, 384, 305–315. [Google Scholar] [CrossRef]
- Gorczyca, I.; Jelonek, O.; Uziębło-Życzkowska, B.; Chrapek, M.; Maciorowska, M.; Wójcik, M.; Błaszczyk, R.; Kapłon-Cieślicka, A.; Gawałko, M.; Budnik, M.; et al. Trends in the Prescription of Non-Vitamin K Antagonist Oral Anticoagulants for Atrial Fibrillation: Results of the Polish Atrial Fibrillation (POL-AF) Registry. J. Clin. Med. 2020, 9, 3565. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | p Value for Trend | |
|---|---|---|---|---|---|---|---|---|
| Number of patients | 585 | 75 | 79 | 102 | 103 | 106 | 120 | |
| Sex (males), (%) | 65.8 | 66.7 | 62.0 | 59.8 | 67.0 | 69.8 | 68.3 | 0.29 |
| Age (years), mean (SD) | 59 (10) | 59 (10) | 60 (10) | 58 (11) | 58 (10) | 60 (11) | 59 (12) | 0.19 |
| BMI (kg/m2), median (Q1; Q3) | 29.4 (26.3; 32.5) | 30.0 (26.1; 33.8) | 29.8 (27.7; 32.6) | 29.9 (25.8; 32.9) | 28.9 (26.1; 32.0) | 29.0 (26.4; 32.0) | 29.4 (26.4; 32.3) | 0.06 |
| CHADS-VASc, median (Q1; Q3) | 2 (1; 3) | 2 (1; 3) | 1 (1; 3) | 2 (1; 3) | 2 (1; 3) | 2 (1; 3) | 2 (1; 3) | 0.01 |
| HASBLED, median (Q1; Q3) | 1 (1; 2) | 1 (1; 2) | 1 (1; 2) | 1 (1; 2) | 1 (0; 2) | 1 (1; 2) | 1 (0; 2) | 0.42 |
| Hypertension, (%) | 67.4 | 69.3 | 70.9 | 68.6 | 70.9 | 65.1 | 61.7 | 0.15 |
| History of diabetes, (%) | 23.6 | 32.0 | 30.4 | 24.5 | 19.4 | 21.7 | 18.3 | <0.01 |
| History of CAD, (%) | 27.9 | 28.0 | 22.8 | 30.4 | 22.3 | 33.0 | 29.2 | 0.45 |
| Hyperlipidemia, (%) | 78.0 | 82.7 | 82.3 | 74.5 | 77.7 | 80.2 | 73.3 | 0.18 |
| Previous MI, (%) | 6.8 | 8.0 | 7.6 | 2.9 | 5.8 | 9.4 | 7.5 | 0.66 |
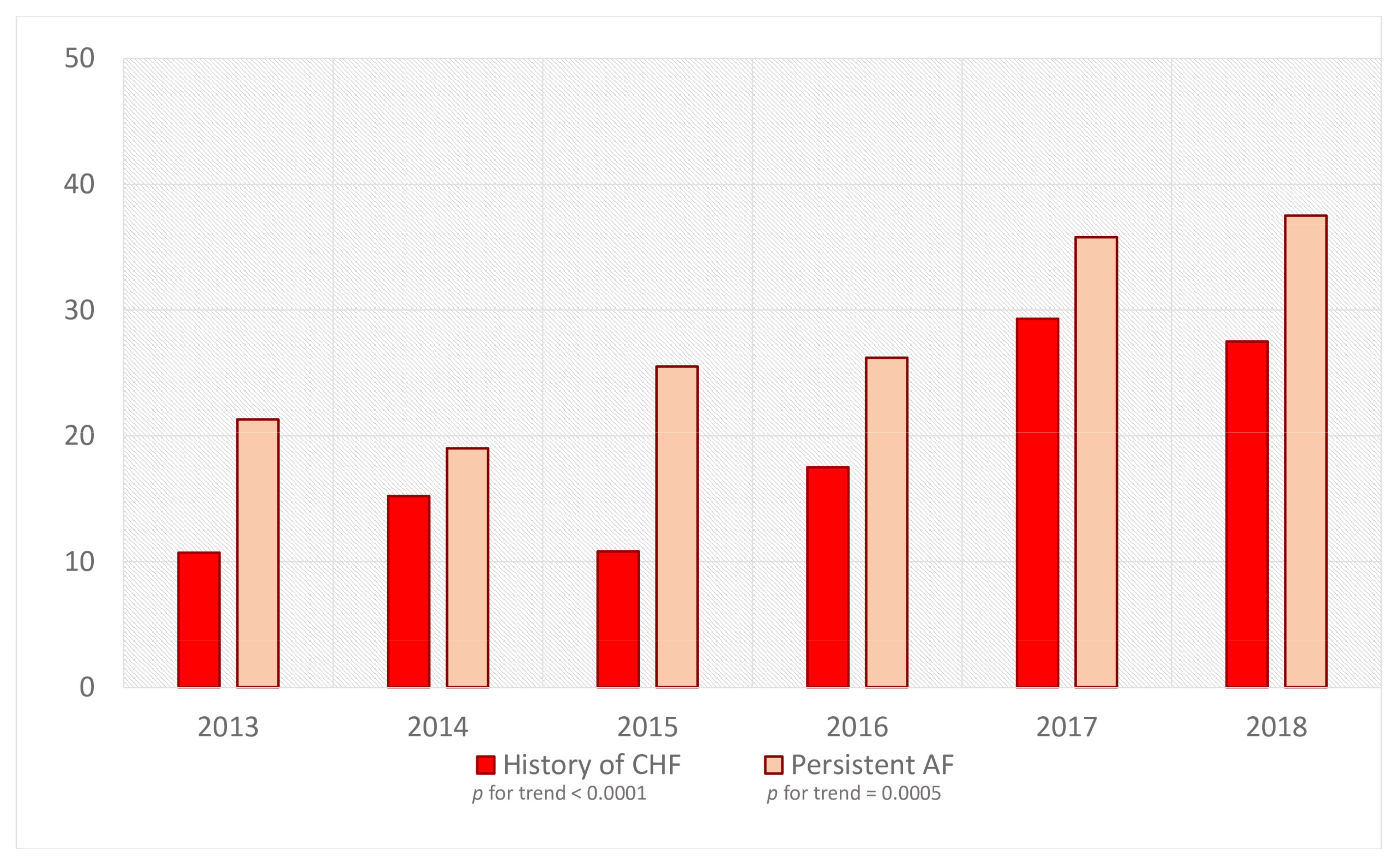
| History of CHF, (%) | 19.3 | 10.7 | 15.2 | 10.8 | 17.5 | 29.3 | 27.5 | <0.001 |
| Implanted ICD/CRT, (%) | 5.6 | 4.0 | 3.8 | 2.0 | 2.9 | 6.6 | 11.7 | <0.01 |
| History of stroke, (%) | 4.4 | 4.0 | 2.5 | 3.9 | 3.9 | 7.6 | 4.2 | 0.39 |
| History of TIA, (%) | 3.6 | 6.7 | 1.3 | 3.9 | 4.8 | 3.8 | 1.7 | 0.29 |
| Prior AF ablation, (%) | 25.1 | 16.0 | 20.3 | 17.7 | 22.3 | 31.1 | 37.5 | <0.001 |
| Atrial fibrillation | ||||||||
| Paroxysmal, (%) | 71.5 | 78.7 | 81.0 | 74.5 | 73.8 | 64.2 | 62.5 | <0.001 |
| Persistent, (%) | 28.5 | 21.3 | 19.0 | 25.5 | 26.2 | 35.8 | 37.5 | <0.001 |
| Total | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | p Value for Trend | |
|---|---|---|---|---|---|---|---|---|
| Number of patients | 585 | 75 | 79 | 102 | 103 | 106 | 120 | |
| Echocardiographic parameters | ||||||||
| LA diameter (mm), mean (SD) | 43 (5) | 42 (5) | 42 (4) | 42 (5) | 43 (5) | 44 (5) | 44 (6) | <0.001 |
| LV ESV (ml), mean (SD) | 54 (25) | 52 (19) | 50 (16) | 51 (23) | 51 (26) | 59 (28) | 58 (28) | 0.03 |
| LV EDV (ml), mean (SD) | 108 (34) | 103 (29) | 106 (28) | 106 (32) | 103 (34) | 116 (36) | 113 (37) | 0.046 |
| LV EF (%), mean (SD) | 51 (9) | 53 (6) | 53 (6) | 52 (9) | 52 (8) | 50 (10) | 49 (10) | <0.001 |
| Procedural data | ||||||||
| PVI alone, (%) | 73.0 | 82.7 | 81.0 | 72.6 | 77.7 | 65.1 | 65.0 | <0.001 |
| LA substrate modification, (%) | 27.0 | 17.3 | 19.0 | 27.4 | 22.3 | 34.9 | 35.0 | <0.001 |
| CTI ablation, (%) | 16.6 | 6.7 | 16.5 | 13.7 | 17.5 | 19.8 | 21.7 | <0.01 |
| In-hospital data | ||||||||
| In-hospital recurrence of AF, (%) | 11.8 | 19.7 | 16.5 | 10.8 | 8.7 | 9.4 | 10.0 | 0.03 |
| Major complications, n (%) | 7 (1.2) | 1 (1.3) | 0 (0.0) | 2 (2.0) | 1 (1.0) | 1 (0.9) | 2 (1.7) | 0.73 |
| Minor complications, n (%) | 23 (3.9) | 3 (4.0) | 4 (5.0) | 3 (2.9) | 3 (2.9) | 4 (3.8) | 6 (5.0) | 0.41 |
| Drugs at discharge | ||||||||
| Beta-blockers, (%) | 88.4 | 86.7 | 84.8 | 86.3 | 87.4 | 90.6 | 92.5 | 0.07 |
| Propafenone, (%) | 52.1 | 46.7 | 59.5 | 58.8 | 64.1 | 43.4 | 42.5 | 0.06 |
| Ca-blockers, (%) | 17.4 | 10.7 | 16.5 | 17.7 | 19.4 | 17.0 | 20.1 | 0.12 |
| Sotalol, (%) | 8.4 | 10.7 | 10.1 | 9.8 | 8.7 | 7.6 | 5.0 | 0.1 |
| Amiodarone, (%) | 8.4 | 6.7 | 11.4 | 8.8 | 4.9 | 8.5 | 10.0 | 0.81 |
| VKA, (%) | 52.7 | 74.7 | 84.8 | 68.6 | 44.7 | 35.8 | 25.8 | <0.001 |
| NOAC, (%) | 47.3 | 25.3 | 15.2 | 31.4 | 55.3 | 64.2 | 74.2 | <0.001 |
| Total | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | p Value for Trend | |
|---|---|---|---|---|---|---|---|---|
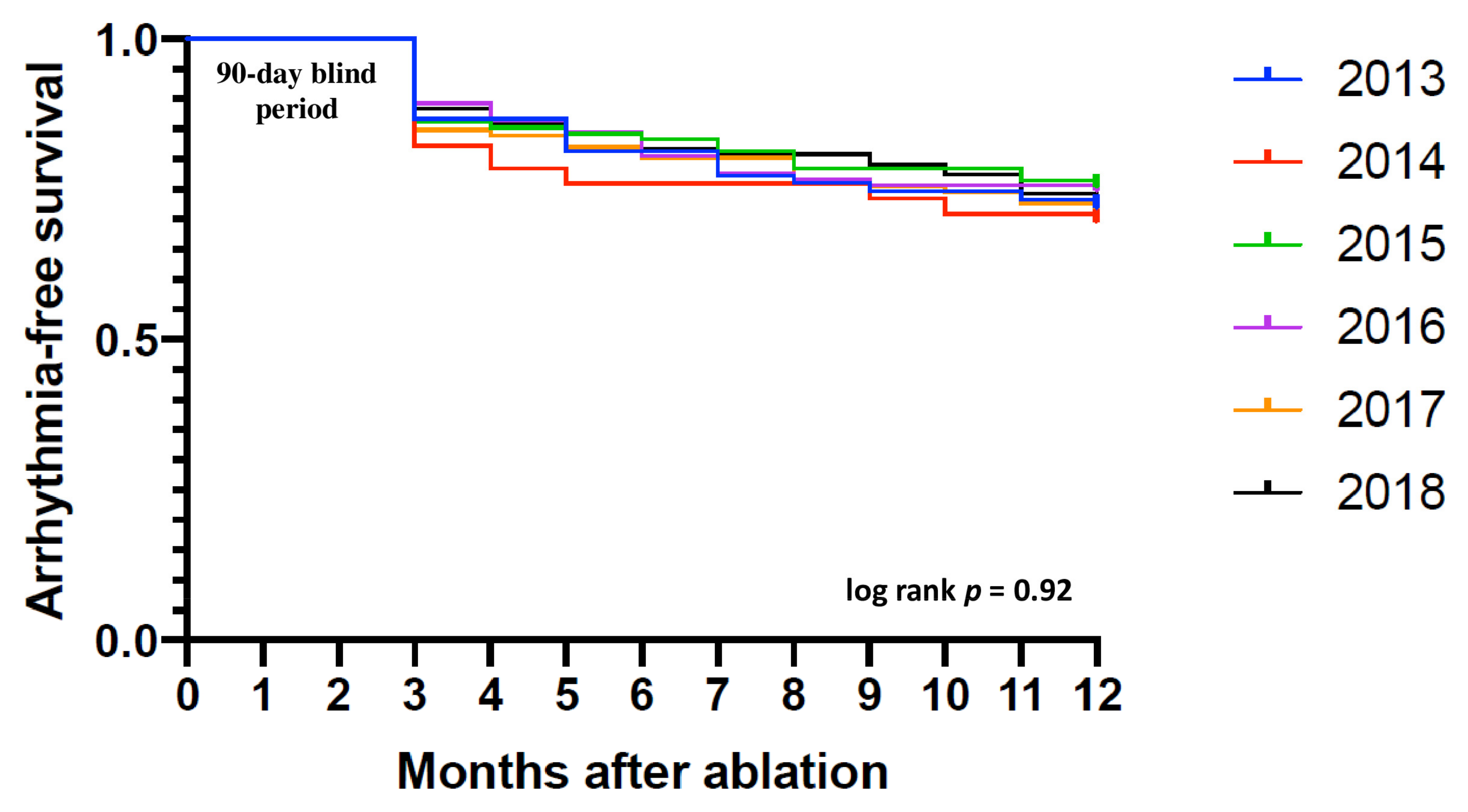
| Freedom from AF/AFl/AT at 6 months following ablation, (%) | 80.7 | 81.3 | 76.0 | 83.3 | 80.6 | 80.2 | 81.7 | 0.75 |
| Freedom from AF/AFl/AT at 9 months following ablation, (%) | 76.4 | 74.7 | 73.4 | 78.4 | 75.7 | 75.5 | 79.2 | 0.48 |
| Freedom from AF/AFl/AT at 12 months following ablation, (%) | 72.6 | 72.0 | 69.6 | 75.5 | 74.8 | 71.7 | 71.7 | 0.69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Myrda, K.; Buchta, P.; Błachut, A.; Skrzypek, M.; Gąsior, M. Temporary Trends Concerning the Extent and Efficacy of Atrial Fibrillation Ablation Using Radiofrequency Energy in a Polish Single-Center Experience. Medicina 2022, 58, 187. https://doi.org/10.3390/medicina58020187
Myrda K, Buchta P, Błachut A, Skrzypek M, Gąsior M. Temporary Trends Concerning the Extent and Efficacy of Atrial Fibrillation Ablation Using Radiofrequency Energy in a Polish Single-Center Experience. Medicina. 2022; 58(2):187. https://doi.org/10.3390/medicina58020187
Chicago/Turabian StyleMyrda, Krzysztof, Piotr Buchta, Aleksandra Błachut, Michał Skrzypek, and Mariusz Gąsior. 2022. "Temporary Trends Concerning the Extent and Efficacy of Atrial Fibrillation Ablation Using Radiofrequency Energy in a Polish Single-Center Experience" Medicina 58, no. 2: 187. https://doi.org/10.3390/medicina58020187
APA StyleMyrda, K., Buchta, P., Błachut, A., Skrzypek, M., & Gąsior, M. (2022). Temporary Trends Concerning the Extent and Efficacy of Atrial Fibrillation Ablation Using Radiofrequency Energy in a Polish Single-Center Experience. Medicina, 58(2), 187. https://doi.org/10.3390/medicina58020187