
Digital Workflow for Implant Placement and Immediate Chairside Provisionalization of a Novel Implant System without Abutment—A Case Report


Abstract
1. Introduction
2. Case Report
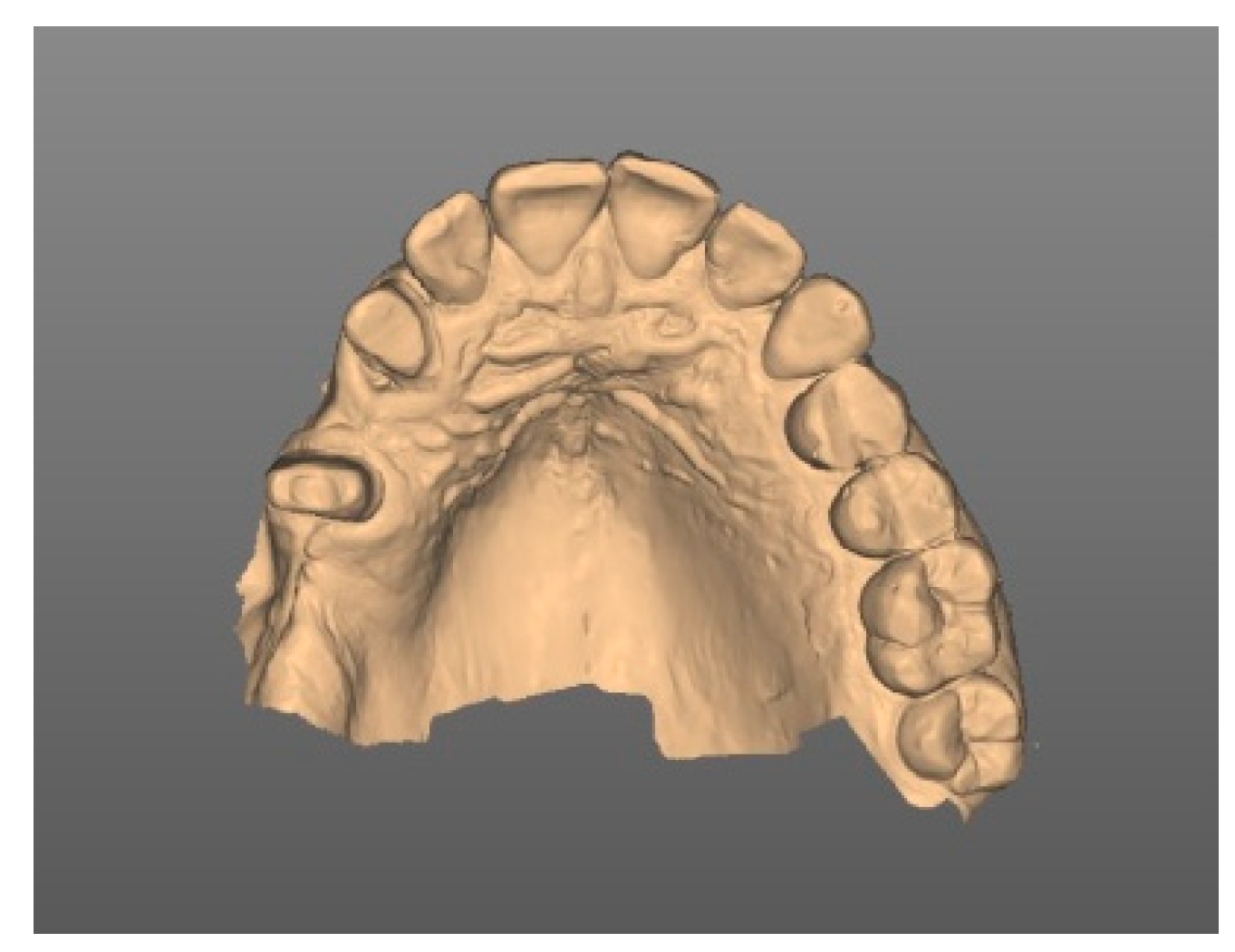
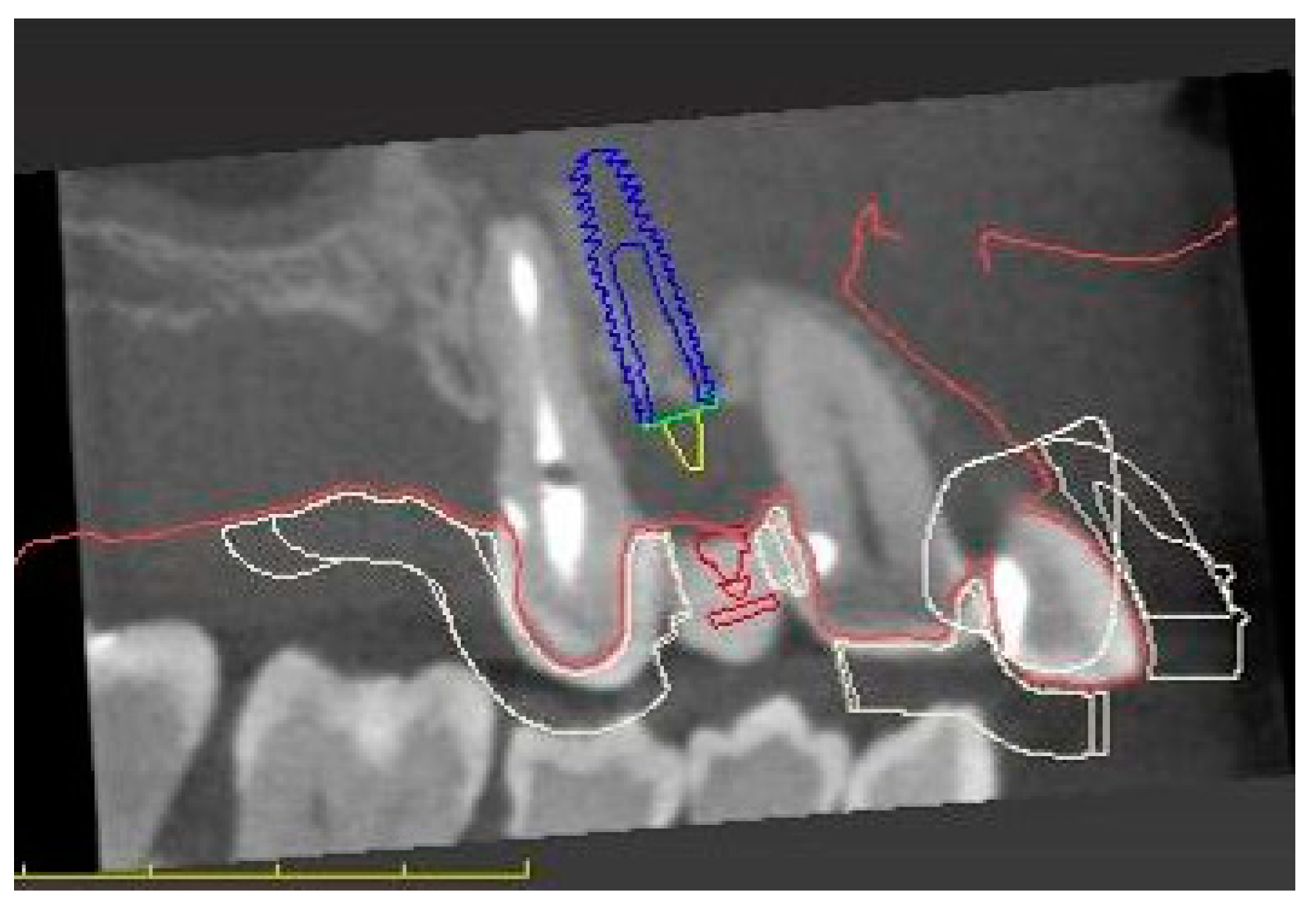
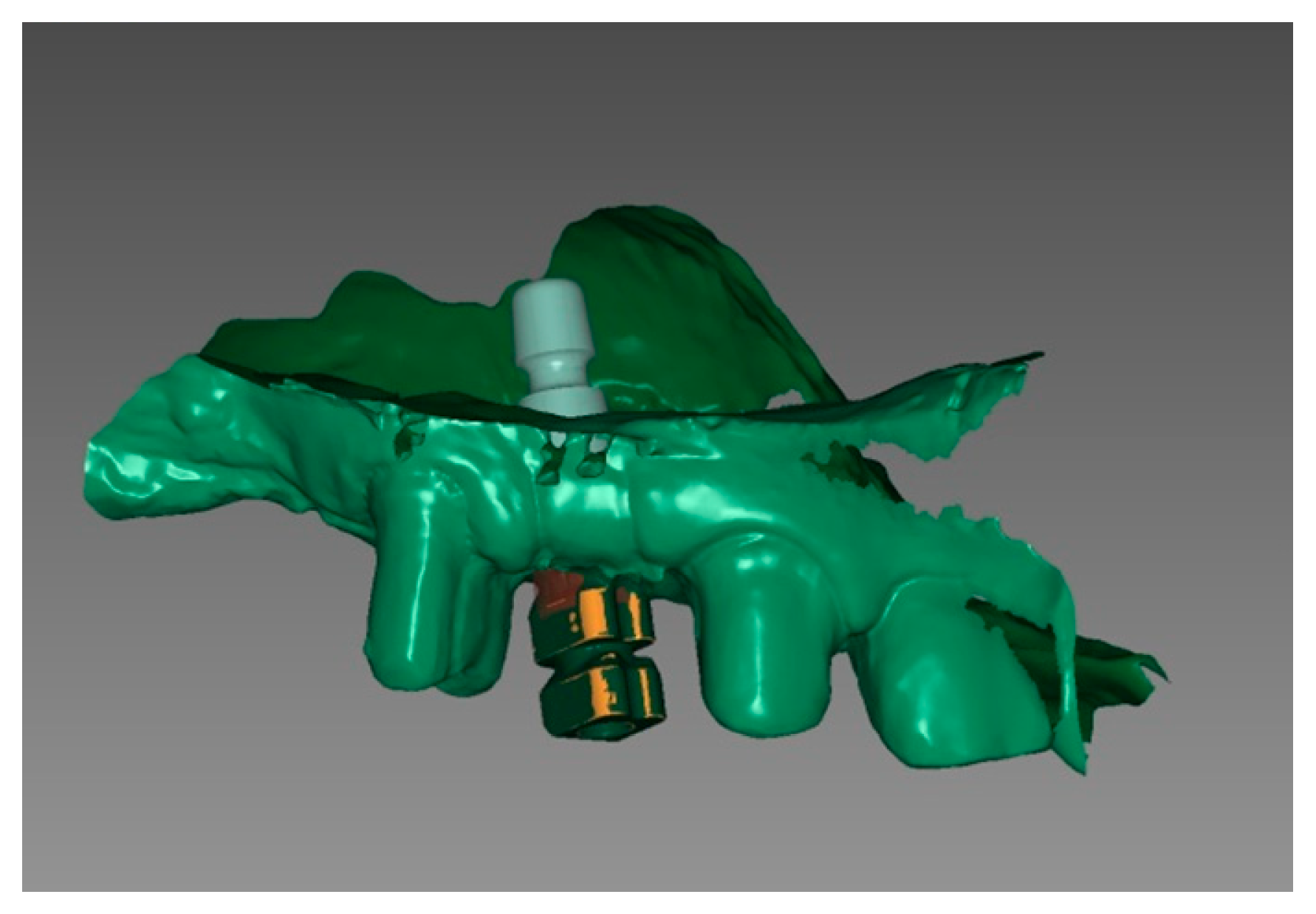
3. Diagnostic and Planning Procedures
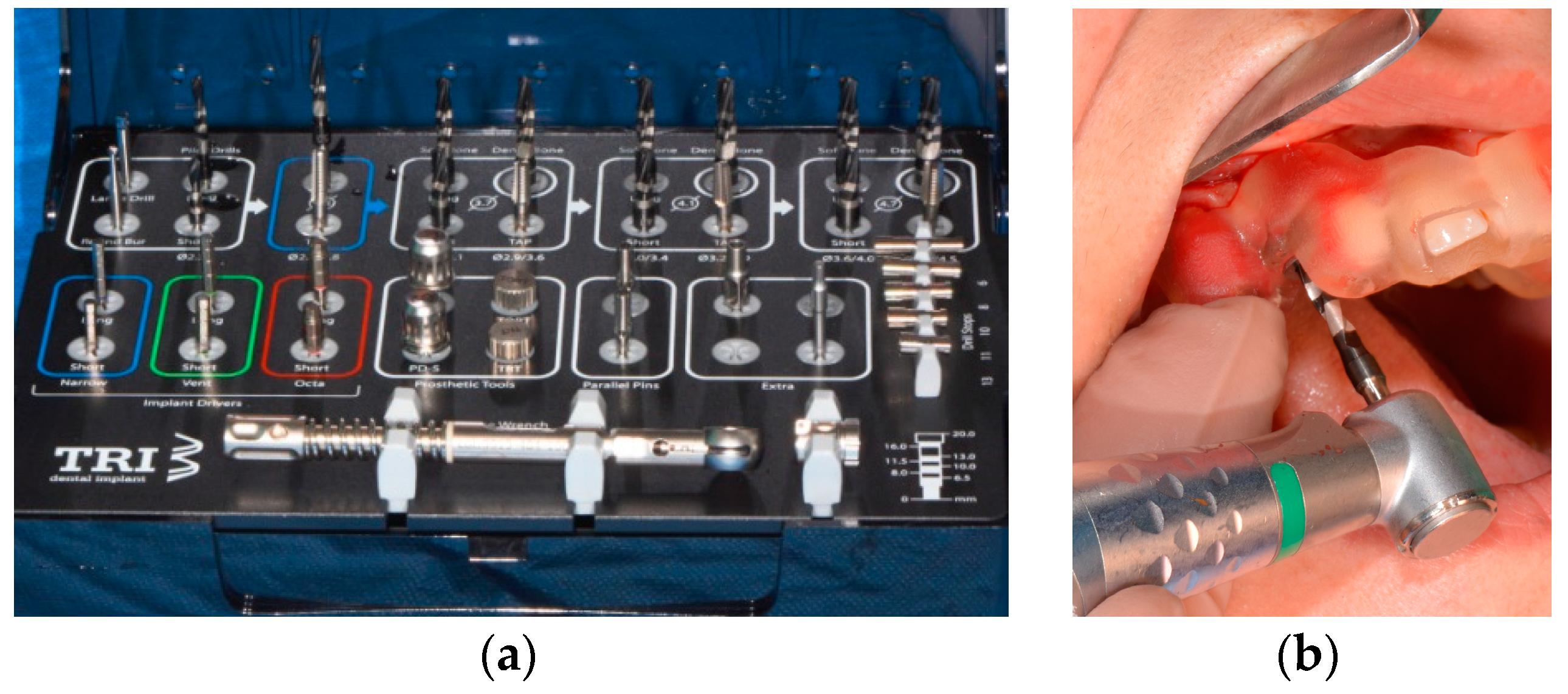
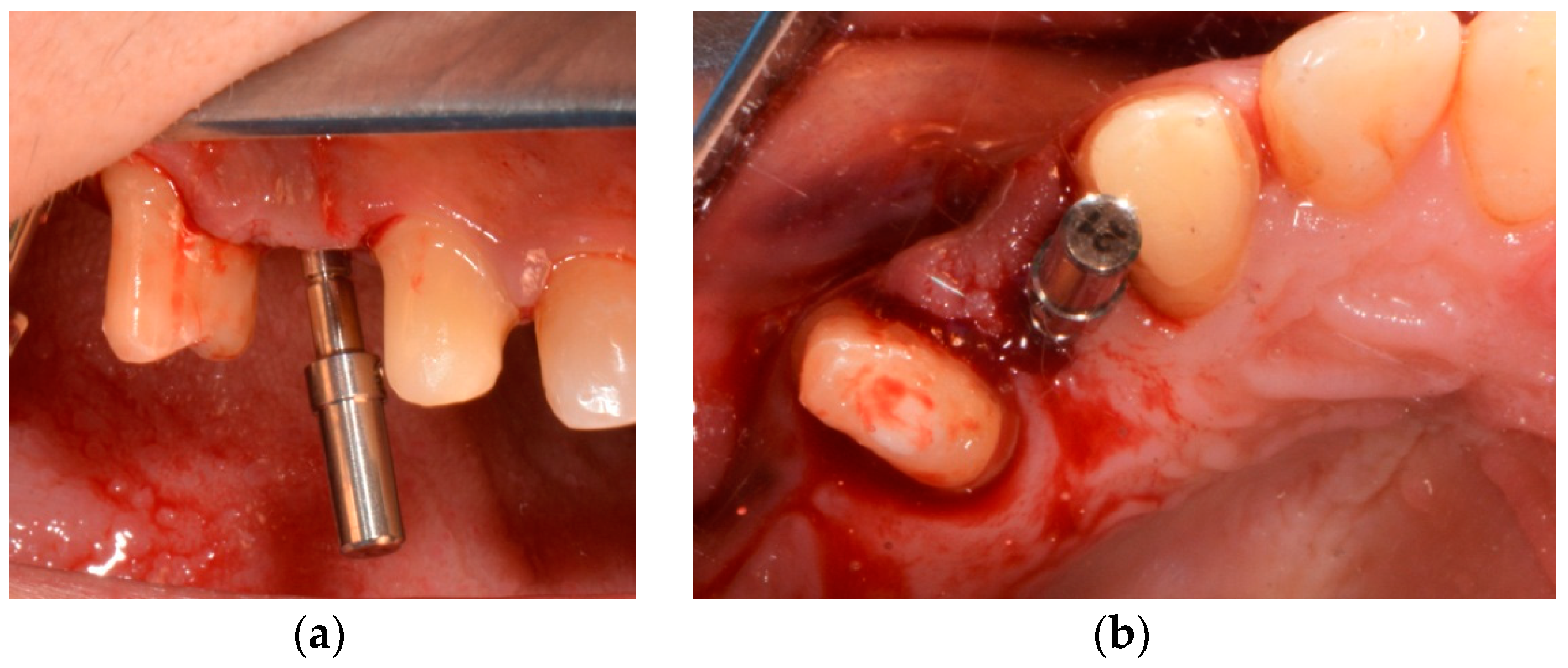
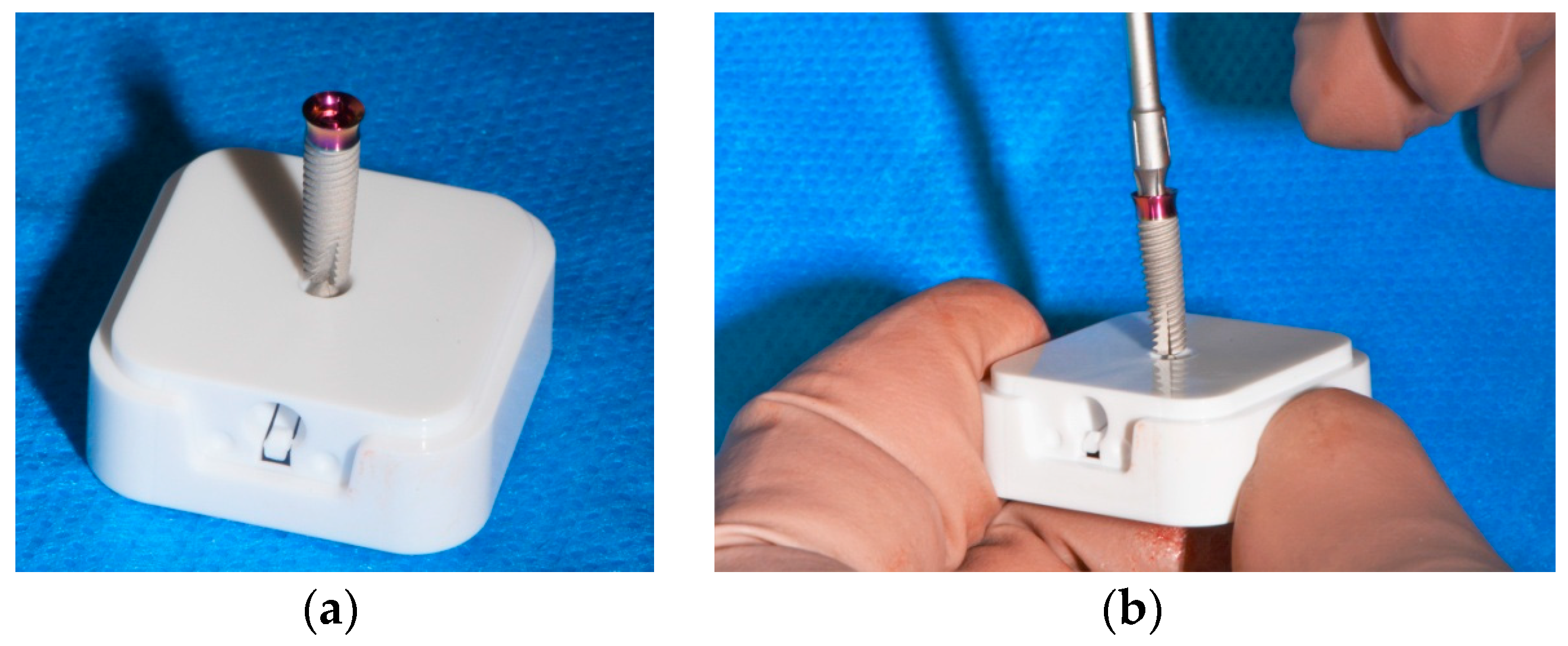
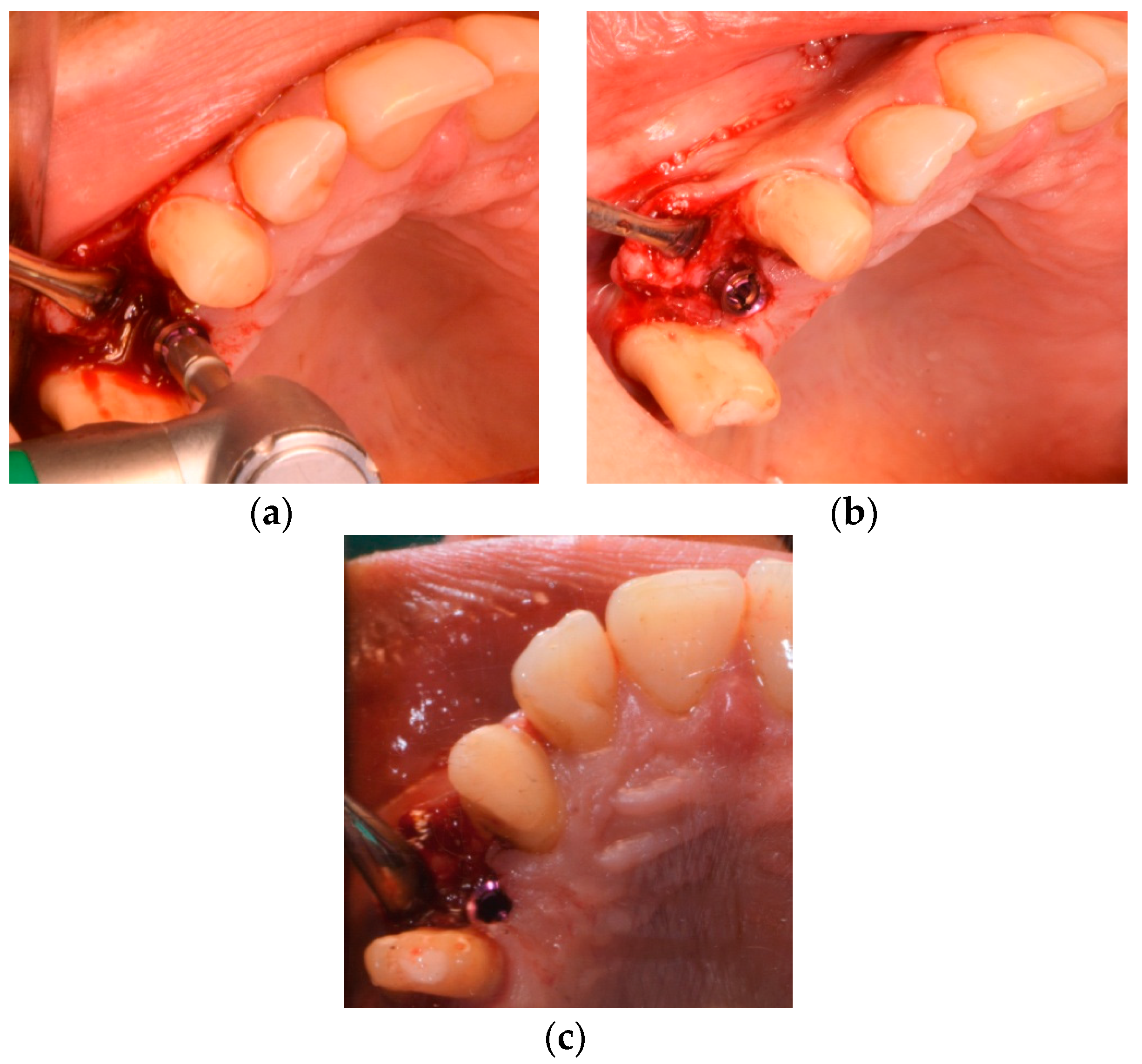
4. Surgical Procedures
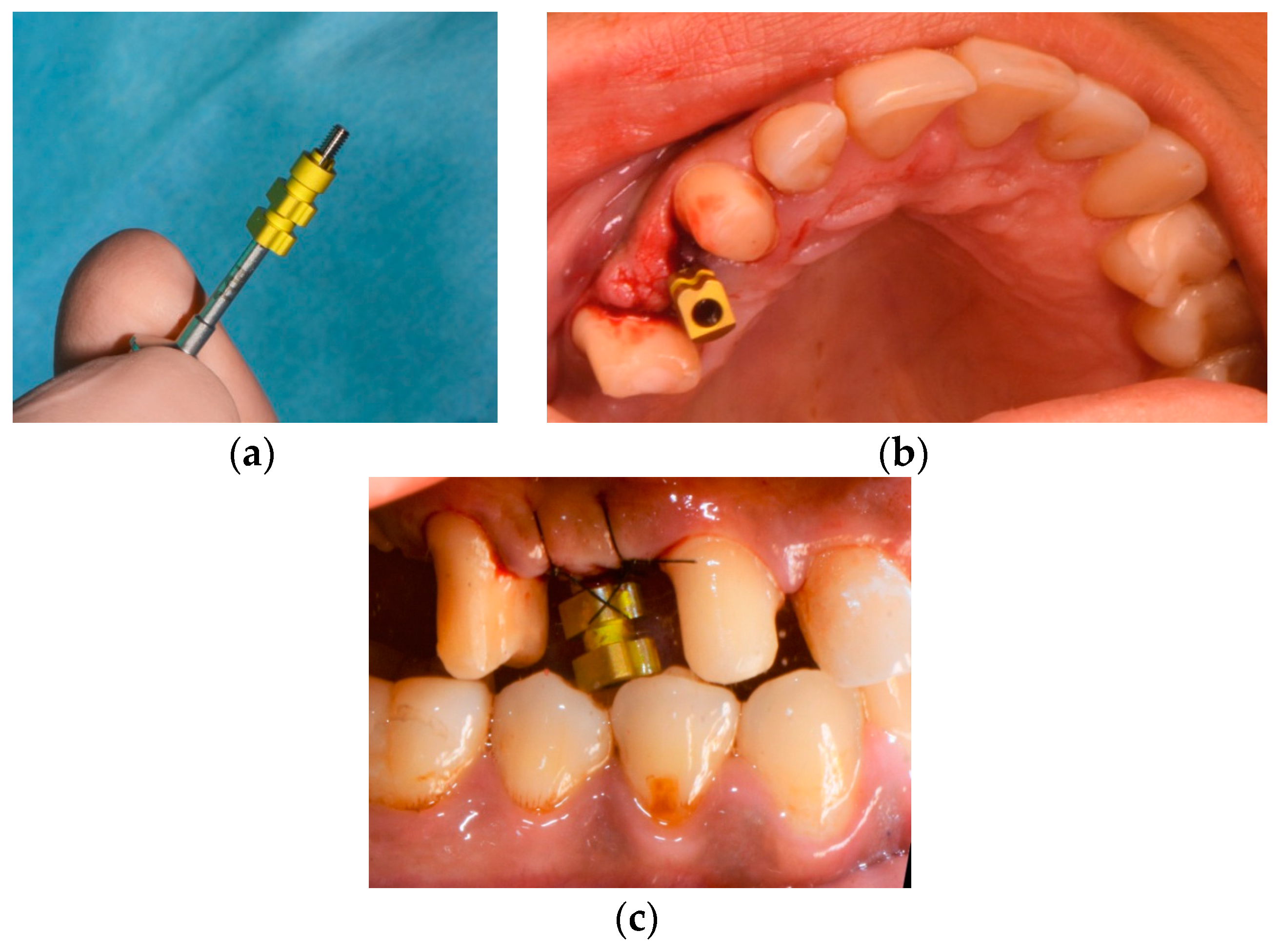
5. Restorative Procedures
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CAD/CAM | Computer-Aided Design/Computer Aided Manufacturing |
| FDP | Fixed dental prosthesis |
| LTT | Long-term temporary |
| CBCT | Cone beam computed tomography |
| DICOM | Digital Imaging and Communications in Medicine |
| PTFE | Polytetrafluorethylen |
References
- Davidowitz, G.; Kotick, P.G. The Use of CAD/CAM in Dentistry. Dent. Clin. N. Am. 2011, 55, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Priest, G. Virtual-designed and computer-milled implant abutments. J. Oral Maxillofac. Surg. 2005, 63, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, T.A. Materials in digital dentistry-a review. J. Esthet. Restor. Dent. 2020, 32, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Blatz, M.B.; Conejo, J. The current state of chairside digital dentistry and materials. Dent. Clin. N. Am. 2019, 63, 175–197. [Google Scholar] [CrossRef]
- Baroudi, K.; Ibraheem, S.N. Assessment of chair-side computer-aided design and computer-aided manufacturing restorations: A review of the literature. J. Int. Oral Health 2015, 7, 96–104. [Google Scholar]
- Kallala, R.; Chaouch, M.H.; Nasr, K.; Courset, T. Step-by-step esthetic rehabilitation with chairside system. Case Rep. Dent. 2021, 2021, 5558158. [Google Scholar] [CrossRef]
- Reda, R.; Zanza, A.; Cicconetti, A.; Bhandi, S.; Guarnieri, R.; Testarelli, L.; Di Nardo, D. A systematic review of cementation techniques to minimize cement excess in cement-retained implant restorations. Methods Protoc. 2022, 5, 9. [Google Scholar] [CrossRef]
- Troedhan, A.; Skiba, D.; Ziad, M.; Wainwright, M. Can cbct-bone-densitometry predict implant stability in augmented sinus-sites? Results of a randomized clinical trial. Clin. Oral Implant. Res. 2019, 30, 10. [Google Scholar] [CrossRef]
- Viegas, V.N.; Dutra, V.; Pagnoncelli, R.; De Oliveira, M.G. Transference of virtual planning and planning over biomedical prototypes for dental implant placement using guided surgery. Clin. Oral Implant. Res. 2010, 21, 290–295. [Google Scholar] [CrossRef]
- Schnitman, P.A.; Wohrle, P.S.; Rubenstein, J.E. Immediate fixed interim prostheses supported by two-stage threaded implants: Methodology and results. J. Oral Implantol. 1990, 16, 96–105. [Google Scholar]
- Schnitman, P.A.; Wöhrle, P.S.; E Rubenstein, J.; DaSilva, J.D.; Wang, N.H. Ten-year results for branemark implants immediately loaded with fixed prostheses at implant placement. Int. J. Oral Maxillofac. Implant. 1997, 12, 495–503. [Google Scholar]
- Tarnow, D.P.; Emtiaz, S.; Classi, A. Immediate loading of threaded implants at stage 1 surgery in edentulous arches: Ten consecutive case reports with 1- to 5-year data. Int. J. Oral Maxillofac. Implant. 1997, 12, 319–324. [Google Scholar]
- Saba, S. Anatomically correct soft tissue profiles using fixed detachable provisional implant restorations. J. Can. Dent. Assoc. 1997, 63, 767–768. [Google Scholar]
- Breeding, L.C.; Dixon, D.L. Transfer of gingival contours to a master cast. J. Prosthet. Dent. 1996, 75, 341–343. [Google Scholar] [CrossRef]
- Neale, D.; Chee, W.W. Development of implant soft tissue emergence profile: A technique. J. Prosthet. Dent. 1994, 71, 364–368. [Google Scholar] [CrossRef]
- Capp, N.J. The diagnostic use of provisional restorations. Restor. Dent. 1985, 1, 92, 94–98. [Google Scholar]
- Moscovitch, M.S.; Saba, S. The use of a provisional restoration in implant dentistry: A clinical report. Int. J. Oral Maxillofac. Implant. 1996, 11, 395–399. [Google Scholar]
- Edelhoff, D.; Beuer, F.; Schweiger, J.; Brix, O.; Stimmelmayr, M.; Guth, J.-F. Cad/cam-generated high-density polymer restorations for the pretreatment of complex cases: A case report. Quintessence Int. 2012, 43, 457–467. [Google Scholar]
- Gomez-Meda, R.; Esquivel, J.; Blatz, M.B. The esthetic biological contour concept for implant restoration emergence profile design. J. Esthet. Restor. Dent. 2021, 33, 173–184. [Google Scholar] [CrossRef]
- Magne, P.; Kim, T.H.; Cascione, D.; Donovan, T.E. Immediate dentin sealing improves bond strength of indirect restorations. J. Prosthet. Dent. 2005, 94, 511–519. [Google Scholar] [CrossRef]
- Lin, W.-S.; Ercoli, C. A technique for indirect fabrication of an implant-supported, screw-retained, fixed provisional restoration in the esthetic zone. J. Prosthet. Dent. 2009, 102, 393–396. [Google Scholar] [CrossRef]
- Mack, M.R. Vertical dimension: A dynamic concept based on facial form and oropharyngeal function. J. Prosthet. Dent. 1991, 66, 478–485. [Google Scholar] [CrossRef]
- Fasbinder, D. Using digital technology to enhance restorative dentistry. Compend. Contin. Educ. Dent. 2012, 33, 666–668, 670, 672. [Google Scholar]
- Skramstad, M.J. Welcome to cerec primescan ac. Int. J. Comput. Dent. 2019, 22, 69–78. [Google Scholar] [PubMed]
- Aziz, A.; El-Mowafy, O.; Paredes, S. Clinical outcomes of lithium disilicate glass-ceramic crowns fabricated with cad/cam technology: A systematic review. Dent. Med. Probl. 2020, 57, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital dentistry: An overview of recent developments for cad/cam generated restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef]
- Ireland, M.F.; Dixon, D.L.; Breeding, L.C.; Ramp, M.H. In vitro mechanical property comparison of four resins used for fabrication of provisional fixed restorations. J. Prosthet. Dent. 1998, 80, 158–162. [Google Scholar] [CrossRef]
- Koksal, T.; Dikbas, I.; Kazazoglu, E. Alternative restorative approach for treatment of patient with extremely worn dentition. N. Y. State Dent. J. 2009, 75, 52–55. [Google Scholar]
- Schmidlin, P.R.; Filli, T.; Imfeld, C.; Tepper, S.; Attin, T. Three-year evaluation of posterior vertical bite reconstruction using direct resin composite-a case series. Oper. Dent. 2009, 34, 102–108. [Google Scholar] [CrossRef]
- Keul, C.; Müller-Hahl, M.; Eichberger, M.; Liebermann, A.; Roos, M.; Edelhoff, D.; Stawarczyk, B. Impact of different adhesives on work of adhesion between cad/cam polymers and resin composite cements. J. Dent. 2014, 42, 1105–1114. [Google Scholar] [CrossRef]
- Reda, R.; Zanza, A.; Galli, M.; De Biase, A.; Testarelli, L.; Di Nardo, D. Applications and clinical behavior of biohpp in prosthetic dentistry: A short review. J. Compos. Sci. 2022, 6, 90. [Google Scholar] [CrossRef]
- Esquivel, J.; Meda, R.G.; Blatz, M.B. The impact of 3d implant position on emergence profile design. Int. J. Periodontics Restor. Dent. 2021, 41, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, A.M. Digital technologies for dental implant treatment planning and guided surgery. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 319–340. [Google Scholar] [CrossRef]
- Al Yafi, F.; Camenisch, B.; Al-Sabbagh, M. Is digital guided implant surgery accurate and reliable? Dent. Clin. N. Am. 2019, 63, 381–397. [Google Scholar] [CrossRef]
- Donker, V.J.J.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J.A. Digital workflow for immediate implant placement and chairside provisionalization in the esthetic zone. Case Rep. Dent. 2022, 2022, 5114332. [Google Scholar] [CrossRef] [PubMed]
- Gamborena, I.; Sasaki, Y.; Blatz, M.B. Predictable immediate implant placement and restoration in the esthetic zone. J. Esthet. Restor. Dent. 2021, 33, 158–172. [Google Scholar] [CrossRef]
- Younes, F.; Cosyn, J.; De Bruyckere, T.; Cleymaet, R.; Bouckaert, E.; Eghbali, A. A randomized controlled study on the accuracy of free-handed, pilot-drill guided and fully guided implant surgery in partially edentulous patients. J. Clin. Periodontol. 2018, 45, 721–732. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 416–435. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Schmid, B.; Belser, U.C.; Lussi, A.; Buser, D. Early loading of non-submerged titanium implants with a sandblasted and acid-etched surface. 5-year results of a prospective study in partially edentulous patients. Clin. Oral Implant. Res. 2005, 16, 631–638. [Google Scholar] [CrossRef]
- Linkevicius, T. Zero Bone Loss-Knochenerhaltende Behandlungskonzepte; Quintessence Publishing: Berlin, Germany, 2021. [Google Scholar]
- Del Amo, F.S.-L.; Lin, G.-H.; Monje, A.; Galindo-Moreno, P.; Wang, H.-L. Influence of soft tissue thickness on peri-implant marginal bone loss: A systematic review and meta-analysis. J. Periodontol. 2016, 87, 690–699. [Google Scholar] [CrossRef]
- Bressan, E.; Paniz, G.; Lops, D.; Corazza, B.; Romeo, E.; Favero, G.A. Influence of abutment material on the gingival color of implant-supported all-ceramic restorations: A prospective multicenter study. Clin. Oral Implant. Res. 2011, 22, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Meijer, H.J.A.; Stellingsma, K.; Meijndert, L.; Raghoebar, G.M. A new index for rating aesthetics of implant-supported single crowns and adjacent soft tissues--the implant crown aesthetic index. Clin. Oral Implant. Res. 2005, 16, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score. Clin. Oral Implant. Res. 2005, 16, 639–644. [Google Scholar] [CrossRef] [PubMed]
- E Jung, R.; Holderegger, C.; Sailer, I.; Khraisat, A.; Suter, A.; Hämmerle, C.H.F. The effect of all-ceramic and porcelain-fused-to-metal restorations on marginal peri-implant soft tissue color: A randomized controlled clinical trial. Int. J. Periodontics Restor. Dent. 2008, 28, 357–365. [Google Scholar]
- Martínez-Rus, F.; Prieto, M.; Salido, M.; Madrigal, C.; Özcan, M.; Pradíes, G. A clinical study assessing the influence of anodized titanium and zirconium dioxide abutments and peri-implant soft tissue thickness on the optical outcome of implant-supported lithium disilicate single crowns. Int. J. Oral Maxillofac. Implant. 2017, 32, 156–163. [Google Scholar] [CrossRef]
- Sailer, I.; Zembic, A.; Jung, R.E.; Hämmerle, C.H.F.; Mattiola, A. Single-tooth implant reconstructions: Esthetic factors influencing the decision between titanium and zirconia abutments in anterior regions. Eur. J. Esthet. Dent. 2007, 2, 296–310. [Google Scholar] [PubMed]
- López-Píriz, R.; Cabal, B.; Goyos-Ball, L.; Fernández, A.; Bartolomé, J.F.; Moya, J.S.; Torrecillas, R. Current state-of-the-art and future perspectives of the three main modern implant-dentistry concerns: Aesthetic requirements, mechanical properties, and peri-implantitis prevention. J. Biomed. Mater. Res. A 2019, 107, 1466–1475. [Google Scholar] [CrossRef]
- Sailer, I.; Asgeirsson, A.G.; Thoma, D.S.; Fehmer, V.; Aspelund, T.; Özcan, M.; Pjetursson, B.E. Fracture strength of zirconia implant abutments on narrow diameter implants with internal and external implant abutment connections: A study on the titanium resin base concept. Clin. Oral Implant. Res. 2018, 29, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Rosentritt, M.; Raab, P.; Hahnel, S.; Stöckle, M.; Preis, V. In-vitro performance of cad/cam-fabricated implant-supported temporary crowns. Clin. Oral Investig. 2017, 21, 2581–2587. [Google Scholar] [CrossRef] [PubMed]
- Staubli, N.; Walter, C.; Schmidt, J.C.; Weiger, R.; Zitzmann, N.U. Excess cement and the risk of peri-implant disease-a systematic review. Clin. Oral Implant. Res. 2017, 28, 1278–1290. [Google Scholar] [CrossRef]
- Nascimento, C.D.; Ikeda, L.N.; Pita, M.S.; e Silva, R.C.P.; Pedrazzi, V.; Junior, R.F.D.A.; Ribeiro, R.F. Marginal fit and microbial leakage along the implant-abutment interface of fixed partial prostheses: An in vitro analysis using checkerboard DNA-DNA hybridization. J. Prosthet. Dent. 2015, 114, 831–838. [Google Scholar] [CrossRef]
- Ioannidis, A.; Gil, A.; Hämmerle, C.H.; E Jung, R.; Zinelis, S.; Eliades, G. Effect of thermomechanical loading on the cementation interface of implant-supported cad/cam crowns luted to titanium abutments. Int. J. Prosthodont. 2020, 33, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Steinebrunner, L.; Wolfart, S.; Bössmann, K.; Kern, M. In vitro evaluation of bacterial leakage along the implant-abutment interface of different implant systems. Int. J. Oral Maxillofac. Implant. 2005, 20, 875–881. [Google Scholar]
- Pereira, J.; Morsch, C.; Henriques, B.; Nascimento, R.M.D.; Benfatti, C.; Silva, F.; López-López, J.; Souza, J. Removal torque and biofilm accumulation at two dental implant-abutment joints after fatigue. Int. J. Oral Maxillofac. Implant. 2016, 31, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Perrotti, V.; Piattelli, A.; Iaculli, F.; Iezzi, G. Sealing capability of implant-abutment junction under cyclic loading: A toluidine blue in vitro study. J. Appl. Biomater. Funct. Mater. 2015, 13, e293–e295. [Google Scholar] [CrossRef]
- Nascimento, C.D.; Miani, P.K.; Pedrazzi, V.; Gonçalves, R.B.; Ribeiro, R.F.; Faria, A.C.L.; Macedo, A.P.; De Albuquerque, R.F. Leakage of saliva through the implant-abutment interface: In vitro evaluation of three different implant connections under unloaded and loaded conditions. Int. J. Oral Maxillofac. Implant. 2012, 27, 551–560. [Google Scholar]
- Verdugo, C.L.; Núñez, G.J.; Avila, A.A.; Martín, C.L.S. Microleakage of the prosthetic abutment/implant interface with internal and external connection: In vitro study. Clin. Oral Implant. Res. 2014, 25, 1078–1083. [Google Scholar] [CrossRef]
- Mishra, S.K.; Chowdhary, R.; Kumari, S. Microleakage at the different implant abutment interface: A systematic review. J. Clin. Diagn. Res. 2017, 11, ZE10–ZE15. [Google Scholar] [CrossRef]
- Jung, R.E.; Al-Nawas, B.; Araujo, M.; Ortiz, G.A.; Barter, S.; Brodala, N.; Chappuis, V.; Chen, B.; De Souza, A.; Faria-Almeida, R.; et al. Group 1 iti consensus report: The influence of implant length and design and medications on clinical and patient-reported outcomes. Clin. Oral Implant. Res. 2018, 29, 69–77. [Google Scholar] [CrossRef]
- Jokstad, A.; Ganeles, J. Systematic review of clinical and patient-reported outcomes following oral rehabilitation on dental implants with a tapered compared to a non-tapered implant design. Clin. Oral Implant. Res. 2018, 29, 41–54. [Google Scholar] [CrossRef]
- Schiegnitz, E.; Al-Nawas, B. Narrow-diameter implants: A systematic review and meta-analysis. Clin Oral Implants Res. 2018, 29, 21–40. [Google Scholar] [CrossRef] [PubMed]
- Lodding, D.W. Long-term esthetic provisional restorations in dentistry. Curr. Opin. Cosmet. Dent. 1997, 4, 16–21. [Google Scholar] [PubMed]
- Güth, J.-F.; E Silva, J.S.A.; Ramberger, M.; Beuer, F.; Edelhoff, D. Treatment concept with cad/cam-fabricated high-density polymer temporary restorations. J. Esthet. Restor. Dent. 2012, 24, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Güth, J.F.; E Silva, J.S.A.; F Beuer, F.; Edelhoff, D. Enhancing the predictability of complex rehabilitation with a removable cad/cam-fabricated long-term provisional prosthesis: A clinical report. J. Prosthet. Dent. 2012, 107, 1–6. [Google Scholar] [CrossRef]
- Stawarczyk, B.; Özcan, M.; Trottmann, A.; Schmutz, F.; Roos, M.; Hämmerle, C. Two-body wear rate of cad/cam resin blocks and their enamel antagonists. J. Prosthet. Dent. 2013, 109, 325–332. [Google Scholar] [CrossRef]
- Attia, A.; Abdelaziz, K.M.; Freitag, S.; Kern, M. Fracture load of composite resin and feldspathic all-ceramic cad/cam crowns. J. Prosthet. Dent. 2006, 95, 117–123. [Google Scholar] [CrossRef]
- Wimmer, T.; Ender, A.; Roos, M.; Stawarczyk, B. Fracture load of milled polymeric fixed dental prostheses as a function of connector cross-sectional areas. J. Prosthet. Dent. 2013, 110, 288–295. [Google Scholar] [CrossRef]
- Kurbad, A. Cad/cam-based polymer provisionals as treatment adjuncts. Int. J. Comput. Dent. 2013, 16, 327–346. [Google Scholar]
- Wiegand, A.; Stucki, L.; Hoffmann, R.; Attin, T.; Stawarczyk, B. Repairability of cad/cam high-density pmma- and composite-based polymers. Clin. Oral Investig. 2015, 19, 2007–2013. [Google Scholar] [CrossRef]
- Joda, T.; Brägger, U. Time-efficiency analysis comparing digital and conventional workflows for implant crowns: A prospective clinical crossover trial. Int. J. Oral Maxillofac. Implant. 2015, 30, 1047–1053. [Google Scholar] [CrossRef]
- Schepke, U.; Meijer, H.J.A.; Kerdijk, W.; Cune, M.S. Digital versus analog complete-arch impressions for single-unit premolar implant crowns: Operating time and patient preference. J. Prosthet. Dent. 2015, 114, 403–406.e1. [Google Scholar] [CrossRef] [PubMed]
- Mühlemann, S.; Kraus, R.D.; Hämmerle, C.H.F.; Thoma, D.S. Is the use of digital technologies for the fabrication of implant-supported reconstructions more efficient and/or more effective than conventional techniques: A systematic review. Clin. Oral Implant. Res. 2018, 29, 184–195. [Google Scholar] [CrossRef] [PubMed]
- Preis, V.; Kammermeier, A.; Handel, G.; Rosentritt, M. In vitro performance of two-piece zirconia implant systems for anterior application. Dent. Mater. 2016, 32, 765–774. [Google Scholar] [CrossRef]
- SSilva, G.C.; Cornacchia, T.M.; de Magalhães, C.S.; Bueno, A.C.; Moreira, A. Biomechanical evaluation of screw- and cement-retained implant-supported prostheses: A nonlinear finite element analysis. J. Prosthet. Dent. 2014, 112, 1479–1488. [Google Scholar] [CrossRef]
- Wittneben, J.-G.; Millen, C.; Brägger, U. Clinical performance of screw- versus cement-retained fixed implant-supported reconstructions--a systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 84–98. [Google Scholar] [CrossRef]
- Torrado, E.; Ercoli, C.; Al Mardini, M.; Graser, G.N.; Tallents, R.H.; Cordaro, L. A comparison of the porcelain fracture resistance of screw-retained and cement-retained implant-supported metal-ceramic crowns. J. Prosthet. Dent. 2004, 91, 532–537. [Google Scholar] [CrossRef]
- Bijjargi, S.; Chowdhary, R. Stress dissipation in the bone through various crown materials of dental implant restoration: A 2-d finite element analysis. J. Investig. Clin. Dent. 2013, 4, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Allum, S.R.; Tomlinson, R.A.; Joshi, R. The impact of loads on standard diameter, small diameter and mini implants: A comparative laboratory study. Clin. Oral Implant. Res. 2008, 19, 553–559. [Google Scholar] [CrossRef]
- E Quek, C.; Tan, K.B.C.; I Nicholls, J. Load fatigue performance of a single-tooth implant abutment system: Effect of diameter. Int. J. Oral Maxillofac. Implant. 2006, 21, 929–936. [Google Scholar]
- Sohrabi, K.; Mushantat, A.; Esfandiari, S.; Feine, J. How successful are small-diameter implants? A literature review. Clin. Oral Implant. Res. 2012, 23, 515–525. [Google Scholar] [CrossRef]
- Klein, M.O.; Schiegnitz, E.; Al-Nawas, B. Systematic review on success of narrow-diameter dental implants. Int. J. Oral Maxillofac. Implant. 2014, 29, 43–54. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Phase | Procedures |
|---|---|
| Gender | female |
| Age | 32 |
| Implant position | Tooth 14 (upper left first premolar) |
| Implant type | Tissue-Level (Matrix, TRI Swiss Implants) |
| Implant diameter platform | 3.7 mm |
| Implant diameter enossal | 3.3 mm |
| Implant length | 11.5 mm |
| Treatment Phase | Procedures |
|---|---|
| Diagnostic | Intraoral scans |
| Cone beam computed tomography scan | |
| Planning | Digital set-up |
| Digital prosthetically driven implant planning | |
| Manufacturing of the surgical template | |
| Surgical | Computer-assisted implant surgery |
| Restorative | Intraoral scans with a scanbody |
| Chairside, computer-aided design and milling of the provisionalization | |
| Placement of the chairside LTT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hölken, F.; Al-Nawas, B.; Meereis, M.; Bjelopavlovic, M. Digital Workflow for Implant Placement and Immediate Chairside Provisionalization of a Novel Implant System without Abutment—A Case Report. Medicina 2022, 58, 1612. https://doi.org/10.3390/medicina58111612
Hölken F, Al-Nawas B, Meereis M, Bjelopavlovic M. Digital Workflow for Implant Placement and Immediate Chairside Provisionalization of a Novel Implant System without Abutment—A Case Report. Medicina. 2022; 58(11):1612. https://doi.org/10.3390/medicina58111612
Chicago/Turabian StyleHölken, Felicitas, Bilal Al-Nawas, Manuela Meereis, and Monika Bjelopavlovic. 2022. "Digital Workflow for Implant Placement and Immediate Chairside Provisionalization of a Novel Implant System without Abutment—A Case Report" Medicina 58, no. 11: 1612. https://doi.org/10.3390/medicina58111612
APA StyleHölken, F., Al-Nawas, B., Meereis, M., & Bjelopavlovic, M. (2022). Digital Workflow for Implant Placement and Immediate Chairside Provisionalization of a Novel Implant System without Abutment—A Case Report. Medicina, 58(11), 1612. https://doi.org/10.3390/medicina58111612