
Mid-Term Outcomes of Laparoscopic Gastric Greater Curvature Plication versus Roux-en-Y Gastric Bypass: Weight Loss, Gastrointestinal Symptoms, and Health-Related Quality of Life

Abstract
:1. Introduction
2. Materials and Methods
2.1. Surgical Technique
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization (WHO). Obesity and Overweight. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 21 March 2020).
- Buchwald, H. Consensus Conference Panel. Consensus conference statement bariatric surgery for morbid obesity: Health implications for patients, health professionals, and third-party payers. Surg. Obes. Relat. Dis. 2005, 1, 371–381. [Google Scholar] [CrossRef]
- Talebpour, M.; Amoli, B.S. Laparoscopic Total Gastric Vertical Plication in Morbid Obesity. J. Laparoendosc. Adv. Surg. Tech. 2007, 17, 793–798. [Google Scholar] [CrossRef]
- El Soueidy, T.; Kassir, R.; Nakhoul, M.; Balian, A.; Nunziante, M.; Safieddine, M.; Perlemuter, G.; Lainas, P.; Dagher, I. Laparoscopic Greater Curvature Plication for the Treatment of Obesity: A Systematic Review. Obes. Surg. 2021, 31, 1168–1182. [Google Scholar] [CrossRef]
- Suarez, D.F.; Gangemi, A. How Bad Is “Bad”? A Cost Consideration and Review of Laparoscopic Gastric Plication Versus Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2021, 31, 307–316. [Google Scholar] [CrossRef]
- Darabi, S.; Talebpour, M.; Zeinoddini, A.; Heidari, R. Laparoscopic gastric plication versus mini-gastric bypass surgery in the treatment of morbid obesity: A randomized clinical trial. Surg. Obes. Relat. Dis. 2013, 9, 914–919. [Google Scholar] [CrossRef]
- Casajoana, A.; Guerrero-Pérez, F.; De Gordejuela, A.G.R.; Admella, V.; Sorribas, M.; Vidal-Alabró, A.; Virgili, N.; Urdiales, R.L.; Montserrat, M.; Pérez-Maraver, M.; et al. Role of Gastrointestinal Hormones as a Predictive Factor for Long-Term Diabetes Remission: Randomized Trial Comparing Metabolic Gastric Bypass, Sleeve Gastrectomy, and Greater Curvature Plication. Obes. Surg. 2021, 31, 1733–1744. [Google Scholar] [CrossRef] [PubMed]
- Mickevičius, A.; Žilvinas, E.; Kiudelis, M.; Jonaitis, L.; Kupčinskas, L.; Maleckas, A.; Pundzius, J. Influence of wrap length on the effectiveness of Nissen and Toupet fundoplication: A prospective randomized study. Surg. Endosc. 2008, 22, 2269–2276. [Google Scholar] [CrossRef] [PubMed]
- Brethauer, S.A.; Kim, J.; El Chaar, M.; Papasavas, P.; Eisenberg, D.; Rogers, A.; Ballem, N.; Kligman, M.; Kothari, S.; ASMBS Clinical Issues Committee. Standardized outcomes reporting in metabolic and bariatric surgery. Obes. Surg. 2015, 25, 587–606. [Google Scholar] [CrossRef]
- Genuth, S.; Alberti, K.G.; Bennett, P.; Buse, J.; Defronzo, R.; Kahn, R.; Kitzmiller, J.; Knowler, W.C.; Lebovitz, H.; Lernmark, A.; et al. Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 2003, 26, 3160–3167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svedlund, J.; Sjodin, I.; Dotevall, G. GSRS—A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef]
- Available online: https://www.economicsnetwork.ac.uk/health/EQ_5D_index_calculator.xls (accessed on 21 August 2021).
- Gudaityte, R.; Adamonis, K.; Maleckas, A. Laparoscopic Gastric Greater Curvature Plication: Intermediate Results and Factors Associated with Failure. Obes. Surg. 2018, 28, 4087–4094. [Google Scholar] [CrossRef]
- Ibrahim, M.; Hany, M.; Zidan, A.; Abouelnasr, A.A.; Abu-Sheasha, G.A. Laparoscopic Sleeve Gastrectomy Versus Laparoscopic Greater Curvature Plication: A Long-Term Follow-up Study on the Complications, Body Mass Index Changes, Endoscopic Findings and Causes of Revision. Obes. Surg. 2021, 31, 5275–5285. [Google Scholar] [CrossRef]
- Talebpour, M.; Motamedi, S.M.K.; Talebpour, A.; Vahidi, H. Twelve year experience of laparoscopic gastric plication in morbid obesity: Development of the technique and patient outcomes. Ann. Surg. Innov. Res. 2012, 6, 7. [Google Scholar] [CrossRef] [Green Version]
- Chahal-Kummen, M.; Blom-Høgestøl, I.K.; Eribe, I.; Klungsøyr, O.; Kristinsson, J.; Mala, T. Abdominal pain and symptoms before and after Roux-en-Y gastric bypass. BJS Open 2019, 3, 317–326. [Google Scholar] [CrossRef] [Green Version]
- Thaher, O.; Hukauf, M.; Stroh, C. Propensity Score Matching Sleeve Gastrectomy vs. Gastric Bypass with 5 Years of Follow-Up. Obes. Surg. 2021, 31, 5156–5165. [Google Scholar] [CrossRef] [PubMed]
- Bauraitė, K.; Mikuckytė, D.; Gudaitytė, R.; Petereit, R.; Maleckas, A. Factors associated with quality of life and weight regain 12 years after Roux-en-Y gastric bypass. Surg. Endosc. 2021. [Google Scholar] [CrossRef] [PubMed]
- Chahal-Kummen, M.; Salte, O.B.K.; Hewitt, S.; Blom-Høgestøl, I.K.; Risstad, H.; Kristinsson, J.; Mala, T. Health benefits and risks during 10 years after Roux-en-Y gastric bypass. Surg. Endosc. 2020, 34, 5368–5376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heidari, R.; Talebpour, M.; Soleyman-Jahi, S.; Zeinoddini, A.; Moghaddam, A.S.; Talebpour, A. Outcomes of Reoperation After Laparoscopic Gastric Plication Failure. Obes. Surg. 2019, 29, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.C.; Jalilvand, A.; Wang, V.; Gupta, A.; Tamer, R.; Diaz, K.; Tamimi, M.; Needleman, B.; Noria, S. Influence of sociodemographic variables on weight loss outcomes up to 3-years following primary bariatric surgery. Surg. Endosc. 2021, 35, 5774–5786. [Google Scholar] [CrossRef] [PubMed]
- Carden, A.; Blum, K.; Arbaugh, C.J.; Trickey, A.; Eisenberg, D. Low socioeconomic status is associated with lower weight-loss outcomes 10-years after Roux-en-Y gastric bypass. Surg. Endosc. 2018, 33, 454–459. [Google Scholar] [CrossRef]
- Barranquero, A.G.; Cimpean, S.; Raglione, D.; Cadière, B.; Maréchal, M.-T.; Pau, L.; Bez, M.; Cadière, G.-B. Impact of the COVID-19 Pandemic and Lockdown on Gastric Bypass Results at 1-Year Follow-up. Obes. Surg. 2021, 31, 4511–4518. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Guide to the Methods of Technology Appraisal. 2013. Available online: https://www.nice.org.uk/process/pmg9/chapter/foreword (accessed on 21 October 2021).
- Xia, Q.; Campbell, J.A.; Ahmad, H.; Si, L.; De Graaff, B.; Otahal, P.; Palmer, A.J. Health state utilities for economic evaluation of bariatric surgery: A comprehensive systematic review and meta-analysis. Obes. Rev. 2020, 21. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| LGGCP n = 50 | LRYGB n = 62 | p-Value | |
|---|---|---|---|
| Sex F/M | 41/9 | 47/15 | 0.492 |
| Age year, mean (SD) | 46.28 (11.53) | 44.76 (11.60) | 0.490 |
| BMI, mean (SD) | 42.60 (4.17) | 42.86 (3.78) | 0.738 |
| Weight kg, mean (SD) | 121.44 (16.88) | 126.50 (18.09) | 0.132 |
| Hypertension, n (%) | 36 (72.0) | 39 (62.9) | 0.309 |
| Type 2 diabetes mellitus, n (%) | 6 (12.0) | 12 (19.35) | 0.292 |
| Outcome | LGGCP (n = 48 at 1 Year, n = 45 at 3 Year) | LRYGB (n = 60 at 1 Year, n = 56 at 3 Year) | p-Value Baseline vs. | p-Value LGGCP vs. LRYGB | |
|---|---|---|---|---|---|
| LGGCP | LRYGB | ||||
| Mean weight, kg (SD) | |||||
| Baseline | - | - | 0.132 | ||
| 1 year | 92.08 (16.12) | 83.47 (13.74) | <0.001 | <0.001 | 0.003 |
| 2 year | 93.39 (15.65) | 82.87 (13.93) | <0.001 | <0.001 | <0.001 |
| 3 year | 101 (18.82) | 87.31 (15.15) | <0.001 | <0.001 | <0.001 |
| Mean BMI, kg/m2 (SD) | |||||
| Baseline | 42.60 (4.17) | 42.86 (3.78) | 0.738 | ||
| 1 year | 32.43 (5.04) | 28.36 (3.60) | <0.001 | <0.001 | <0.001 |
| 2 year | 32.93 (4.92) | 28.12 (3.42) | <0.001 | <0.001 | <0.001 |
| 3 year | 35.47 (5.71) | 29.70 (3.83) | <0.001 | <0.001 | <0.001 |
| %TWL (SD) | |||||
| 1 year | 23.61 (9.73) | 33.58 (7.62) | <0.001 | ||
| 2 year | 19.51 (9.23) | 34.05 (8.05) | <0.001 | ||
| 3 year | 16.51 (10.64) | 30.43 (8.80) | <0.001 | ||
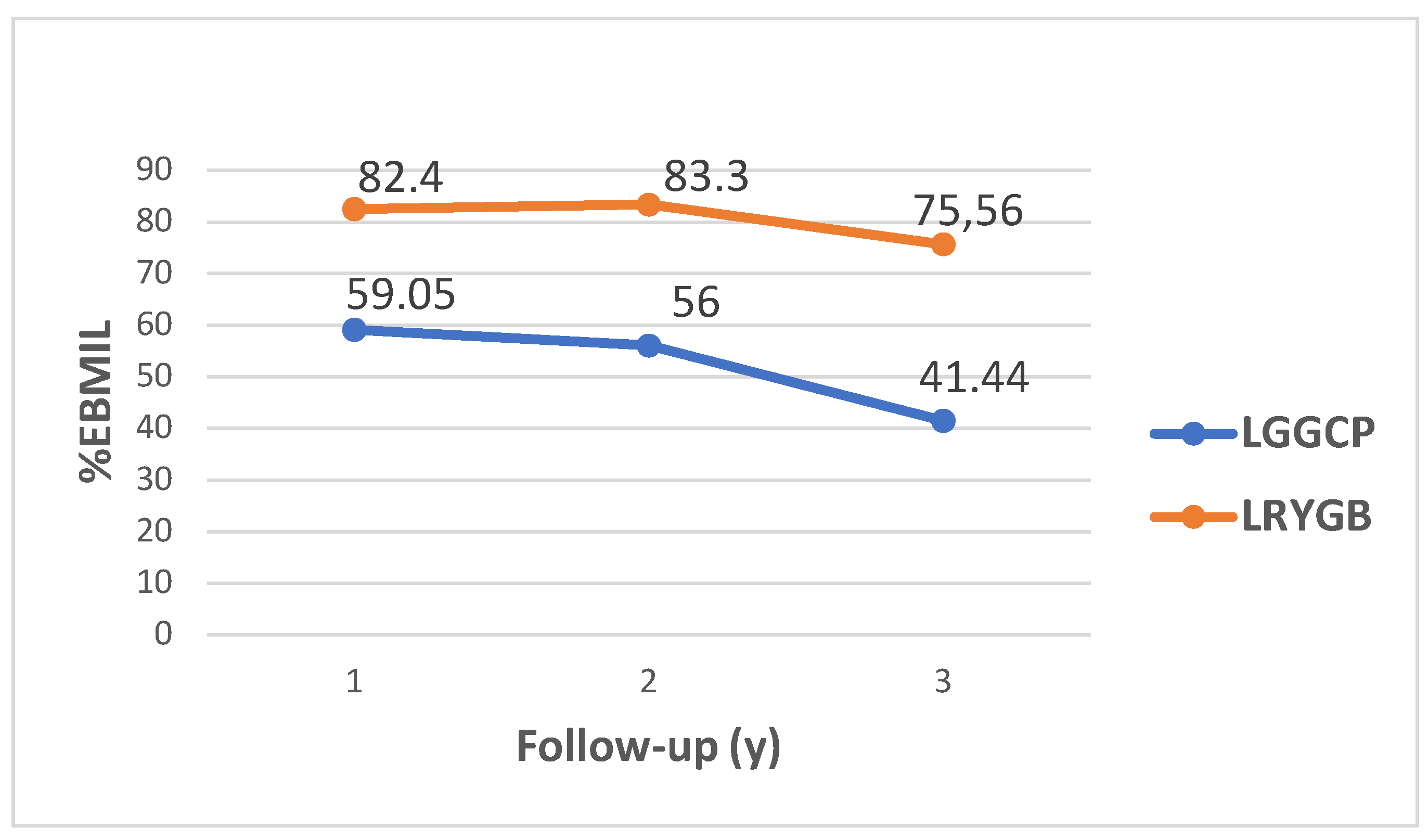
| %EBMIL (SD) | |||||
| 1 year | 59.05 (25.34) | 82.40 (19.03) | <0.001 | ||
| 2 year | 56.00 (24.34) | 83.30 (19.20) | <0.001 | ||
| 3 year | 41.44 (26.74) | 75.56 (19.14) | <0.001 | ||
| LGGCP n = 32 | LRYGB n = 36 | p-Value | |
|---|---|---|---|
| n (%) | n (%) | ||
| Remission * | 19 (59.4) | 25 (69.4) | 0.247 |
| Improvement ** | 9 (28.1) | 11 (30.6) | |
| No change | 3 (9.4) | - | |
| Worse | 1 (3.1) | - |
| LGGCP n = 5 | LRYGB n = 11 | p-Value | |||
|---|---|---|---|---|---|
| T2DM Treatment before Surgery | OAD Medications, n (%) | Insulin or Insulin with OAD Medications, n (%) | OAD Medications, n (%) | Insulin or Insulin with OAD Medications, n (%) | |
| Complete remission * | 3 (60) | - | 7 (63.6) | 2 (18.2) | 1.000 |
| Improvement | - | 1 (20) | - | 2 (18.2) | |
| No change | 1 (20) | - | - | - | |
| Before Surgery | 1 Year after Surgery | 3 Year after Surgery | ||||
|---|---|---|---|---|---|---|
| Typical GERD Symptoms | No GERD Symptoms | Persistence of GERD Symptoms | New Onset of GERD Symptoms | Persistence of GERD Symptoms | New Onset of GERD Symptoms | |
| LGGCP | 30 (60%) | 20 (40%) | 15 (50%) | 4 (20%) | 12 (40%) | 6 (30%) |
| LRYGB | 33 (55%) | 27 (45%) | 5 (15%) | 1 (3.7%) | 3 (9%) | 2 (7.4%) |
| p-value | 0.566 | <0.001 | <0.001 | |||
| LGGCP n = 45 | LRYGB n = 56 | p-Value Baseline vs. | p-Value * | ||
|---|---|---|---|---|---|
| Abdominal Pain | Mean; Median (25th–75th Percentile) | Mean; Median (25th–75th Percentile) | LGGCP | LRYGB | |
| Before | 1.79; 1.67 (1.0–2.0) | 1.80; 1.67 (1.0–2.0) | 0.981 | ||
| 1 year after | 1.44; 1.0 (1.0–1.66) | 1.36; 1.0 (1.0–1.83) | 0.003 | <0.001 | 0.824 |
| 3 year after | 1.01; 1.0 (1.0–1.0) | 1.20; 1.0 (1.0–1.33) | <0.001 | <0.001 | <0.001 |
| Reflux | |||||
| Before | 2.03; 1.5 (1.0–2.5) | 1.81; 1.5 (1.0–2.5) | 0.557 | ||
| 1 year after | 1.82; 1.0 (1.0–2.5) | 1.13; 1.0 (1.0–1.0) | 0.246 | <0.001 | <0.001 |
| 3 year after | 1.79; 1.25 (1.0–2.5) | 1.18; 1.0 (1.0–1.0) | 0.432 | <0.001 | <0.001 |
| Indigestion | |||||
| Before | 2.34; 2.25 (1.75–3.0) | 2.34; 2.25 (1.75–3.0) | 0.104 | ||
| 1 year after | 1.68; 1.75 (1.0–2.0) | 1.68; 1.75 (1.0–2.0) | <0.001 | 0.950 | 0.098 |
| 3 year after | 1.39; 1.5 (1.0–1.75) | 1.39; 1.5 (1.0–1.75) | <0.001 | <0.001 | 0.461 |
| Diarrhoea | |||||
| Before | 1.67; 1.0 (1.0–1.92) | 1.67; 1.33 (1.0–2.0) | 0.555 | ||
| 1 year after | 1.40; 1.0 (1.0–1.66) | 1.62; 1.33 (1.0–2.0) | 0.286 | 0.914 | 0.076 |
| 3 year after | 1.16; 1.0 (1.0–1.0) | 1.20; 1.0 (1.0–1.0) | 0.015 | 0.001 | 0.479 |
| Constipation | |||||
| Before | 1.89; 1.33 (1.0–2.33) | 1.97; 1.67 (1.0–2.33) | 0.601 | ||
| 1 year after | 1.68; 1.33 (1.0–2.0) | 1.37; 1.0 (1.0–1.66) | 0.367 | <0.001 | 0.057 |
| 3 year after | 1.26; 1.0 (1.0–1.33) | 1.21; 1.0 (1.0–1.33) | 0.005 | <0.001 | 0.313 |
| Outcome | EQ-5D-3L Index, Mean; Median (25th–75th Percentile) | p-value Baseline vs. | p-Value | ||
|---|---|---|---|---|---|
| LGGCP | LRYGB | LGGCP | LRYGB | ||
| Before | 0.636; 0.639 (0.500–0.761) | 0.707; 0.715 (0.496–1.000) | 0.091 | ||
| After 1 year | 0.859; 1.000 (0.757–1.000) | 0.898; 1.000 (0.783–1.000) | <0.001 | <0.001 | 0.247 |
| After 3 year | 0.762; 0.779 (0.690–0.794) | 0.898; 1.000 (0.783–1.000) | 0.003 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gudaityte, R.; Kavaliauskaite, A.; Maleckas, A. Mid-Term Outcomes of Laparoscopic Gastric Greater Curvature Plication versus Roux-en-Y Gastric Bypass: Weight Loss, Gastrointestinal Symptoms, and Health-Related Quality of Life. Medicina 2022, 58, 64. https://doi.org/10.3390/medicina58010064
Gudaityte R, Kavaliauskaite A, Maleckas A. Mid-Term Outcomes of Laparoscopic Gastric Greater Curvature Plication versus Roux-en-Y Gastric Bypass: Weight Loss, Gastrointestinal Symptoms, and Health-Related Quality of Life. Medicina. 2022; 58(1):64. https://doi.org/10.3390/medicina58010064
Chicago/Turabian StyleGudaityte, Rita, Agne Kavaliauskaite, and Almantas Maleckas. 2022. "Mid-Term Outcomes of Laparoscopic Gastric Greater Curvature Plication versus Roux-en-Y Gastric Bypass: Weight Loss, Gastrointestinal Symptoms, and Health-Related Quality of Life" Medicina 58, no. 1: 64. https://doi.org/10.3390/medicina58010064
APA StyleGudaityte, R., Kavaliauskaite, A., & Maleckas, A. (2022). Mid-Term Outcomes of Laparoscopic Gastric Greater Curvature Plication versus Roux-en-Y Gastric Bypass: Weight Loss, Gastrointestinal Symptoms, and Health-Related Quality of Life. Medicina, 58(1), 64. https://doi.org/10.3390/medicina58010064