
Long-Term Outcomes of Chronic Cough Reduction after Laparoscopic Nissen Fundoplication—A Single-Center Study

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
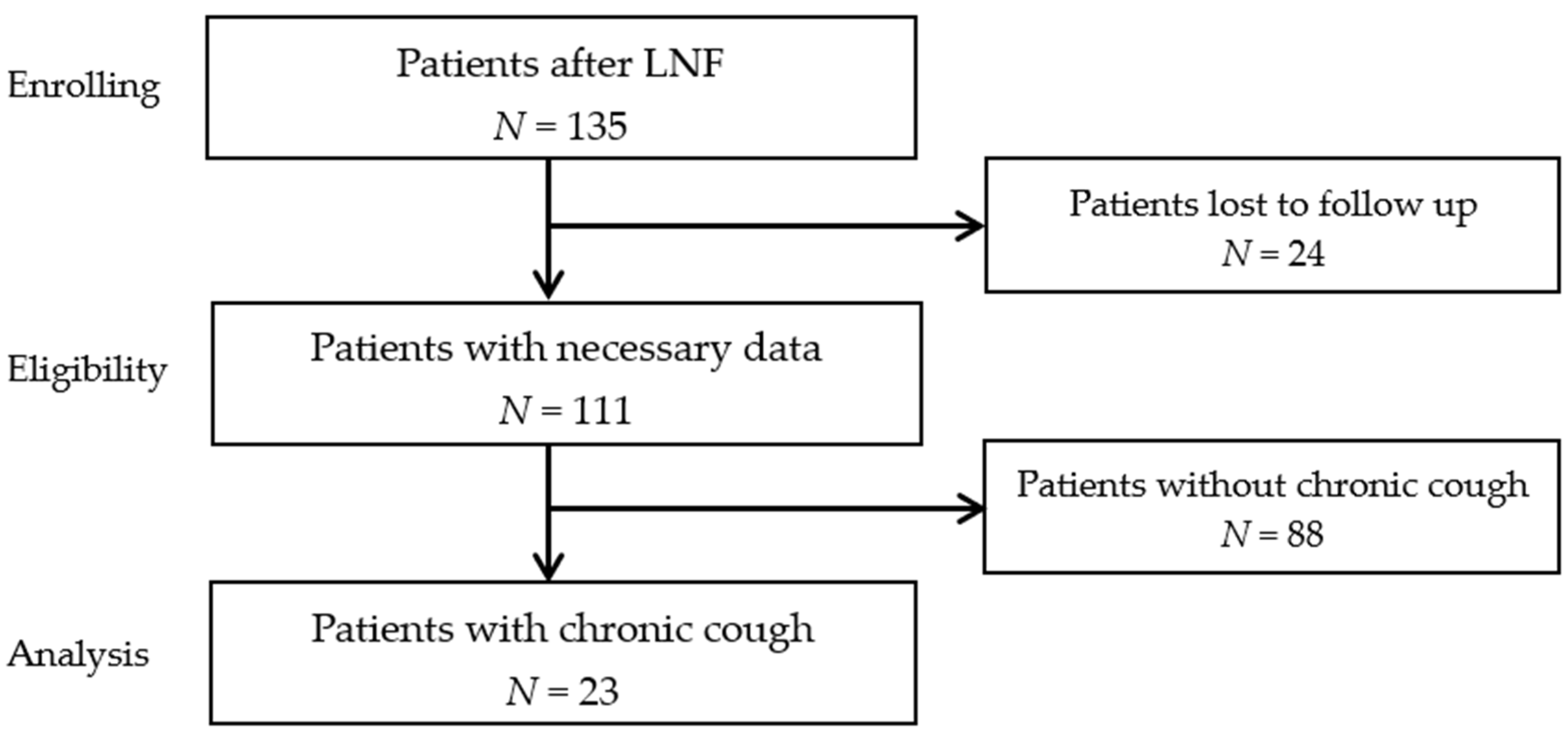
2.1. Patient Selection
2.2. Surgical Technique
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frazzoni, M.; Piccoli, M.; Conigliaro, P.; Frazzoni, L.; Melotti, G. Laparoscopic fundoplication for gastroesophageal reflux disease. World J. Gastroenterol. 2014, 20, 14272–14279. [Google Scholar] [CrossRef] [PubMed]
- Tack, J.; Pandolfino, J.E. Pathophysiology of Gastroesophageal Reflux Disease. Gastroenterology 2018, 154, 277–288. [Google Scholar] [CrossRef]
- Badillo, R.; Francis, D. Diagnosis and treatment of gastroesophageal reflux disease. World J. Gastrointest. Pharmacol. Ther. 2014, 5, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, D.S.; Fass, R. Current Trends in the Management of Gastroesophageal Reflux Disease. Gut Liver 2018, 12, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Tsoukali, E.; Sifrim, D. Investigation of extraesophageal gastroesophageal reflux disease. Ann. Gastroenterol. 2013, 26, 290–295. [Google Scholar] [PubMed]
- Hulme, K.; Deary, V.; Dogan, S.; Parker, S.M. Psychological profile of individuals presenting with chronic cough. ERJ Open Res. 2017, 3, 00099–02016. [Google Scholar] [CrossRef]
- Morice, A.; Dicpinigaitis, P.; McGarvey, L.; Birring, S.S. Chronic cough: New insights and future prospects. Eur. Respir. Rev. 2021, 30, 210127. [Google Scholar] [CrossRef]
- Satia, I.; Badri, H.; Al-Sheklly, B.; Smith, J.A.; Woodcock, A.A. Towards understanding and managing chronic cough. Clin. Med. 2016, 16, 92–97. [Google Scholar] [CrossRef]
- Tustumi, F.; Bernardo, W.M.; da Rocha, J.R.; Szachnowicz, S.; da Costa Seguro, F.C.; Bianchi, E.T.; Takeda, F.R.; de Miranda Neto, A.A.; Sallum, R.A.; Cecconello, I. Anti-reflux surgery for controlling respiratory symptoms of gastro-esophageal reflux disease: A systematic review and meta-analysis. Asian J. Surg. 2021, 44, 2–10. [Google Scholar] [CrossRef]
- Perotin, J.M.; Launois, C.; Dewolf, M.; Dumazet, A.; Dury, S.; Lebargy, F.; Dormoy, V.; Deslee, G. Managing patients with chronic cough: Challenges and solutions. Ther. Clin. Risk Manag. 2018, 14, 1041–1051. [Google Scholar] [CrossRef]
- Stefanidis, D.; Hope, W.W.; Kohn, G.P.; Reardon, P.R. Guidelines for surgical treatment of gastroesophageal reflux disease. Surg. Endosc. 2010, 24, 2647–2669. [Google Scholar] [CrossRef]
- Jo, S.Y.; Kim, N.; Lim, J.H.; Shin, C.M.; Park, Y.S.; Lee, D.H.; Jung, H.C. Comparison of gastroesophageal reflux disease symptoms and proton pump inhibitor response using gastroesophageal reflux disease impact scale questionnaire. J. Neurogastroenterol. Motil. 2013, 19, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Coyne, K.; Wiklund, I. The gastro-oesophageal reflux disease impact scale: A patient management tool for primary care. Aliment. Pharm. Ther. 2007, 25, 1451–1459. [Google Scholar] [CrossRef] [PubMed]
- Park, A.; Weltz, A.S.; Sanford, Z.; Addo, A.; Zahiri, H.R. Laparoscopic antireflux surgery (LARS) is highly effective in the treatment of select patients with chronic cough. Surgery 2019, 166, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Adaba, F.; Ang, C.W.; Perry, A.; Wadley, M.S.; Robertson, C.S. Outcome of gastrooesophageal reflux-related respiratory manifestations after laparoscopic fundoplication. Int. J. Surg. 2014, 12, 241–244. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lugaresi, M.; Aramini, B.; Daddi, N.; Baldi, F.; Mattioli, S. Effectiveness of antireflux surgery for the cure of chronic cough associated with gastroesophageal reflux disease. World J. Surg. 2015, 39, 208–215. [Google Scholar] [CrossRef]
- Iqbal, M.; Batch, A.J.; Moorthy, K.; Cooper, B.T.; Spychal, R.T. Outcome of surgical fundoplication for extra-oesophageal symptoms of reflux. Surg. Endosc. 2009, 23, 557–561. [Google Scholar] [CrossRef]
- Brouwer, R.; Kiroff, G.K. Improvement of respiratory symptoms following laparoscopic Nissen fundoplication. ANZ J. Surg. 2003, 73, 189–193. [Google Scholar] [CrossRef]
- Kaufman, J.A.; Houghland, J.E.; Quiroga, E.; Cahill, M.; Pellegrini, C.A.; Oelschlager, B.K. Long-term outcomes of laparoscopic antireflux surgery for gastroesophageal reflux disease (GERD)-related airway disorder. Surg. Endosc. 2006, 20, 1824–1830. [Google Scholar] [CrossRef]
- Holcomb, C.N.; Switzer, N.J.; Jlilvand, A.; Belle, P.; McNally, M.; Perry, K. Impact of psychiatric disorders on patient satisfaction after Nissen Fundoplication. Surg. Endosc. 2020, 34, 1829–1834. [Google Scholar] [CrossRef]
- Sontag, S.J.; O’Connell, S.; Khandelwal, S.; Greenlee, H.; Schnell, T.; Nemchausky, B.; Chejfec, G.; Miller, T.; Seidel, J.; Sonnenberg, A. Asthmatics with gastroesophageal reflux: Long term results of a randomized trial of medical and surgical antireflux therapies. Am. J. Gastroenterol. 2003, 98, 987–999. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, R.; Petersen, H.; Olberg, P.; Johnsen, G.; Fjøsne, U.; Kleveland, P.M. Airway symptoms and sleeping difficulties in operated and non-operated patients with gastroesophageal reflux disease. Scand. J. Gastroenterol. 2012, 47, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Kiljander, T.; Rantanen, T.; Kellokumpu, I.; Kööbi, T.; Lammi, L.; Nieminen, M.; Poussa, T.; Ranta, A.; Saarelainen, S.; Salminen, P. Comparison of the effects of esomeprazole and fundoplication on airway responsiveness in patients with gastro-oesophageal reflux disease. Clin. Res. J. 2013, 7, 281–287. [Google Scholar] [CrossRef]
- Zhang, C.; Hu, Z.W.; Yan, C.; Wu, Q.; Wu, J.M.; Du, X.; Liu, D.G.; Luo, T.; Li, F.; Wang, Z.G. Nissen fundoplication vs proton pump inhibitors for laryngopharyngeal reflux based on pH-monitoring and symptom-scale. World J. Gastroenterol. 2017, 23, 3546–3555. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No | Chronic Use of PPIs | Undergo the Surgery Again | Recommendation of Surgery | Recurrence of Symptoms | Time of Recurrence [Months] |
|---|---|---|---|---|---|
| 1 | No | Yes | Yes | No | |
| 2 | No | Do not know | Do not know | Yes | 12 |
| 3 | Yes | Yes | Yes | No | |
| 4 | No | Yes | Yes | No | |
| 5 | No | Yes | Yes | No | |
| 6 | Yes | Do not know | No | Yes | 12 |
| 7 | No | Yes | Yes | No | |
| 8 | No | Yes | Yes | No | |
| 9 | No | Yes | Yes | No | |
| 10 | No | No | Do not know | Yes | 18 |
| 11 | No | Yes | Yes | No | |
| 12 | No | Yes | Yes | No | |
| 13 | No | Do not know | Yes | No | |
| 14 | Yes | Yes | Yes | No | |
| 15 | Yes | No | No | Yes | 6 |
| 16 | No | Yes | Yes | No | |
| 17 | No | Yes | Yes | No | |
| 18 | No | Yes | Yes | No | |
| 19 | No | Yes | Yes | No | |
| 20 | No | No | No | Yes | 6 |
| 21 | No | Yes | Yes | No | |
| 22 | No | Yes | Yes | No | |
| 23 | No | Yes | Yes | No |
| Questions | Before LNF | After LNF | p | ||
|---|---|---|---|---|---|
| Median | 25–75% IQR | Median | 25–75% IQR | ||
| How often have you had pain in your chest or behind the breastbone? | 2 | 1–3 | 4 | 3–4 | <0.001 |
| How often have you had a burning sensation in your chest or behind the breastbone? | 2 | 1–3 | 4 | 3–4 | <0.001 |
| How often have you had regurgitation or an acid taste in your mouth? | 2 | 1–3 | 4 | 3–4 | <0.001 |
| How often have you had pain or burning in your upper stomach? | 3 | 1–4 | 4 | 3–4 | 0.03 |
| How often have you had a sore throat or hoarseness that is related to your heartburn or acid reflux? | 2 | 1–3 | 4 | 3–4 | <0.001 |
| How often have you had difficulty getting a good night’s sleep because of your symptoms? | 2 | 1–4 | 4 | 3–4 | <0.001 |
| How often have your symptoms prevented you from eating or drinking any of the foods you like? | 2 | 1–4 | 4 | 3–4 | 0.002 |
| How frequently have your symptoms kept you from being fully productive in your job or daily activities? | 2 | 1–3 | 4 | 4–4 | <0.001 |
| How often do you take additional medication other than what the physician old you to take (such as Maalox, Alusal, Manti)? | 3 | 2–4 | 4 | 4–4 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dowgiałło-Gornowicz, N.; Masiewicz, A.; Kacperczyk, J.; Lech, P.; Saluk, S.; Osowiecka, K.; Michalik, M. Long-Term Outcomes of Chronic Cough Reduction after Laparoscopic Nissen Fundoplication—A Single-Center Study. Medicina 2022, 58, 47. https://doi.org/10.3390/medicina58010047
Dowgiałło-Gornowicz N, Masiewicz A, Kacperczyk J, Lech P, Saluk S, Osowiecka K, Michalik M. Long-Term Outcomes of Chronic Cough Reduction after Laparoscopic Nissen Fundoplication—A Single-Center Study. Medicina. 2022; 58(1):47. https://doi.org/10.3390/medicina58010047
Chicago/Turabian StyleDowgiałło-Gornowicz, Natalia, Anna Masiewicz, Justyna Kacperczyk, Paweł Lech, Sławomir Saluk, Karolina Osowiecka, and Maciej Michalik. 2022. "Long-Term Outcomes of Chronic Cough Reduction after Laparoscopic Nissen Fundoplication—A Single-Center Study" Medicina 58, no. 1: 47. https://doi.org/10.3390/medicina58010047
APA StyleDowgiałło-Gornowicz, N., Masiewicz, A., Kacperczyk, J., Lech, P., Saluk, S., Osowiecka, K., & Michalik, M. (2022). Long-Term Outcomes of Chronic Cough Reduction after Laparoscopic Nissen Fundoplication—A Single-Center Study. Medicina, 58(1), 47. https://doi.org/10.3390/medicina58010047