
Association between Advanced Lung Inflammation Index and 30-Day Mortality in Patients with Acute Respiratory Distress Syndrome

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
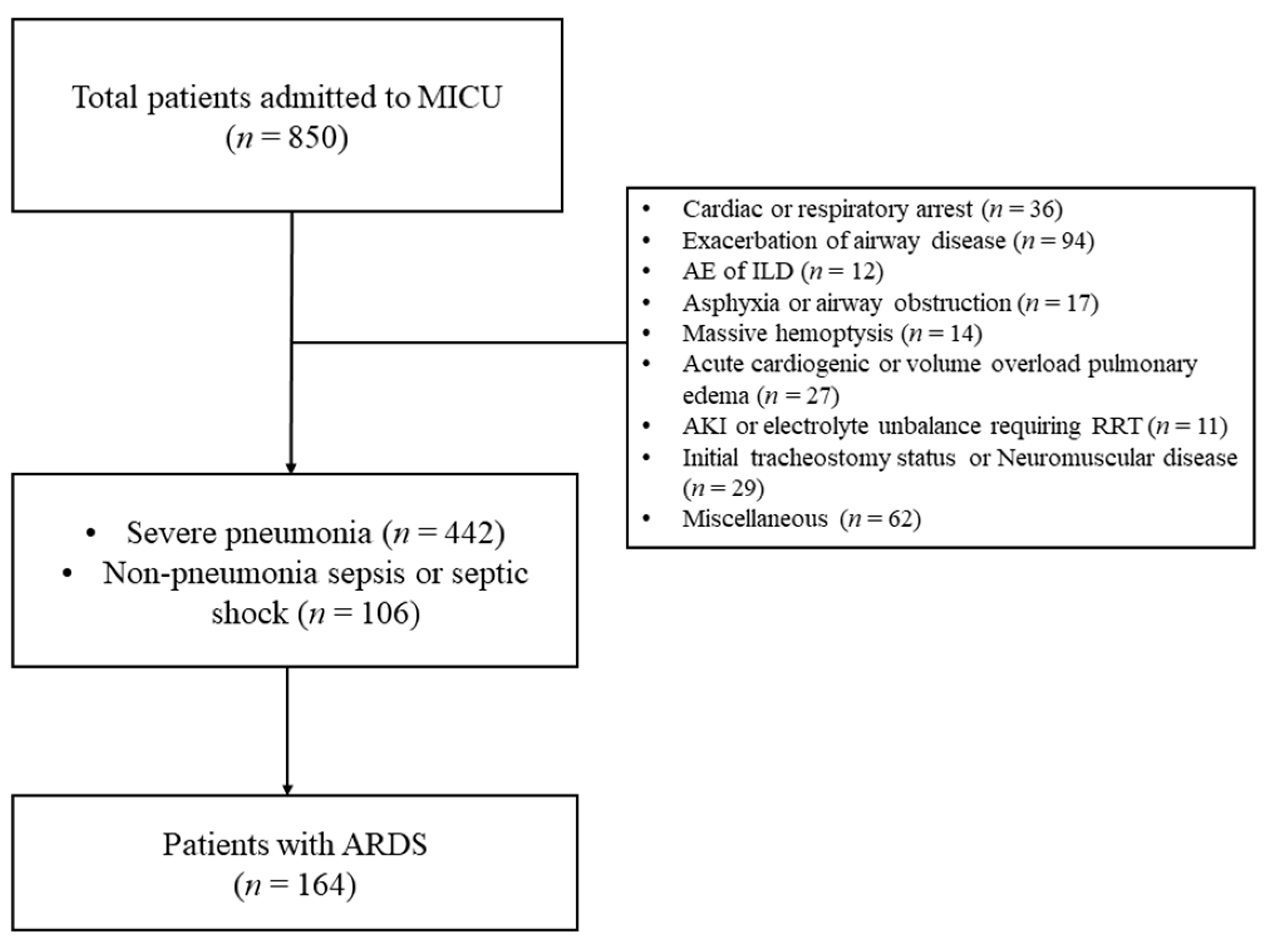
2.1. Patients
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ashbaugh, D.; Bigelow, D.B.; Petty, T.; Levine, B. Acute respiratory distress in adults. Lancet 1967, 2, 319–323. [Google Scholar] [CrossRef]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, R.O.; Weaver, L.K.; Collingridge, D.; Parkinson, R.B.; Chan, K.J.; Orme, J.F., Jr. Two-year cognitive, emotional, and quality-of-life outcomes in acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2005, 171, 340–347. [Google Scholar] [CrossRef]
- Herridge, M.S. Recovery and long-term outcome in acute respiratory distress syndrome. Crit. Care Clin. 2011, 27, 685–704. [Google Scholar] [CrossRef] [PubMed]
- Herridge, M.S.; Tansey, C.M.; Matte, A.; Tomlinson, G.; Diaz-Granados, N.; Cooper, A.; Guest, C.B.; Mazer, C.D.; Mehta, S.; Stewart, T.E.; et al. Functional disability 5 years after acute respiratory distress syndrome. N. Engl. J. Med. 2011, 364, 1293–1304. [Google Scholar] [CrossRef] [Green Version]
- Herridge, M.S.; Moss, M.; Hough, C.L.; Hopkins, R.O.; Rice, T.; Bienvenu, J.; Azoulay, E. Recovery and outcomes after the acute respiratory distress syndrome (ARDS) in patients and their family caregivers. Intensive Care Med. 2016, 42, 725–738. [Google Scholar] [CrossRef]
- Reiss, L.K.; Schuppert, A.; Uhlig, S. Inflammatory processes during acute respiratory distress syndrome: A complex system. Curr. Opin. Crit. Care 2018, 24, 1–9. [Google Scholar] [CrossRef]
- Cressoni, M.; Chiumello, D.; Chiurazzi, C.; Brioni, M.; Algieri, I.; Gotti, M.; Nikolla, K.; Massari, D.; Cammaroto, A.; Colombo, A.; et al. Lung inhomogeneities, inflation and [18F]2-fluoro-2-deoxy-D-glucose uptake rate in acute respiratory distress syndrome. Eur. Respir. J. 2016, 47, 233–242. [Google Scholar] [CrossRef] [Green Version]
- Jafri, S.H.; Shi, R.; Mills, G. Advance lung cancer inflammation index (ALI) at diagnosis is a prognostic marker in patients with metastatic non-small cell lung cancer (NSCLC): A retrospective review. BMC Cancer 2013, 13, 158. [Google Scholar] [CrossRef] [Green Version]
- Ozyurek, B.A.; Ozdemirel, T.S.; Ozden, S.B.; Erdoğan, Y.; Ozmen, O.; Kaplan, B.; Kaplan, T. Does advanced lung inflammation index (ALI) have prognostic significance in metastatic non-small cell lung cancer? Clin. Respir. J. 2018, 12, 2013–2019. [Google Scholar] [CrossRef]
- Wang, Y.; Ju, M.; Chen, C.; Yang, D.; Hou, D.; Tang, X.; Zhu, X.; Zhang, D.; Wang, L.; Ji, S.; et al. Neutrophil-to-lymphocyte ratio as a prognostic marker in acute respiratory distress syndrome patients: A retrospective study. J. Thorac. Dis. 2018, 10, 273–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiumello, D.; Colombo, A.; Algieri, I.; Mietto, C.; Carlesso, E.; Crimella, F.; Cressoni, M.; Quintel, M.; Gattinoni, L. Effect of body mass index in acute respiratory distress syndrome. Br. J. Anaesth. 2016, 116, 113–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, Y.N.; Luo, J.; Yu, H.; Wang, Y.W.; Hu, Y.H.; Liu, D.; Liang, Z.A. Can body mass index predict clinical outcomes for patients with acute lung injury/acute respiratory distress syndrome? A meta-analysis. Crit. Care 2017, 21, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeboer, S.H.; Oudemans-van Straaten, H.M.; Groeneveld, A.B. Albumin rather than C-reactive protein may be valuable in predicting and monitoring the severity and course of acute respiratory distress syndrome in critically ill patients with or at risk for the syndrome after new onset fever. BMC Pulm. Med. 2015, 15, 22. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.; Caldwell, E.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Willerson, J.T.; Ridker, P.M. Inflammation as a cardiovascular risk factor. Circulation 2004, 109, Ii2–Ii10. [Google Scholar] [CrossRef] [Green Version]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef]
- Ware, L.B.; Matthay, M.A. The acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1334–1349. [Google Scholar] [CrossRef]
- Williams, A.E.; Chambers, R.C. The mercurial nature of neutrophils: Still an enigma in ARDS? Am. J. Physiol. Lung. Cell Mol. Physiol. 2014, 306, L217–L230. [Google Scholar] [CrossRef] [Green Version]
- Kangelaris, K.N.; Prakash, A.; Liu, K.D.; Aouizerat, B.; Woodruff, P.G.; Erle, D.J.; Calfee, C.S. Increased expression of neutrophil-related genes in patients with early sepsis-induced ARDS. Am. J. Physiol. Lung Cell Mol. Physiol. 2015, 308, L1102–L1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokgoz, S.; Kayrak, M.; Akpinar, Z.; Seyithanoglu, A.; Guney, F.; Yuruten, B. Neutrophil lymphocyte ratio as a predictor of stroke. J. Stroke 2013, 22, 1169–1174. [Google Scholar] [CrossRef]
- Balta, S.; Demirkol, S.; Aparci, M.; Celik, T.; Ozturk, C. The neutrophil lymphocyte ratio in coronary heart disease. Int. J. Cardiol. 2014, 176, 267. [Google Scholar] [CrossRef]
- Kang, M.H.; Go, S.I.; Song, H.N.; Lee, A.; Kim, S.-H.; Kang, J.-H.; Jeong, B.-K.; Kang, K.M.; Ling, H.; Lee, G.-W. The prognostic impact of the neutrophil-to-lymphocyte ratio in patients with small-cell lung cancer. Br. J. Cancer 2014, 111, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Go, S.I.; Lee, A.; Lee, U.S.; Choi, H.J.; Kang, M.H.; Kang, J.-H.; Jeon, K.N.; Park, M.J.; Kim, S.-H.; Lee, G.-W. Clinical significance of the neutrophil-lymphocyte ratio in venous thromboembolism patients with lung cancer. Lung Cancer 2014, 84, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Garrow, J.S.; Webster, J. Quetelet’s index (W/H2) as a measure of fatness. Int. J. Obes. 1985, 9, 147–153. [Google Scholar]
- Skurk, T.; Alberti-Huber, C.; Herder, C.; Hauner, H. Relationship between adipocyte size and adipokine expression and secretion. J. Clin. Endocrinol. Metab. 2007, 92, 1023–1033. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, A.W., Jr. Obesity-induced inflammation: A metabolic dialogue in the language of inflammation. J. Intern. Med. 2007, 262, 408–414. [Google Scholar] [CrossRef]
- Pickkers, P.; de Keizer, N.; Dusseljee, J.; Weerheijm, D.; van der Hoeven, J.G.; Peek, N. Body mass index is associated with hospital mortality in critically ill patients: An observational cohort study. Crit. Care Med. 2013, 41, 1878–1883. [Google Scholar] [CrossRef]
- Sakr, Y.; Alhussami, I.; Nanchal, R.; Wunderink, R.G.; Pellis, T.; Wittebole, X.; Vincent, J.L. Being Overweight Is Associated With Greater Survival in ICU Patients: Results From the Intensive Care Over Nations Audit. Crit. Care Med. 2015, 43, 2623–2632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, K.; Zhou, J.; Liu, X.; Hassan, E.; Badawi, O. The Obesity Paradox Is Not Observed in Critically Ill Patients on Early Enteral Nutrition. Crit. Care Med. 2017, 45, 828–834. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 341, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Artero, A.; Zaragoza, R.; Camarena, J.J.; Sancho, S.; Gonzalez, R.; Nogueira, J.M. Prognostic factors of mortality in patients with community-acquired bloodstream infection with severe sepsis and septic shock. J. Crit. Care 2010, 25, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, J.; Kim, K.; Jo, Y.H.; Rhee, J.; Kim, T.Y.; Hwang, S.S. Albumin and C-reactive protein have prognostic significance in patients with community-acquired pneumonia. J. Crit. Care 2011, 26, 287–294. [Google Scholar] [CrossRef]
- Aman, J.; van der Heijden, M.; van Lingen, A.; Girbes, A.R.; van Nieuw Amerongen, G.P.; van Hinsbergh, V.W.; Groeneveld, A.J. Plasma protein levels are markers of pulmonary vascular permeability and degree of lung injury in critically ill patients with or at risk for acute lung injury/acute respiratory distress syndrome. Crit. Care Med. 2011, 39, 89–97. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | Total | Survivor | Non-Survivors | p-Value |
|---|---|---|---|---|
| N = 164 | N = 64 | N = 100 | ||
| Age, years old | 73 (60–79.8) | 66 (53.8–76.8) | 75 (65.3–80) | 0.001 |
| Gender, male | 120 (73.2) | 48 (75) | 72 (72) | 0.67 |
| Body mass index (kg/m2) | 21.5 (19–24.6) | 22.3 (20.4–25.2) | 20.8 (18.6–24) | 0.019 |
| Diabetes mellitus | 47 (28.7) | 19 (29.7) | 28 (28) | 0.82 |
| Ischemic heart disease | 12 (7.3) | 4 (6.3) | 8 (8) | 0.77 |
| Heart failure | 5 (3) | 2 (3.1) | 3 (3.0) | 1 |
| Chronic kidney disease | 11 (6.7) | 4 (6.3) | 7 (7) | 1 |
| Chronic liver disease | 21 (12.8) | 10 (15.6) | 11 (11) | 0.39 |
| Cerebrovascular disease | 29 (17.7) | 15 (23.4) | 14 (14) | 0.12 |
| Active malignancy | 18 (11) | 7 (10.9) | 11 (11) | 0.99 |
| COPD | 16 (9.8) | 7 (10.9) | 9 (9) | 0.68 |
| APACHE II | 26 (22–26) | 23 (20–26) | 30 (25–34) | <0.001 |
| SOFA | 12 (10–14) | 11 (9–13) | 13 (11–15) | <0.001 |
| ARDS severity | 0.001 | |||
| mild | 16 (9.8) | 12(18.8) | 4 (4) | |
| moderate | 88 (53.7) | 37 (57.8) | 51 (51) | |
| severe | 60 (36.6) | 15 (23.4) | 45 (45) | |
| Septic shock | 118 (72) | 39 (60.9) | 79 (79) | 0.012 |
| Cardiac arrest | 14 (8.5) | 6 (9.4) | 8 (8) | 0.76 |
| Acute kidney injury | 106 (64.6) | 31 (48.4) | 75 (75) | 0.001 |
| RRT | 48 (29.3) | 9 (14.1) | 39 (39) | 0.32 |
| Transfusion of blood products * | 37 (22.6) | 10 (15.6) | 27 (27) | 0.089 |
| Steroid | 37 (22.6) | 11 (17.2) | 26 (26) | 0.19 |
| Prone position | 6 (3.7) | 2 (3.1) | 4 (4) | 1 |
| ECMO | 16 (9.8) | 7 (10.9) | 9 (9) | 0.68 |
| Variables | Total | Survivors | Non-Survivors | p-Value |
|---|---|---|---|---|
| N = 164 | N = 64 | N = 100 | ||
| NLR | 11.8 (5.6–20.9) | 9.2 (4.8–17.9) | 14.2 (7.2–21.8) | 0.048 |
| Hb, g/dL | 11.5 (9.6–12.8) | 12.2 (10.4–13.5) | 11 (9.4–12.6) | 0.01 |
| Platelet, ×103/mm3 | 184 (127.2–290.5) | 194.5 (141.5–275.8) | 162 (110.2–291) | 0.35 |
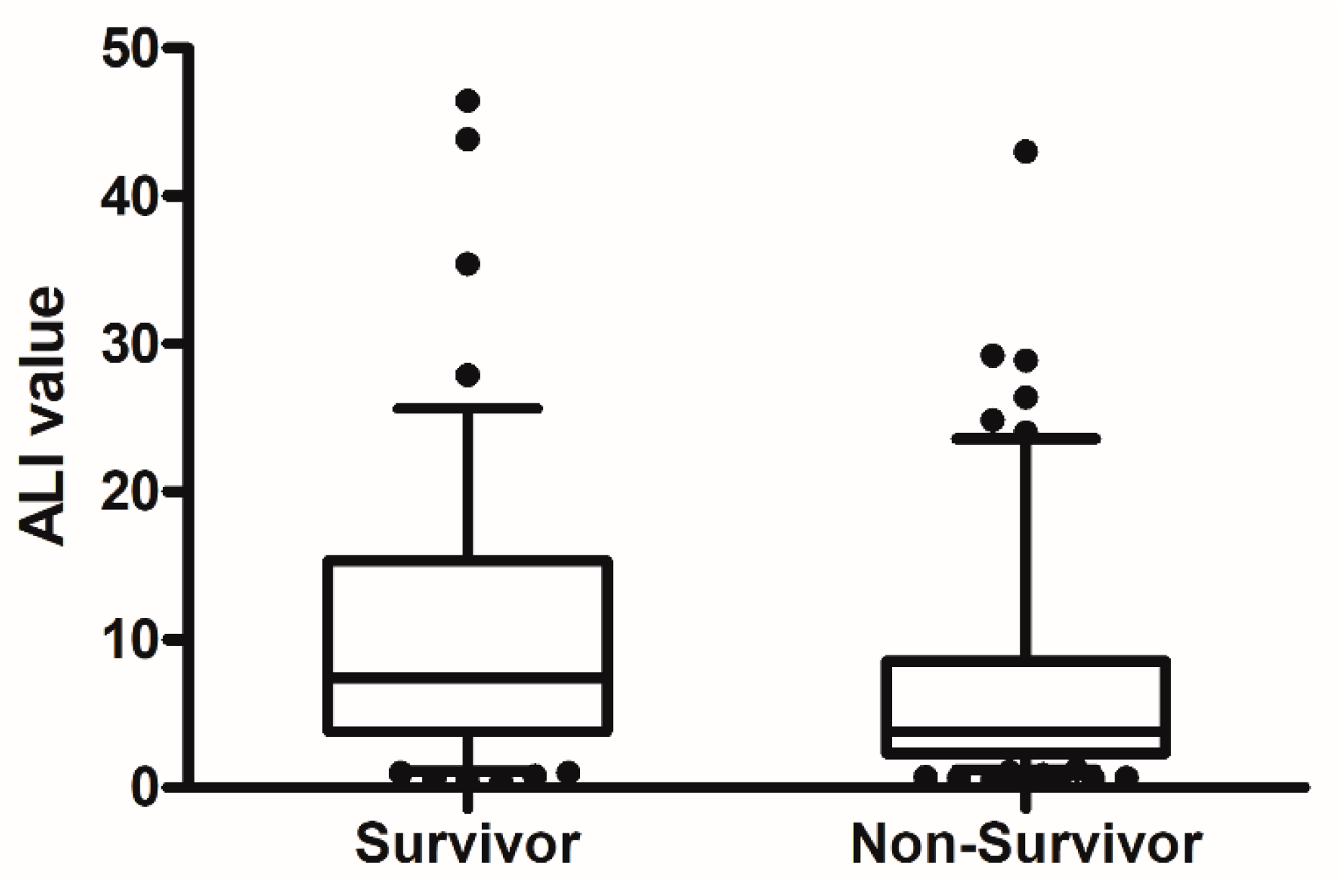
| ALI | 4.51 (2.53–12.32) | 7.39 (3.79–15.36) | 3.81 (2.29–8.56) | 0.005 |
| Albumin, g/dL | 2.6 (2.3–3.1) | 2.8 (2.5–3.3) | 2.6 (2.2–2.9) | 0.001 |
| CRP, mg/dL | 17.9 (9.5–27.1) | 18.6 (11.3–27.6) | 17.7 (8.9–26.4) | 0.44 |
| Lactate, mmol/L | 3.2 (2–5.8) | 2.8 (1.7–5.5) | 3.5 (2.1–6.1) | 0.124 |
| pH | 7.32 (7.22–7.4) | 7.36 (7.29–7.42) | 7.28 (7.19–7.39) | <0.001 |
| PaCO2, mmHg | 38 (32–45) | 35 (30–41.7) | 41 (33.2–46) | 0.002 |
| Bicarbonate, mmol/L | 18 (16–22) | 19.5 (17–21) | 18 (15–22) | 0.228 |
| P/F ratio | 115 (84.1–153.8) | 130 (100–194.8) | 106 (77–142.5) | 0.002 |
| Vt, mL | 6.85 (6.02–7.89) | 7.31 (6.25–8.27) | 6.75 (6.01–7.79) | 0.077 |
| PEEP, cmH2O | 8 (5–10) | 8 (5–10) | 8.5 (6–10) | 0.21 |
| FiO2 | 0.8 (1–0.6) | 0.6 (0.52–0.83) | 0.8 (0.6–1) | 0.002 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Age | 1.034 | 1.010–1.058 | 0.004 | 1.014 | 0.984–1.044 | 0.364 |
| APACHEII | 1.219 | 1.134–1.310 | <0.001 | 1.184 | 1.077–1.303 | 0.001 |
| Shock | 2.411 | 1.203–4.834 | 0.013 | 1.364 | 0.529–3.514 | 0.520 |
| AKI | 3.194 | 1.639–6.224 | 0.001 | 2.001 | 0.748–5.351 | 0.167 |
| Hb, g/dL | 0.825 | 0.713–0.954 | 0.009 | 0.802 | 0.656–0.981 | 0.032 |
| PaCO2, mmHg | 1.055 | 1.018–1.093 | 0.003 | 1.086 | 1.031–1.143 | 0.002 |
| P/F ratio | 0.989 | 0.983–0.995 | 0.001 | 0.997 | 0.988–1.005 | 0.424 |
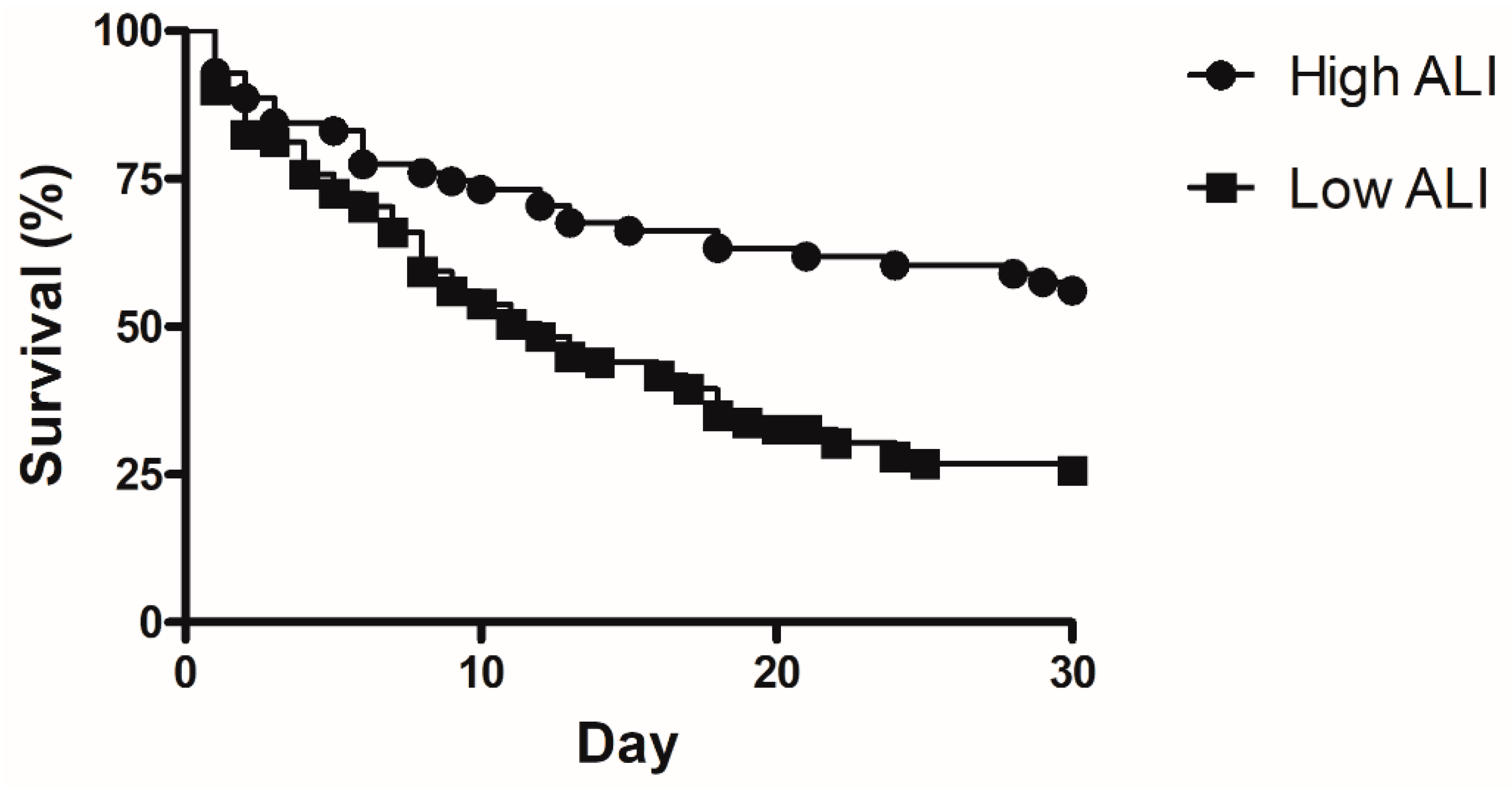
| Low ALI value | 3.542 | 1.835–6.837 | <0.001 | 3.001 | 1.202–7.492 | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heo, M.; Jeong, J.; Heo, I.; Ju, S.; Lee, S.; Jeong, Y.; Lee, J.; Kim, H.; Yoo, J. Association between Advanced Lung Inflammation Index and 30-Day Mortality in Patients with Acute Respiratory Distress Syndrome. Medicina 2021, 57, 800. https://doi.org/10.3390/medicina57080800
Heo M, Jeong J, Heo I, Ju S, Lee S, Jeong Y, Lee J, Kim H, Yoo J. Association between Advanced Lung Inflammation Index and 30-Day Mortality in Patients with Acute Respiratory Distress Syndrome. Medicina. 2021; 57(8):800. https://doi.org/10.3390/medicina57080800
Chicago/Turabian StyleHeo, Manbong, Jonghwan Jeong, Ire Heo, Sunmi Ju, Seungjun Lee, Yiyeong Jeong, Jongdeog Lee, Hocheol Kim, and Jungwan Yoo. 2021. "Association between Advanced Lung Inflammation Index and 30-Day Mortality in Patients with Acute Respiratory Distress Syndrome" Medicina 57, no. 8: 800. https://doi.org/10.3390/medicina57080800
APA StyleHeo, M., Jeong, J., Heo, I., Ju, S., Lee, S., Jeong, Y., Lee, J., Kim, H., & Yoo, J. (2021). Association between Advanced Lung Inflammation Index and 30-Day Mortality in Patients with Acute Respiratory Distress Syndrome. Medicina, 57(8), 800. https://doi.org/10.3390/medicina57080800