
Immunomodulatory Effects of Atractylodes lancea in Healthy Volunteers with Dosage Prediction for Cholangiocarcinoma Therapy: A Modelling Approach


Abstract
1. Introduction
2. Results
2.1. Pharmacokinetics Analysis
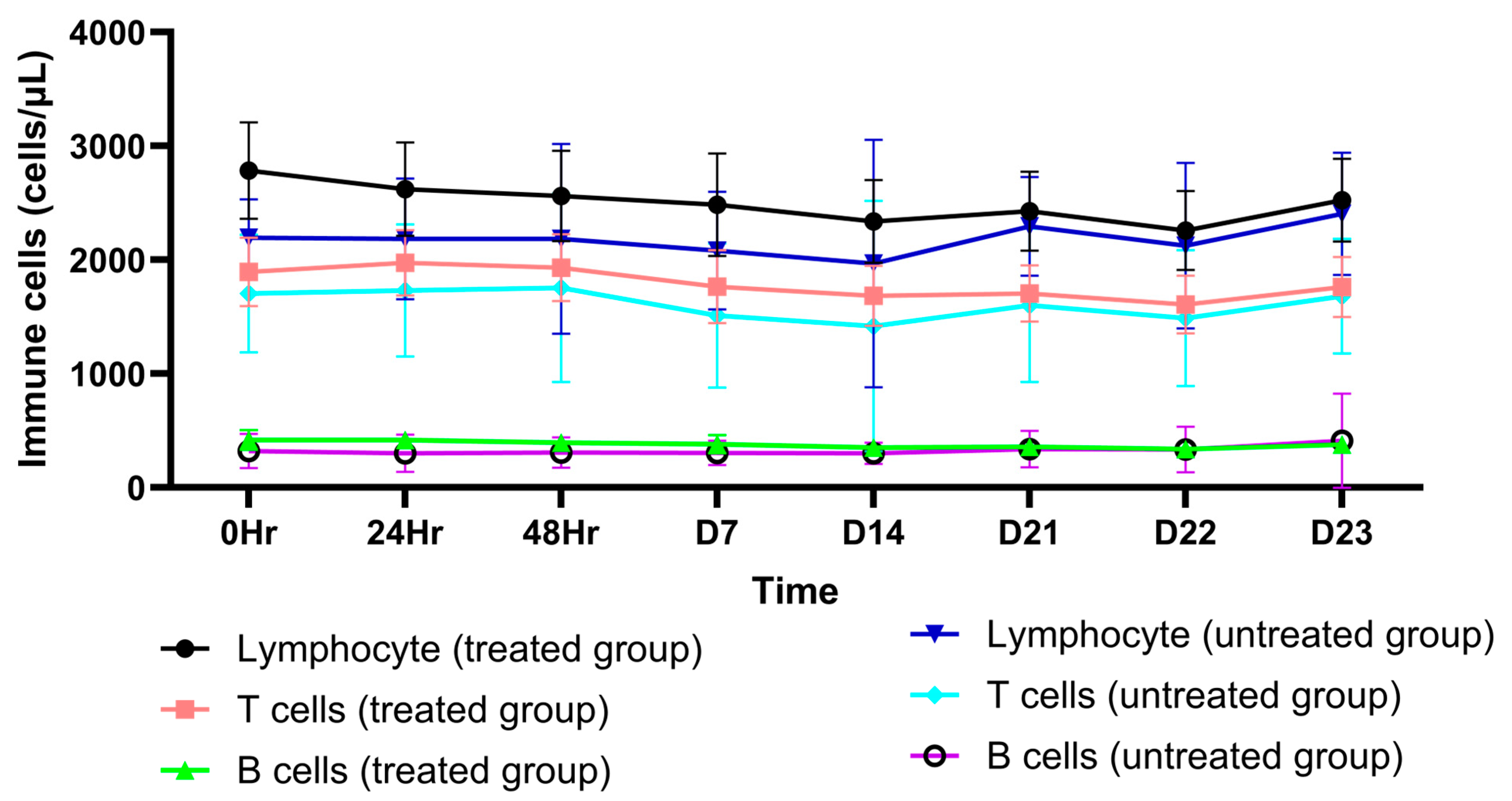
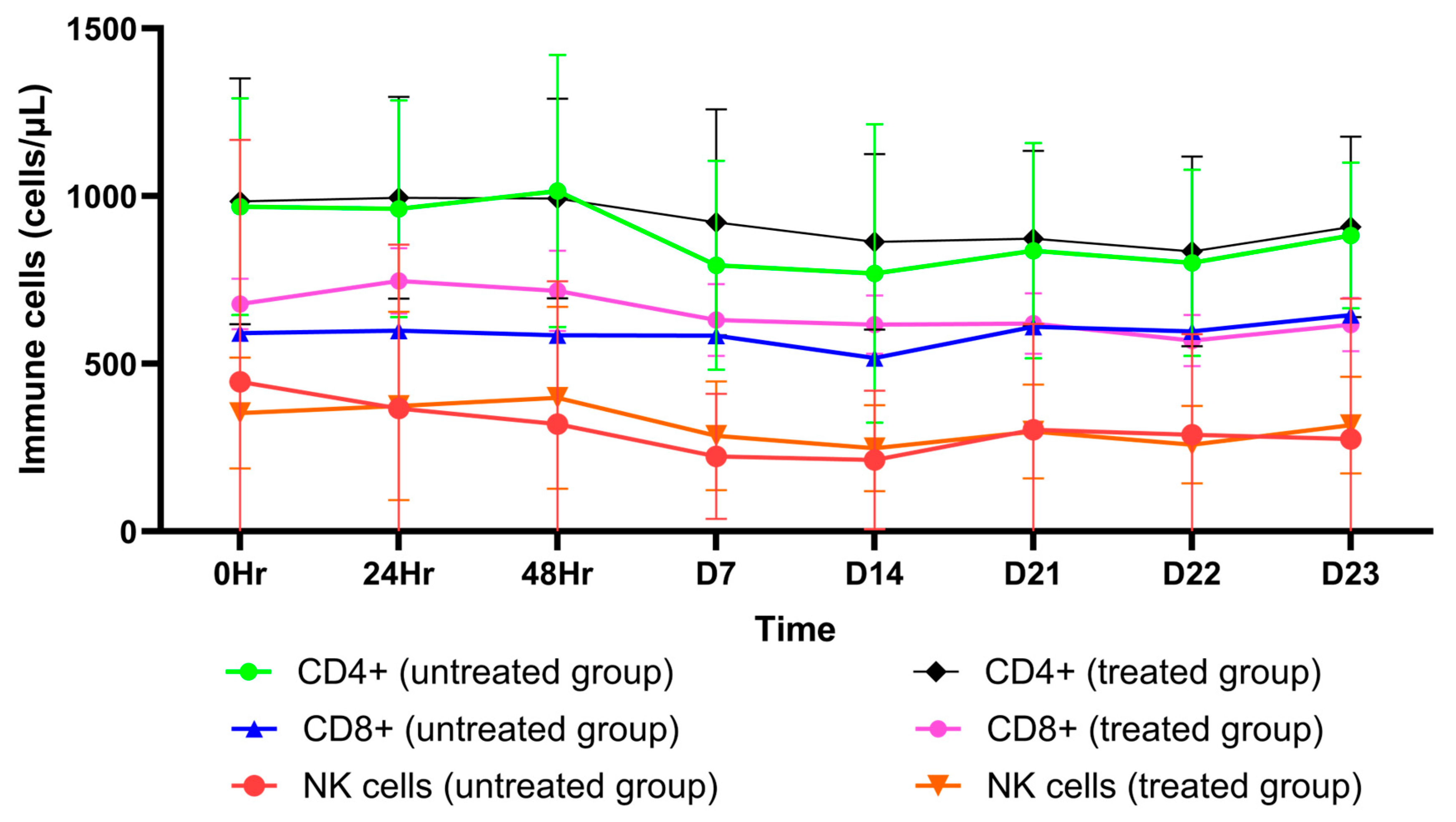
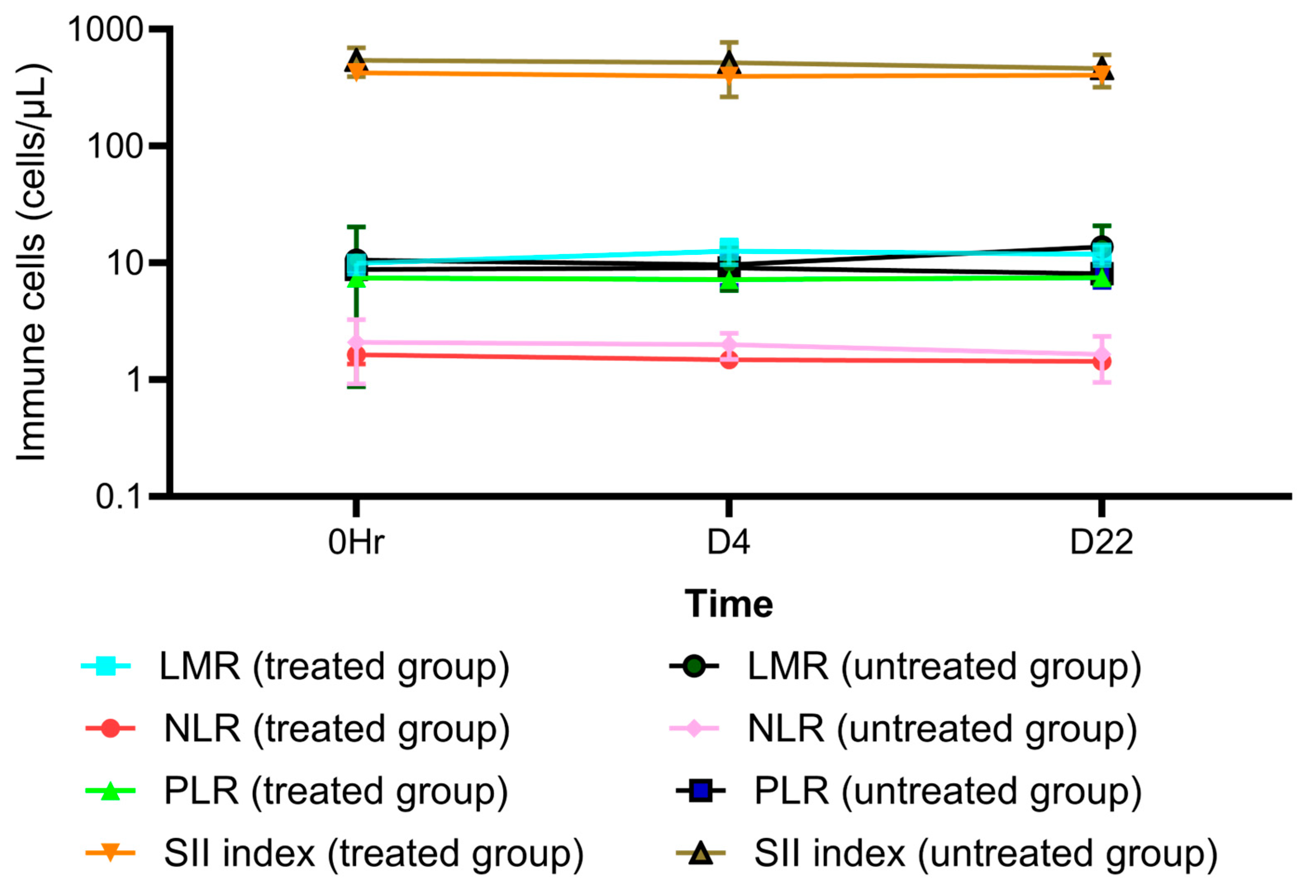
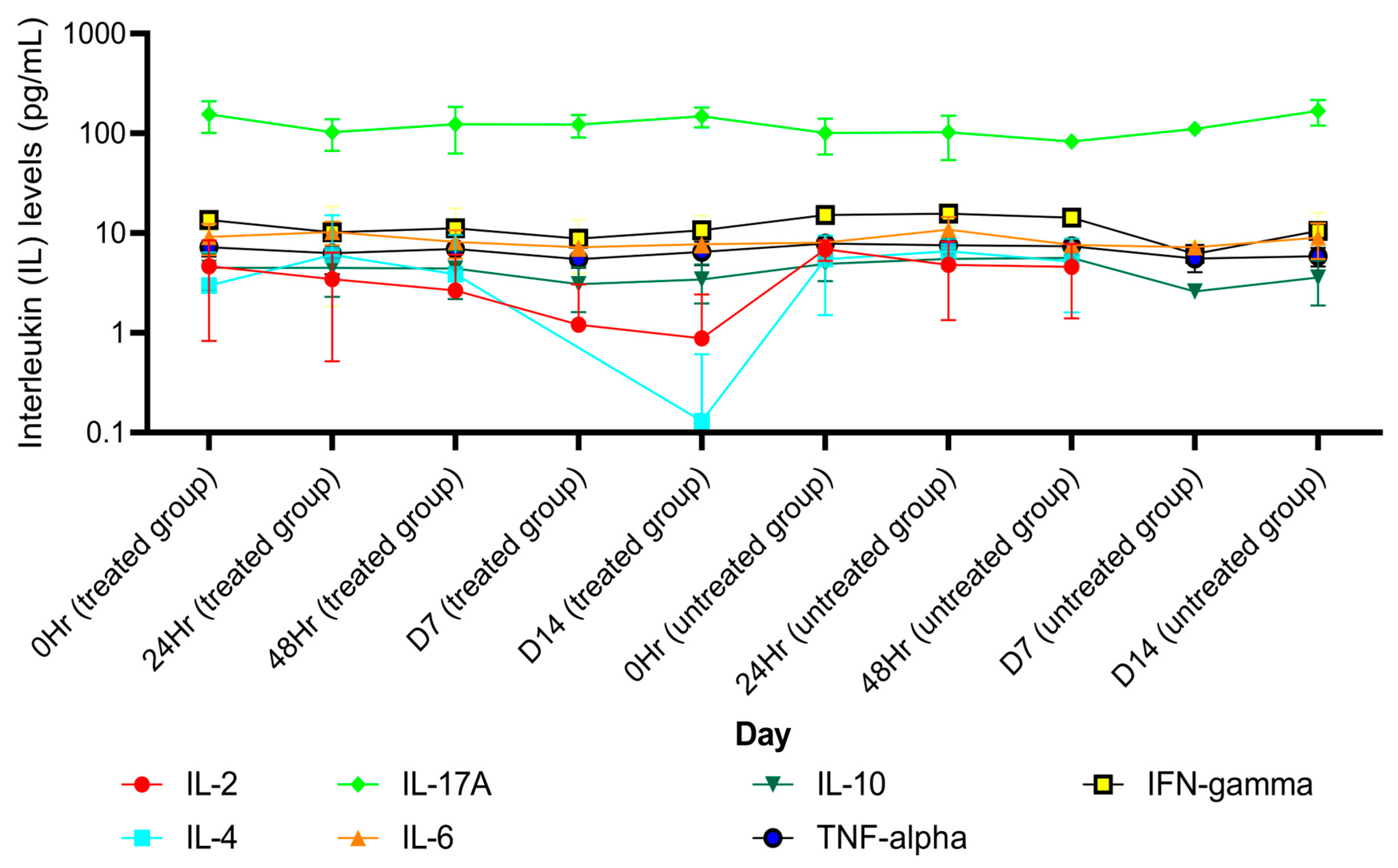
2.2. Immunomodulatory Effect of AL (Atractylodin): Effects on Circulating Peripheral Blood Cells, Immune Cells, and Pro-Inflammatory Cytokines
2.3. Model Validation and Sensitivity Analysis
2.4. Safety Assessment of the Simulated AL Regimens
2.4.1. Hematological Toxicities
2.4.2. Hepatotoxicities
3. Discussion
3.1. FIH Dose Regimen
3.2. The MTD Regimens
3.3. Recommended AL Dose Regimens for Phase-2A Clinical Trial
3.4. The Roles of Circulating Peripheral Cytokines and Peripheral Immune Cells in iCCA Therapy Based on Immunological Classification
4. Materials and Methods
4.1. Data Sources
4.2. Pharmacokinetic Analysis
4.3. Statistical Analysis
4.4. Model Construction
4.5. Model Validation
4.6. Sensitivity Analysis
4.7. Prediction of MTD Dosage Regimens Based on Immunomodulatory Activities
4.8. Prediction of MTD Regimens Based on Toxicity Criteria
4.9. Virtual Population Simulation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Loeuillard, E.; Conboy, C.B.; Gores, G.J.; Rizvi, S. Immunobiology of cholangiocarcinoma. JHEP Rep. 2019, 1, 297–311. [Google Scholar] [CrossRef] [PubMed]
- Job, S.; Rapoud, D.; Dos Santos, A.; Gonzalez, P.; Desterke, C.; Pascal, G.; Elarouci, N.; Ayadi, M.; Adam, R.; Azoulay, D.; et al. Identification of four immune subtypes characterized by distinct composition and functions of tumor microenvironment in intrahepatic cholangiocarcinoma. Hepatology 2021, 72, 965–981. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Larrañaga, M.; González-López, E.; Roa-Bautista, A.; Rodrigues, P.M.; Díaz-González, Á.; Banales, J.M.; López-Hoyos, M.; Santos-Laso, A.; Crespo, J. Immune checkpoint inhibitors: The emerging cornerstone in cholangiocarcinoma therapy? Liver Cancer 2021, 10, 545–560. [Google Scholar] [CrossRef]
- Ueno, M.; Ikeda, M.; Morizane, C.; Kobayashi, S.; Ohno, I.; Kondo, S.; Okano, N.; Kimura, K.; Asada, S.; Namba, Y.; et al. Nivolumab alone or in combination with cisplatin plus gemcitabine in Japanese patients with unresectable or recurrent biliary tract cancer: A non-randomised, multicentre, open-label, phase 1 study. Lancet. Gastroenterol. Hepatol. 2019, 4, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Kulma, I.; Panrit, L.; Plengsuriyakarn, T.; Chaijaroenkul, W.; Warathumpitak, S.; Na-Bangchang, K. A randomized placebo-controlled phase I clinical trial to evaluate the immunomodulatory activities of Atractylodes lancea (Thunb) DC. in healthy Thai subjects. BMC Complement. Altern. Med. 2021, 21, 61. [Google Scholar] [CrossRef] [PubMed]
- Na-Bangchang, K.; Kulma, I.; Plengsuriyakarn, T.; Tharavanij, T.; Kotawng, K.; Chemung, A.; Muhamad, N.; Karbwang, J. Phase I clinical trial to evaluate the safety and pharmacokinetics of capsule formulation of the standardized extract of Atractylodes lancea. J. Trad. Complement. Med. 2021, 11, 343–355. [Google Scholar] [CrossRef]
- Shebley, M.; Sandhu, P.; Riedmaier, A.E.; Jamei, M.; Narayanan, R.; Patel, A.; Peters, S.A.; Reddy, V.P.; Zheng, M.; de Zwart, L.; et al. Physiologically based pharmacokinetic model qualification and reporting procedures for regulatory submissions: A consortium perspective. Clin. Pharmacol. Ther. 2018, 104, 88–110. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P. Report from the EMA workshop on qualification and reporting of physiologically based pharmacokinetic (PBPK) modeling and simulation. CPT Pharmacomet. Syst. Pharmacol. 2017, 6, 71–72. [Google Scholar] [CrossRef]
- Liu, H.; Zhang, Q.D.; Li, Z.H.; Zhang, Q.Q.; Lu, L.G. Efficacy and safety of gemcitabine-based chemotherapies in biliary tract cancer: A meta-analysis. World J. Gastroenterol. 2014, 20, 18001–18012. [Google Scholar] [CrossRef]
- Möhring, C.; Feder, J.; Mohr, R.U.; Sadeghlar, F.; Bartels, A.; Mahn, R.; Zhou, T.; Marinova, M.; Feldmann, G.; Brossart, P.; et al. First line and second line chemotherapy in advanced cholangiocarcinoma and impact of dose reduction of chemotherapy: A retrospective analysis. Front. Oncol. 2021, 11, 717397. [Google Scholar] [CrossRef]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N. Engl. J. Med. 2020, 362, 1273–1281. [Google Scholar] [CrossRef]
- Griffiths, J.I.; Wallet, P.; Pflieger, L.T.; Stenehjem, D.; Liu, X.; Cosgrove, P.A.; Leggett, N.A.; McQuerry, J.A.; Shrestha, G.; Rossetti, M.; et al. Circulating immune cell phenotype dynamics reflect the strength of tumor-immune cell interactions in patients during chemotherapy. Proc. Nat. Acad. Sci. USA 2020, 117, 16072–16082. [Google Scholar] [CrossRef] [PubMed]
- Goeppert, B.; Frauenschuh, L.; Zucknick, M.; Stenzinger, A.; Andrulis, M.; Klauschen, F.; Joehrens, K.; Warth, A.; Renner, M.; Mehrabi, A.; et al. Prognostic impact of tumor-infiltrating immune cells on biliary tract cancer. Br. J. Cancer 2013, 109, 2665–2674. [Google Scholar] [CrossRef] [PubMed]
- Jun, X.; Fu, P.; Lei, Y.; Cheng, P. Pharmacological effects of medicinal components of Atractylodes lancea (Thunb) DC. Chin. Med. 2018, 13, 59. [Google Scholar] [CrossRef]
- Kida, A.; Mizukoshi, E.; Kido, H.; Toyama, T.; Terashima, T.; Arai, K.; Yamashita, T.; Fushimi, K.; Yamashita, T.; Sakai, Y.; et al. The characteristics of the immune cell profiles in peripheral blood in cholangiocarcinoma patients. Hepatol. Int. 2021, 15, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Jin, B.; Hu, W.; Su, S.; Xu, H.; Lu, X.; Sang, X.; Yang, H.; Mao, Y.; Du, S. The prognostic value of systemic inflammation response index in cholangiocarcinoma patients. Cancer Mag. Res. 2021, 13, 6263–6277. [Google Scholar] [CrossRef]
- Ren, Z.; Yue, Y.; Zhang, Y.; Dong, J.; Liu, Y.; Yang, X.; Lin, X.; Zhao, X.; Wei, Z.; Zheng, Y.; et al. Changes in the peripheral blood Treg cell proportion in hepatocellular carcinoma patients after transarterial chemoembolization with microparticles. Front. Immunol. 2021, 12, 624789. [Google Scholar] [CrossRef]
- Cheon, Y.K.; Cho, Y.D.; Moon, J.H.; Jang, J.Y.; Kim, Y.S.; Kim, Y.S.; Lee, M.S.; Lee, J.S.; Shim, C.S. Diagnostic utility of interleukin-6 (IL-6) for primary bile drug cancer and changes in serum IL-6 levels following photodynamic therapy. Am. J. Gastroenterol. 2007, 102, 2164–2170. [Google Scholar] [CrossRef]
- Vainer, N.; Dehlendorff, C.; Johansen, J.S. Systematic literature review of IL-6 as a biomarker or treatment target in patients with gastric, bile duct, pancreatic, and colorectal cancer. Oncotarget 2018, 9, 29820–29841. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Li, Z.; Hu, G. Prognostic role of intratumoral IL-17A expression by immunohistochemistry in solid tumors: A meta-analysis. Oncotarget 2017, 8, 66382–66391. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Kang, H.; Fung, A.; Zhao, H.; Wang, T.; Ma, D. The role of interleukin 17 in tumour proliferation, angiogenesis, and metastasis. Mediat. Inflamm. 2014, 2014, 623759. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, C.; Lu, S.; Xu, Y.; Li, Z.; Jiang, H.; Ma, Y. Tumor-associated macrophages in cholangiocarcinoma: Complex interplay and potential therapeutic target. EBioMedicine 2021, 67, 103375. [Google Scholar] [CrossRef]
- Mirlerkar, B. Tumor promoting roles of IL-10, TGF-β, IL-4, and IL-35: Its implications in cancer immunotherapy. Sage Open Med. 2022, 10, 20503121211069012. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, H.; Fujieda, K.; Senju, S.; Ikeda, T.; Oshiumi, H.; Nishimaru, Y. Immune-suppressive effects of interleukin-6 on T-cell-mediated anti-tumor immunity. Cancer Sci. 2018, 109, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Chinen, T.; Kannan, A.K.; Levine, A.G.; Fan, X.; Klein, U.; Zheng, Y.; Gasteiger, G.; Feng, Y.; Fontenot, J.D.; Rudensky, A.Y. An essential role of IL-2 receptor in Treg cell function. Nat. Immunol. 2016, 17, 1322–1333. [Google Scholar] [CrossRef] [PubMed]
- Ye, C.; Brand, D.; Zheng, S.G. Targeting IL-2: An unexpected effect in treating immunological diseases. Signal Transduct. Target. Ther. 2018, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Galluzzi, L.; Buque, A.; Kepp, O.; Zitvogel, L.; Kroemer, G. Immunological effects of conventional chemotherapy and targeted anticancer agents. Cancer Cell 2015, 28, 690–714. [Google Scholar] [CrossRef]
- Saeheng, T.; Na-Bangchang, K.; Siccardi, M.; Rajoli, R.K.R.; Karbwang, J. Physiologically-based pharmacokinetic modeling for optimal dosage prediction of quinine co-administered with ritonavir-boosted lopinavir. Clin. Pharmacol. Ther. 2020, 107, 1209–1220. [Google Scholar] [CrossRef] [PubMed]
- Saeheng, T.; Na-Bangchang, K.; Karbwang, J. Utility of physiologically based pharmacokinetic (PBPK) modeling in oncology drug development and its accuracy: A systematic review. Eur. J. Clin. Pharm. 2018, 74, 1365–1376. [Google Scholar] [CrossRef] [PubMed]
- Butthongkomvong, K.; Sirachainan, E.; Jhankumpha, S.; Kumdang, S.; Sukhontharot, O. Treatment outcome of palliative chemotherapy in inoperable cholangiocarcinoma in Thailand. Asian Pac. J. Cancer Prev. 2013, 14, 3565–3568. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Parameter | Value |
|---|---|---|
| Group 1 (Day 1) | ||
| 1 | AUC (µmol⋅h/L) | 0.55 |
| 2 | Cmax (µmol/L) | 0.25 |
| 3 | Vz/F (L/kg) | 11.33 |
| 4 | CL/F (L/h/kg) | 5.01 |
| 5 | T1/2 (h) | 1.63 |
| Group 2 (Day 1) | ||
| 6 | AUC (µmol·h/L) | 0.64 |
| 7 | Cmax (µmol/L) | 0.28 |
| 8 | Vz/F (L/kg) | 14.12 |
| 9 | CL/F (L/h/kg) | 7.55 |
| 10 | T1/2 (h) | 1.27 |
| Group 2 (Day 21) | ||
| 11 | AUC (µmol·h/L) | 0.72 |
| 12 | Cmax (µmol/L) | 0.30 |
| 13 | Vz/F (L/kg) | 13.41 |
| 14 | CL/F (L/h/kg) | 8.04 |
| 15 | T1/2 (h) | 1.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeheng, T.; Karbwang, J.; Na-bangchang, K. Immunomodulatory Effects of Atractylodes lancea in Healthy Volunteers with Dosage Prediction for Cholangiocarcinoma Therapy: A Modelling Approach. Pharmaceuticals 2025, 18, 198. https://doi.org/10.3390/ph18020198
Saeheng T, Karbwang J, Na-bangchang K. Immunomodulatory Effects of Atractylodes lancea in Healthy Volunteers with Dosage Prediction for Cholangiocarcinoma Therapy: A Modelling Approach. Pharmaceuticals. 2025; 18(2):198. https://doi.org/10.3390/ph18020198
Chicago/Turabian StyleSaeheng, Teerachat, Juntra Karbwang, and Kesara Na-bangchang. 2025. "Immunomodulatory Effects of Atractylodes lancea in Healthy Volunteers with Dosage Prediction for Cholangiocarcinoma Therapy: A Modelling Approach" Pharmaceuticals 18, no. 2: 198. https://doi.org/10.3390/ph18020198
APA StyleSaeheng, T., Karbwang, J., & Na-bangchang, K. (2025). Immunomodulatory Effects of Atractylodes lancea in Healthy Volunteers with Dosage Prediction for Cholangiocarcinoma Therapy: A Modelling Approach. Pharmaceuticals, 18(2), 198. https://doi.org/10.3390/ph18020198