
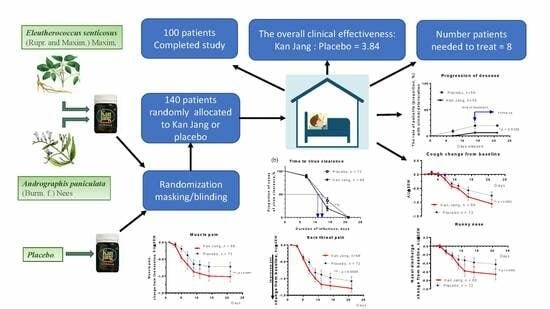
Efficacy of Kan Jang® in Patients with Mild COVID-19: A Randomized, Quadruple-Blind, Placebo-Controlled Trial



Abstract
:
1. Introduction
2. Results
2.1. Patients
Demographic and Baseline Characteristics
2.2. Efficacy
2.2.1. Primary Endpoints
The Rate of Patients with Clinical Deterioration and Virus Clearance
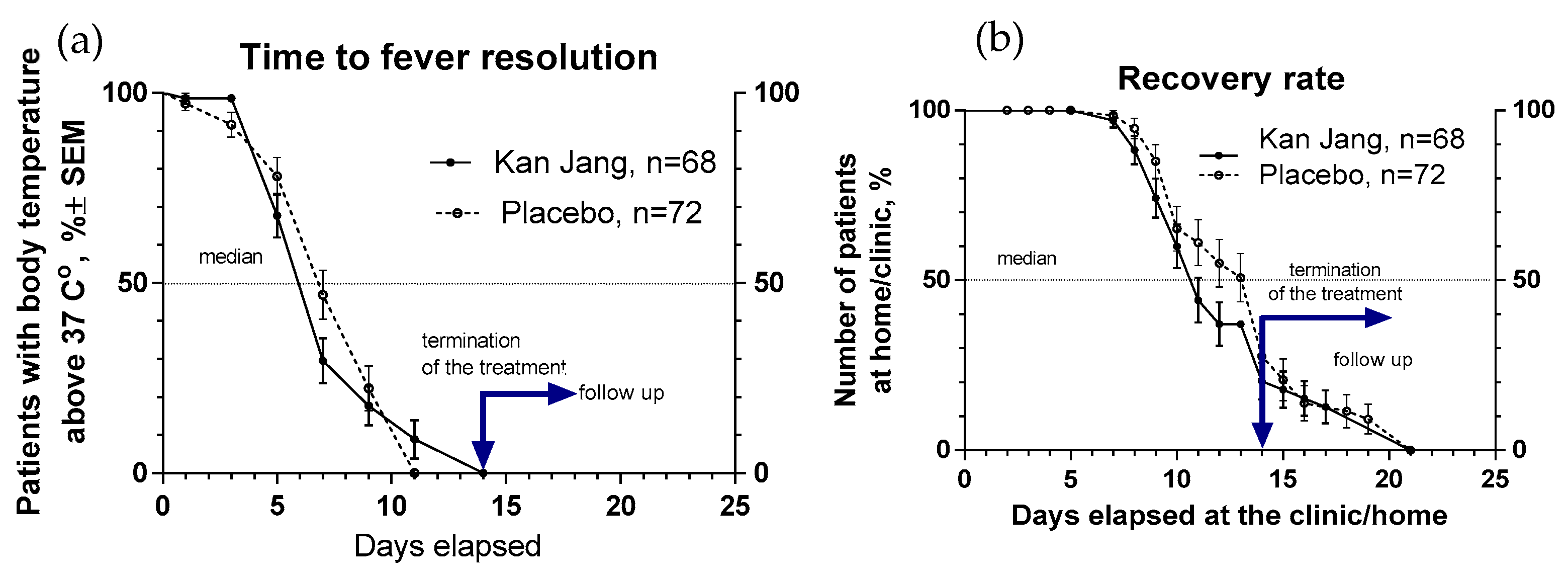
Recovery Time and Time to Fever Resolution
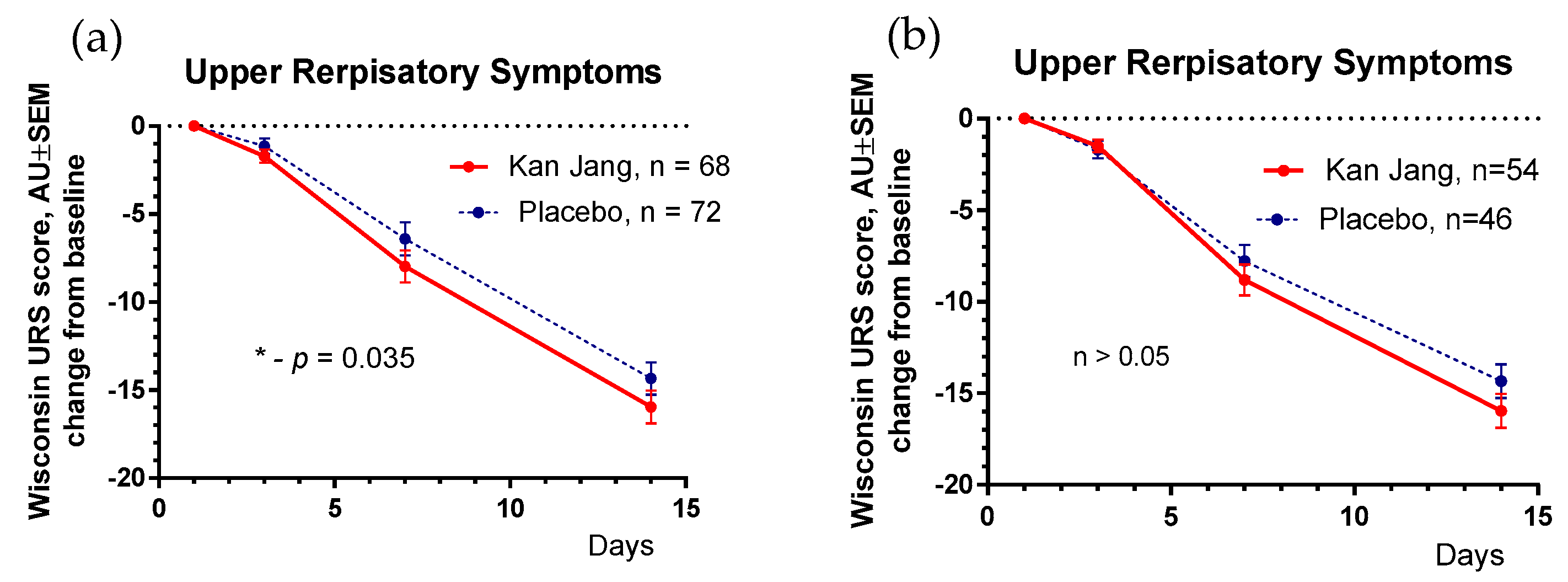
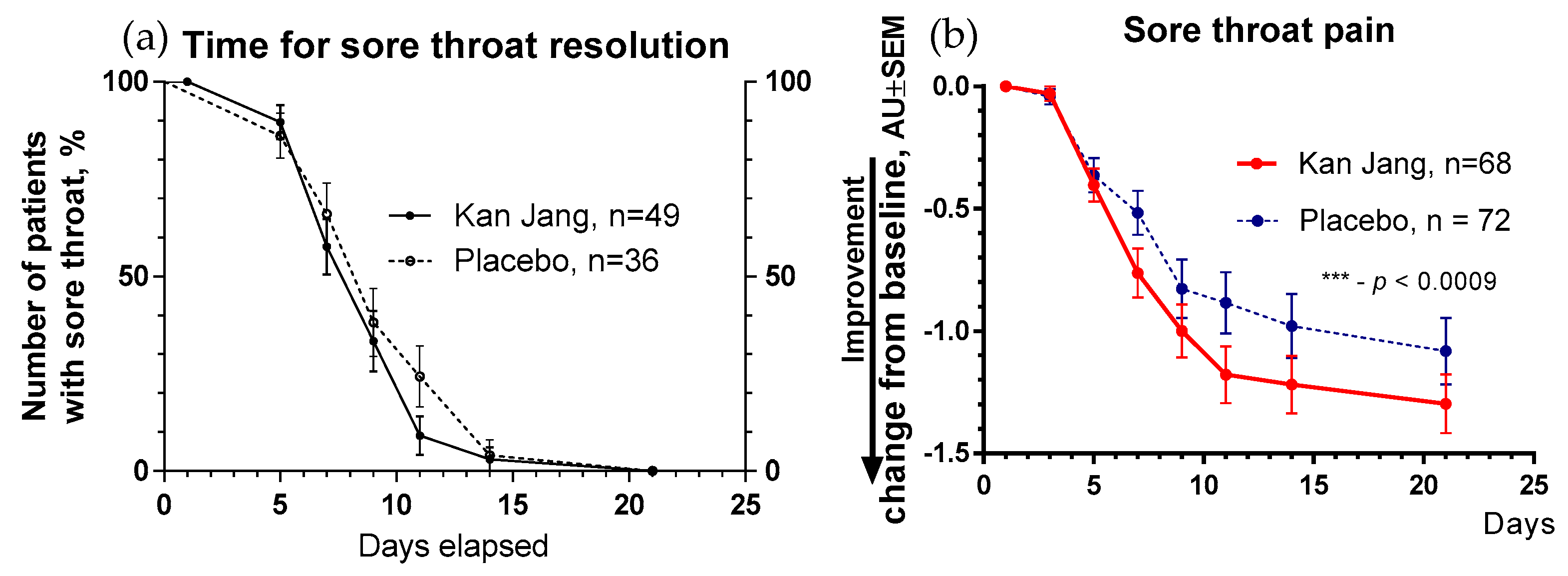
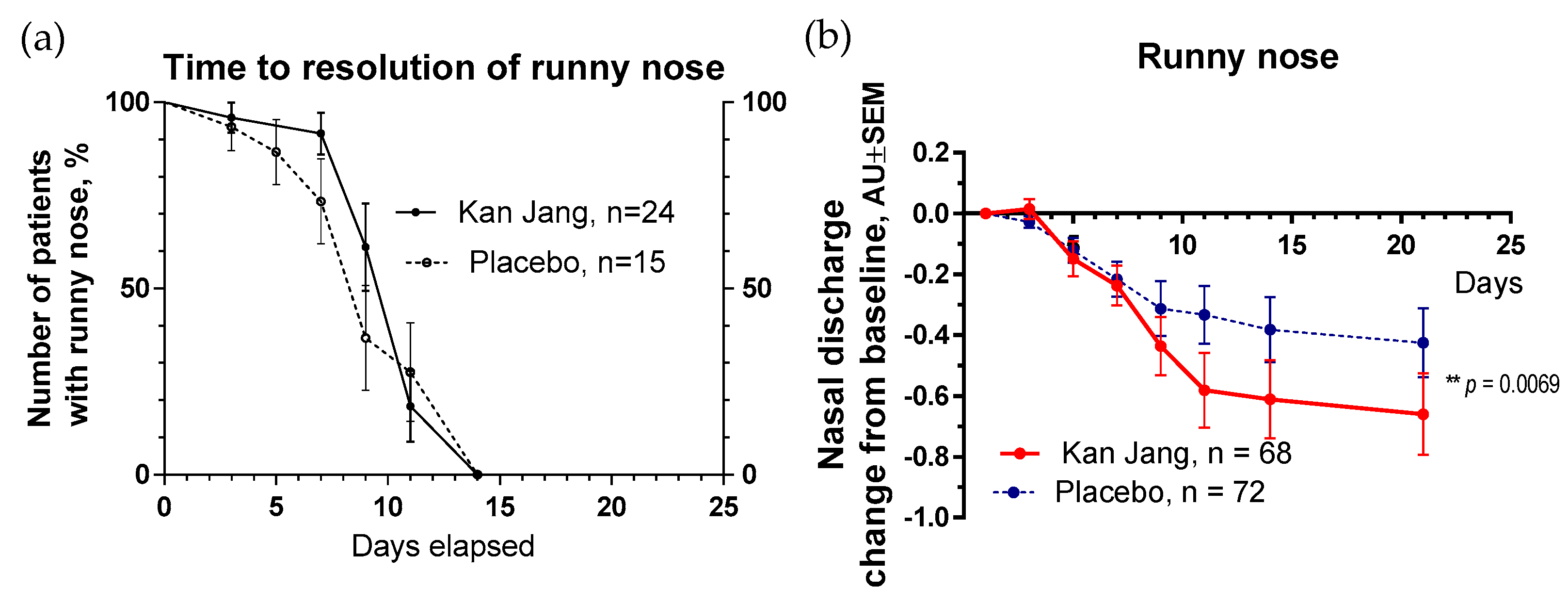
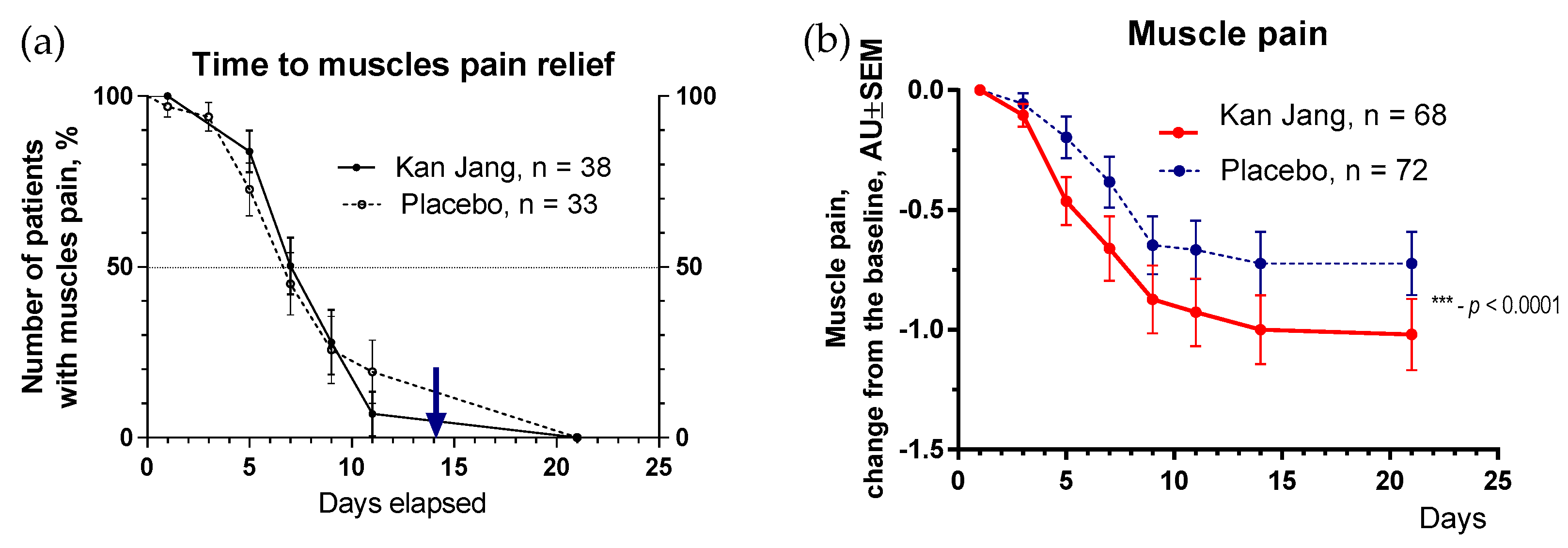
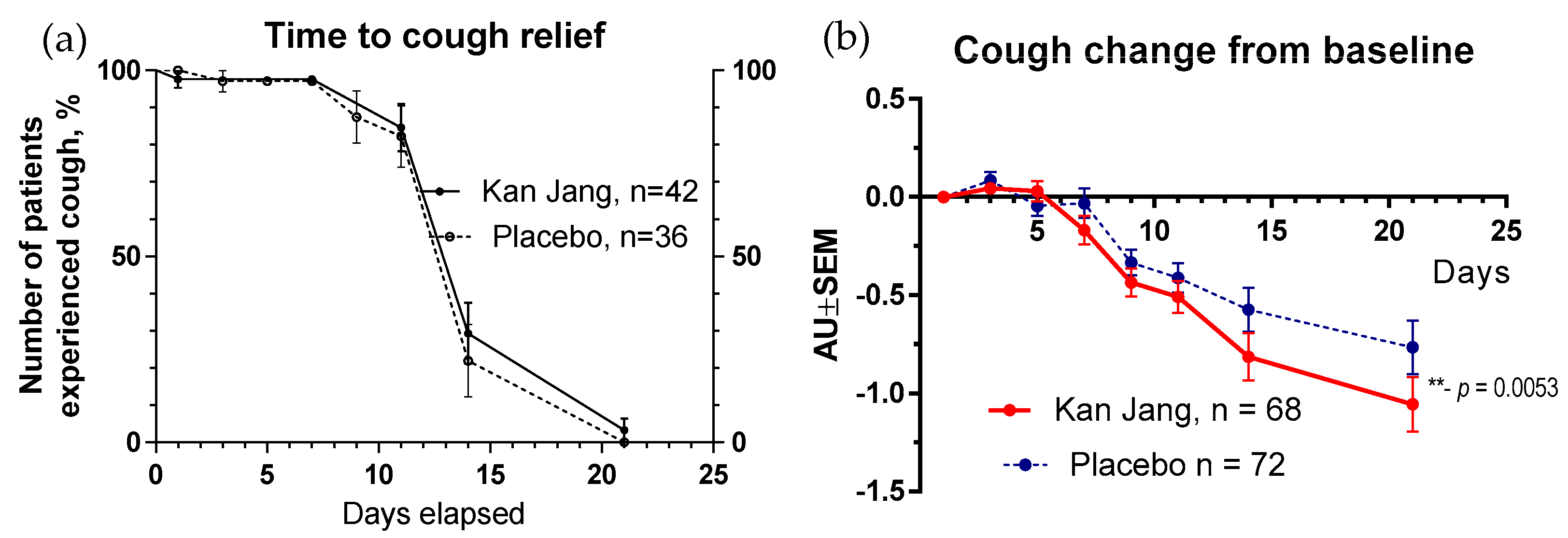
The Severity and Time to Resolution of Inflammatory Symptoms
2.2.2. Secondary Endpoints
Blood Serum Markers of Immune Response and Inflammation
Physical Activity and Physical and Cognitive Performance
2.3. Safety
3. Discussion
4. Materials and Methods
4.1. Study Design, Recruitment, Screening of Patients, and Schedule of Examinations
4.2. Datasets Analyzed and Evaluation of Compliance
4.3. Study Population and Inclusion and Exclusion Criteria
4.4. Intervention, Comparator, Doses, and Treatment Regimens
4.5. Randomization, Blinding, and Allocation Concealment
4.5.1. Randomization and Blinding
4.5.2. Allocation Concealment
4.5.3. Implementation and Blinding
4.6. Efficacy and Safety Outcomes and Endpoints
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; van de Veen, W.; Brüggen, M.C.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef] [PubMed]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Vardhana, S.A.; Wolchok, J.D. The many faces of the anti-COVID immune response. J. Exp. Med. 2020, 217, e20200678. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Fan, Y.; Lai, Y.; Han, T.; Li, Z.; Zhou, P.; Pan, P.; Wang, W.; Hu, D.; Liu, X.; et al. Coronavirus infections and immune responses. J. Med. Virol. 2020, 92, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Schijns, V.; Lavelle, E.C. Prevention and treatment of COVID-19 disease by controlled modulation of innate immunity. Eur. J. Immunol. 2020, 50, 932–938. [Google Scholar] [CrossRef]
- Lega, S.; Naviglio, S.; Volpi, S.; Tommasini, A. Recent Insight into SARS-CoV2 Immunopathology and Rationale for Potential Treatment and Preventive Strategies in COVID-19. Vaccines 2020, 8, 224. [Google Scholar] [CrossRef]
- Yang, R.; Liu, H.; Bai, C.; Wang, Y.; Zhang, X.; Guo, R.; Wu, S.; Wang, J.; Leung, E.; Chang, H.; et al. Chemical composition and pharmacological mechanism of Qingfei Paidu Decoction and Ma Xing Shi Gan Decoction against Coronavirus Disease 2019 (COVID-19): In silico and experimental study. Pharmacol. Res. 2020, 157, 104820. [Google Scholar] [CrossRef]
- Panossian, A.; Brendler, T. The Role of Adaptogens in Prophylaxis and Treatment of Viral Respiratory Infections. Pharmaceuticals 2020, 13, 236. [Google Scholar] [CrossRef]
- Panossian, A.; Seo, E.J.; Wikman, G.; Efferth, T. Synergy assessment of fixed combinations of Herba Andrographidis and Radix Eleutherococci extracts by transcriptome-wide microarray profiling. Phytomedicine 2015, 22, 981–992. [Google Scholar] [CrossRef]
- Panossian, A.; Efferth, T. Network Pharmacology of Adaptogens in the Assessment of Their Pleiotropic Therapeutic Activity. Pharmaceuticals 2022, 15, 1051. [Google Scholar] [CrossRef]
- Melchior, J.; Palm, S.; Wikman, G. Controlled clinical study of standardized Andrographis paniculata extract in common cold—A pilot trial. Phytomedicine 1997, 3, 315–318. [Google Scholar] [CrossRef]
- Melchior, J.; Spasov, A.A.; Ostrovskij, O.V.; Bulanov, A.E.; Wikman, G. Double-blind, placebo-controlled pilot and phase III study of activity of standardized Andrographis paniculata Herba Nees extract fixed combination (Kan Jang®) in the treatment of uncomplicated upper-respiratory tract infection. Phytomedicine 2000, 7, 341–350. [Google Scholar] [CrossRef]
- Gabrielian, E.S.; Shukarian, A.K.; Goukasova, G.I.; Chandanian, G.L.; Panossian, A.G.; Wikman, G.; Wagner, H. A double blind, placebo-controlled study of Andrographis paniculata fixed combination Kan Jang in the treatment of acute upper respiratory tract infections including sinusitis. Phytomedicine 2002, 9, 589–597. [Google Scholar] [CrossRef]
- Kulichenko, L.L.; Kireyeva, L.; Malyshkina, E.N.; Wikman, G. A randomized, controlled study of Kan Jang® versus amantadine in the treatment of influenza in Volgograd. J. Herb. Pharmacother. 2003, 173, 188–194. [Google Scholar] [CrossRef]
- Spasov, A.A.; Ostrovskij, O.V.; Chernikov, M.V.; Wikman, G. Comparative controlled study of Andrographis paniculata fixedcombination, Kan Jang and an Echinacea preparation as adjuvant, in the treatment of uncomplicated respiratory disease in children. Phytother. Res. 2004, 18, 47–53. [Google Scholar] [CrossRef]
- Panossian, A.; Wikman, G. Efficacy of Andrographis paniculata in upper respiratory tract (URT) infectious diseases and the mechanism of action. In Evidence and Rational Based Research on Chinese Drugs; Wagner, H., Ulrich Merzenich, G., Eds.; Springer: Vienna, Austria, 2012; pp. 137–180. [Google Scholar]
- Narimanyan, M.; Jamalyan, K.; Balyan, A.; Barth, A.; Palm, S.; Wikman, G.; Panossian, A. Early intervention with Kan Jang® to treat upper-respiratory tract infections: A randomized, quadruple-blind study. J. Tradit. Complement. Med. 2021, 11, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Ratiani, L.; Pachkoria, E.; Mamageishvili, N.; Shengelia, R.; Hovhannisyan, A.; Panossian, A. Efficacy of Kan Jang® in Patients with Mild COVID-19: Interim Analysis of a Randomized, Quadruple-Blind, Placebo-Controlled Trial. Pharmaceuticals 2022, 15, 1013. [Google Scholar] [CrossRef] [PubMed]
- Jain, V.K.; Iyengar, K.P.; Vaishya, R. Differences between first wave and second wave of COVID-19 in India. Diabetol. Metab. Syndr. 2021, 15, 1047–1048. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection Is Suspected: Interim Guidance. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/clinical-management-of-novel-cov.pdf (accessed on 28 July 2023).
- Lamb, Y.N. Nirmatrelvir Plus Ritonavir: First Approval. Drugs 2022, 82, 585–591. [Google Scholar] [CrossRef]
- National Institutes of Health. Antiviral Drugs That Are Approved, Authorized, or Under Evaluation for the Treatment of COVID-19. In COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines; Last Updated: 29 April 2022; National Institutes of Health: Bethesda, MD, USA, 2022; Available online: https://files.covid19treatmentguidelines.nih.gov/guidelines/covid19treatmentguidelines.pdf; pp. 140–221. https://files.covid19treatmentguidelines.nih.gov/guidelines/section/section_36.pdf; (accessed on 29 April 2022). [Google Scholar]
- Molnupiravir_COVID19-MSD—Art 5(3)—Conditions for Use (europa.eu). Available online: https://www.ema.europa.eu/en/documents/referral/lagevrio-also-known-molnupiravir-mk-4482-covid-19-article-53-procedure-conditions-use-conditions_en.pdf (accessed on 7 August 2022).
- Yuvejwattana, S. Thailand Clears Use of Herbal Medicine for COVID-19 Treatment; Bloomberg; 30 December 2020, 7:02 AM GMT+1. Available online: https://www.bloomberg.com/news/articles/2020-12-30/thailand-clears-use-of-herbal-medicine-for-covid-19-treatment (accessed on 28 July 2023).
- Yearsley, C. Thailand Approves Asian Herb Andrographis to Treat COVID-19. HerbalGram. 2021, 129, 35–37. [Google Scholar]
- Karbwang, J.; Na-Bangchang, K. Repurposed drugs for COVID-19 treatment. J. Thai. Trad. Alt. Med. 2021, 19, 285–302. [Google Scholar]
- World Health Organization. Therapeutics and COVID-19. Therapeutic Management of Hospitalized Adults with COVID-19; Last Updated: 24 February 2022. Available online: https://www.covid19treatmentguidelines.nih.gov/management/clinicalmanagement/hospitalized-adults--therapeutic-management/ (accessed on 7 August 2022).
- Tong, L.; Ma, Z.; Zhou, Y.; Yang, S.; Yang, Y.; Luo, J.; Huang, J.; Wang, F. Combination of Chinese herbal medicine and conventional western medicine for coronavirus disease 2019: A systematic review and meta-analysis. Front. Med. 2023, 10, 1175827. [Google Scholar] [CrossRef] [PubMed]
- Ji, Z.; Hu, H.; Qiang, X.; Lin, S.; Pang, B.; Cao, L.; Zhang, L.; Liu, S.; Chen, Z.; Zheng, W.; et al. Traditional Chinese Medicine for COVID-19: A Network Meta-Analysis and Systematic Review. Am. J. Chin. Med. 2022, 50, 883–925. [Google Scholar] [CrossRef]
- Wu, H.T.; Ji, C.H.; Dai, R.C.; Hei, P.J.; Liang, J.; Wu, X.Q.; Li, Q.S.; Yang, J.C.; Mao, W.; Guo, Q. Traditional Chinese medicine treatment for COVID-19: An overview of systematic reviews and meta-analyses. J. Integr. Med. 2022, 20, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Xu, N.; Zhou, Y.; Song, J.; Liu, J.; Zhu, H.; Jiang, J.; Xu, Y.; Li, R. Contribution of traditional Chinese medicine combined with conventional western medicine treatment for the novel coronavirus disease (COVID-19), current evidence with systematic review and meta-analysis. Phytother. Res. 2021, 35, 5992–6009. [Google Scholar] [CrossRef]
- Liang, S.B.; Fang, M.; Liang, C.H.; Lan, H.D.; Shen, C.; Yan, L.J.; Hu, X.Y.; Han, M.; Robinson, N.; Liu, J.P. Therapeutic effects and safety of oral Chinese patent medicine for COVID-19: A rapid systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2021, 60, 102744. [Google Scholar] [CrossRef]
- Wanaratna, K.; Leethong, P.; Inchai, N.; Chueawiang, W.; Sriraksa, P.; Tabmee, A.; Sirinavin, S. Efficacy and Safety of Andrographis paniculata Extract in Patients with Mild COVID-19: A Randomized Controlled Trial. medRxiv. 2021. Available online: https://www.semanticscholar.org/paper/Efficacy-and-safety-of-Andrographis-paniculata-in-A-Wanaratna-Leethong/1f40a6181de4e0f15ab296673794210e82236455 (accessed on 7 August 2022).
- Rattanaraksa, D.; Khempetch, R.; Poolwiwatchaikool, U.; Nimitvilai, S.; Loatrakul, O.; Srimanee, P. The efficacy and safety of Andrographis paniculata extract for the treatment of COVID-19 patients with mild symptoms, Nakhonpathom hospital. Reg. Med. J. 2021, 40, 269–281. [Google Scholar]
- Tanwettiyanont, J.; Piriyachananusorn, N.; Sangsoi, L.; Boonsong, B.; Sunpapoa, C.; Tanamatayarat, P.; Kanchanasurakit, S.; Na-Ek, N. The efficacy of Andrographis paniculata (Burm.f.) Wall. ex Nees crude extract in hospitalized mild COVID-19 patients: A retrospective cohort study. medRxiv 2022. [Google Scholar] [CrossRef]
- Shanker, K.; Rangnekar, H.; Wele, A.; Soni, P.; Gaikwad, P.; Pal, A.; Bawankule, D.U.; Chanda, D. A randomized controlled pilot study of add-on therapy of CIM-MEG19 (standardized Andrographis paniculata formulation) in mild to moderate COVID-19. Phytomed. Plus. 2023, 3, 100398. [Google Scholar] [CrossRef]
- Zhang, X.; Lv, L.; Zhou, Y.; Xie, L.; Xu, Q.; Zou, X.; Ding, Y.; Tian, J.; Fan, J.; Fan, H.; et al. Efficacy and safety of Xiyanping injection in the treatment of COVID-19: A multicenter, prospective, open-label and randomized controlled trial. Phytother. Res. 2021, 35, 4401–4410. [Google Scholar] [CrossRef]
- Kaewdech, A.; Nawalerspanya, S.; Assawasuwannakit, S.; Chamroonkul, N.; Jandee, S.; Sripongpun, P. The use of Andrographis paniculata and its effects on liver biochemistry of patients with gastrointestinal problems in Thailand during the COVID-19 pandemic: A cross sectional study. Sci. Rep. 2022, 12, 18213. [Google Scholar] [CrossRef]
- Tanwettiyanont, J.; Piriyachananusorn, N.; Sangsoi, L.; Boonsong, B.; Sunpapoa, C.; Tanamatayarat, P.; Na-Ek, N.; Kanchanasurakit, S. Use of Andrographis paniculata (Burm.f.) Wall. ex Nees and risk of pneumonia in hospitalised patients with mild coronavirus disease 2019: A retrospective cohort study. Front. Med. 2022, 9, 947373. [Google Scholar] [CrossRef]
- Intharuksa, A.; Arunotayanun, W.; Yooin, W.; Sirisa-Ard, P. A Comprehensive Review of Andrographis paniculata (Burm. f.) Nees and Its Constituents as Potential Lead Compounds for COVID-19 Drug Discovery. Molecules 2022, 27, 4479. [Google Scholar] [CrossRef] [PubMed]
- Izcovich, A.; Siemieniuk, R.A.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Kum, E.; Qasim, A.; Khamis, A.M.; Rochwerg, B.; Agoritsas, T.; et al. Adverse effects of remdesivir, hydroxychloroquine and lopinavir/ritonavir when used for COVID-19: Systematic review and meta-analysis of randomised trials. BMJ Open 2022, 12, e048502. [Google Scholar] [CrossRef] [PubMed]
- Gupte, V.; Hegde, R.; Sawant, S.; Kalathingal, K.; Jadhav, S.; Malabade, R.; Gogtay, J. Safety and clinical outcomes of remdesivir in hospitalised COVID-19 patients: A retrospective analysis of active surveillance database. BMC Infect. Dis. 2022, 22, 1. [Google Scholar] [CrossRef] [PubMed]
- Shang, Y.X.; Shen, C.; Stub, T.; Zhu, S.J.; Qiao, S.Y.; Li, Y.Q.; Wang, R.T.; Li, J.; Liu, J.P. Adverse Effects of Andrographolide Derivative Medications Compared to the Safe use of Herbal Preparations of Andrographis paniculata: Results of a Systematic Review and Meta-Analysis of Clinical Studies. Front. Pharmacol. 2022, 13, 773282. [Google Scholar] [CrossRef]
- Brekhman, I.I. On Antitoxic Action of Eleutherococcus; Meditsina: Moscow, Russia, 1982; Volume 37. [Google Scholar]
- HMPC—Committee on HerbalMedicinal Products. Assessment Report on Eleutherococcus senticosus (Rupr. etMaxim.) Maxim, Radix.EMA/HMPC/680615/2013. 25 March 2014, pp. 1–51. Available online: https://www.ema.europa.eu/en/documents/herbal-report/final-assessment-report-eleutherococcus-senticosus-rupr-et-maxim-maxim-radix_en.pdf (accessed on 30 May 2022).
- Seo, E.J.; Klauck, S.M.; Efferth, T.; Panossian, A. Adaptogens in chemobrain (Part II): Effect of plant extracts on chemotherapy induced cytotoxicity in neuroglia cells. Phytomedicine 2019, 58, 152743. [Google Scholar] [CrossRef]
- Seo, E.J.; Klauck, S.M.; Efferth, T.; Panossian, A. Adaptogens in chemobrain (Part III): Antitoxic effects of plant extracts towards cancer chemotherapy-induced toxicity-transcriptome-wide microarray analysis of neuroglia cells. Phytomedicine 2019, 56, 246–260. [Google Scholar] [CrossRef]
- Panossian, A.; Seo, E.J.; Klauck, S.M.; Efferth, T. Adaptogens in chemobrain (part IV): Adaptogenic plants prevent the chemotherapeutics-induced imbalance of redox homeostasis by modulation of expression of genes encoding Nrf2-mediated signaling proteins and antioxidant, metabolizing, detoxifying enzymes in neuroglia cells. Longhua Chin. Med. 2020, 3, 4. [Google Scholar]
- Lim, X.Y.; Chan, J.; Tan, T.Y.; Teh, B.P.; Mohd Abd Razak, M.R.; Mohamad, S.B.; Syed Mohamed, A.F. Andrographis paniculata (Burm. F.) Wall. Ex Nees, Andrographolide, and Andrographolide Analogues as SARS-CoV-2 Antivirals? A Rapid Review. Nat. Prod. Commun. 2021, 16, 1934578X211016610. [Google Scholar] [CrossRef]
- Gagnier, J.J.; Boon, H.; Rochon, P.; Moher, D.; Barnes, J.; Bombardier, C.; CONSORT Group. Recommendations for reporting randomized controlled trials of herbal interventions: Explanation and elaboration. J. Clin. Epidemiol. 2006, 59, 1134–1149. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unit | Group A Kan Jang | Group B Placebo | Signif. of Difference | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameters | n | Mean | SD. | n | Mean | SD. | p-Value | ||
| Age | Years | 68 | 50.35 | 17.82 | 72 | 45.74 | 16.82 | 0.143 b | |
| Gender, Male/Female, %—53/87 = 61% | Male/Female | 68 | 28/40 = 70% | 72 | 25/47 = 53% | 0.785 | |||
| BMI | kg/m2 | 68 | 24.58 | 3.274 | 72 | 24.52 | 3.376 | 0.908 b | |
| Start of symptoms | days | 68 | <3 | 72 | <3 | ||||
| Viral load, SARS-CoV-2 | % | 68 | 100 | 72 | 100 | ||||
| Body temperature | °C | 68 | 37.86 | 0.58 | 72 | 37.7 | 0.59 | 0.148 b | |
| Fatigue | 100% patients | A.U. | 68 | 1.794 | 0.407 | 72 | 1.819 | 0.539 | 0.755 b |
| Headache | 91% of patients | AU. | 64 | 1.859 | 0.393 | 63 | 1.794 | 0.480 | 0.443 b |
| Sore throat | 62% of patients | AU. | 49 | 1.776 | 0.422 | 38 | 1.632 | 0.633 | 0.2573 b |
| Cough | 55% of patients | AU. | 41 | 1.902 | 0.490 | 36 | 1.833 | 0.378 | 0.606 b |
| Pain in muscles ** | 51% of patients | AU. | 39 | 1.872 ** | 0.656 | 32 | 1.469 ** | 0.671 | 0.013 a |
| Runny nose | 27% of patients | AU. | 23 | 1.957 | 0.475 | 15 | 1.733 | 0.458 | 0.247 b |
| Loss of smell ** | 16% of patients | AU. | 8 | 2.375 ** | 0.744 | 14 | 1.714 ** | 0.469 | 0.036 b |
| Loss of taste | 4% of patients | AU. | 4 | 2.500 | 0.577 | 2 | 3.000 | 0 | 0.312 b |
| Physical activity ** | AU. | 68 | 12.75 ** | 2.984 | 72 | 13.85 ** | 3.005 | 0.019 b | |
| Physical activity (daily walk) ** | min | 68 | 7.279 ** | 8.614 | 72 | 12.57 ** | 13.45 | 0.008 b | |
| Decreased attention (d2-test) | %E (errors) | 68 68 | 28.34 | 21.47 | 72 | 26.00 | 26.83 | 0.189 b | |
| URTI ** | WI score | 68 | 17.59 * | 6.497 | 72 | 14.69 * | 5.832 | 0.006 a | |
| QOL | WI score | 68 | 36.29 | 12.15 | 72 | 37.14 | 12.81 | 0.163 b | |
| Blood serum IL-6 (normal level < 7 pg/mL) | pg/mL | 68 | 12.60 | 54.29 | 72 | 9.39 | 17.86 | 0.970 b | |
| D-dimer (normal range from 0.1 to 0.5 mg/L) | mg/L | 68 | 0.812 | 1.528 | 72 | 4.431 | 32.94 | 0.672 b | |
| C-reactive protein (normal level < 5 mg/L) | mg/L | 68 | 12.74 | 13.82 | 72 | 16.86 | 23.30 | 0.989 | |
| ALT (normal level < 35 U/L) | U/L | 68 | 27.69 | 19.90 | 72 | 26.79 | 20.46 | 0.831 | |
| AST (normal level < 32 U/L) | U/L | 68 | 25.32 | 19.07 | 72 | 26.83 | 19.49 | 0.241 | |
| Total WBC count (normal range: 3.6–11.0 × 109 cells/L) | 109/L | 68 | 5.872 | 1.863 | 72 | 5.271 | 1.936 | 0.064 | |
| Erythrocytes, RBC (normal range: 3.8–5.8 × 1012 cells/L) | 1012/L | 68 | 4.699 | 0.479 | 72 | 4.770 | 0.601 | 0.231 | |
| Hemoglobin, Hb (normal range: 13.5–17.0 g/dL) | g/dL | 68 | 12.95 | 1.647 | 72 | 13.51 | 1.706 | 0.053 | |
| Hematocrit, HCT (normal range: 40–50, L/L) | L/L | 68 | 40.48 | 4.924 | 72 | 41.56 | 6.179 | 0.064 | |
| Platelet count (normal range: 150–380 × 103 cells/μL) | 103 μL | 68 | 207.1 | 49.49 | 72 | 200.8 | 51.22 | 0.565 | |
| Neutrophil count (normal range: 1.8–7.5 × 109 cells/L) | 109/L | 68 | 60.090 * | 11.80 | 72 | 62.49 * | 13.43 | 0.458 | |
| Lymphocyte count (normal range: 1.0–4.0 × 109 cells/L) | 109/L | 68 | 28.72 * | 11.47 | 72 | 27.54 * | 12.33 | 0.560 | |
| Monocyte count (normal range: 0.1–1.0 × 109 cells/L) | 109/L | 68 | 9.194 * | 15.47 | 72 | 6.457 * | 3.572 | 0.132 | |
| Eosinophil count (normal range: 0.1–0.4 × 109 cells/L) | 109/L | 68 | 1.615 * | 1.391 | 72 | 1.285 * | 1.136 | 0.144 | |
| Basophil Count (normal range: 0.01–0.1 × 109 cells/L) | 109/L | 68 | 0.471 * | 0.229 | 72 | 0.477 * | 0.296 | 0.722 | |
| Treatment | Follow-Up | |||||||
|---|---|---|---|---|---|---|---|---|
| Day 1 Screening | Day 3 | Day 5 | Day 7 | Day 9 | Day 11 | Day 14 | Day 21 | |
| Doctor’s visits | 1 Baseline | 2 | 3 | 4 | ||||
| Eligibility check/information | * | |||||||
| Informed consent | * | |||||||
| Clinical examination | * | * | * | * | ||||
| Enrollment and allocation to intervention | * | |||||||
| Treatment (Kan Jang or placebo) | * | * | * | * | * | * | * | |
| Biomarker assessments | ||||||||
| Body temperature (fever) | * | * | * | * | * | * | * | * |
| COVID-19 PCR test | * | * | * | * | ||||
| Blood serum cytokine IL-6 (pg/mL) | * | * | * | * | ||||
| D-dimer (mg/L) | * | * | * | |||||
| C-reactive protein (mg/L) | * | * | * | |||||
| Blood cell count analysis | * | * | * | |||||
| ALT/AST | * | * | ||||||
| Clinician- and observer-reported outcome assessments | ||||||||
| Cognitive performance (tests for attention and memory): d2 test Wisconsin URS survey score | * * | * | * * | * * | * | |||
| Drug intake accountability | * | |||||||
| Adverse events | * | * | * | |||||
| Patient-reported outcome assessments | ||||||||
Mild COVID-19 symptoms:
| * | * | * | * | * | * | * | * |
| Workout, min | * | * | * | * | ||||
| Physical activity (questionnaire) | * | * | * | * | ||||
| Paracetamol intake recording Rescue medication intake recording | * * | * * | * * | * * | * * | * * | * * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ratiani, L.; Pachkoria, E.; Mamageishvili, N.; Shengelia, R.; Hovhannisyan, A.; Panossian, A. Efficacy of Kan Jang® in Patients with Mild COVID-19: A Randomized, Quadruple-Blind, Placebo-Controlled Trial. Pharmaceuticals 2023, 16, 1196. https://doi.org/10.3390/ph16091196
Ratiani L, Pachkoria E, Mamageishvili N, Shengelia R, Hovhannisyan A, Panossian A. Efficacy of Kan Jang® in Patients with Mild COVID-19: A Randomized, Quadruple-Blind, Placebo-Controlled Trial. Pharmaceuticals. 2023; 16(9):1196. https://doi.org/10.3390/ph16091196
Chicago/Turabian StyleRatiani, Levan, Elene Pachkoria, Nato Mamageishvili, Ramaz Shengelia, Areg Hovhannisyan, and Alexander Panossian. 2023. "Efficacy of Kan Jang® in Patients with Mild COVID-19: A Randomized, Quadruple-Blind, Placebo-Controlled Trial" Pharmaceuticals 16, no. 9: 1196. https://doi.org/10.3390/ph16091196
APA StyleRatiani, L., Pachkoria, E., Mamageishvili, N., Shengelia, R., Hovhannisyan, A., & Panossian, A. (2023). Efficacy of Kan Jang® in Patients with Mild COVID-19: A Randomized, Quadruple-Blind, Placebo-Controlled Trial. Pharmaceuticals, 16(9), 1196. https://doi.org/10.3390/ph16091196